
Abstract
The results of this study showed the importance of autonomous motivation for healthy eating. Autonomous motivation and female gender were the determinants most strongly associated with fruits, vegetables, and berries intake among patients with type 2 diabetes. Other determinants of fruits, vegetables, and berries intake were high education, high social support, high age, and a strong sense of coherence. Autonomous motivation and self-care competence mediated the effect of perceived autonomy support from a physician on fruits, vegetables, and berries intake. Thus, physicians can promote patients’ fruits, vegetables, and berries intake by supporting their autonomous motivation and self-care competence. The results are in line with self-determination theory.
Background
Type 2 diabetes is rapidly increasing all over the world. Approximately 415 million adult people already have diabetes, and this number is expected to rise to 642 million by 2040 (International Diabetes Federation, 2015). In Finland, 550,000 people have diabetes of which 91 percent is type 2 (National Institute for Health and Welfare (THL), 2016). Incidence of type 2 diabetes is related with overweight and obesity, which are major health problems worldwide, increasing also the risk of other chronic diseases such as coronary heart disease and ischemic stroke (Anderson et al., 2003; World Health Organization (WHO), 2018). Healthy eating decreases the risk of type 2 diabetes, and eating regulation is one of the main targets in diabetes care in order to reach glycemic control and to avoid diabetes-related complications (American Diabetes Association, 2014).
Despite many technical breakthroughs in health care, human behavior remains the key factor that determines optimal health outcomes (Ryan et al., 2008). This challenges researchers and health-care personnel to find out effective ways to promote long-term change in patients’ health behavior. Theory-based research is needed in order to recognize behavioral mediators of health outcomes. One important area of focus is patients’ experience and motivation (Ryan et al., 2008).
Eating regulation encompasses, besides weight management, behaviors such as choosing healthful foods (Verstuyf et al., 2012). Patients with diabetes are advised to eat foods rich in fiber such as vegetables, fruits, berries, and wholegrain corn, and low in hard fat, sugar, and salt (Finnish Diabetes Association, 2017). Several studies have shown that the Mediterranean diet is effective in improving glycemic control, weight loss, and good high-density lipoprotein (HDL) cholesterol. The Mediterranean diet is rich in fruits, vegetables, legumes, olive oil, and unrefined cereals, and low in meat and meat products, and, moreover, contains moderate amounts of dairy products (mostly cheese and yogurt), fish, and wine (Ajala et al., 2013; Esposito et al., 2009). Eating healthful food, a regular meal rhythm including breakfast, and avoidance of binge eating has been found to be associated with successful weight maintenance (Elfhag and Rössner, 2005).
Only a minority of patients with type 2 diabetes are likely to be intrinsically motivated to regulate their eating behavior. Intrinsic motivation means that the value of behavior is fully internalized, and motivation to perform the behavior is fully autonomous (self-determined). Intrinsically motivated individuals find healthy eating challenging and interesting, and regulate their eating behaviors because they take pleasure in fixing healthy meals (Pelletier et al., 2004; Ryan and Deci, 2000).
If the initiative for eating regulation comes from the health-care personnel, motivation for change comes outside of self and is not self-determined. Changing eating habits often involves physical and/or psychological discomfort and, thus, in many cases, is not inherently interesting or pleasurable (Verstuyf et al., 2012). Studies have shown that long-term change in eating behavior and maintenance of weight loss is difficult (Madden et al., 2008). However, the value of healthy eating should be internalized because without internalization, permanent behavior change is unlikely to happen (Ryan et al., 2008).
According to self-determination theory (SDT), individuals can be placed on a motivational continuum ranging from amotivation to intrinsic motivation. That is, motivation can vary from amotivation, or unwillingness, to passive compliance, and to active personal commitment (Ryan and Deci, 2000). Amotivated individuals find no interest or motivation to change their eating behavior. Externally regulated individuals are motivated to regulate their eating behavior in order to get rewards (e.g. positive comments) or avoid negative consequences (e.g. criticism). Individuals with introjected regulation feel ashamed or guilty if they eat unhealthy (Pelletier et al., 2004; Ryan et al., 2008). In identified regulation, motivation is based on persons’ belief that eating regulation is good for their health and well-being. In integrated regulation, the value of healthy eating is internalized even more strongly as one important value among other central values in the person’s life. In controlled motivation (external and introjected motivations), the predominant feeling is pressure, often associated with ambivalence, whereas feeling of willingness is more present in more autonomous forms of motivations (identified, integrated, and intrinsic motivations) (Ryan and Deci, 2000; Silva et al., 2014). Therefore, autonomous forms of motivations are more likely to lead to maintenance of change in eating behavior (Ryan et al., 2008).
Are health-care personnel able to promote internalization of the value of healthy eating habits? According to SDT, this is possible if the health-care climate is autonomy-supportive, that is, interaction with health-care personnel satisfies patients’ needs for autonomy (self-determination), competence (effectance), and relatedness (belonging). These three needs are seen to be basic psychological needs universal to all human beings (Ryan and Deci, 2000). Satisfaction of these needs is essential for psychological growth, integrity, and well-being. Feelings of being self-determined, competent, and related to others give sufficient energy to make and maintain the change in lifestyle (Silva et al., 2014; Williams et al., 2004). The SDT model assumes that an autonomy-supportive health-care climate increases patients’ perceived competence and autonomous regulation of behavior leading to maintained behavior change (Silva et al., 2008).
Health-care personnel can support patients’ sense of autonomy and autonomous motivation if they give meaningful rationale for health behavior change, listen to patients’ opinions, consider different options with them, and avoid an authoritarian and guilt-inducing attitude. Competence is best supported by collaborative goal-setting, considering optimal challenges and by giving practical guidance and informative non-judgmental feedback. Sense of relatedness is supported by showing genuine concern, respect, and empathy and by being available in case of need (Ryan et al., 2008; Silva et al., 2014).
Pelletier et al. (2004) found that women with a self-determined regulatory style were more successful in regulating their eating behaviors and more concerned by the quality, instead of quantity, of foods they ate, compared with women who reported a non-self-determined regulatory style. The intervention study by Williams et al. (1996) showed that autonomously motivated participants attended the dieting program more regularly and were more successful in losing weight and maintaining their weight loss at the 23-month follow-up. In addition, autonomy supportiveness of the health-care staff predicted participants’ autonomous motivation for weight loss. The studies by Silva et al. (2010) and Koponen et al. (2018b) showed similar results. Interventions that emphasize a person-centered and autonomy-supportive communication style have been proven to be successful in long-term maintenance of change in eating habits (Samdal et al., 2017). An autonomy-supportive health-care climate has been shown to be associated also with patients’ self-management behavior regarding medical adherence (Williams et al., 1998, 2009) and physical activity (Fortier et al., 2007).
Besides autonomy-supportive health-care climate, autonomous motivation, and self-care competence, many other life-context factors, such as depression and socioeconomic status, may also decrease or increase success in eating regulation. However, in studies based on SDT, the effects of these other factors have been widely overlooked. The prevalence of depressive symptoms has been shown to be higher in patients with type 2 diabetes than in the general population (Ali et al., 2006; Anderson et al., 2001; Nouwen et al., 2010), and an association between depressive symptoms and poor self-management of diabetes has been found in many studies (Ali et al., 2006; De Groot et al., 2001; Dirmaier et al., 2010; Egede and Ellis, 2010; Gonzalez et al., 2007). Low socioeconomic status predicts poor dietary habits (Laaksonen et al., 2007), whereas a strong sense of coherence may enhance competence to cope with chronic illness (Antonovsky, 1987). Significant others in the person’s social context may also enhance success in eating regulation if they are autonomy-supportive (Williams et al., 1998).
This study investigated (a) whether perceived autonomy support (from a physician), autonomous motivation, and self-care competence were associated with fruits, vegetables, and berries intake (FVBI) among patients with type 2 diabetes when the effects of other important life-context factors (perceived health, medication, duration of diabetes, mental health, stress, and social support) were controlled for and (b) whether autonomous motivation and self-care competence mediated the effect of perceived autonomy support on FVBI.
We hypothesized that (a) the positive association between perceived autonomy support, autonomous motivation, self-care competence, and FVBI remains even after the effect of the other important life-context factors is controlled for and (b) autonomous motivation and self-care competence mediate the effect of perceived autonomy support on FVBI.
Methods
Data collection
The respondents were first identified from the register of the Social Insurance Institution of Finland (Kela) in 2011. This Finnish government agency keeps the register of all persons who have entitlement to a special reimbursement for medicines because of chronic diseases such as diabetes. To be included in this study, the persons had to fulfill the following inclusion criteria:
(a) Had entitlement to a special reimbursement for medicines used in the treatment of type 2 diabetes (International Classification of Diseases, 10th revision (ICD-10) code, E11) in 2000–2010, and the right was valid in September 2011 and onward;
(b) Born between 1936 and 1991 (aged 20–75 years), alive, and had no safety prohibition at the time of the data collection;
(c) Finnish as native language;
(d) One of the five study municipalities as place of residence.
A total of 7575 persons have fulfilled the inclusion criteria. Based on power analysis, a sample of 5167 persons was collected: 2000 persons from each of the two large municipalities and all persons (i.e. 1167) from the three small municipalities. There were 2962 (57%) men and 2205 women (43%) in the sample, corresponding to the rate of sex in the total population of patients with type 2 diabetes in the study municipalities.
The first version of the questionnaire was tested by a pilot study (n = 50) in May 2011, and the final revised version was mailed to respondents in September 2011. Two reminders to non-respondents were sent out: the first one in October, and the second one with a new copy of the questionnaire in November. The final response rate was 56 percent (range = 54%–59% across municipalities, n = 2866). The response rate was associated with sex and age: women responded slightly more often (57%) than men (54%), and the response rate was highest (63%) in the oldest age group (65–75 years), lower (55%) in the age group of 55–64 years, and lowest (36%) in the age group of 20–54 years.
Ethical considerations
The research plan was accepted by the Ethical Committee of the Hjelt Institute, University of Helsinki, and the permission to conduct the study was received from Kela. The sample was collected by the qualified statistician who worked at Kela, and the questionnaires with an information letter were posted from Kela. The information letter emphasized that participating in this mail survey was voluntary. The respondents gave their consent to participate by the act of returning the questionnaire. Respondents filled questionnaires and returned them directly to the researchers by mail. Each questionnaire was provided with an identification number which was needed in order to check for non-response. Identity of respondents was not revealed to the researchers at any stage of the sample or data collection, and only the researchers saw the content of the questionnaires.
Respondents
The mean age of respondents was 63 (standard deviation (SD) = 8, range = 27–75) years, and 56 percent of them were men. Over half (56%) of the respondents were retired because of old age, 60 percent were married, and 60 percent had less than higher professional education. The majority (83%) of the respondents had a municipal primary-care health center as their primary-care place in diabetes care, and 74 percent used oral medication only for diabetes therapy (Table 1).
Sociodemographic background factors of respondents.

GLP-1: glucagon-like peptide-1.
Numbers are based on survey responses. Data are missing due to non-response.
Measures
In this study, FVBI was the sum of intake of fruits, fresh vegetables, cooked vegetables, and berries during the last week (7 days). All measures used in the study are presented in Table 2. Cronbach’s alphas of the measures chosen for the final analyses varied from .75 to .95 and can be regarded acceptable (>.70) or excellent (>.80) (Andresen, 2000).
Measures used in the study.

Averaged sum scales for perceived autonomy support, autonomous motivation, self-care competence, energy, emotional well-being, sense of coherence, life stress, social support in diabetes, and FVBI were calculated. The respondent was included in the analysis if she or he had answered at least to 70 percent of the items in the different scales. For example, on the six-item Health Care Climate Questionnaire (measuring perceived autonomy support), the respondent had to answer at least to four items, and the missing values were replaced with the mean counted from the existing values on that scale.
Statistical procedures
Descriptive statistics were estimated and the baseline associations between independent variables, covariates, and dependent variables were tested with Pearson’s chi-square tests, t-tests, or one-way analysis of variance depending on the measurement scale of the variable of interest. In the final analyses, multivariate linear regression analysis was used. The correlations between study variables were explored before further analyses by Pearson’s correlations. The level of statistical significance was set at p < .05. The variables to the regression models were chosen on theoretical and statistical basis. Of the independent variables that measured the same phenomena, such as mental health (energy, emotional well-being, diagnosed depression, and a sense of coherence), only the one that correlated most strongly with FVBI was chosen to the final linear regression analyses in order to avoid multicollinearity problems.
The averaged sum-scale measuring FVBI was normally distributed. The distribution of autonomy support, autonomous motivation, self-care competence, energy, emotional well-being, sense of coherence, and social support scales was skewed to the right, and the distribution of the life stress scale was skewed to the left but without influence on the analysis. Statistical requirements for normal distribution, linearity, and homoscedasticity of regression residuals were fulfilled. List-wise deletion of missing data was used.
In the mediation analyses between perceived autonomy support, autonomous motivation, self-care competence, and FVBI, the instructions reported by Baron and Kenny (1986) were followed. First, the mediator was regressed on the independent variable. Second, the dependent variable was regressed on the independent variable. Third, the dependent variable was regressed on both the independent variable and the mediator. A mediation exists if the predicted associations hold on each step of the analysis and if the effect of the independent variable on the dependent variable is less in the third step than in the second step. The mediation is perfect if the independent variable has no effect when the mediator is controlled. Statistical significance of the mediation was calculated by the Sobel test (Preacher and Leonardelli, 2001). SPSS version 23 was used.
Results
Preliminary analysis
A majority of the respondents (74%) assessed that they had received enough knowledge, advice, and guidance from their principal primary-care health center regarding healthy foods and a suitable diet for them, and a special diet had been recommended to 61 percent of the respondents. Over one-third (37%) reported that it was often or almost always difficult to follow the diet, and almost the same amount (36%) had not followed the recommended diet on a single day during the last week.
During the last week, 53 percent of the respondents had eaten fruits, 45 percent fresh vegetables, 23 percent berries, and 20 percent cooked vegetables at least once a day. FVBI was associated with obesity: 53 percent of those with smallest intake (the third with smallest intake) were obese compared with 44 percent with largest intake (the third with largest intake) (p < .001). Corresponding percentages regarding poor glycemic control (⩾7%) were 70 and 63 percent (p < .01) and regarding high blood pressure (⩾140/90) 45 and 32 percent (p < .001).
The four variables measuring mental health or positive personality orientation (energy, emotional well-being, diagnosed depression, and sense of coherence) correlated moderately or strongly with each other (–.38 to .78). Only the correlation between a sense of coherence and depression was quite weak (–.33). Correlations between the four variables and FVBI were weak. Of these four variables, a sense of coherence correlated most strongly with FVBI (.18, p < .001), whereas Pearson’s correlations between energy, emotional well-being and diagnosed depression, and FVBI were .14 (p < .001), .14 (p < .001), and –.04 (p < .05), respectively. Therefore, a sense of coherence was included as an independent variable to the multivariate linear regression analyses.
The three variables measuring physical health (perceived health, and the number of chronic diseases and diabetes complications) correlated with each other but quite weakly. Of these three variables, perceived health correlated most strongly with FVBI (–.12, p < .001), whereas Pearson’s correlations between the number of chronic diseases and diabetes complications and FVBI were .04 (p > .05) and –.06 (p < .01), respectively. Therefore, perceived health was included as an independent variable to the multivariate linear regression analyses.
Primary analyses
Table 3 shows that autonomous motivation and gender correlated most strongly with FVBI but the correlations were quite modest. In addition, social support, a sense of coherence, and self-care competence correlated positively with FVBI. The positive associations of female gender, autonomous motivation, social support, and a sense of coherence with FVBI remained even after the effects of other central life-context factors were controlled for. Other predictors of FVBI were high education and high age (Table 4). Autonomous motivation mediated the effect of autonomy support from a physician on self-care competence, which further mediated the effect of autonomous motivation on FVBI (Table 5).
Correlation matrix between study variables.

FVBI: fruits, vegetables, and berries intake.
p < .05; **p < .01; ***p < .001.
Multivariate linear regression models on the association of perceived autonomy support, autonomous motivation, self-care competence, and other important life-context factors with fruits, vegetables, and berries intake (FVBI).

ns.p > .05; * p < .05; ***p < .001.
Mediation analysis between perceived autonomy support from a physician, autonomous motivation, self-care competence, and fruits, vegetables, and berries intake (FVBI).
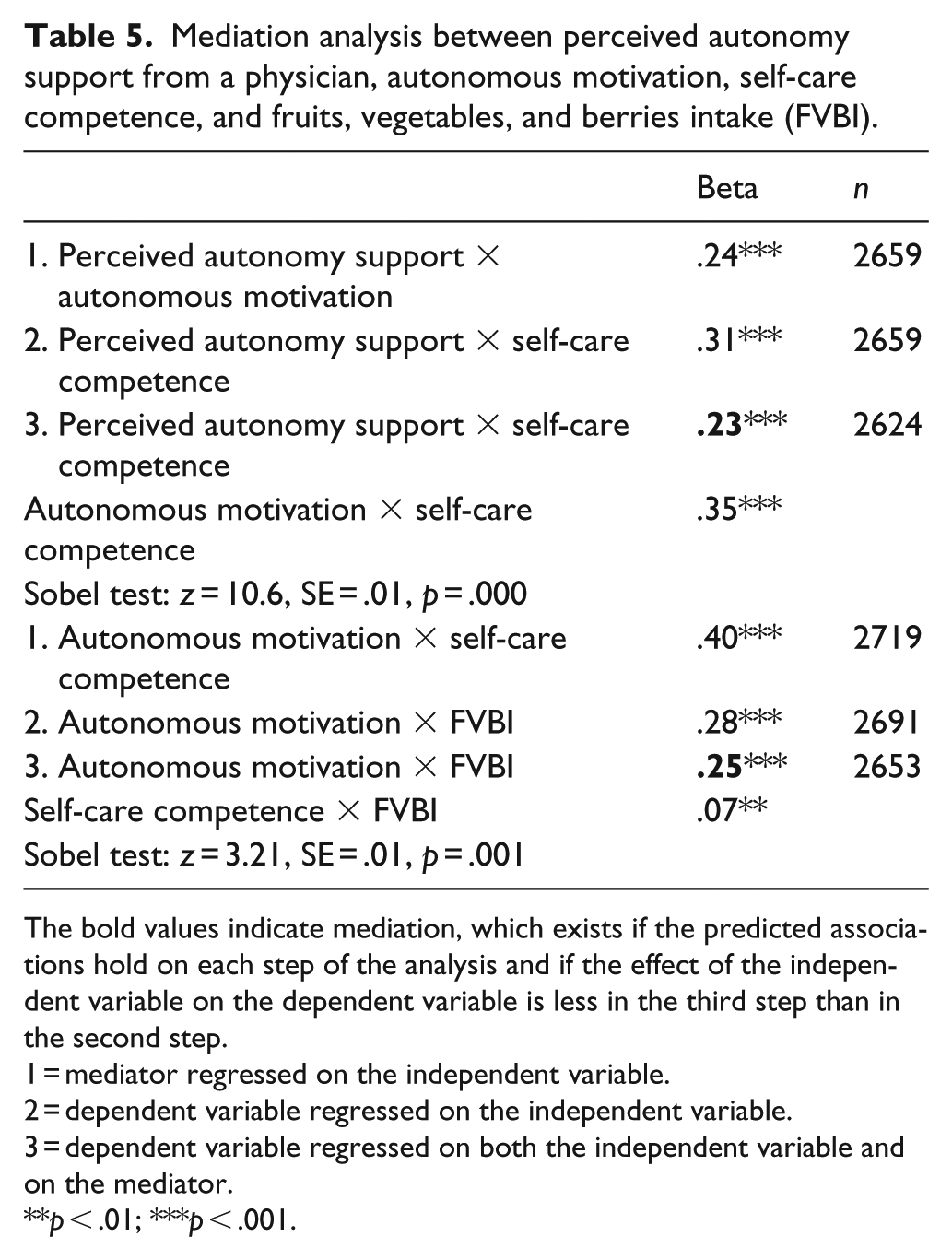
The bold values indicate mediation, which exists if the predicted associations hold on each step of the analysis and if the effect of the independent variable on the dependent variable is less in the third step than in the second step.
1 = mediator regressed on the independent variable.
2 = dependent variable regressed on the independent variable.
3 = dependent variable regressed on both the independent variable and on the mediator.
p < .01; ***p < .001.
Discussion
This study investigated intake of fruits, vegetables, and berries among patients with type 2 diabetes and factors associated with it. The results showed that most of the respondents had received enough information, advice, and guidance on healthy eating in primary care. However, many found it difficult to follow the recommended diet, and all had not eaten fruits, vegetables, or berries every day. High FVBI was associated with less weight, better glycemic control, and lower blood pressure.
Female gender and autonomous motivation were the strongest determinants of FVBI. Also, higher education, social support, higher age, and a sense of coherence were positively associated with FVBI. Autonomy support from a physician was not directly associated with FVBI but through autonomous motivation and self-care competence as could be hypothesized based on SDT process model (Williams et al., 1998).
Previous studies similarly showed that autonomous motivation was the strongest predictor of health behavior among the variables studied in that context: physical activity, success in increasing physical activity, and success in weight management (Koponen et al., 2017, 2018a, 2018b). Autonomous motivation was more strongly associated with FVBI than self-care competence. This result is somewhat inconsistent with the results from other studies that stress the importance of self-efficacy for fruits and vegetable intake (Shaikh et al., 2008). In our study, self-care competence had a mediating role between autonomous motivation and FVBI.
Socioeconomic differences in FVBI have been found also in other studies (Baker and Wardle, 2003; Graham et al., 2018). One possible explanation for these differences is economic insecurity, which in lower socioeconomic positions may limit possibilities to choose healthy foods (Graham et al., 2018). The results of sex differences are in line with earlier studies revealing lower FVBI among men in general (De Irala-Estevez et al., 2000) and as a means to achieve weight control (Mulgrew et al., 2019). The important role of social support on FVBI has also been recognized (Anderson et al., 2003). Different health behaviors may have different predictors. In earlier studies (Koponen et al., 2017, 2018a), it was found that social support was negatively associated with physical activity. Those who need and get more social support in their diabetes care might be the ones who have worse health, and as poor health hinders physical activity, this could explain the negative association between social support and physical activity. Eating, however, possibly occurs more often in a family or work-related setting (Mata et al., 2011) and, thus, social support may be more important for choosing healthy food than for physical activity.
Of the four variables measuring mental health or positive personality orientation (energy, emotional well-being, diagnosed depression, and a sense of coherence), a sense of coherence was most strongly associated with FVBI. This result is in line with the results by Wainwright et al. (2007). However, our earlier studies showed that perceived energy was a better predictor of health behavior regarding physical activity, success in increasing physical activity, and success in weight management than a sense of coherence (Koponen et al., 2017, 2018a, 2018b). Perhaps, it takes more energy to increase one’s physical activity than to change one’s eating habits. Also, physical activity may in turn increase feelings of energy.
Many studies have found higher prevalence of depression among patients with diabetes compared with the whole population and an association between depression and poor self-care (Ali et al., 2006; Anderson et al., 2001; Nouwen et al., 2010). In our data, the prevalence of depression was also higher (22%) than in the whole population (5%) (Koponen et al., 2015; Pirkola et al., 2005). However, of the four affective variables, diagnosed depression was most weakly and a sense of coherence most strongly associated with FVBI. This result supports the view of Fisher et al. (2010) that minor affective variables are better predictors of self-care than a diagnosed major depressive disorder and is in line with results from our previous studies (Koponen et al., 2015, 2017, 2018a, 2018b).
Strengths and limitations of the study
One limitation of surveys is the fact that results are based on self-reports of respondents, and objective measurements to confirm these results are seldom available. In this study, we were able to evaluate the reliability of the results by comparing basic information (diagnosis age, duration of diabetes, medication, HbA1c-values, and body mass index (BMI)), reported by the patients, with register data from the whole country (Valle ja työryhmä, 2010) and with the electronic medical records from the municipal primary-care health centers in the study municipalities (Koponen et al., 2013a, 2013b). This comparison showed that percentiles, means, and medians of the mentioned variables, as reported by the patients in our survey, corresponded well with data from the other sources (Koponen et al., 2013a, 2013b; Valle ja työryhmä, 2010).
The cross-sectional data limit the possibility to make conclusions about directionality of the hypothesized relations. However, it is reasonable to believe that care provided by the primary-care health center had influenced patients’ motivation for FVBI. Almost all respondents (95%) had been at least 1 year and 84 percent over 2 years in care in their current and principal primary-care health center, and 75 percent had a family doctor or a “regular” doctor.
The large sample size, high response rate, high internal consistencies of the measures, and the possibility to control the effect of many important confounding factors were the strengths of this study. Previous studies based on SDT have largely overlooked these confounding factors. Future studies should consider also the role of additional factors in food choice and weight management, such as feelings of fatness and other body image variables (Mulgrew et al., 2019), and factors that help to overcome barriers between an intention to act and adoption of the planned behavior (Vézina-Im et al., 2019).
Conclusion
This study gave additional support for SDT by showing the central role of autonomous motivation for FVBI. Also, the effect of autonomy support from a physician on FVBI was mediated by autonomous motivation and self-care competence as could be predicted by the SDT process model. The results indicate that physicians can promote patients’ FVBI by focusing especially on supporting their autonomous motivation and self-care competence.
Footnotes
Acknowledgements
The authors thank the participants in this study for their cooperation and Ritva Laamanen (PhD) for participating in planning the research project.
Authors’ contributions
AMK, NS, and SS participated in planning the study. AMK formulated the initial hypotheses and conducted the statistical analyses. AMK and NS interpreted the results. AMK wrote the first draft of the manuscript and all the later versions. NS and SS reviewed and revised the manuscript. All the authors approved the final manuscript for submission to the journal.
Availability of data and materials
A license for collecting the data through Kela was granted for the present study. The data are not publicly available but a license can be requested from the data providers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The research plan was accepted by the Ethical Committee of the Hjelt Institute, University of Helsinki, and the permission to conduct the study was received from Kela. The respondents gave their consent to participate by the act of returning the questionnaire.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Insurance Institution of Finland, Samfundet Folkhälsan i Svenska Finland, and the Finnish Cultural Foundation, Varsinais-Suomi Regional Fund.