
Abstract
Approximately 64,000,000 people in the United States report binge drinking at least once in the past month. Unlike overeating and oversleeping, “overdrinking”—defined as drinking more than a person intends to drink—does not exist in the literature. Terms such as binge and problem drinking do not consider the intent of the drinker. The results of this pilot study suggest that most people drink more than they intend to drink. Moreover, they also report often being surprised that they overdrank. Smartphones may help overdrinkers be less often surprised by overdrinking and may prevent drinkers from developing an alcohol use disorder.
Keywords
Binge drinking contributes significantly to health problems, violence, sexual assaults, and accidental deaths (Centers for Disease Control and Prevention (CDC), 2013; Dwyer-Lindgren et al., 2015). Based on a 2014 Federal study of 138,000 drinkers, approximately 64,000,000 people in the United States binge drink at least one time per month (Esser et al., 2014), and the CDC reports that binge drinkers average 4.4 binge drinking episodes per month and drink on average 7.9 drinks per drinking episode. Half of the approximately 80,000 deaths attributable to alcohol are the result of binge drinking (CDC, 2001). Mokdad et al. (2004) report alcohol consumption as the third leading cause of death in the United States, and the World Health Organization (WHO) (2014) attributes approximately 3.3 million deaths per year worldwide to harmful alcohol use.
Sacks et al. (2015) estimate the cost of binge drinking at $190 billion per year in the United States; approximately 40 percent of that cost, $80 billion, accrues to the U.S. Government. The median cost to states is $2.6 billion per year, and Bouchery et al. (2011) estimate that binge drinking contributes to most of the estimated $746 per person per year cost of excessive alcohol consumption. One study suggests that non-dependent (based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria) drinkers cost society more than dependent drinkers (Woerle et al., 2007).
Binge drinking is defined by the Federal Government as more than five drinks for men and more than four drinks for women on one occasion (National Institute on Alcohol Abuse and Alcoholism (NIAAA), 2004). The term “overdrinking” does not exist in the literature. 1 However, terms that reflect eating, sleeping, and spending beyond an intended or set limit do, that is, overeating (Adriaanse et al., 2016; Schmidt and Martin, 2015; Sinclair-McBride and Cole, 2016), oversleeping (Kikuchi et al., 2011; Ohayon and Roberts, 2015), and overspending (e.g. Nguyen, 2016). Overdrinking is defined here as drinking more alcohol than an individual intended to drink, whether or not that meets or exceeds the Federal definitions of “binge drinking” and/or “excessive drinking.” However, it is not known how many intend to binge drink and how many do so inadvertently. Although many college students intentionally binge drink, including “pregame” drinking (Borsari et al., 2007; Zamboanga and Olthuis, 2016), it seems probable that many adult, non-alcohol-dependent drinkers do not intend to overdrink, even though they may do so quite frequently.
The first of 11 criteria for an alcohol use disorder (AUD) in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) is “Had times when you ended up drinking more, or longer, than you intended?” (American Psychiatric Association, 2013). If coupled with only one of the other ten criteria, for example, #2, “More than once wanted to cut down or stop drinking, or tried to, but couldn’t” or #10, “Had to drink much more than you once did to get the effect you want. Or found that your usual number of drinks had much less effect than before,” a person would meet the DSM-5 criteria for a “mild” AUD. However, most overdrinkers, even though they may drink “more or longer, that [they] intended,” in fact, may not meet DSM-5 AUD criteria.
Many overdrinkers would also probably not meet the criteria for any form of alcohol abuse or dependence set by the World Health Organization’s International Classification of Diseases, 10th Revision (ICD-10; American Medical Association, 2017). The ICD-10 criteria are now mandated to be used by all health care providers covered under the Health Insurance Portability and Accountability Act (HIPAA), not the DSM-5. The best ICD-10 codes for overdrinkers may be F10.9, “Alcohol use, unspecified,” F10.92, “Alcohol use, unspecified with intoxication,” or F10.92, “Alcohol use, unspecified with intoxication, uncomplicated,” when and if appropriate. Esser et al.’s (2014) study also noted that most excessive drinkers are not “alcoholics” or dependent on alcohol (using the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) criteria). Overdrinking is typical of drinkers who have been referred to as “problems drinkers,” and many may also engage in intentional binge drinking. However, it does not refer to the type of drinking typical of people with moderate to severe alcohol misuse disorders. Overdrinking reflects the idea of behaving in a way that is beyond what one intended, as do the terms overeating, overspending, and oversleeping.
There is no specified amount of food or sleep or alcohol that a particular individual ought to eat, sleep, spend, or drink in order to avoid health or financial problems. There are suggested Federal guidelines, but the amount of calories or hours of sleep required varies significantly from individual to individual. Similarly, while binge drinking is precisely defined by the Federal Government for males and females, the definitions do not take into account individual differences in metabolism and weight or the intent of the drinker at that time. Labels are important, especially in the alcohol misuse field. “Hazardous drinkers,” “heavy drinkers,” and “binge drinkers” do not reflect the fact that many people may intend to drink less, but, like overeaters, drink more than they had thought they would or had planned to.
Overdrinking and overeating
Insight into reducing overdrinking behavior might be gained by looking at the research related to a similar behavior, overeating. In total, 45 percent of successful dieters report losing weight on their own versus 55 percent who report using a weight loss program (Thomas et al., 2014). But approximately 80 percent regain the weight they have lost and many gain more, that is, most overeaters do not lose weight and keep it off (Kraschnewski et al., 2010; Mann et al., 2007). That would be analogous to most overdrinkers returning to binge or excessive drinking and many becoming alcohol dependent. In reality, only approximately 6 percent of drinkers become alcohol dependent (Esser et al., 2014). Evidently, most overdrinkers moderate their behavior over time.
In the eating behavior literature, one focus is on “restrained” and “unrestrained” eaters (cf. Herman and Mack, 1975; Wansink and Chandon, 2014), similar to what some researchers have called “restrained drinkers” (Bensley, 1991; Collins, 1993; Collins and Muraven, 2007). Restrained eaters are also described as “chronic dieters” and unrestrained as “normal” eaters by Stroebe et al. (2013).
Stroebe et al. (2013) present considerable research evidence in support of their proposed “goal conflict” theory of overeating. The research evidence suggests that restrained eaters/chronic dieters are caught between two conflicting goals: the “eating enjoyment” goal and the “weight control” goal. For most overeaters, many cues in a food-rich environment “prime the goal of eating enjoyment” (p. 110). As a result, thoughts related to the weight control goal are inhibited and a “preferential processing” of enjoyable eating occurs, leading to overeating. Stroebe et al. (2013) suggest that hedonic factors, that is, the pleasure associated with eating, play the key role in overeating, something very similar to what may occur in overdrinking. In the case of overdrinking, the goal of not overdrinking may fall victim to “enjoyment factors.”
However, in some restrained eaters, this does not occur. The factors that explain this difference are still not understood. Cues from enjoyable looking food appear to prime for the weight control goal, not the eating enjoyment goal, and those restrained eaters do not succumb to overeating and do not gain back the weight they have successfully lost. It is hypothesized that some individuals may have more working memory capacity and can therefore keep their weight control goals in mind, and some research (Houben et al., 2011; Nowakowska-Domagała et al., 2017) indicates that something similar may be occurring gradually in overdrinkers.
Marks (2015, 2016) proposes that overeaters get stuck in a “Circle of Discontent.” His Circle of Discontent Theory (CODT) suggests that the driving force is homeostasis and dyshomeostasis. When people feel uncomfortable because they are hungry, they attempt to correct this homestatic imbalance by eating; however, then they often become discontented because they have eaten too much. This leads to negative affect, leading to an attempt to self-soothe by eating more. Many other factors, such as developmental problems resulting from poor attachment as a child and genetic factors, are hypothesized to also play a role.
Limit violation effect
Intentional setting of limits may have an impact on subsequent drinking behavior but not always a beneficial one. In 1993, Collins, Lapp, and Izzo introduced the concept of a limit violation effect (LVE) for drinkers who were trying to limit the amount they drank. They hypothesized that an LVE might function in a similar fashion to the abstinence violation effect (AVE) proposed by Marlatt and Gordon (1985). Marlatt and Gordon (1985) hypothesized that the effect of violating an intention to abstain could turn into a lapse, for example, one drink into a full night of drinking or even a complete relapse to the old behavior pattern. Self-blame and the resultant negative affect were hypothesized to contribute to more drinking in an attempt to alleviate the negative mood and self-blame. Similarly, Collins (1993) hypothesized that the setting of a goal to limit drinking (in people wanting to cut down or moderate, not abstain completely) may contribute to heavy drinking if the limit is violated.
Individuals appear to differ in the extent to which the LVE, negative affect, and more drinking interaction are found. Two studies of social drinkers, one of an underage group and the other of a community sample, using hand-held computers and ecological momentary assessments (EMAs), looked at the effects of drinking beyond a self-set limit (Muraven et al., 2005a, 2005b). Individuals who attributed a limit violation to internal factors experienced more negative affect and tended to drink more when they drank again, not less. The negative affect-overdrinking effect was also stronger in people who were already heavy drinkers. After violating their limit, they drank more heavily the next night, not less. The two studies, both using EMA, tracked a combined number of 150 people and collected over 2500 observations, providing evidence of an LVE among both an underage sample and a community sample of social drinkers. And, as the authors suggest, this vicious cycle effect may help explain the way some people move from occasional overdrinking to developing a severe AUD.
Reducing unintentional binge drinking (overdrinking): EMAs and just-in-time adaptive interventions
The need for technologies designed to help overdrinkers moderate their behavior exists partly because most drinkers do not see the need for treatment and do not seek treatment, and the forms of treatment available are not well designed for them (Grant, 1997; Saunders et al., 2006). The proliferation of smartphone apps and wearables and the popularity of using such devices to attempt to intentionally change health-related behaviors are growing (Krebs and Duncan, 2015). The evidence for the effectiveness of ecological momentary interventions (EMIs) and just-in-time adaptive interventions (JITAIs) are also increasing (Zhao et al., 2016).
Gonzalez and Dulin (2015), using a smartphone-based treatment system for a group of participants diagnosed with an AUD, found that those using the program had significantly more days abstinent and significantly fewer heavy drinking days and drinks per week. Dulin et al. (2014) using the same treatment program with a similar group reported that the participants using the system decreased their hazardous drinking days by 52 percent. In addition, only 25 percent of their drinking days were hazardous drinking days versus 56 percent for the participants not using the program.
Suffoletto and Chung (2016) investigated the potential effectiveness of a text messaging system to alter drinking behavior in non-treatment-seeking college students. They found three distinct classes of students: (1) those who did not intend to drink, (2) those who intended to drink but also planned to limit the number of drinks consumed (had a limit in mind), and (3) those who intended to drink but did not plan to limit their drinking. The text messaging program designed to encourage a reduction in drinking had the greatest impact on those students reported not intending to drink that weekend. It had the least impact among those intending to drink but not intending to limit their drinking.
Reich et al. (2015) found significant individual differences in the manner in which various factors affected a change in drinking behavior. In a 5-year study of binge drinking, they followed 645 young people aged 18–23, collecting over 700,000 data points. Impulsivity and sensation seeking tended to predict the intensity of a binge drinking episode, while sociability and expectancies tended to predict the number of drinking episodes. Changes in drinking behavior were primarily the result of fewer binge drinking episodes per week, not fewer drinks per episode. At the beginning of the study, almost 60 percent of the participants reported having at least one binge drinking episode in the past 4 weeks. But, at the end of the study, that number had dropped to approximately 45 percent.
This study proposes to focus on a sample of a large group of understudied individuals: the millions of people who are not suffering from a moderate or severe AUD who unintentionally overdrink. The first research objective is to gain a better understanding of overdrinking in a community sample. Several questions are of interest: Do many people have a limit in mind when they drink alcohol? If so, do they often exceed that limit, as many people often overeat although intending not to do so? To what extent do people intentionally try to drink less, similar to the way people attempt to limit the number of calories they consume when they eat? If they overdrink, are they surprised by that behavior? And if they change their behavior over time, does that occur because they intentionally try to cut down or does it occur as some kind of “maturing out” process; that is, as they age, they drink less? And if they try to cut down intentionally, is that a difficult process for many people?
The ongoing research objective is to learn how to accelerate moderating or stopping binge drinking using emerging technologies, in particular smartphones and wearables. EMAs and intensive longitudinal data (ITD) collection provide an opportunity to better understand overdrinking and to develop EMIs and JITAIs to help overdrinkers change. Moreover, such micro-interventions may be able to accelerate that change. That, in turn, may decrease the number of overdrinkers who become alcohol dependent.
Method
A survey was conducted using a Qualtrics survey linked to Amazon’s Mechanical Turk (MTurk). This was done to ensure the confidentiality of the MTurk workers’ responses considering the nature of the questions being asked. Qualtrics generates a random number that MTurks can use at the end of the survey to obtain payment for their participation. A study by Buhrmester et al. (2011) found that MTurk sample participants “are slightly more demographically diverse than are standard Internet samples” and “significantly more diverse than typical American college samples” and that the “data obtained are at least as reliable as those obtained via traditional methods” (p. 3). A study by Goodman et al. (2013) also found that MTurk samples and traditional samples were quite similar. A total of 105 MTurk workers responded to a very brief survey about overdrinking alcohol and were paid $50 for their participation. The respondents ranged in age from 21 to 68. Of them, 41 percent were between the ages of 21 and 30, 33 percent were 31–40, 18 percent were 41–50, and 9 percent were 51 or over. And 58 percent were male and 42 percent female. They identified with a fairly broad range of ethnic groups: 65 percent identified as white; 21 percent as Asian; 8 percent as Latino/a or Hispanic; 2 percent as black; and 5 percent were unclassifiable.
Survey takers (workers), part of the Amazon Mechanical Turk (MTurk) platform, were paid to complete a brief survey consisting of nine questions regarding their drinking of alcohol. The three questions of greatest interest were as follows: (1) “If you drink, do you usually have a limit in mind?” (2) “How often do you drink beyond what you intend to drink. That is, you drink more than you planned to drink?” (3) “If you overdrink, are you surprised later, for example, the next day that it happened?” For the last two questions, participants responded to a 5-point Likert-type scale ranging from “never” to “every time I drink.”
The survey also asked whether the respondents sometimes binge drank on purpose, if they had tried to cut down and, if they had tried to cut down, how easy or difficult they had found that to do, responding to a similar five-point Likert-type scale ranging from “very difficult” to “very easy.” If they were drinking less than in the past, the respondents were asked whether they thought that seemed to have happened as they aged or whether they had intentionally tried to cut down or moderate their drinking.
If they had cut down their drinking, they were also asked whether they had done that by reducing the number of times they drank or the number of drinks per drinking episode or both. The statistical software R was used to clean and analyze the data, including Chi-square analyses of the possible interactions.
Results
Prior to analyzing the data, some responses were removed. Qualtrics estimated that the survey would take 3 min to complete. We removed any respondent who took 55 s or less, leaving us with 72 respondents. Another six were removed because they answered that they did not drink alcohol. Missing values were filled with the mean of the sample. A Chi-square analysis did not reveal any significant gender differences.
Perhaps not surprisingly, 86 percent of the respondents reported overdrinking, defined as drinking beyond what a person intends to drink, at least “once in a while.” And 30 percent said that this occurred “almost half of the time,” 8 percent reported it happening “almost every time,” and 6 percent said, “every time” (see Figure 1).

Percentage of respondents who reported having a limit in mind when they drink.
There was no relationship between drinking beyond what they intended to drink and most of the other factors, for example, having a limit in mind, trying to cut down, ease of cutting down, with one exception, being surprised when it happened (see below).
A total of 56 percent of the respondents said that they “usually have a limit in mind” if they drink (see Figure 2). A Chi-square analysis performed on the data revealed a significant relationship between those who had a limit in mind and how easy or difficult it was to cut down (χ2(2, N = 66) = 8.60, p = .01).

Percentage of respondents who reported having a limit in mind when they drink.
A total of 51 percent of the respondents reported being surprised the next day that they had overdrunk. When asked whether they were “surprised later that it happened, for example, the next day,” 84 percent answered in the affirmative; 20 percent said that it happened “about half the time,” and 31 percent said that they were surprised either “almost every time” (20%) or “every time” (11%; see Figure 3). A Chi-square analysis performed on these data revealed that those who reported usually having a limit in mind were also often surprised (χ2(2, N = 66) = 7.14, p = .03). However, even a large portion (68%) of those who reported not usually having a limit in mind reported being surprised at least once in a while or more often when they overdrank.

How often respondents reported being surprised that they had overdrunk.
A Chi-square analysis indicated that those who reported drinking more than they intended to drink were also significantly more often likely to be surprised (χ2(4, N = 66) = 10.94, p = .03). Of the 56 respondents who reported drinking beyond what they intended to drink at least once in a while, 50 were surprised “about half the time,” “almost every time,” or “every time.”
It is also interesting that many respondents who answered “yes” to the question regarding whether or not they binge drank or overdrank on purpose (63% of the sample) were also surprised at times when they overdrank, perhaps because they were surprised when they unintentionally overdrank.
A majority (58%) of the respondents said that they had tried to cut down on drinking, “like many people try to cut down on how much they eat.” In trying to do so, 46 percent reported finding it “very difficult” (18%) or “somewhat difficult” (28%; see Figure 4). A Chi-square analysis revealed that respondents who reported trying to cut down on drinking also reported at times purposely binge drinking or overdrinking (χ2(1, N = 66) = 4.44, p = .04). However, there was no relationship between reported trying to cut down and ease or difficulty in trying to cut down.
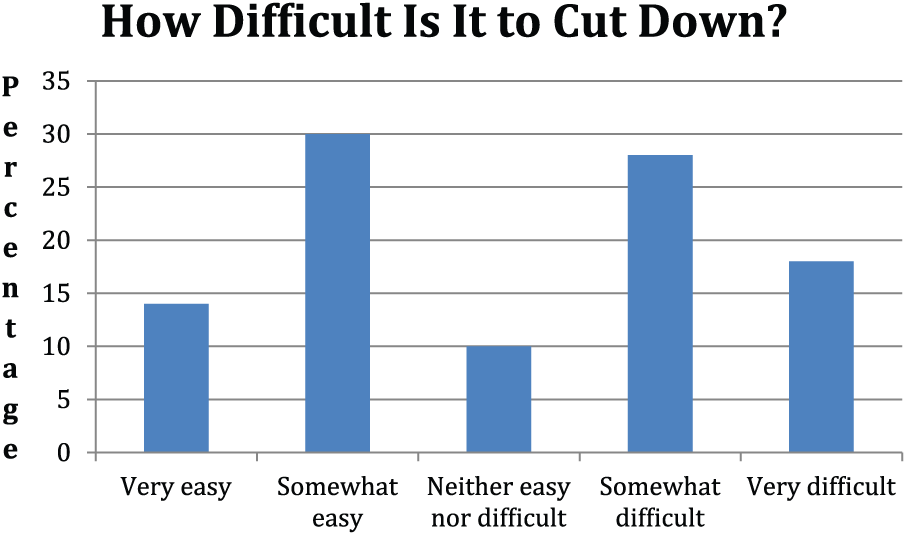
Reported difficulty of cutting down.
If the respondents reported drinking less than in the past, 34 percent reported drinking fewer times per week, 26 percent reported drinking fewer drinks per drinking episode, and 40 percent reported doing both. As noted earlier, a Chi-square analysis did not find any significant gender differences. However, males may use trying to drink fewer drinks per drinking episode more often than females. Finally, if they felt that they were drinking less than in the past, 62 percent thought that that had occurred as they aged, but 38 percent attributed that to having intentionally tried to moderate or stop (see Figure 5).

Method used to cut down.
Discussion
Heavy drinking, excessive drinking, and binge drinking all refer to a standard established by the research community or the Federal Government. They do not refer to what an individual considers “too much.” The data from this study indicate that many drinkers have a limit in mind when they drink and that a large percentage (86%) exceed their limit at least once in a while; 44 percent exceed their limit almost half of the time or more.
Unintentional binging: the surprise factor
A large number of respondents reported being surprised that they had overdrunk; they did not expect to exceed their limit when they started drinking, even though that appears to happen frequently for many of these respondents. Metastability may contribute to the surprise factor in overdrinking considering that human neurology may exhibit metastable properties. A system is said to be metastable when it looks stable but a small change stimulates a subsequent, very large change (Fingelkurts and Fingelkurts, 2004; Outlier and Kelso, 2006; Rabinovich et al., 2008). For example, repeatedly dropping a kernel of rice (the same stimuli) onto a table will eventually create what appears to be a stable pile. But eventually, the addition of just one more grain of rice (the same stimulus again) will create a large change in the pile, that is, an “avalanche” of rice. Then the pile will again appear stable. Neurologically, people may be wired up with two “programs” almost equally set to run. One may be the “not-overdrinking program” and one the “overdrinking program.” But the addition of one more drink—the impact of a bit more ethanol in the prefrontal cortex—causes a rather sudden shift, causing the overdrinking program to become predominant.
Moreover, such a shift is not expected. Hence, many overdrinkers report being “surprised” when it occurs. The surprise may be compounded by the fact that several previous drinking episodes did not result in overdrinking, leading an overdrinker to have a false sense of security; they have conquered the problem. The drinking days without problems make them think that the probability of overdrinking is less and less likely. However, if the system is metastable, the future is far from certain.
Lloyd et al. (2001) have proposed that systems are homeodynamic in contrast to homeostatic. That is, change over time is the norm not the exception, and systems do not necessarily return to their previous, stable position, as homeostasis suggests. They also note that many systems exhibit “bistable switches … as well as chaotic behavior” (p. 133), such that a system may go quite suddenly from one state to another. The manner in which human societies have organized the use of time and the way habits and routines affect human behavior over time may make instances when human behaviors quite dramatically change from one form to another less evident. At the end of a day, however, such changes may occur more frequently. Many people make plans to do an hour or so of work or paying bills after dinner and then quite suddenly “decide” to watch TV or go online. In the case of overeating, they plan not to eat desert, and then eat not just half of what is offered—perhaps their original intention—but the whole serving, and sometimes seconds. In terms of overdrinking, many people plan to have “just two” and then have three or more.
When one considers how people change types of behavior and attempt to maintain those changes, assuming that the system is stable may predispose overdrinkers to more lapses and relapses. This is consistent with West’s proposal that a good theory has to take into account the “inherent unstability” of the human mind (West and Brown, 2013: 9).
Theory-informed smartphone apps
Increasingly, people are using apps and wearables to intentionally try to change various health behaviors. A majority of respondents in this study said that they had tried to cut down, consistent with the extensive research that shows that most drinkers moderate their behavior slowly over time (cf. Lopez-Quintero et al., 2011; Sobell et al., 1996). Reich et al. (2015) found that the respondents from their 18- to 23-year-old sample cut down primarily by reducing the number of times that they binge drank; but when they drank, they did not drink less. Similarly, in a much earlier study (Collins et al., 1998), excessive drinkers reduced their overall consumption, but not the number of drinks per drinking episode. In contrast, in this survey of a broader age group sample, approximately a third of the respondents reported having cut down by drinking fewer times per week, a third by drinking fewer drinks per drinking episode, and a third by doing both.
Research into how difficult drinkers find reducing alcohol misuse does not appear to exist, but many respondents in this study said that they found it somewhat or very difficult to do so. These findings are consistent with what Toneatto et al. (1999) found in their study of untreated former cocaine users; half had found it somewhat or extremely difficult to stop. Research into the dynamics of self-change reflects significant individual differences (Littlefield et al., 2010; Reich et al., 2015; Vergés et al., 2012). Overdrinkers may moderate or stop their behavior very differently from the way alcohol-dependent drinkers do. Witkiewitz et al. (2014), for example, report that non-treatment-seeking heavy drinkers showed more linear forms of drinking behavior change than heavy drinkers who had been in treatment.
How might theory inform the development of an app to help overdrinkers change their behavior? Naslund et al. (2017) argue that all interventions should be theory based, but one meta-analysis found that behavior change techniques (BCTs) based on two prominent theories, social cognitive theory and the transtheoretical model, were not more effective than those not linked to a theory (Prestwich et al., 2014). Kwasnicka et al. (2016) reviewed 100 theories of behavior change maintenance and found considerable overlap but no “integrated theory of behavior change maintenance” (p. 115). All the popular theories appear to have their deficiencies and their critics (Sniehotta et al., 2014; West, 2006) and to date basing interventions on theories has not improved their effectiveness (Prestwich et al., 2014).
Naslund et al. (2017) found four theories as “among the most widely cited models of health behavior, and [that they] have been used extensively to guide successful interventions targeting behaviors including lifestyle habits …” (p. 2): (1) the health belief model, (2) the theory of planned behavior (TPB), (3) the transtheoretical model, and (4) social cognitive theory.
The TPB (Ajzen, 1991) might be an obvious choice for app development, as changing overdrinking behavior may often involve intentional, planned behavior (although some respondents in this study thought that it had just happened over time as they aged). Intentions are central to the TPB. Of the four theories discussed by Naslund et al. (2017), the TPB was cited as using “prompts and motivation strategies to support behavioral intentions, and increase ability by building self-efficacy through encouragement and skill building” (p. 3). Attitudes, perceived behavior control (a combination of self-efficacy and the degree to which you believe you can control the outcome), and subjective norms (what you think others would do and want you to do) all contribute to intentions; according to the theory, intentions are closest in time to the actual behavior. However, not all studies have found a connection of intentions and behavior (Sheeran, 2002) and numerous people have criticized the TPB, although others have acknowledged its key role in the ongoing development of theories (Hagger, 2015).
Some research suggests that implementation intentions are more effective than behavioral intentions alone. Implementation intentions involve an “if-then strategy,” for example, “If it is 4 pm, I will go to the gym” (Armitage, 2016; Gollwitzer, 1999; Hagger and Luszczynska, 2014). In a study of condom use among non-injecting drug users, implementation intentions (“I have detailed plans of what I will say if my partner refuses to use a condom.”) had a greater impact than simple behavioral intentions (“I intend to use a condom.”; Nydegger et al., 2017). As noted earlier, in one study of college-age participants, those who reported intending to limit their drinking over the weekend showed the most responsiveness to the text messaging program over a 12-week period as compared with those who did not intend to limit their drinking (Suffoletto and Chung, 2016). And according to one study, implementation intentions “reduced the capacity of past behavior to predict future behavior” (Orbell et al., 1997: 945).
Armitage (2009), in a study of 248 participants from a broad community sample, ages 18 to 74, found that selecting an experimenter-provided implementation intention worked as effectively as a self-generated implementation. This suggests that a smartphone app that provided implementation intentions might be effective with users. Moreover, one meta-analysis of computer-delivered interventions (CDIs) for excessive alcohol consumption found that prompting commitment to goals and goal reviews resulted in larger effects (Black et al., 2016). Combining implementation intentions with protective behavioral strategies (PBSs) might make an app more effective, for example, “If I am drinking, I will not try to keep up with my friends” and “If I am drinking, I will alternate non-alcoholic drinks” (Borden et al., 2011; Pearson, 2013).
An alternative choice for theory-informed app development might be the temporal self-regulation theory (TST; Cameron, 2010; Hall and Fong, 2010). The TST may be a particularly good fit because it acknowledges the fact that behavior is dynamic and occurs over time. In the case of overdrinking, each episode occurs over time in terms of hours, and the development of chronic overdrinking or the moderation of overdrinking occurs, if it occurs, over months and years. With some exceptions (e.g. Muraven et al., 2015a, 2015b; Reich et al., 2015; Witkiewitz et al., 2014), temporal aspects of behavior change have been relatively ignored by alcohol misuse researchers. TST also focuses on self-regulation, something that many overdrinkers are trying to get better at, even when under the influence of alcohol.
West (West, 2006; West and Brown 2013) reviewed the many theories of motivation and addiction and proposed a synthetic theory of motivation (PRIME). PRIME attempts to synthesize what West hypothesizes are the five key elements of the human motivational system: “plans (conscious mental representations of future actions plus commitment); responses (starting, stopping or modifying actions); impulses/inhibitory forces (can be consciously experienced as urges); motives (can be consciously experienced as desires); evaluations (evaluative beliefs)” (West and Brown, 2013: 195). He then proposes a theory of addiction based on PRIME. As noted earlier, part of the PRIME theory suggests that the human mind is inherently unstable and that this instability (or metastability) may help explain why people may quite suddenly “change their mind” and behave quite differently from how they thought they would behave or had intended to behave. West (West, 2006; West and Brown, 2013) also puts considerable importance on the notion of identity, specifically, in his case, “smoker” and “non-smoker.” A desired identity—“non-smoker” or “someone who does not overdrink”—may play an important role in determining the way plans, evaluations, motives, and impulses/inhibitions ultimately change a behavior pattern, and a study by Montes et al. (2017) suggests that that may be correct for some problem drinkers. Participants who made the transition from problem drinker to non-problem drinker during the 2-year follow-up period had a “7 times greater likelihood of being in a rapidly decreasing heavy drinking latent trajectory class compared with participants who did not make the same transition” (p. 721).
Reducing the surprise factor in unintentional binge drinking
West (West, 2006; West and Brown, 2013) suggests that human behavior may behave somewhat like the weather and that a good theory of addictions should incorporate insights from chaos theory. In a similar vein, Bishop (2016) suggested that an episode of binge drinking is similar to a weather event and proposed a “meteorology-inspired” model to predict binge drinking. Weather theory proposes that specific factors must come together to produce a thunderstorm, tornado, or hurricane. However, in contrast to the behavior of any particular hurricane—which only behaves once and then is gone—the behavior of most humans is relatively recurring, stable and predictable; they behave similarly again and again. Their work and home schedules make that so, and drinking and overdrinking occur mostly at night and, in general, increase from Thursday to Friday to Saturday (Demers et al., 2002; Kuntsche and Labhart, 2012; Wood et al., 2007). Consequently, predicting episodes of overdrinking may actually be easier than predicting the weather, especially for drinkers who are not grappling with a severe AUD. (Persons with a severe AUD may be unemployed and drink throughout the day.) With computers, artificial intelligence, and predictive analytics, hurricane predictions have improved dramatically over the past 20 years.
Given the surprise factor, making overdrinkers more aware of the probability of overdrinking on any given evening—and at moments within the evening—might be very helpful. Factors such as the time of day, day in the week, location, fatigue, and affect could be used to make such predictions (Bishop, 2016). The same or very similar “storm” may occur over and over in a particular individual, unlike real weather systems. A smartphone application could learn and adjust interventions to make an individual aware that a number of factors are coming together, which in the past have made him or her particularly vulnerable. The probability of overdrinking could then be sent to the phone. However, not all weather conditions spawn a tornado; it is a probabilistic situation. Will a particular individual change her behavior based on the prediction? That will probably depend on her intentions and the environmental factors at the time.
SlipBuddy was recently developed to inform overeaters of the distinct patterns in their overeating (Tulu et al., 2017). For example, a special, individualized model was developed for one overeater who tended to overeat when she was tired. A different individualized model was developed for another overeater who tended to overeat when he was frustrated. That is, the smartphone algorithms were adjusted based on what the system had learned about the individual’s behavior over time. Something similar could be developed for individual overdrinkers who probably differ significantly in the unique combination of factors that must coalesce for them to overdrink. Users could be sent something akin to a severe weather alert warning them of the probability of overdrinking that night as well as self-selected and/or self-created micro-interventions designed to help them pursue their goal of less overdrinking.
A-CHESS (Addiction Comprehensive Health Enhancement Support System), a smartphone application for drinkers leaving an inpatient program, has been successfully developed to predict relapse and to send texts to the user and a designated counselor (Gustafson et al., 2014). A-CHESS was developed for people who had been patients in an inpatient, hospital program but could probably be adapted for overdrinkers.
Bae et al. (2017) developed a machine learning model that was able to identify three different types of behavior—non-drinking, drinking, and heavy drinking—96.6 percent of the time outside of a laboratory in a sample of 21- to 28-year-olds using passively collected smartphone data. Their collection of individual historical data such as the average time between keystrokes and travel activity helped improved their predictions. They expect soon to be able to predict drinking episodes; text messages could then be sent in advance that might help the user to prevent or reduce overdrinking.
Limitation and strengths
This pilot study is the first to assess the extent to which drinkers, perhaps frequent binge drinkers, unintentionally drink more than they had intended to drink. It is also the first to report a “surprise” factor in unfulfilled intentions. As discussed above, overdrinking behavior may manifest metastability, reflecting the hypothesized inherent instability of neural networks in the human brain (West, 2006). Helping people anticipate and deter sudden shifts in their behavior, for example, from intended moderate drinking to overdrinking, may reduce the frequency and intensity of overdrinking.
This pilot study is also the first to use Amazon’s MTurk linked to Qualtrics to obtain a broader community sample of drinking behavior. Although MTurk samples and traditional samples may be quite similar, Goodman et al. (2013) found that MTurk workers were lower in self-esteem and less extraverted, characteristics that might be relevant when studying overdrinking. On the other hand, despite the known, widespread prevalence of binge drinking and excessive drinking and the fact that millions change this behavior over time, little is known about how they do it and how they maintain the change. This approach could be used to further investigate which strategies are used to change this very common, risky health behavior and which strategies help to maintain the change.
However, this research did not assess whether being surprised the next day has any effect on subsequent drinking, as suggested by LVE research (Collins, 1993; Muraven et al., 2005a, 2005b). Future research might help determine the extent to which the surprise factor coupled with a possible LVE contributes to overdrinking over time. It also did not ask whether the respondents had ever been diagnosed with an AUD or whether or not they had ever been into treatment for an AUD. Consequently, it is not known how many of the respondents who reported being surprised when they overdrank were also suffering from a moderate or severe AUD.
Despite these limitations, this study suggests a new approach to the problem of binge drinking. The traditional approach of adding controls in the environment, for example, increasing taxes on alcohol, managing the density of bars and stores, and enforcing the age limit and drunk driving laws, may be effective. However, technological help for individuals who do not want to overdrink may add another important component to managing this costly and increasing problem.
Conclusion
Smartphone apps may be ideal for decreasing overdrinking and the prevention of AUDs for many reasons: (1) younger people use smartphones much more than older people, and the intensity of officially defined binge drinking is much higher in younger people (9.3 drinks per episode in the 18–14 age group) than in older people (5.7 drinks per episode in the 65+ age group; CDC, 2012); (2) men are much less likely to seek counseling or therapy than women (Parent et al., 2018) but binge drink far more frequently than women (5.0 per month and 9.0 drinks per occasion vs 3.2 times per month and 5.9 drinks; CDC, 2012); (3) apps are increasingly being used for self-care purposes and all adult-age groups binge drink: 28.2 percent of the 18–24 age group; only 3.8 percent of the 65+ age group report binge drinking, but they do so more frequently than any other age group (5.5 times per month vs an average of 4.0 times per month for the other age groups; CDC, 2012). Currently and in the past, most treatment efforts have been focused on persons with severe AUDs and who are in treatment. More attention needs to be given to the millions of overdrinkers who contribute to approximately 3.1 million alcohol-related deaths worldwide each year (WHO, 2014). Little help has been available for them. This pilot study suggests that much overdrinking may be inadvertent and unintentional and surprise the overdrinker. Smartphone apps could help overdrinkers be more aware of the probability of unexpected shifts in drinking behavior and help them change their overdrinking behavior more rapidly and earlier in their lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.