
Abstract
This study explored experiences of adolescents living with cancer, focusing on physical and psychosocial problems. Semi-structured interviews were carried out on 18 adolescents aged between 12 and 18 years. Transcripts were analyzed using thematic analysis. Results showed that the adolescents faced a lot of physical, psychological, and social problems due to cancer diagnosis, treatment, and care. In order to improve their well-being and quality of life, psychosocial interventions should be incorporated in biomedical interventions that adolescents with cancer receive. This study proposes cost-effective interventions that can be implemented in resource-restricted sub-Saharan countries like Zambia.
Introduction
Cancer is a major public health problem. It is in fact one of the leading cause of deaths in developed countries (Ferlay et al., 2010; Sener and Grey, 2005; Siegel et al., 2016; Thun et al., 2009) and second to cardiovascular diseases in developing countries (Walubita, 2015). In spite of being a public health problem, reports of technological advances in developed countries around its early detection, treatment, improved supportive therapies, and collaborative multi-centered clinical trials have been found to be responsible for the reduced mortality rates and higher quality of life (Andersen et al., 2009; Weiner et al., 2003). The case presented in many developing countries, particularly, sub-Saharan Africa (SSA), is different. For example, heightened mortality rates are due to late diagnosis, while quality of life borders on lack of access to appropriate therapeutic facilities and drugs, limited treatment as well as psychological services (Admani et al., 2008; Israels et al., 2010; Jemal et al., 2011; Kayula Childhood Cancer Foundation, 2012; Kruger et al., 2013; World Health Organization (WHO), 2009; Zambia Childhood Cancer Foundation, 2013).
The incidence of childhood cancer is present in most countries. In Zambia, the setting for this study shows increased overall cancer incidences including childhood cancer (Chintu et al., 1995; Slone et al., 2014; Walubita, 2015; Zyaambo et al., 2013). Cancer diagnosis affects both the child and the family and has implications for physical and psychological health, as well as socio-economic well-being of the victim and the immediate family. Many families face challenges to achieve normality after diagnosis (Andersen et al., 2009; Golden-Kreutz and Andersen, 2004; Golden-Kreutz et al., 2005). Furthermore, diagnosis of cancer is a major source of psychosocial challenges including compromised quality of life (Eilertsen et al., 2012; Kabinga, 2006; Walubita, 2015), emotional distress (Thornton et al., 2007), poor intimate relationships (Kornblith and Ligibel, 2003; Yurek et al., 2000), financial strain (Arndt et al., 2004), employment disruption and job loss (Bradley et al., 2005; Hewitt et al., 1999), and post-traumatic stress disorder (Shelby et al., 2008) to the victim and their family. In addition, cancer treatments (radiotherapy, chemotherapy, and surgery) adversely affect both physical and psychosocial well-being of young cancer patients (Li et al., 2013). Others report long-term mental health effects like depression and low esteem (Choi et al., 2014; Gorman et al., 2014; Li et al., 2013). These biopsychosocial effects of cancer have implications for the general well-being and quality of life of patients in many SSA countries with weak health care services and systems for cancer patients.
Investigating the life efficacy (how one thrives in life after hard times) of those diagnosed with childhood cancer is imperative for advancing an understanding of their psychosocial well-being. We believe that understanding the psychosocial well-being is dependent on the experiences of young cancer patients. The psychosocial inquiry into this phenomenon will help not only to understand the effects of childhood cancer but also provide strategic direction for interventions that could increase life efficacy of the affected children and their families. Some researchers report social benefits like reduced stress and improved quality of life based on an understanding of the diagnosis burden (Andersen et al., 2009; Jim et al., 2006). However, applications of such models that have worked in other contexts require careful consideration as the socio-cultural environment in which this study is situated is different.
Against this background, this study was undertaken to explore the experiences of adolescents diagnosed with cancer. In Zambia, literature addressing childhood cancer primarily focuses on prevalence, experiences, psychological well-being, and quality of life of caregivers (Kabinga, 2006; Walubita, 2015), with very little focus on the actual experiences of young cancer patients. It is hoped that this study will provide a perspective of the personal experiences of having cancer and cancer treatments through the self-reflective insights of young cancer patients. In addition, given the focus of the study, it is envisaged that the results of this study will help healthcare providers in Zambia to give equal importance to psychological and social well-being as given to the treatment itself. Thus, the objectives of this study were threefold: (1) establish the physical well-being of adolescents, (2) explore the social well-being of adolescents with cancer, and (3) explore the psychological well-being of adolescents with cancer.
Methods
Study location
Zambia is located in the southern part of Africa with an estimated population of 15,500,000 inhabitants (World Bank, 2016). Zambia is categorized as a lower middle-income nation (World Bank, 2016). The study was conducted in Lusaka city. Lusaka is the biggest city in Zambia with approximately 2,198,996 inhabitants (Central Statistical Office, 2010).
Study site
The study was conducted at the Kayula Childhood Cancer Foundation (KCCF) and University Teaching Hospital (UTH) Cancer Clinic. KCCF is a Zambian non-governmental organization (NGO) that was set up to help children undergoing treatment for cancer and to actively promote awareness of childhood cancer in Zambia. KCCF supports the work of Zambia’s only cancer treatment facility, located at Lusaka’s UTH Children’s Cancer clinic, by offering a “Transit House” that provides lodging, food, care, and transport services to child cancer patients undergoing chemotherapy treatment, especially those children from far areas. UTH is the main referral hospital located in Lusaka city and currently serves all adult and childhood cancer cases.
Sampling procedure and sample size determination
Participants were adolescents recruited using a purposive sampling method from the KCCF and UTH in Lusaka. Adolescents with cancer who were between 10 and 19 years of age, according to the WHO’s definition of adolescent (WHO, n.d.), and currently on chemotherapy met the inclusion criteria. Adolescents were included in the study if they were diagnosed with cancer at least 6 months before the study. The adolescents were either on chemotherapy, radiotherapy, scheduled for surgery, or were under observation following treatment. Nearly all patients included on the study were on painkillers. In total, 21 adolescents with cancer were approached but 3 were too frail to participate in the study. Therefore, the final sample size consisted of 18 adolescents. Majority (17) of the adolescents had suspended schooling because of long absence from school due to hospitalization (Table 1). We were able to reach interview code saturation from our adolescents’ interviews as opposed to descriptive and theoretical saturation (Guest et al., 2006) due to small sample size. Even though the criterion for descriptive and theoretical saturation was not achieved and the potential for complex understanding of the phenomenon of interest was constrained, code saturation was able to identify core categories that have good explanatory power (Bowen, 2008).
Demographic characteristics.

Data collection
This study employed semi-structured interviews because this qualitative methodology is particularly useful when researchers aim to understand the lived experiences, opinions, stories, and views of the specific respondents on a certain phenomenon (Knudsen et al., 2012). Interviews were conducted using five core open-ended questions covering physical, psychological, and social aspects of cancer. All the interviews were held in a quiet place that was most convenient to participants, and interviews were conducted by the first author (S.S.). The majority of interviews were conducted in English and three interviews in Nyanja, Bemba, or Lozi (three local Bantu languages). The interviewer is a native Lozi speaker and individual multilingualism is common in Zambia. Interviews were audio recorded, and notes were taken after permission was obtained from the facility in-charge, guardians, and the participants themselves. Notes were taken as a precautionary measure and for reference when making clarifications and probes during the interviews. Interviews that were in the local languages were translated to English, and all the transcripts were checked for accuracy by G.H. (supervisor to S.S.), who is fluent in two of the three local languages (Nyanja and Bemba) and English. The interviews lasted between 40 and 50 minutes.
Ethical approval
The study was approved by the Biomedical Research Ethics Committee of the University of Zambia. Permission was sought from the facilities before the participants were approached. All the guardians gave informed written consent, and the adolescents gave verbal assent. Most interviews were emotional. Therefore, the interviewees were asked if the interview could be stopped during the interview process.
Data analysis
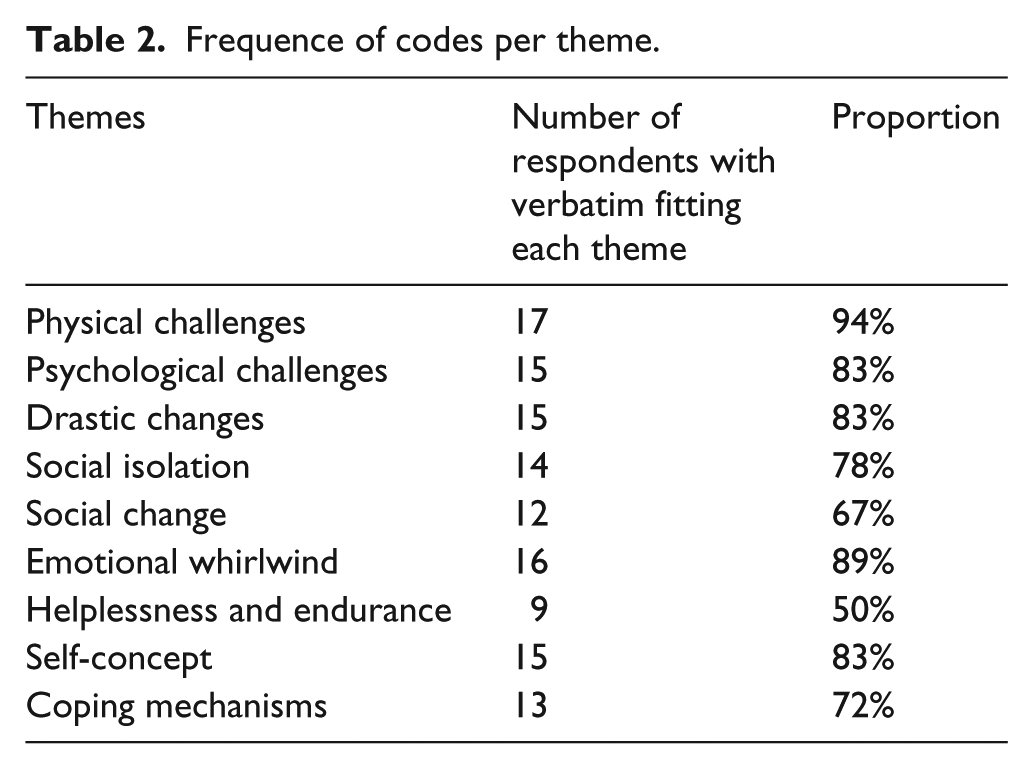
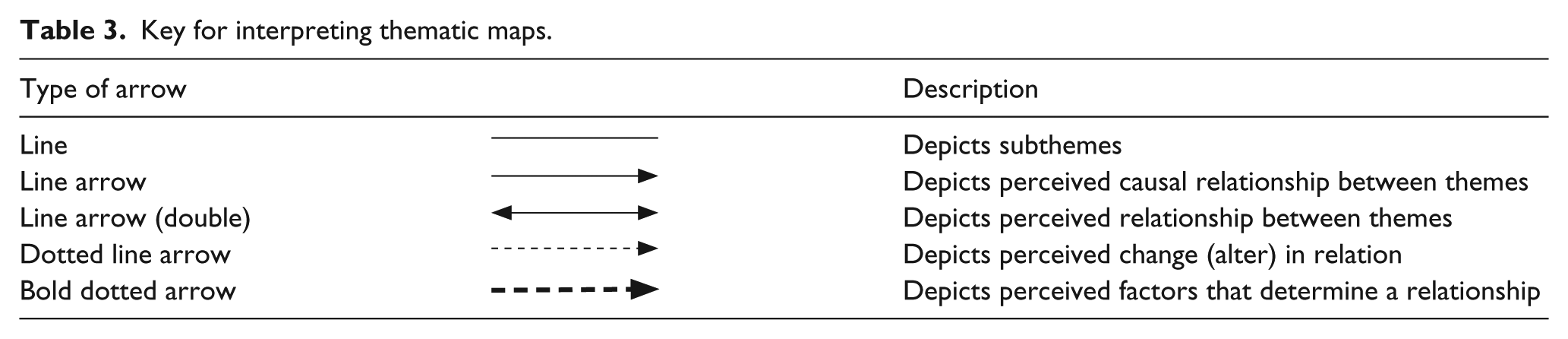
Audio recorded interviews were transcribed verbatim and translated to English whenever applicable and further checked for accuracy. In order to develop the themes and the categories, as near as possible to the material, an inductive category process was used (Knudsen et al., 2012; Mayring, 2000). After careful and thorough reading and re-reading, the initial coding and categorization of the themes was done by the third author and verified by the first and second authors (to ensure trustworthiness). Sentences or paragraphs related through their content or context were assigned codes, and related codes were finally categorized as themes (including both latent and manifest themes) in a tally table. This process continued until no new themes emerged from the data. Emergent themes were discussed and refined by the authors. Data were analyzed manually. The frequency of coded themes was then established by counting the participants who had their verbatim in each thematic unit (Table 2). In addition, thematic maps were created through a careful analysis of verbatims under each theme by focusing on how they interacted with each other based on manifest and latent analysis of threads to each meaning unit at theme level. A key for interpreting the maps is provided below (see Table 3).
Frequence of codes per theme.
Key for interpreting thematic maps.
Results
This study explored three objects: physical well-being of adolescents living with cancer, social well-being, and psychological well-being of adolescents with cancer. Thematic analysis resulted in the identification of nine themes. Under the first objective, three themes emerged: physical challenges, psychological challenges, and drastic changes. For objective two, two themes were identified: social isolation and social change, while for objective three, four themes were identified: emotional whirlwind, helplessness and endurance, self-concept, and coping mechanisms. The results below are presented according to the themes under each study objective.
Physical well-being of adolescents
Findings of the study showed that adolescents faced physical and psychological challenges directly linked to the physical well-being while at the same time making drastic changes in order to cope with the disease.
Physical challenges
All the adolescents were unwell most of the time, with the majority reporting aching of different body parts, feeling weak, and vomiting. One female adolescent had this to say about her ailing body and vomiting episodes: I am usually sick and always vomit. It is really hard for me to live like this. Female (12 years)
The vomiting was mainly caused by the treatment the adolescents were getting, especially chemotherapy. The reaction to treatment not only made them vomit or feel nauseous but they also reported feeling dizzy, tired, hungry, and sometimes muscle pains. These experiences can be substantiated by one quotation: I am tired of living like this [starts crying] … I don’t think my life will ever change [sobbing]. I am tired of vomiting, feeling dizzy and I am usually hungry. Female (12 years)
The adolescents experienced medicine and treatment exhaustion. Because of the joint and muscle pain that some adolescents reported experiencing, they were often given pain killers that contributed to medicine exhaustion. Furthermore, chemo and radiation therapy, and surgery conducted on adolescents as part of treatment were considered to be exhausting (treatment exhaustion), especially to those that commuted from other cities for treatment to Lusaka city. Longer hospitalization, sometimes accompanied by intensive care, was felt as an exhausting experience. Some felt they were fatigued of being in and out of the hospital. One adolescent said this, I am fed-up of being in and out of the hospital and the medication and chemo [chemotherapy] I have to undergo. Female (13 years)
Beyond treatment exhaustion, the adolescents faced yet another physical challenge—changes in the sense of taste. Some adolescents narrated how foodstuffs they previously enjoyed tasted differently, but in a bad way. Ironically, foodstuffs that tasted good for the adolescents were often discouraged on medical grounds. This posed a challenge because sensation change entailed they did not enjoy the food. Moreover, most adolescents reported feeling hungry frequently due to the treatment or side effects the medicine had on them. This situation was exacerbated by the patients’ inability to enjoy food. One girl with bone cancer experienced this, I don’t eat a lot, I feel tired when I eat a lot. I also crave food that I am not allowed to eat. But also, when I eat too much I vomit and visit the toilet a lot. So sometimes I don’t eat or just eat a bit. Female (12 years)
Psychological challenges
Psychological challenges experienced by adolescents emanated from the physical challenges they faced (Figure 1). Helplessness and shock (life blow) were the two main issues that formed this theme. Surgery caused a high sense of helplessness because adolescents could not save a body part that was operated upon to prevent spread of cancer. While being diagnosed with cancer was shocking, being maimed seemed to affect the adolescents even more: When I found out I had cancer and my doctor told me that they will remove my leg, I was in complete shock. I did not want it to happen … [silent and then cries] … my mother told me I had no choice but allow my leg be removed. Female (12 years)

Thematic analysis findings on living with cancer.
Drastic changes
Physical challenges caused adolescents to make drastic changes in order to live a manageable life after being diagnosed with cancer. Some changes were made in order to make them adapt in their physical, social, and psychological environments. One major change that was made to their lives was to avoid diets that were not medically suitable for them. Sugar and meat were some of the consumables that were not allowed: The doctor told me to stop taking white sugar and eating meat and I love meat a lot. Female (12 years)
On the flip side, some adolescents had to reduce on the amount of food they were eating or avoided food all together because it made them nauseated, and it was a measure to prevent vomiting. Thus, adolescents starved themselves as a prevention measure in order to avoid vomiting the food, which they had few options to choose from: Most of the time I am hungry but I can’t eat because I feel nauseated whenever I eat food. So I don’t eat anything the whole day sometimes to avoid vomiting … Female (15 years)
While some adolescents avoided eating because it made them feel nauseated, some adolescents avoided eating because they were immobile after being amputated and hence had difficulties accessing the toilets on their own. To avoid soiling themselves, some adolescents avoided eating as a preventive measure. One adolescent had this to say, It’s hard, sometimes the doctors are busy, and there are no people to take care of me. Sometimes I mess myself and have no one to help me clean up. Sometimes I don’t eat to avoid messing myself. Female (13 years)
Connected with issues of avoiding eating food in order to circumvent going to the toilet were the issues of depending on others to do routine activities, including going to the toilet. In some cases, the adolescents depended on apparatus to drain body waste. For instance, urinary catheters were inserted in some adolescents to help drain urine: Silence … umm they plug into me a catheter, that’ where I usually do everything [author insertion - depose of human waste]. Female (12 years)
Functional dependence on others (mainly guardians and health workers) and on apparatus made the adolescents feel incapable and bound.
Interestingly, a thematic map analysis showed that physical challenges caused life changes and the psychological challenges adolescents faced. Figure 1 shows how factors discussed above influence the well-being of the adolescents.
Social well-being of the adolescents
Two themes (social isolation and social change) emerged under the investigation of social well-being of adolescents with cancer. A myriad of factors, including rejection and ostracization by family members, loss of social ties, restriction (due to hospitalization), self-isolation, loneliness, socially uncomfortable, stigmatization, and self-pity, fall under this theme, while economic burden, family tension, and different lifestyle are factors that formed the theme social change.
Social isolation
Some adolescents reported being rejected by their relatives, friends, or romantic partners after learning they had cancer. One girl who was worried about finding a romantic partner said, I also worry about marriage and whether I will be able to have children in the future. People say people with cancer cannot have children. Female (15 years)
Adolescents were rejected by their significant others because they were seen as a burden to others from the economic and social point of view. Rejection and family ostracization was associated with cost and labor associated with taking care of a cancer patient. One girl narrated how after coming to the capital city for treatment, her only relative (aunt) in Lusaka rejected her and her parents because she was busy with work, and therefore, she opted to stay at KCCF, a transit home for children with cancer: My aunt refused that we stay in her house while I was being treated at the hospital. She said she was busy and did not have money to buy food in the house. Female (12 years)
Another girl mentioned how her friends and boys avoided her after learning she had cancer. The church, which often is a place of solace, was also found to have peers who shunned to interact with the adolescents: They [friends/peers] don’t even talk to me anymore and the boys at church usually avoid me. Female (12 years)
Social rejection and perceived inquisitiveness from the public, mainly because cancer patients have baldheads due to cancer treatment, made adolescents socially uncomfortable. Therefore, some adolescents avoided being in the public (self-isolation) because of the attention they attracted: I feel uncomfortable in public and people look at me in a weird manner, so I no longer go around in public. Female (12 years)
Furthermore, because adolescents avoided social settings and most of them had friends who avoided them, they lived lonely lives. Longer duration of hospitalization made adolescents feel even lonelier. They felt deserted: I don’t have friends to chat with … it feels really bad and I feel alone. Female (18 years)
Data showed that not all peers and friends avoided adolescents with cancer, but their behavior of portraying pity made the adolescents feel bad. Because adolescents perceived pity from others, such behavior made adolescents feel like they were eliciting pity from others “pity party” whenever they went out. This exacerbated the situation and made them go into self-isolation: Not everyone avoids me but other people instead pity me and I don’t like it. It makes me feel bad like am very sick. Female (15 years)
Stigmatization was one of the biggest problems that the adolescents faced. Adolescents were mostly stigmatized because people felt cancer was contagious, although there was some element of self-stigmatization, especially among the girls. Surprisingly, even family members thought it was contagious. One boy with retinoblastoma narrated how his father stopped him from playing with his friends because he could transmit cancer to them—“… but my dad refuses me to play with my friends because he thinks I can infect them with the cancer.” Situations like this made adolescents feel lonely: At home, especially my aunties and uncles, they do not take care of me because they think they will get cancer. I also don’t go to school and my friends from school don’t visit me because they think they will get cancer. Female (12 years)
Social change
Some physical changes also affected their social well-being. Majority of the adolescents were restricted to their homes, and they reduced their social interactions because they were dependent on others to take them for social activities and to use conveniences such as toilets. This also meant they stopped participating in outdoor activities and sports: I can no play volleyball as I used to, I can’t even walk to the toilet on my own (cries). Female (12 years)
Because majority of the adolescents were dependent on others to go about their everyday lives, this brought tension in the family. There was disruption of family members’ social activities because they had to spend time with the adolescents, and in some cases, family members accused each other of witchcraft as the cause of cancer. Family disagreement and tensions related to the adolescent’s cancer were common mainly because cancer was taking a toll on family finances: It has affected my family because my grandmother seems to be losing money and it has brought a lot of talking in the family as some people at the village are advising my grandmother to take me to a witchdoctor to find out who bewitched me … Female (13 years)
One adolescent mentioned how her siblings hated her because their mother was only paying attention to her at the expense of her siblings. There was also a perception that adolescents made their caregiver tired because of the work they did for them. This made the adolescents feel guilty, although their caregivers did not mention being tired taking care of them: … she seems tired even physically because she is always with me, taking care of me. She seems tired at times but she does not want to tell me … because she leaves her schedule and whatever she is doing to take care of me. Even at the hospital she spends night taking care of me. Female (15 years)
Further analysis of our data using thematic mapping showed that physical challenges faced by the adolescents caused social changes and social isolation. In addition, both social change and social isolation altered their social well-being. Figure 2 shows the intricate relationship between the themes.

Thematic analysis findings on social well-being of adolescents with cancer.
Psychological well-being of adolescents with cancer
Four themes emerged under this objective, namely emotional whirlwind, helplessness and endurance, self-concept, and coping mechanism. A number of emotional experiences, including hatred, fear (of death), guilty, and worry (dying alone), were mentioned. These emotions were compounded by psychosocial issues such as pain, suicidal ideation, perceived abandonment, unhelpful thoughts, stress, and wishful thinking. Issues surrounding self-concept included loss of self-confidence, self-blame, burdensome, and unattractive and acceptance of the condition were common.
Emotional whirlwind
Some adolescents hated themselves after surgery even when they knew that amputation was the only way cancer could be prevented. Not having a body part was emotionally painful to the adolescents. One girl kept crying while describing how amputating her leg had made her not only start walking with crutches but also how dependent she had become on her caregiver and lost the opportunity to play sports she loved so much. While some adolescents underwent a lot of emotional pain, some adolescents went through physical pain: I can’t see properly. I can’t even cry when I feel like crying because my eye pains so much that I just have to be strong. Male (12 years)
Data also showed that adolescents experienced guilt in two areas: one, they felt guilty because they were a burden to others and two, because there was role reversal. Instead of them helping caregivers with household chores, caregivers were literally doing everything for the adolescents. The guilt was so intense that some adolescents felt dying was a better option for them: I feel bad and most of the time I just want to die. [Starts ‘crying’] Most of the time I feel like I am just troubling my mum. I ask a lot of questions. This disease is bad. Starts ‘crying’. Female (12 years)
Although some adolescents felt dying was a good option than to be a burden, fear of death was also common among adolescents. The inevitability of death scared them, especially those who were given a time frame before their time to die: I am scared of dying here. The doctor told my father that I won’t live longer so I don’t know if I will ever see my friends. My friend died yesterday here so I feel like I am next. [silence] … I try not to think about it especially the issue of dying. Female (12 years)
The guilt and fear of death sometimes culminated into suicidal ideation and negative thought (often unhelpful thoughts). Unhelpful thoughts included self-blame for perceived abandonment of friends and relatives. There was a feeling that their illness caused tension in the family and loss of social ties: I feel bad, like everything that is happening is because of me. I wish I was never born. Male (15 years)
Worry about future adaption and adjustment was also a concern. Not only did the adolescents worry about adapting and adjusting in the face of perceived abandonment by friends and relatives, they were also worried about adapting in school, work, and romantic relationship contexts in the near future. The degree of worrying among adolescents was very troublesome because the adolescents were more worried about adult life than their current life: I feel like my life has ended because I can’t go to school and I don’t think I will ever get married. So I will end up alone because even men avoid me. This is hard for me. Men avoid me, I am uneducated. These thoughts trouble me. Female (12 years)
Consequently, because of worries such as these relating to adapting in school, work, and romantic relationships contexts, adolescents were imbued with wishful thinking. Adolescents wished one day they would wake up without cancer: [Starts crying] I hate staying in this place with such problems. I just wish I could wake up and find this was just a dream. Female (17 years)
Data showed that the lack of detachment to positive wishful thinking caused a sense of helplessness among adolescents with terminal cancer. They felt helpless amid their social ambitions and goals, which they could no longer achieve because of the illness: The fact that cancer has no medication I don’t know if I will ever get well. I know I won’t live like my friends. I will never get the chance to go to UNZA (University of Zambia—author insertion) like my friends. Some of my friends will even get married and I don’t think I will ever have that. Female (12 years)
The sense of helplessness sometimes made the adolescents question why they had to continue with the treatment. However, some adolescents endured with the treatment as a sign of love to their caregivers who had sacrificed a lot for them. Therefore, some adolescents took the treatment as a sign of love to significant others: Whenever I get chemo, I feel bad and I want to stop it. I have to be there for my mother because she loves me. Male (15 years)
Self-concept
The physical and psychosocial consequences of cancer made adolescents develop a negative self-concept. Adolescents had labeled themselves “burdens to others.” Some adolescents labeled themselves as “unattractive.” The label unattractive was common among girls, and they attributed loss of friends and lack of interest from boys as results of their perceived unattractiveness. As a result, some adolescents lost self-confidence: Yes, I have no friends and have no one to play with. I have lost my confidence. Female (12 years)
Some adolescents accepted their situation following the diagnosis of cancer and more especially treatment and surgery and had developed positive self-concepts as a result. Unlike those who perceived themselves as burdens and unattractive, positive self-image was common especially among the boys.
Stress and coping mechanisms
To cope with the stress emanating from physical, psychological, and social stressors, a number of coping mechanisms were mentioned including adaptive, emotion, and avoidance strategies. Sleeping, as a way of not only adapting to pain but also avoiding it, was mentioned. In addition, crying (emotional strategy) was a common strategy that was mentioned: I just cry about it and usually feel better afterward I also distract myself and try not to think about it by chatting with friends. Male (15 years)
Prayer, thought interruption, and suppression of bad thoughts were also mentioned as coping mechanisms: I am able to chat with friend and distract myself. When I think of my problems, I begin to cry so I don’t like thinking about problems. Female (13 years)
Analysis using thematic maps showed that psychological and emotional whirlwind, helplessness and endurance, self-concept, and the coping mechanisms adolescents used determined their psychological well-being (Figure 3).

Thematic analysis findings on psychological well-being.
Discussion
The objective of this study was to explore lived experiences of adolescents with cancer, particularly focusing on physical, social, and their psychological well-being. The threat that cancer has to the well-being of those affected by it cannot be overemphasized (Banda, 2006; Eilertsen et al., 2012; Kabinga, 2006; WHO, 2014). Like the findings of other studies (Eilertsen et al., 2012; Kabinga, 2006; Li et al., 2013), results of this study suggest that every part of the adolescents’ lives had changed due to cancer. In this study, the impact of childhood cancer experience was psychosocially and physically profound. Like other pediatric patients, our patients had problems with social relations and adjustments, self-concept, and stress related to treatment, surgery, chemotherapy, and radiation (Hudson et al., 2003; Ishida et al., 2010; Li et al., 2013; Stam et al., 2006; Von Essen et al., 2000). This study found that tiredness, weakness, fatigue, pain, and change of appetite were common. These are usual changes and experiences albeit differing in intensity and degree for each patient. To have cancer, it means that one or more of these changes will be experienced. These physical changes may affect the quality of life and the emotional state of cancer patients (Michel et al., 2010; Servitzoglou et al., 2008; Von Essen et al., 2000).
Our finding converges with those from the literature that adolescents are affected by their physical appearance following surgery (Hudson et al., 2003; Li et al., 2013; Stam et al., 2006; Von Essen et al., 2000). Surgery sometimes caused them to be maimed because through this process others lost legs, arm, or sight in order to prevent spread of cancer. The psychosocial impact resulting from the cancer experience seemed to differ in level and intensity, although the site of surgery appeared to be an important factor (Marcus, 2012). Given that adolescence is crucial for identity and self-concept formation (Kail and Cavanaugh, 2017), the psychological implication of adolescents with cancer is that they were strongly affected by the way they looked and were looked at by others. Diagnosis, treatment, and surgery of cancer can affect one’s self-concept because of bodily changes that comes with it such as bald heads, surgery, and in the worst scenario, amputation. Therefore, the part of the body affected by the disease or surgery plays an important role in the adolescents’ sense of self and body integrity. When you are not ashamed or scared to reveal yourself, your self-concept tends to be positive. We also found that adolescents were largely helpless as they could not present surgery on affected body parts because it was a matter of life or death. This problem seemed to affect girls more than boys because of the society’s expectations of a female body and how they should look. This explains why they were worried about their chances for romantic relationship and marriage.
In addition, our findings reveal that the girls were not only worried about the possibility of finding a life partner but also worried about the possibility of conceiving and bearing children. There is evidence on how cancer treatment affects fertility (Waimey et al., 2015), and young people have the cause to worry about their fertility. A recent discovery on lab-grown eggs could, in future, safeguard the fertility of girls with cancer ahead of potentially harmful medical treatment, such as chemotherapy (University of Edinburg, 2018). However, such technological advances are far from safeguarding fertility and ameliorating fertility anxiety. Worry about fertility was not surprising because literature shows that worry about fertility begins to rise around the age of 16 and continues until the age of 22 (McDonnell et al., 2017). With regard to perceived challenges with romantic relationship, this anxiety mostly emanated from physical changes resulting for treatment and surgery. In light of the accrued perceptions, most of the girls reported that they avoided social contexts because of the self-concept they had formed about themselves, following the diagnosis of the disease and surgery. Moreover, a good number of adolescents mentioned facing stigmatization from family members and peers who thought it was a contagious disease or because adolescents looked different. This is consistent with findings from South Africa among adult cancer patients (Wallace et al., 2018). In this study, the cultural factors and location of the cancer, especially if certain body parts (associated with masculine and feminine roles) were affected, as well as having visible cancers/side-effects influenced stigmatization against adolescents.
The experience of distress after cancer diagnosis is not unexpected nor is it unusual for cancer patients to experience distress during treatment (Michel et al., 2010; Servitzoglou et al., 2008; Stein et al., 2008; Von Essen et al., 2000). Distress in these adolescents is often associated with diagnoses and treatments. As established already, adolescence is a unique and important phase in development that represents a period of increased risk for adverse psychosocial outcomes (Granowetter, 1994; Steinberg, 2005), therefore, the period itself exacerbates levels of distress. Like other studies, we also report that adolescents in this study showed some anxiety regarding their health, particularly, the worry that they were going to die. Although the overall cure rate for cancer is around 60 percent, a substantial number of children with cancer still do not survive the disease in developed countries (Andrykowski and Hunt, 1993; Greaves, 2006; Olson et al., 1997; Savage and Schüz, 2011). This means that in least developed countries like Zambia, survival rates are even lower and justifies anxiety around cancer-related death (Greaves, 2006; Olson et al., 1997; Savage and Schüz, 2011).
In our study, common signs of depression were identified from the respondents’ verbatim including being worried, sad, guilty, anger episodes, and sometimes lack of sleep and appetite consistency with previously reported findings (Michel et al., 2010; Servitzoglou et al., 2008). Anxiety and other emotional experiences of these adolescents have implications on their adjustment and quality of life (Banda, 2006; Eilertsen et al., 2012; Kabinga, 2006). One other interesting observation from our data is a sense of guilt that adolescents experienced due to over-dependence on caregivers and role reversal. This sense of guilt was profound because of the cultural context in which these patients found themselves. In the Zambian culture, children are seen as helpers of caregivers, and most children take pride in participating in daily household activities and chores. However, due to physical changes which brought incapacitation, most adolescents were unable to help, instead caregivers performed chores that normally they would do and this heightened the sense of guilt.
While diagnosis and treatment can have some positive response depending on age and characteristics, we found none in our data expressing enhanced self-esteem, greater life appreciation and meaning, heightened spirituality, and greater feelings of peace and purposefulness (Bower et al., 2011; Cohen and Mount, 2000). However, sense of acceptance was found in some adolescents, especially younger ones, more especially the boys. This observed variability may suggest individual differences in response to cancer. We speculate that boys were more likely to accept the situation because of less cultural expectation on body perfectionism compared to girls, also younger ones aged below 15 could have accepted the situation because they did not yet understand the implications of the physical changes on romantic relationships and social adjustment.
With physical and psychological problems that adolescents with cancer face, we illustrate that these have the potential to disrupt normal social functioning of the adolescents. Based on the thematic map, there seems to be a relationship between psychological challenges and making life changes among the adolescents. Fatigue, immobility, and worry, for example, affect their social interactions. Being capable of doing normal daily activities is one of the determinants of quality of life of cancer patients (Cohen and Mount, 2000; Michel et al., 2010; Servitzoglou et al., 2008). However, most of our adolescents indicated that cancer treatment and surgery affected their normal daily activities and social interactions. In developed countries, even children with prosthetics in their upper or lower limbs face lifetime functional limitations (Pruitt et al., 1996). In Zambia, most children, if not all, have no prosthetics, suggesting a high degree of physical and functional impairment compared to their Western counterparts. We found that sporting activities such as school participation and interaction with friends, including sleep patterns, were reported to have changed for our adolescents. These findings on adolescents are not unique. In an adult sample of Canadian and Iranian cancer patients, daily activities were perceived to have changed in a negative way—sleeping or taking a nap during the day, watching TV, performing household chores, exercise, sports, and going out for a walk were reported to have changed (Shahidi et al., 2014).
With all these serious physical and psychosocial issues that adolescents go through, coping with the changes that come with cancer are important for their well-being. While our data showed that the adolescents were not offered formal counseling, some indicated that some medical doctors attending to them often offered advice on how to cope with the disease. However, many of the adolescents adopted their own coping mechanisms, including sleeping, crying, prayer, talking to friends, or avoiding thinking about the problems (cancer and treatment). We observed that limited access to more adaptive and relaxing mechanisms to a larger extent determined the mechanisms our adolescents adopted. In Canada, for instance, adults with cancer relaxed from the pressures of cancer through reading, watching TV, going out for walks, listening to music, and exercising or sporting compared to their Iranian counterparts who relaxed through getting involved in religious/spiritual activities, visiting with family, sleeping, visiting with friends, and taking a trip (Shahidi et al., 2014). From our analyses, cultural differences and socio-economic factors determined the mechanism likely to be adopted for relaxation or coping. We suggest that clinicians should use contextual and practical relaxation and coping mechanisms available to patients. Notwithstanding the importance of coping, physicians, and nurses in the lives of cancer patients, this study did not examine these practitioners’ perceptions, awareness, knowledge, and available interventions on psychosocial issues experienced by children with cancer and their families. These are areas of future research that could be important to the puzzle that we are addressing.
Loneliness and isolation were found to affect adolescents. The two do not just affect the psychosocial well-being of the children, but also affect the mental and physical well-being of the children. For instance, loneliness has been found to associate with frequent visits to a doctor, school drop-out, depression, suicidal ideation, low-self-esteem, social anxiety, eating disorder, and sleeping problems (Ergen and Çikrikci, 2018; Gerst-Emerson and Jayawardhana, 2015; Huang et al., 2017; Maes et al., 2017), all to some extent found in our study. Adolescents with cancer mainly experienced reduced social interaction due to treatment and social isolation resulting from the stigma they experienced which in turn induced loneliness which also triggered some biophysical issues mentioned above.
Recognizing that physical symptoms like fatigue, pain, and nausea can heighten emotional distress, anxiety, and depression (Cancer Council, 2016), we recommend that measures such as planning to do things when a patient feels less tired, limiting daytime naps for a better night sleep experience, and exercising be encouraged to help adolescents manage fatigue (American Cancer Society, 2014; Cancer Council, 2016). Eating a balanced diet and small portions more often during the day are some of the ways patients can manage appetite issues. For those whose experience change in the way they see and feel about themselves, we recommend helping them to see themselves from the inside (they are still the same person with great personality) and can also participate in interventions such as “Look Good, Feel Better.” Furthermore, as shown in thematic map 1, physicians should concentrate on improving the physical well-being of adolescents because it is the source of psychological challenges and poor quality of life. Interventions such as these can ameliorate and improve life experience of these patients. The most important thing to do and help patients during this period is to develop some ideas on how to handle physical and emotional changes resulting from the treatment (American Cancer Society, 2014; Cancer Council, 2016) and incorporate psychosocial counseling during the treatment.
This study has limitation besides the obvious relating to subjectivity of respondents’ views. For instance, failure to reach descriptive and theoretical saturation suggest that the sample size was small, and future studies should consider big sample sizes to surface more issues affecting adolescents with cancer. However, the strength of this study is the use of thematic maps which allowed the researcher to understand the underlying structure of threads in the text which could form the basis for validation using quantitative designs. The study has also theoretical and clinical impact that can inform biopsychosocial interventions for cancer patients. The implication of this study is the urgent need to improve physical and psychological care of not only Zambian patients with cancer but also patients of other SSA countries with weak health care services.
In conclusion, adolescents with cancer in Zambia experienced profound physical and psychosocial changes that need immediate attention. Adolescents do not just experience negative emotions following diagnosis, living with cancer to these children involves body changes, surgery, and/or several medical procedures including fertility-threatening chemo and radiation therapy. Their social and psychological well-being is also adversely affected. The narrative from these adolescents echoes their cries—“every part of me has changed.” Our study brings unique knowledge of the childhood cancer victims in relation to the experiences that pertain to psychological and social well-being. This information is critical to understanding not only their way of life but also for prospective interventions that need information about their actual experiences. Mechanisms to save brains and improve quality of life for these patients are limited, and there is need for immediate improvement of their health and general quality of life.
Footnotes
Acknowledgements
SS collected and transcribed data and commented on the manuscript. TC-K wrote the introduction, verified analysis, and made comments to the manuscript. GH conducted the analysis and wrote the methodology and discussion sections.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Biomedical Research Ethics Committee of the University of Zambia.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.