
Abstract
This review identified associations between illness perception and health outcomes of patients with a medical diagnosis included in the Hospital Readmissions Reduction Program. Inclusion criteria were English language, use of quantitative methodology, health outcomes specified, and identifiable effect size and statistical significance of the relationship. Most of the 31 studies in this review showed that favorable illness perception has been associated with better health outcomes, while unfavorable illness perception has been associated with worse outcomes. A multifaceted approach might include behavioral, clinical, educational, and psychosocial components to improve one’s illness perception through educative, cognitive-behavioral, or psychodynamic counseling.
Perception of illness is a patient’s cognitive appraisal and personal understanding of a medical condition and its potential consequences (Broadbent et al., 2015). Illness perception focuses on how an individual experiences and mentally frames living with a disease (Weinman and Petrie, 1997). This may include both positive and negative illness beliefs that can influence the ability to cope with the disease and to perceive it as manageable or threatening (Bonsaksen et al., 2015). This review identified and synthesized the literature on the associations between illness perception and the health of patients with any of the six medical diagnoses included in the Hospital Readmissions Reduction Program (HRRP), which requires the Centers for Medicare and Medicaid Services to reduce payments to hospitals with excess readmissions. These diagnoses are heart failure (HF), chronic obstructive pulmonary disease (COPD), myocardial infarction (MI), coronary artery bypass graft (CABG), pneumonia, and total hip and/or knee arthroplasty (THA/TKA).
The study of illness perception emerged from previous research on the Common Sense Model of illness representation (Leventhal et al., 1980), wherein patients assimilate lay information, personal experience, and information from the social environment to form an interpretation of the impact of the disease on their life (Hagger et al., 2017). In illness perception, the integration of both abstract and concrete health information influences the patient’s cognitive representations and emotional responses and facilitates the assignment of meaning to the disease and illness experience (Dempster et al., 2015). Individuals will assess the effects on the illness and themselves over time, which can lead to changes in their cognitive representations and emotional responses in a type of feedback loop (Broadbent et al., 2015).
Most often, illness perception is measured using one of three versions of the Illness Perception Questionnaire (IPQ): the original IPQ (80 items across five domains of illness perception), Revised Illness Perception Questionnaire (IPQ-R; 70 items across nine domains), and Brief Illness Perception Questionnaire (Brief IPQ; nine items across nine domains). The list of domains assessed by the three versions of this instrument includes coherence, concern, consequences, control (personal and treatment), emotional representation, identity, and timeline (acute/chronic and cyclical) (Broadbent et al., 2006; Moss-Morris et al., 2002; Weinman et al., 1996). The domains of illness perception are defined in Table 1.
Domains of illness perception.

The original IPQ includes the domains of consequences, cure/control, identity, and timeline, which are based on the self-regulation model by Leventhal and colleagues (Weinman et al., 1996). The consequences domain comprises expected physical, emotional, and social effects and outcomes of the illness on the patient’s life. The control domain relates to how one perceives the possibility of recovering from or managing the illness, which incorporates both personal control and treatment control. The identity domain includes what it means to label oneself as having the disease and which symptoms are attributed to it. Finally, the timeline domain involves how long an individual thinks the illness will last.
The IPQ has been amended in response to researchers’ critical review and questions regarding the internal consistency of the timeline and cure/control subscales (Moss-Morris et al., 2002). The IPQ-R separates the timeline domain into two distinct subscales in order to address both the acute/chronic nature and cyclical aspects of some diseases (Moss-Morris et al., 2002). In addition, confidence in one’s personal ability to control the illness and the effectiveness of treatment were divided into two distinct subscales (Figueiras and Alves, 2007). The revision also incorporated the emotional representation domain from the self-regulation model and a coherence domain to assess whether the patient believes the personal representation of the illness is a useful interpretation (Moss-Morris et al., 2002).
The Brief IPQ was developed as a rapid assessment, particularly for severely ill patients, the elderly, and those who have literacy issues (Broadbent et al., 2006). The subscales of the Brief IPQ are represented by single items with an additional question regarding concern about the illness (Broadbent et al., 2006).
Methods
A search of MEDLINE via PubMed, PsycINFO, and CINAHL was conducted using a combination of subject headings and keywords (Table 2) to identify studies meeting the inclusion criteria through 2017. Terms for diagnoses in the HRRP were compiled from existing systematic reviews and refined based on the returned results. After initially screening titles and abstracts for relevance, full-text articles were reviewed for inclusion criteria.
Literature search strategy.

Inclusion criteria were as follows (1) reports published in the English language, (2) empirical studies using quantitative methodology (qualitative studies and case reports excluded), (3) mental health, health behaviors, and physical health outcomes measured, and (4) identifiable effect size and statistical significance of relationships provided. When the only statistically significant effect sizes given in a study were correlations, the study was included if the bivariate correlation was less than –.30 or greater than .30. Correlations between –.30 and .30 were considered negligible and were omitted (Hinkle et al., 1988).
Results
Tables 3 to 7 summarize the findings from the 31 studies that met inclusion criteria. The number of studies on HF, COPD, MI, CABG, and THA/TKA were 2, 6, 13, 5, and 7, respectively. Two of these studies involved both MI and CABG patients. No studies on pneumonia met inclusion criteria; therefore, this HRRP diagnosis was not included in this review. The associations between illness perception and health outcomes in patients with these five diagnoses are summarized below. The results are discussed based on category of health outcomes (mental health, health behaviors, and physical health).
Heart failure studies.

Chronic obstructive pulmonary disease studies.

QOL: quality of life; FEV: forced expiratory volume in 1 second; IPQ-R: Revised Illness Perception Questionnaire.
Myocardial infarction studies.

QOL: quality of life; PTSD: post-traumatic stress disorder; HRQOL: health-related quality of life.
Coronary artery bypass graft studies.
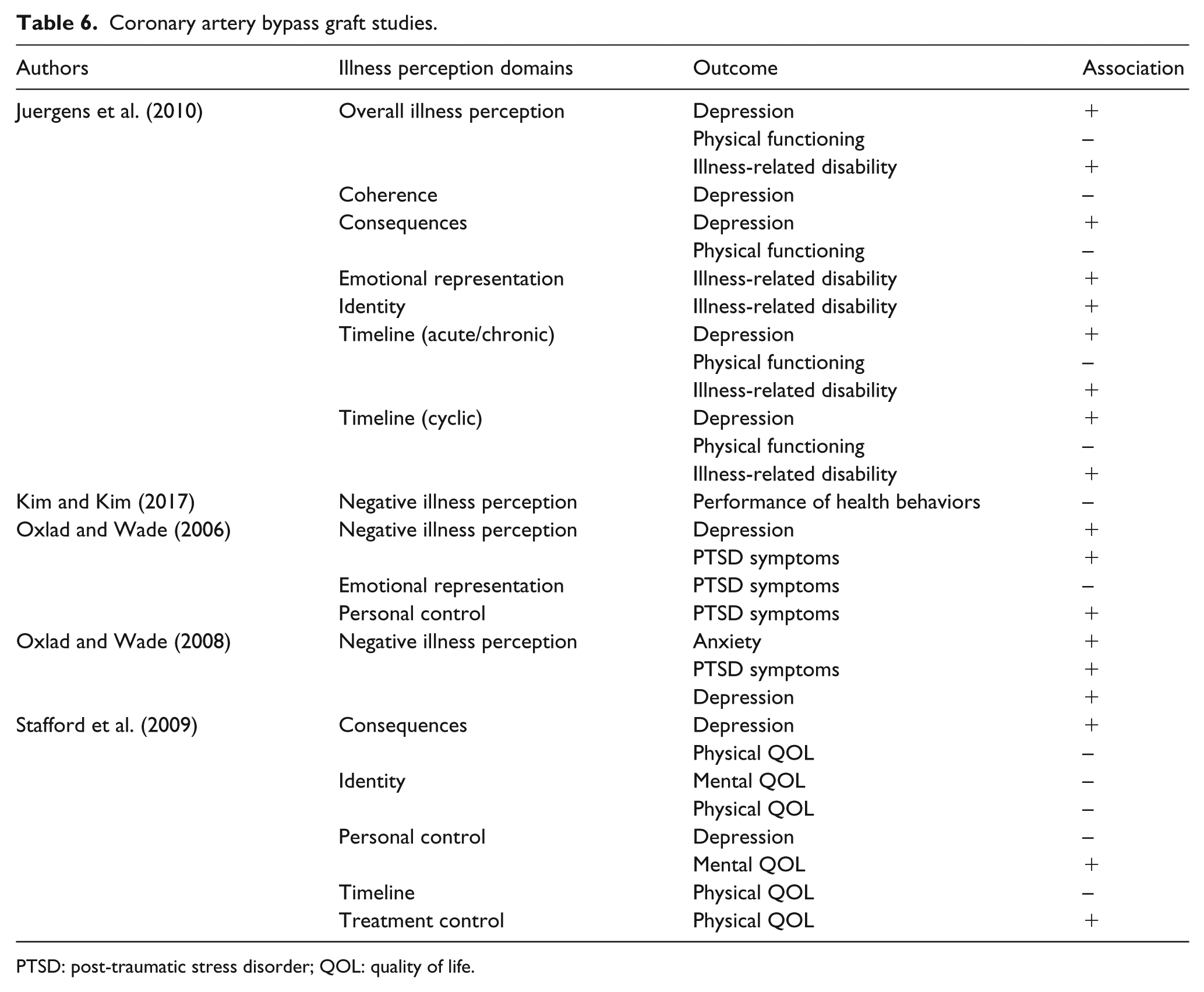
PTSD: post-traumatic stress disorder; QOL: quality of life.
Total hip or knee arthroplasty studies.

Mental health
Quality of life
Quality of life (QOL) is a multidimensional concept that includes physical, psychological, emotional, and spiritual well-being given the context of life circumstances, cultural norms, and personal values (Haas, 1999). Health-related QOL addresses how illness, injury, and/or treatment impacts well-being and prior experiences of normalcy (Megari, 2013). Chronic diseases and their treatments can be disruptive and thereby negatively impact QOL.
When assessed by the IPQ instrument and its versions, illness perception domains are often associated with QOL. For example, Borge et al. (2014) studied the illness perception of breathlessness in COPD patients and reported that the coherence, concern, consequences, emotional representation, and identity domains were all associated with lower global QOL. Other studies of COPD patients have described similar findings regarding overall QOL. One such study by Tiemensma et al. (2016) utilized the Brief IPQ to assess illness perception and found that the concern, consequences, emotional representation, and identity domains were all associated with lower QOL.
Several studies have focused on the relationship between illness perception and the mental domain of QOL. In a study of patients recently hospitalized for an MI or CABG surgery, the personal control domain was associated with higher mental QOL (Stafford et al., 2009). In contrast, the following domains were associated with lower mental QOL in COPD, MI, and CABG patients: consequences (Alsén et al., 2010), emotional representation (Alsén et al., 2010; Bonsaksen et al., 2014), and identity (Stafford et al., 2009). Vaske et al. (2017) found that a higher score on the Brief IPQ, indicating more threatening illness perception, was associated with worse mental QOL in COPD patients. Perceiving an illness to have negative consequences, not surprisingly, has been associated with lower emotional QOL (French et al., 2005).
Social QOL involves interactions, personal relationships, and integration into the broader society (Megari, 2013). Studies by French et al. (2005) and Scharloo et al. (2000) reported that negative beliefs about the consequences and symptoms of an illness, respectively, were associated with lower social QOL.
Well-being and self-efficacy
In COPD patients, the consequences, emotional representation, and identity domains have been shown to be associated with worse mental health (Borge et al., 2014). Another study of COPD patients who were attending pulmonary rehabilitation showed that perceiving many consequences and emotional effects of COPD, as well as having negative overall illness perception, were associated with worse psychological well-being after program completion (Zoeckler et al., 2014). Illness perception also can influence well-being after surgical procedures, including THA/TKA. For example, the consequences and emotional representation domains have been associated with worse psychological well-being in patients after THA/TKA (Magklara and Morrison, 2016).
Self-efficacy is the self-perception that an individual can achieve results that are important to them, which may contribute to the engagement in and maintenance of health behaviors (Bandura, 1977; Frei et al., 2009). In THA/TKA patients, Magklara and Morrison (2016) investigated the relationship between illness perception and self-efficacy. The perception of high personal understanding and the belief that treatment will help were positively associated with general self-efficacy and rehabilitation self-efficacy (Magklara and Morrison, 2016). In contrast, a negative belief about the emotional effects was associated with lower self-efficacy (Magklara and Morrison, 2016).
Anxiety and depression
Illness perception is often associated with anxiety and depression in patients with chronic conditions (Costa et al., 2016). Nahlén Bose et al. (2016) studied illness perception in HF patients. Only the treatment control domain was associated with lower anxiety (Nahlén Bose et al., 2016; Pinto et al., 2017), whereas the consequences and identity domains were associated with higher anxiety (Nahlén Bose et al., 2016). Negative illness perception in general has been associated with higher anxiety (Cherrington et al., 2004; Oxlad and Wade, 2008), as has the emotional representation domain (Pinto et al., 2013, 2017). The domains of concern, consequences, and identity have been associated with a diagnosis of acute stress disorder (Oflaz et al., 2014).
Dickens et al. (2008) studied the relationship between negative illness perception and the development of depression post-MI. Personal control and treatment control in that study were associated with 50 percent lower likelihood of depression. In that study, the perception that the condition would last a long time was associated with more severe depression (Dickens et al., 2008). Other studies exploring illness perception and depression reported that believing that one has a thorough understanding of the condition (Juergens et al., 2010) and perceiving high control over the condition (Pinto et al., 2013, 2017; Stafford et al., 2009) were associated with less depression. Other domains associated with greater depression include consequences (Juergens et al., 2010; Nahlén Bose et al., 2016; Stafford et al., 2009), emotional representation (Pinto et al., 2013, 2017), identity (Nahlén Bose et al., 2016), and timeline (Juergens et al., 2010; Pinto et al., 2013). Negative illness perception in general has been associated with higher depression scores in several studies (Cherrington et al., 2004; Juergens et al., 2010; Oxlad and Wade, 2006, 2008).
Post-traumatic stress disorder
Post-traumatic stress disorder (PTSD) symptoms are not uncommon among patients who have experienced acute medical events (Roberge et al., 2010). Associations between illness perception and PTSD have been examined in patients who experienced an MI or have undergone CABG surgery. Negative associations have been reported between the following domains and PTSD: coherence (Ruiz et al., 2011; Sheldrick et al., 2006), personal control (Oxlad and Wade, 2006), and treatment control (Ruiz et al., 2011; Sheldrick et al., 2006). However, the domains of coherence and treatment control have been associated with higher PTSD in one study (Marke and Bennett, 2013). Illness perception domains associated with greater PTSD symptoms have been the following: concern (Marke and Bennett, 2013; Oflaz et al., 2014), consequences (Marke and Bennett, 2013; Oflaz et al., 2014; Ruiz et al., 2011; Sheldrick et al., 2006), emotional representation (Oflaz et al., 2014; Oxlad and Wade, 2006; Ruiz et al., 2011; Sheldrick et al., 2006), identity (Marke and Bennett, 2013; Oflaz et al., 2014), and personal control (Marke and Bennett, 2013). Similarly, negative overall illness perception has been associated with PTSD symptoms (Oxlad and Wade, 2006, 2008).
Health behaviors
Personal health behavior has been identified as the single most important modifiable factor in terms of improving healthcare outcomes (Schroeder, 2007). Negative overall illness perception has been linked to worse health behaviors following an MI or CABG (Kim and Kim, 2017). In contrast, MacInnes (2013) reported that the domains of consequences, coherence, treatment control, and timeline were all associated with better self-care in patients with HF. Attending cardiac rehabilitation following an MI is associated with higher survival rates and better outcomes (Martin et al., 2012). Attributing many symptoms to the condition itself has been associated with better attendance at cardiac rehabilitation following an MI (Whitmarsh et al., 2003). In this regard, Broadbent et al. (2009) conducted a randomized controlled trial to investigate the impact of an illness perception intervention for patients following an MI. The intervention consisted of four 30-minute in-hospital sessions with a health psychologist. Investigators found that this intervention led to both increased exercise and greater return to work.
Physical health
Physical quality of life
Studies of illness perception in patients have often examined its relationship to the physical domain of QOL (Alsén et al., 2010; Bonsaksen et al., 2014; Stafford et al., 2009). In these studies, perceiving high control over a cardiac condition was associated with better physical QOL (Alsén et al., 2010; Stafford et al., 2009), whereas the domains of consequences (Alsén et al., 2010; Bonsaksen et al., 2014; French et al., 2005; Stafford et al., 2009), identity (Bonsaksen et al., 2014; Stafford et al., 2009), and timeline (Alsén et al., 2010; Stafford et al., 2009) were associated with worse physical QOL. Similarly, associations have been found between negative overall illness perception in patients with COPD and lower physical QOL (Vaske et al., 2017). In another study of COPD patients, the concern, consequences, and identity domains were all associated with worse physical health (Borge et al., 2014).
Disability and physical function
A study involving CABG patients investigated the association between illness perception prior to surgery and health outcomes 3 months post-operatively (Juergens et al., 2010). The domains associated with greater physical disability included timeline, consequences, emotional representation, and identity, with the authors noting that negative illness perception more generally has been associated with greater physical disability (Juergens et al., 2010). In a study of surgical patients following THA/TKA, the consequences and identity domains also were associated with greater physical disability (Magklara and Morrison, 2016).
The timeline and consequences domains, as well as negative overall illness perception, have been associated with worse physical functioning (Juergens et al., 2010). The belief that one has a thorough understanding of the condition, in contrast, has been associated with better knee function following TKA, whereas the perception of many negative consequences, emotional effects, and symptoms have been associated with worse knee function (Hanusch et al., 2014).
Decreased heart rate variability (HRV) has been reported to predict greater mortality following an MI (Kleiger et al., 1987). The domains of coherence, personal control, and timeline have been associated with greater HRV following an MI (Princip et al., 2016).
Pain and fatigue
Studies have explored the domains most frequently associated with pain after THA/TKA. These included the domains of concern, consequences, emotional representation, identity, and personal control (Lindberg et al., 2016a, 2016b, 2017). Two other studies have identified the emotional representation domain as one that is strongly associated with postoperative pain in these patients (Pinto et al., 2013, 2017). In another study, the consequences domain was associated with less pain (Lindberg et al., 2016b).
Fatigue has been identified as one of the most frequent and troublesome symptoms after MIs (Fredriksson Larsson et al., 2015). Perceiving high control over the condition has been associated with less fatigue following an MI, whereas the consequences, emotional representation, and timeline domains have been associated with more fatigue (Alsén et al., 2010).
Other physical health outcomes
In patients with COPD, physical health outcomes have included ease and efficiency of breathing. The following domains have been associated with greater breathlessness in these patients: concern, consequences, emotional representation, and identity (Borge et al., 2014). The domains of concern, consequences, and identity also were associated with lower FEV1 (forced expiratory volume in 1 second) in that study. In COPD patients attending pulmonary rehabilitation, negative overall illness perception has been associated with lower 6-minute walk test scores after program completion (Zoeckler et al., 2014).
The emotional representation domain has been associated with fewer outpatient clinic visits among patients with COPD (Scharloo et al., 2000), whereas negative overall illness perception also has been associated with more complications during in-hospital recovery following an MI (Cherrington et al., 2004).
Discussion
This review identified and synthesized the literature on the relationships between illness perception and the health of patients with the HRRP diagnoses. When illness perception is measured with a version of the IPQ, high scores on the consequences, emotional representation, identity, and timeline domains represent unfavorable beliefs about an illness’ negative consequences, emotional effect, number of symptoms, and chronicity or cyclical nature. High scores on the coherence and control domains represent favorable beliefs about one’s personal understanding of an illness and its controllability. Most studies in this review show that high coherence and high control are associated with better mental health, health behaviors, and physical health outcomes.
Quality of the research findings
Measurement
All studies in this review used the IPQ, Brief IPQ, or IPQ-R. These three instruments have demonstrated solid reliability and validity (Broadbent et al., 2006; Moss-Morris et al., 2002; Weinman et al., 1996) and have been used in both inpatient and outpatient settings. To our knowledge, no other instruments measure illness perception across a wide range of medical diagnoses.
Study design
Most studies using the IPQ, Brief IPQ, and IPQ-R have used a cross-sectional design (Broadbent et al., 2015). The 13 prospective cohort studies cited in this review measured different outcomes at various time points for specific diagnoses. In studies of patients undergoing CABG, associations were found between illness perception and anxiety and depression 3 months and 6 months later (Juergens et al., 2010; Oxlad and Wade, 2008), as well as disability and physical functioning 3 months later (Juergens et al., 2010). In studies of COPD patients, illness perception was found to be associated with QOL 1 year later (Bonsaksen et al., 2014; Scharloo et al., 2000), as well as outpatient clinic visits 1 year later (Scharloo et al., 2000). Following an MI, patients’ illness perception was associated with in-hospital recovery during their hospital stay (Cherrington et al., 2004), as well as PTSD 1 month, 3 months, and 6 months later (Marke and Bennett, 2013; Sheldrick et al., 2006). In THA/TKA patients, illness perception prior to surgery has been associated with postoperative anxiety (Pinto et al., 2013, 2017), depression (Pinto et al., 2013, 2017), and pain trajectory (Lindberg et al., 2016a, 2016b, 2017; Pinto et al., 2013, 2017). Illness perception was related to knee function 6 weeks and 1 year following TKA (Hanusch et al., 2014).
The only study that involved an illness perception intervention, which consisted of four 30-minute in-hospital sessions with a health psychologist, examined the impact on exercise and return to work (Broadbent et al., 2009). Future interventional studies are needed to determine the impact of similar interventions on mental health, health behaviors, and physical health outcomes.
Limitations
Limitations of this review include variation in duration of diagnosis, as well as timing of measurement. Time elapsed between diagnosis, measurement of illness perception, and assessment of health outcomes varied among studies included in the review. Greater elapsed time may affect both illness perception and health outcomes.
Implications for clinical practice
Because of the many determinants of mental and physical health, interventions to prevent untimely readmission of patients with HF, COPD, MI, CABG, or THA/TKA may require combined approaches that include behavioral, clinical, educational, and psychosocial components. The findings of this review suggest that interventions that target illness perception should be part of such a multifaceted approach to improving health outcomes in patients with the above diagnoses. Assessment of illness perception with a validated instrument rather than an open-ended interview can better inform healthcare providers and guide the education and care provided to patients. The development of an intervention with behavioral, clinical, educational, and psychosocial components may improve one’s illness perception.
Conclusion
Illness perception domains are related in different ways to mental health, health behaviors, and physical health outcomes in patients with HF, COPD, MI, CABG, or THA/TKA, diagnoses that are associated with high risk for hospital readmission. Future interventional studies are needed to determine how to improve domains of illness perception to make them more positive and less threatening, which may lead to better health outcomes in these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.