
Abstract
Spiritual approaches in healthcare settings proved effective in reducing the negative outcomes of dehumanization processes impacting health professionals and patients. Although previous literature focused on explicit measures of spirituality, the present research explored the role of implicit components of spirituality and their effects on the humanization of patients in two healthcare contexts. Professionals from hospices and nursing homes completed an implicit task to assess whether the diverse representation of death as physical or spiritual led to perceive patients with more uniquely human traits. Results showed that only for hospice participants, implicit and explicit spirituality predicts more humanness attribution to patients. This article discusses palliative care models and death education as a resource for reducing dehumanization.
Introduction
Nowadays, the person-centered approach (Omi, 2007), as opposed to the illness-centered one, assumes in contexts of care a bio-psycho-socio-spiritual perspective (Sulmasy, 2002); this frame considers spiritual and religious outcomes as highly relevant when coping with suffering and pain. Indeed, many studies have widely confirmed such a positive effect of spirituality on the ability to deal with stress and, furthermore, that believers report higher levels of life satisfaction (Ano and Vasconcelles, 2005; Galea, 2014). The idea of significant relationships between these dimensions, personal growth, and well-being is widely endorsed (Meador, 2004; Pargament et al., 2004) and religious beliefs appear to be particularly useful in response to life’s challenges, especially when individuals have to cope with life stressors and severe pathologies (Oman and Thoresen, 2005; Pargament et al., 2004; Testoni et al., 2016a). In the wake of these studies, some scholars inquired how nurses and healthcare professionals might have an active role in caring for the spiritual needs of patients (Balboni et al., 2009); although this factor assumes the crucial role of support at the end of life (Edwards et al., 2010; Meador, 2004; Phelps et al., 2009; Puchalski et al., 2009). Embracing a spiritual care approach implies, on one hand, being empathic, caring, and supportive to the patients while, on the other, recognizing and respecting their spiritual needs through the active listening and discussing of the religious and transcendental issue (Baldacchino, 2005; Edwards et al., 2010; Pargament, 2007). Especially, to manage this dimension, Dania Baldacchino (2005) suggests that “the essence of spiritual care is being in doing whereby personal spirituality and therapeutic use of self-contribute towards effective holistic care” (p. 594). However, these relevant factors might be underestimated due to the lack of training on these issues and the lack of time for addressing spiritual needs while being in care (Testoni et al., 2016a).
Taking into consideration the effects of these inadequacies, which might inhibit professionals from providing ameliorative holistic nursing, we decided to analyze how the fundamental concept of “soul” that pivots spirituality intervenes in the humanization of patients’ care. Specifically, we explored how the idea of “soul” and its implicit assumptions and representations (Solomon et al., 2017) might be related to the dehumanization of patients. Indeed, the soul in traditional Western culture has been considered as the essential and main human characteristic, which differentiates human beings from any other kind of being (Solomon et al., 2017; Testoni et al., 2017a).
Implicit beliefs consist of mental associations and evaluations, between an object and its attributes, which might be activated in response to external or internal stimuli. Derived from early or recent socialization experiences (Rudman et al., 2007) or from verbal descriptions of the target (Gawronski et al., 2005), they affect thoughts and behaviors at an automatic level. Some implicit associations might be available without the acknowledgment of an individual, even if they are in open disagreement with that specific association (Goff et al., 2008). Therefore, even people explicitly convinced that a spiritual dimension or a soul exists might implicitly associate the idea of an afterlife with concepts indicating that this content has no substantial (ontological) consistency, implying it is a mere myth. Since in post-modern society, this seems to be the more common representation, it could be useful to study this possible non-deliberative contradiction. Previous research has shown that implicit cognition does affect not only automatic responses but also deliberate behaviors, even in healthcare contexts (Testoni, 2016a). Therefore, inquiring these processes might be relevant for analyzing the possible cognitive dissonances in the spiritual aspects of care (Testoni et al., 2017c, 2016b; Trifiletti et al., 2014) and their impact on other dimensions of care.
Research on dehumanization processes has changed our understanding of interpersonal and intergroup relationships (Capozza et al., 2016, 2013; Haque and Waytz, 2012; Haslam, 2006); it also proved that perceiving a patient as a complete human being is one of the many obstacles faced by health professional in order to maintain a positive quality of care (Haque and Waytz, 2012). Dehumanization in healthcare contexts has structural causes (Haque and Waytz, 2012) embedded in the know-how of medical procedures, and these processes can produce both functional and non-functional outcomes (Haque and Waytz, 2012), which might increase the risks of psychological and physical distress for both healthcare professionals and patients (LaBouff et al., 2010). How professional approaches to spiritual beliefs and personal representations of death might, in our opinion, influence its humanness attribution (HA) to patients and colleagues (Testoni et al., 2016a, 2017c; Trifiletti et al., 2014).
To test whether the implicit representations of the soul might affect the infra-humanization processes (e.g. perceiving patients as not fully human) in the hospitalized contexts (Trifiletti et al., 2014), we recruited a sample of workers from hospice and nursing homes in Italy. These two groups of professionals were chosen as comparable samples since they share a strong saliency of their guests’ death as incoming or inevitable, although they follow different care models and strategies. Also, most participants reported a Catholic background. Therefore, we expected their representations of the afterlife, God, and dying to be consistent with Christian beliefs. Finally, the present research discusses the introduction of specific spiritual curricula and death education courses as a possible solution for professionals working in the end-of-life field (Baldacchino, 2005; Edwards et al., 2010; Testoni et al.,2016a, 2017c) and in nursing homes (Carpenter et al., 2010; Ersek and Wilson, 2003).
Methods
Aim and objectives
Following previous literature (Galea, 2014), we predicted that being spiritual—both at implicit and explicit levels—might play a decisive role in perceiving patients as more human. The cognitive task Go/no-Go Association Task (GNAT; Nosek and Banaji, 2001) explored four different implicit representations of the transcendental domain, obtained through the combination of two target categories (“Existence” and “Nothingness”) with two attribute categories (“Physical” and “Soul”). We expected that those who had a stronger implicit representation of our mortal existence or its opposite as permeated with a soul might use more Uniquely Human Traits (Capozza et al., 2016, 2013) to describe patients and guests compared to other types of non-spiritual implicit representations (e.g. “Existence” or “Nothingness” as “Physical”). Moreover, we expected that the explicit spirituality of participants might positively affect the attribution of humanness to patients and colleague, whereas conceptualizing death as annihilation (Testoni et al., 2015) could inhibit representing others as fully human beings (Capozza et al., 2016, 2013).
Developing a cognitive task
To develop the GNAT (Nosek and Banaji, 2001) for the implicit representation of the soul, we required reliable word stimuli for the cognitive task. A pre-test was conducted recruiting 79 participants through random sampling and snowballing in Padova. In all, 43 women and 36 men, age ranging from 18 to 63 (M = 37.3; standard deviation (SD) = 13.63) years, completed a pen and paper questionnaire in which they rated a total of 48 words, 12 for each concept, as representative of the respective category (Existence, Nothingness, Soul, Physical) using a 7-point Likert-type scale (from 1 = “not at all” to 7 = “totally”). Participants were also asked to evaluate whether these words had a positive or negative valence on a 7-point Likert-type scale (from 1 = “totally negative” to 7 = “totally positive”) and provided demographical information, religious identity, and belief in God. Participants signed ethical consent and received a full debriefing. Through reliability analysis, five words for each category, the following stimuli were chosen as representative of the four categories:
Existence: identity, thinking, birth, being, willpower.
Nothingness: void, absence, loss, abyss, end.
Physical: body, flesh, material, physical, waste.
Soul: aura, spirit, essence, afterlife, light.
Procedure
The lab sessions were conducted in a quiet room inside a facility of each health institution. Participants were seated in front of a computer, were informed by the experimenter, and signed the first consent without revealing the real aims of the study. Afterward, participants completed a cognitive task GNAT (Nosek and Banaji, 2001) using a PC and a questionnaire, the task was developed using OpenSesame (Mathôt et al., 2012). At the end of each lab session, which lasted on average of 30 minutes, the experimenter provided a full debriefing and a second consent form to sign. Data collection started in January 2016 and lasted until December 2016.
Measures
GNAT
The GNAT (Nosek and Banaji, 2001) is a cognitive task that measures the strength of associations in memory between two target categories (e.g. Existence and Nothingness) and two attribute categories (e.g. Soul and Physical) using the errors and reaction times as an index of accuracy. The task consisted of eight blocks of trials, four practice blocks (one for every single category), and four experimental blocks (consisting of the combinations of target attribute category). During each block, a single word from one of the four categories appeared for 1000 ms at the center of the screen. If one word belonged to the current block category, the participant had to press the space key as fast as possible (defined as a “signal” trial). But, a participant had to restrain itself from pressing the space key if one word was from a different category (defined as a “noise” trial). The sensitivity index d′ (Nosek and Banaji, 2001; Stanislaw and Todorov, 1999) represents the strength of the association, and it is calculated from the ratio of Hit (correct signal trials) and False Alarms (errors during noise trials) for each block category. Higher values of d′ can be interpreted as a preference for the target and attribute combination (e.g. those who conceive the afterlife as connected to a spiritual realm will be more accurate and fast in associating the words representing the Nothingness category with those of the Soul category). Figure 1 shows an example procedure for the GNAT (Nosek and Banaji, 2001).

An example procedure for the Go/no-Go Association Task employed in the research and word stimuli for each category.
Nothingness-soul
As one of the four GNAT (Nosek and Banaji, 2001) blocks, it measures the association between the target category “Nothingness” and the attribute category “Soul.” Higher scores in this implicit religious measure can be interpreted as a preference to associate concepts related to death/afterlife with the transcendental idea of a soul.
HA
The questionnaire included two versions of this 8-item scale: the first one referring to patients and the other colleagues of their institution. Participants were asked to rate on a 5-point scale (from 1 = “does not describe at all” to 5 = “describes a lot”) to what extent these two groups can be described using Uniquely Human Traits (e.g. reasoning, rationality, morality, intellective abilities), hence as fully human, or with Non-Uniquely Human Traits (e.g. instinct, drive, impulsiveness, impetus), more dehumanizing since they are shared with animals (Capozza et al., 2016, 2013; Trifiletti et al., 2014).
Spirituality
Developed from the “Spiritual Orientation Inventory” (Elkins et al., 1988), this 8-item scale measured the extent to which participants believed in a spiritual and transcendental dimension not necessarily related to religious organizations. Participants rated their agreement on a 5-point scale (from 1 = “totally disagree” to 5 = “totally agree”).
Testoni Death Representation Scale
The Testoni Death Representation Scale (TDRS) consists of 6 items rated on a 5-point scale (from 1 = “totally disagree” to 5 = “totally agree”) and explores the participant’s representation of death on a continuum from passage to annihilation (Testoni et al., 2015). High scores in this scale indicate a preference for viewing death as annihilation, whereas low scores indicate a tendency to see death as a passage toward an afterlife.
Quest religious orientation (QUEST)
A 7-item scale was constructed using the religious orientation QUEST Scale (Batson and Schoenrade, 1991), which measures the degree to which a person lives its religion as a quest for answering existential dilemmas while following a critical approach to religious issues (Cronbach’s α = .81). Participants rated their agreement on a 5-point scale (from 1 = “totally disagree” to 5 = “totally agree”).
Social desirability
To measure the self-serving distortions that might lead a participant to provide a positive and unrealistic view of themselves, eight items were taken from the “How I think questionnaire” (Nas et al., 2008). Participants rated their agreement on a 5-point scale (from 1 = “totally disagree” to 5 = “totally agree”).
Preliminary analyses and theoretical model
Scores from the GNAT (Nosek and Banaji, 2001) were obtained using a Signal Detection Theory approach (Nosek and Banaji, 2001; Stanislaw and Todorov, 1999) and d′ indexes calculated for each block using SPSS 24. During the data analysis, we excluded 13 participants for incomplete data in the questionnaire or for having too many errors in the GNAT task. We employed the procedure suggested by Williams and Kaufmann (2012) to compute the reliability for the GNAT using a Random Sample of Split Halves. The mean of the RaSSH distribution of random split-half correlations for the Nothingness-Soul block was M = .82 (SD = .93), which is generally considered a good reliability (Williams and Kaufmann, 2012); also, the d′ of the first and second halves of the GNAT did not differ, like those of the odd and even halves (Williams and Kaufmann, 2012).
Since spiritual beliefs, concerning human existence or a transcendental afterlife, might reduce dehumanization processes, we expected that a spiritual approach could lead to more humanization. Our central hypothesis was that the implicit and explicit measures of spirituality could affect or predict the scores of the HA of Patients for both healthcare groups. The theoretical model also included work experience and demographic variables (age, gender, and education) of participants as possible predictors of Spirituality and HA of Patients. All demographics are shown in Table 1.
Demographics for the two healthcare groups and the whole sample.
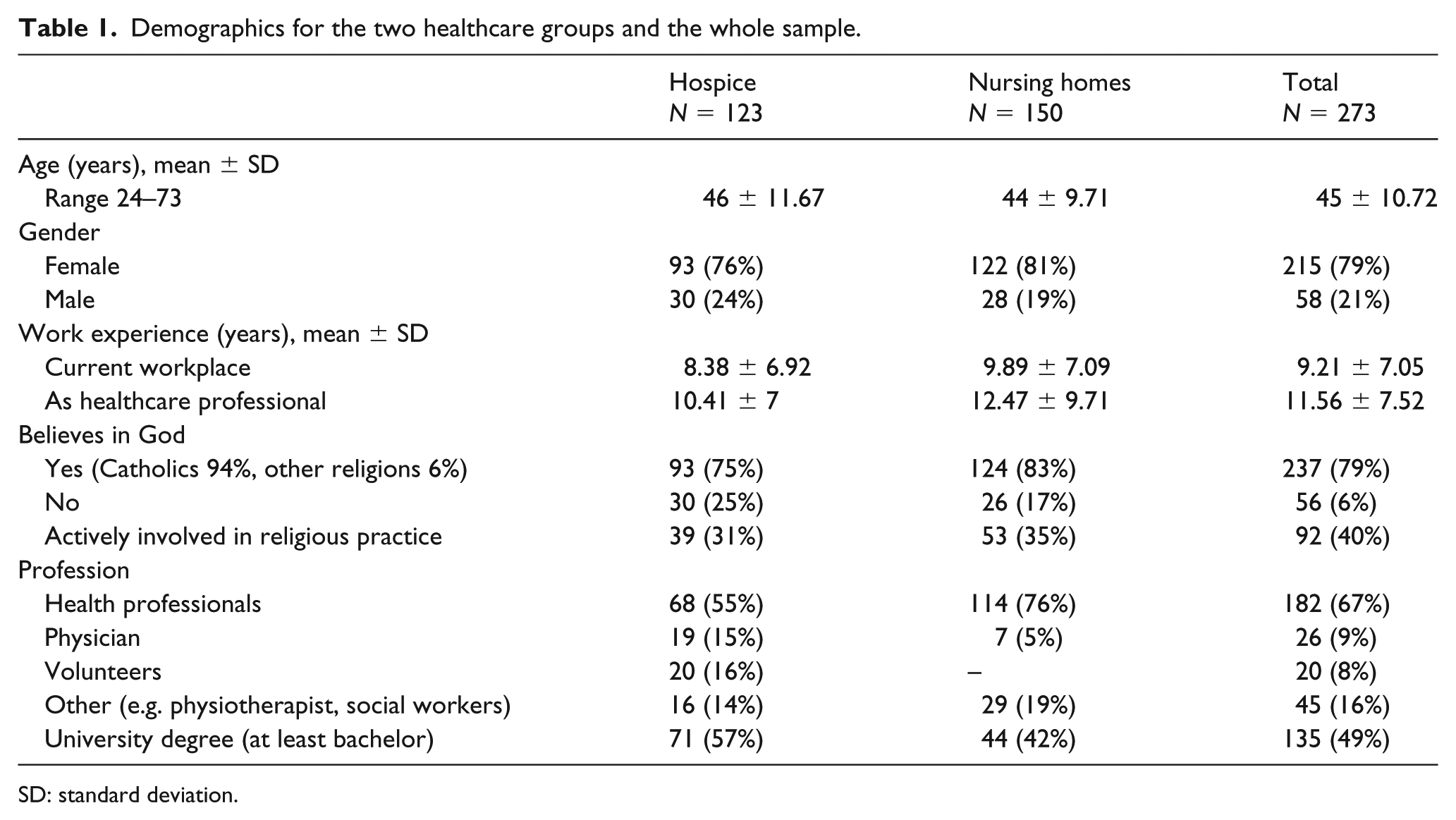
SD: standard deviation.
Results
Group differences
An independent sample t-test compared the average means for each healthcare group (hospice and nursing homes), including the implicit block Nothingness-Soul and the explicit variables from the questionnaire as shown in Table 2. Regarding the HA of patients, results showed that participants of the hospice group achieved higher scores in the HA to patients scale and, hence, used more Uniquely Human Traits (Capozza et al., 2016, 2013) to describe patients compared to the Nursing Homes participants. The effect size is moderately strong (Cohen’s d = .40), and we can interpret these results as a relevant difference between these groups, those who work in hospice tend to describe those around them at work as more human. Also, a considerable group difference emerged from the religious orientation QUEST Scale (Batson and Schoenrade, 1991). The higher scores obtained by the hospice professionals might indicate a more open and critical approach to religious matters. Also, the two groups differ by age and work experience in the field of healthcare. As shown in Table 2, the nursing home participants were on average younger and more experienced in their field compared to the hospice workers. Table 3 shows the means and correlation analyses divided by groups.
Reliability t-tests, means, and standard deviations of hospice and nursing homes participants.

Means, standard deviations, and correlations between variables for the hospice and nursing home participants.

p < .05, **p < .01.
Path-analysis
Several path analyses, divided by group, were conducted to identify predictors and mediators of HA to patients (Capozza et al., 2016, 2013) using a Robust Maximum Likelihood Method with LISREL 8.80. The initial model include Attribution of Humanness to Patients as dependent variable, the implicit scores from the Nothingness-Soul block and the Spirituality scale as mediators, and the following sociodemographic variables of participants: age, gender (male gender coded as 1 and female gender coded as 0), work experience (e.g. expressed in years), and degree of education (having a university degree of any level coded as 1 and not having a university degree of any level coded as 0). Only the Nothingness-Soul implicit block was included in the final model since it was the only index, out of the four, that achieved statistical significance when testing different models.
Regarding the Hospice participants, the final model (Figure 2) shows an adequate fit to data using following fit indices: Satorra-Bentler Scaled Chi-Square χ2 (degree of freedom (df) = 9, N = 120) = 7.22, p = .61, root mean square error approximation (RMSEA) = 0, comparative fit index (CFI) = 1. There are four significant path coefficients: the negative direct effects of age and male gender on Spirituality scale and the positive direct effects of Spirituality scale and the Nothingness-Soul block scores on HA to patients. This result implies that for hospice participants both having an explicit spiritual approach in life and implicitly associating the afterlife with concepts of soul positively predicts the HA to patients (Capozza et al., 2016, 2013). Overall, this model explains the 11 percent of the total variance. For the nursing home group, the same model shows an adequate fit to data: χ2 (df = 9, N = 140) = 9.01, p = .44, RMSEA = 0, CFI = 1, but only one significant relationship emerged, degree of education on the Nothingness-Soul block scores. No predictors of HA to patients were found.

The theoretical model of humanness attribution to patients in hospice.
Discussion
This study analyzed the implicit components of spirituality and death representation by measuring the automatic associations between the concepts of Existence and Nothingness with the concept of Soul (vs an exclusively Physical categorization). Using a non-randomized and systematic sample, the research explored how these associations are related to infra-humanization processes in health professionals (e.g. physicians, nurses, social workers, psychologists, and volunteers) employed in hospices and nursing homes.
Main findings
Results showed that associating the idea of Nothingness with the concept of Soul significantly induced more human categorizations of patients in hospice participants. Since those who were more spiritual tend to humanize more, enhancing spiritual skills and employing a spiritual approach can play a significant role in associating patients with Uniquely Human Traits (Capozza et al., 2016, 2013; Trifiletti et al., 2014). In fact, through the path analysis emerged that both implicit and explicit components of spiritual attitudes did affect the humanization of patients, although our model was valid only for the hospice professionals and not for nursing home participants.
Comparing these two groups made clear that different models of care might lead to different attitudes and approaches to the patients (Edwards et al., 2010; Meador, 2004). In our opinion, this difference might stem from the specific training received by hospice workers as end-of-life-care professionals. Since their closeness with the suffering and dying of guests, it is recognized every year, and they follow mandatory training in palliative care and death education. As previous literature highlights, death education is more than just a “better way” to cope with death and mortality, it provides a multidisciplinary approach that develops functional skills, reflexive attitudes, open discourses, and practices to live and work with those who are suffering and dying (Balboni et al., 2009; Baldacchino, 2005; Sulmasy, 2002; Testoni et al., 2016a, 2017b, 2017c).
Considering the positive relationship between the Nothingness-Soul implicit measure and the Spirituality scores, both the explicit and implicit beliefs about spiritual life do affect the degree to which we describe them as human and having Uniquely Human Traits (Capozza et al., 2016, 2013). Furthermore, employing spiritual training and contemplative practices, while following a centered-person approach to healthcare (Omi, 2007), could be an essential step for reducing dehumanization processes in contexts of care, as shown by healthcare facilities implementing palliative care models. As previous research suggests (Ersek and Wilson, 2003), endorsing the practices and principles of the palliative model in nursing homes can enhance the overall quality of care and, therefore, improve the well-being of patients regardless of their health condition (Edwards et al., 2010; Phelps et al., 2009; Puchalski et al., 2009). Finally, since spiritual beliefs are not necessarily related to religious faiths and organizations, healthcare professionals need to be mindful and open to different approaches to the spiritual domain, the sacred and our mortality.
Limitations of the research and further developments
The first limit of this study concerns our sample characteristics regarding gender (men and women) and faith (Catholic believers vs non-believers). Since most of our participants consisted of Catholic women (80%), it was not possible to draw strong assumptions about differences between these groups. The gender gap in career status was another relevant difference in our sample, as physicians were mostly male, whereas most nurses and healthcare operators were females. These disparities hindered the possibility of highlighting specific strategies of humanization by gender, faith, and professional role. Future research will need to recruit more male and non-believer participants of different career status in order to assess whether these factors affect how health professionals cope with terminally ill or dying patients and elderly people.
Future studies should also address how having different morals and strategies to cope with the saliency of death in end-of-life contexts (Testoni et al., 2017b, 2017c) can lead to the same positive outcomes provided by spirituality, a process that has to be further inquired using specific variables for non-believers. Indeed, our findings suggest that non-believers are emphathetic to patients and colleagues, as there were no significant differences between these two groups on the HA scales. Finally, different types of measure (e.g. primary and secondary emotions, evaluation of actual behavior) or variables (e.g. burnout, coping strategies, group identification, and death anxiety) might be inquired in future research to address the different relationships between dehumanization and psychosocial outcomes (Capozza et al., 2016; Goff et al., 2008; Haslam, 2006; Trifiletti et al., 2014).
Conclusion
Exploring the implicit components of spirituality (LaBouff et al., 2010; Testoni et al., 2016b) enhanced our understanding of the relationships between humanization and spirituality in healthcare contexts. Future research might further inquire our implicit spiritual assumptions through future research with different health professionals and patients. Differences in care models do have an impact on the dehumanization process, both at an implicit and explicit level. Employing these approaches, the palliative and person-centered, has the potential to improve the bio-psycho-socio-spiritual (Sulmasy, 2002) well-being of diverse populations, effectively contributing to the well-being of both patients and professionals.
Footnotes
Acknowledgements
We thank the bachelor and master’s degree students who actively engaged the research and helped us with the data collection process across the different health institutions: Sara Bachiorri, Maria Brunello, Marco Lungaro, Michela Mezzaro, and Elena Taboga. Our gratitude also goes to all the health professionals that took part in the research and to the hospice and nursing homes executives for allowing us to conduct it.
Authorship
Aurelio Castro and Ines Testoni designed the research, drafted the paper and revised it. Specifically, Ines Testoni wrote the Introduction and Aurelio Castro the Methods paragraph, the Discussion paragraph must be attributed to both. Lucia Ronconi and Aurelio Castro were in charge of the data analysis and wrote together the third paragraph, Results. Inest Testoni, Adriano Zamperini, Augusto Caraceni, and Padmah Galantin made a contribution to the acquisition of the data, provided major revisions to the paper and approved the version to be published. Research data can be obtained by contacting the main authors, Aurelio Castro and Ines Testoni.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The research presented in this paper received the approval of the Ethical Committee of the University of Padova, School of Psychology (date: 18/03/2016).
Informed consent
Participants were fully informed after the experiments, and written consent was obtained.