
Abstract
This study aimed to investigate the mediating role of spiritual health in the relationship between ego-strength and adjustment to heart disease. In total, 327 patients with coronary artery disease (138 women, 189 men) completed the Ego-Strength Scale, Adjustment to Illness Scale, and Spiritual Well-Being Scale. Results showed that both ego-strength and spiritual health had a significantly positive correlation with adjustment to heart disease. Results also revealed that spiritual health mediated the relationship between ego-strength and adjustment to heart disease. More improvement in adjustment to heart disease requires more improvement in patients’ spiritual health as well as to ego-strength.
Introduction
Cardiovascular diseases are the leading cause of death all over the world (Mozaffarian et al., 2016). In 2008 over 17 million people died of these illnesses, over 3 million of which occurred under the age of 60, a phenomenon which is largely preventable (Mendis et al., 2011). Cardiovascular diseases, when chronic, often come with more mental and physical stress (Marin et al., 2009). These illnesses require pharmacological treatments as well as following long-term diets in order to be controlled. Progressive physical disability is the common characteristic of these illnesses. Therefore, these diseases induce profound changes in a person’s life, resulting in negative effects on his quality of life and well-being (De Ridder et al., 2008). Accordingly, after illness diagnosis, patients are confronted with new situations that challenge their habitual coping strategies. As a result, they must find other coping ways for adjustment to such conditions (Taylor and Aspinwall, 1996).
Adjustment to illness can be viewed as the process to maintain a positive view of the self and the world in the face of a physical problem (Sharpe and Curran, 2006). Several models explain how patients could achieve adjustment. These include cognitive adaption theory, which emphasizes acceptance and understanding of mastery over an illness (Taylor, 1983). Another is personality model, which emphasizes the role of personality factors like optimism or neuroticism in adjustment, and stress and coping model that emphasizes strategies used by patients to deal with adaptive tasks imposed through diseases (Adler and Matthews, 1994). Based on stress and coping model, a chronic disease is composed of many challenges and emphasizes appraisal process and coping that explains the difference in patients’ performance in their adaptive tasks. This model emphasizes the patient’s role in adjustment to stresses. This model has been clarified by a self-regulation model in recent years (Sharpe and Curran, 2006). According to personality model concerning adjustment to illness, one can predict that ego-strength as a personality characteristic (Besharat, 2016; Besharat et al., 2014, 2015) is associated with adjustment to disease (Hyphantis et al., 2008; Koochaki-Ravandi et al., 2015; Settineri et al., 2012; Teimourpour et al., 2015).
Ego-strength points to a person’s view of his problem, his typical reaction to distress, and his adaptive ability in an emotional situation (Besharat, 2016; Settineri et al., 2012). In other words, ego-strength indicates ego effectiveness in regulating motivations and impulses and adjusting to environment (Singh and Anand, 2015). Ego-strength is a variable that can predict adaptability (Symister and Friend, 2003) because it represents the extent of ego effectiveness in doing adapting task with environmental demands. In a healthy mind with a suitable function, there is a consistency among its id, ego, and superego and ego-strength helps in emotional balance maintenance while waiting or working for achieving more improvement (Engler, 2014). Block and Block (1980) introduced two main characteristics as two ego-strength components: ego control and ego resilience. Ego control is the ability of the change in ego responses and placing them along with standards such as ideals, values, social expectations, and supporting them for achieving long-term goals. Ego resilience is an inner psychological characteristic and affects an individual’s response to stressful factors. People with higher ego resiliency adapt more quickly, have an ability to plan long-term goals, recover from harms faster, and, while confronting them, become less anxious and frustrated. Ego control and ego resilience indicate maturity, capability, and impact adjustment ability to environmental and personal demands (Block and Block, 1980). Ego-strength reflects the related style of playing professional and family roles and considered as personal and social functions (Frederick, 2013). In psychotherapy, the concept of ego-strength points to individuals’ ability in ego identity maintenance, apart from the existence of mental sadness, pain, distress, and conflict between inner needs and outer demands (Frederick, 2013).
People with strong ego-strength struggle toward self-realization and individuality achievement and meanwhile admit their dependence on others. They accept conflicts, respect the individuality and reality of their existence, and avoid any blind adherence (Markstrom and Marshall, 2007). Research findings (Besharat et al., 2015; Carver and Scheier, 2016; Folkman, 2008; Jamil et al., 2015; Kim and Park, 2016; Loevinger, 1998; Settineri et al., 2012) have confirmed the relationship between ego-strength and general health. Although preliminary studies on resilience and heart disease have shown that patients with higher levels of resilience showed better recovery in patients with coronary heart disease (Chan et al., 2006) and acute coronary syndrome (Arrebola-Moreno et al., 2014), there is a dearth of research specifically on the relationship between ego-strength and adjustment to heart disease. Given the role of ego-strength in general health, one purpose of this study was investigating the relationship between ego-strength and adjustment to heart disease. However, there is this pressing question: Is the relationship between ego-strength and adjustment to illness a simple one or other psychological variables might have a role in the relationship between them? Accordingly, the other aim of this study was to investigate the mediating role of spiritual health in the relationship between ego-strength and adjustment to heart disease.
Spiritual health is a capability that provides a consistent and integrated relationship between intrapsychic forces and results in stability in life, peace, consistency, and feeling of close relationship with self, God, society, and environment (Craven and Hirnle, 2003). Spirituality is a vital and integrating force in life that helps an individual achieve more balance in physical, mental, and social well-being (Young and Koopsen, 2010). Spirituality is relevant to personal awareness of existence and experience of feeling and inner beliefs, which give meaning, value, and purpose to life and, in this way, make it possible for a person to be in peace with self, God, and others as well as achieving consistency with environment (Fisher, 2010). Spirituality is a concept beyond religion and religious adherence, because it is an effort for being meaningful and purposive in life, even for those who do not believe in God (Richardson, 2014; Torskenæs et al., 2013). World Health Organization defines spiritual health beyond biological, psychological, and social dimensions of health and emphasizes its effects on people’s general health and happiness (Strawbridge et al., 1997). Biopsychosocial–spiritual model considers the whole existence of a person (Beng, 2004; Sulmasy, 2002) and forces health professionals to take the whole existence of a person into account. Therefore, human being may be a multi-dimensional being that all these dimensions are connected. A disease by causing a disorder in bio dimension affects other dimensions and that is why a comprehensive care must consider all the dimensions and the relation among them (Richardson, 2014).
Spirituality, medicine, and health have always been in relation with each other (Koenig et al., 2012). Illness, suffering, and facing death represent an inevitable experience for everyone and spirituality could play an important role in the process of confrontation and adjustment to these experiences and recovery from diseases (Walton, 1999). Spirituality improves capability coping with a disease and recovery speed (Sacco et al., 2014; Unantenne et al., 2013). Accordingly, some researchers believe that in the process of a patient’s treatment it is necessary to consider the patient as a whole and from all the aspects. If only the physical disease is taken into account, the recovery process will be interrupted (Koenig, 2000). On the whole, various studies emphasize the role of spirituality and its importance in a person’s physical and mental health (Ballew et al., 2012; Bonelli and Koenig, 2013; Heydarzadegan and Koochakzaei, 2015; Koenig, 2009; Koenig et al., 2012; Liu et al., 2011), as well as in clinical outcomes (Delaney et al., 2011; Dubois et al., 2012; Naghi et al., 2012). Religion and spirituality could prevent depression, frustration, self-harm, and suicidal tendencies (Bonelli and Koenig, 2013; Miller et al., 2012), simplify negative emotion regulation (McCullough and Willoughby, 2009), and help the person as a source of relaxation in distressed times (Pargament et al., 2000). Therefore, spirituality might be related to and influenced by ego-strength. This is another gap calling for further investigation.
On the other hand, spirituality could influence adjustment to disease. As one of the determining aspects of health helping the individual to cope with stressful conditions in life, spiritual health can lead to many physical and mental improvements (World Health Organization, 2013). Preliminary evidence indicated that spiritual health and spirituality may result in changes in quality of life (Beery et al., 2002), rehabilitation (Nadarajah et al., 2013), indices of various physiological disturbances (Morris, 2001), and outcomes of psychological interventions (Warber et al., 2011) in patients with coronary heart disease. However, controversial results are also reported (Blumenthal et al., 2007; Delaney et al., 2011).
To address previously mentioned gaps and shed light on existing research findings, we predicted that spiritual health could affect the relationship between ego-strength and adjustment to heart disease. The main purpose of this study was to investigate the mediating role of spiritual health in the relationship between ego-strength and adjustment to heart disease. We tested our research hypotheses in the following manner: (1) there is a positive correlation between ego-strength and adjustment to heart disease; (2) there is a positive correlation between spiritual health and adjustment to heart disease; (3) spiritual health has a mediating role in the relationship between ego-strength and adjustment to heart disease. Findings of interactions between ego-strength, spiritual health, and adjustment to heart disease may have an incremental contribution to the existent literature and help empirical understanding of the process of adjustment to illness. Moreover, the findings can help health theories incorporating such variables into the psychotherapeutic approaches for health professionals.
Method
Participants and procedure
This research is a descriptive study. The statistical population of the study was cardiovascular patients. In total, 327 cardiovascular patients (189 men (58%), 138 women (42%)) participated in this study. The participants were recruited among patients who referred to Afshar Hospital in Yazd/Iran by physicians. The sampling method was purposive considering entering from the mentioned population. The inclusion criteria were suffering from cardiovascular disease, being literate, not suffering from other serious medical diseases except coronary artery disease, not suffering from a major psychiatric disorder, and not having substance dependence.
The study was approved by Department of Psychology and University of Tehran ethics under grant number 5106003/1/65. Upon hospital management approval and support, necessary data collection about cardiovascular diseases commenced by consulting with cardiovascular specialists. All participants signed an informed consent document prior to performing the research procedure. After explaining the subject and the purpose of the research to the participants and expressing their tendency, they completed the questionnaires. Furthermore, assurance was given on the confidentiality of results. The participants’ age ranged from 31 to 63 years (M = 52.39 years, standard deviation (SD) = 6.23). The mean of marital duration was 28 years (SD = 9.12), and the mean of disease duration was 2.38 years (SD = 1.75). Of the participants, 35 percent (N = 115) were business professionals, 14 percent (N = 46) were employees, 15 percent (N = 50) were retired, 40 percent (N = 114) were unemployed, and .6 percent (N = 2) left their job status unknown. And 11.5 percent (N = 38) had elementary education, 34.5 percent (N = 112) had junior high school education, 31 percent (N = 101) held a high school diploma, 6 percent (N = 20) held an associate’s degree, 11.5 percent (N = 37) had a bachelor degree, 4 percent (N = 12) had a master or doctorate degree, and 1.5 percent (N = 7) left their educational status unknown. Economic status of the participants revealed that 27.5 percent (N = 90) had a low level of economic status, 58.5 percent (N = 191) had a middle level, 13 percent (N = 42) had a high level, and nearly 1 percent (N = 4) left their economic status unknown. The participants completed the research questionnaires as follows.
Measures
Ego-Strength Scale
The Ego-Strength Scale (ESS; Besharat, 2016) consists of 25 items validated to measure the power of ego in controlling and managing difficult life situations and conditions. All items are rated along a 5-point Likert-type scale ranging from 1 (not at all) to 5 (very much). Psychometric properties of the ESS have been assessed and confirmed in several studies in both clinical (n = 372) and general population (n = 1257) groups (Besharat, 2016). The ESS consists of five subscales including ego control, ego resiliency, mature defense mechanisms, problem-focused coping strategies, and positive emotion-focused coping strategies. All subscales were internally consistent in this study. Cronbach’s alpha coefficients ranged from .73 to .91.
Adjustment to Illness Scale
The Adjustment to Illness Scale (AIS; Besharat, 2005) is a 12-item self-report questionnaire developed to measure adjustment to medical diseases in a 7-point Likert-type scale from 0 (strongly disagree) to 7 (strongly agree). Higher scores represent higher levels of adjustment to illness and involving in daily-life activities despite experiencing and enduring stresses and limits caused by illness. Psychometric properties of the AIS have been confirmed in samples of clinical groups with medical diseases (Besharat, 2005). Cronbach’s alpha coefficient was .79 in this study.
Spiritual Well-Being Scale
The Spiritual Well-Being Scale (SWBS; Ellison, 1983; Paloutzian and Ellison, 1982) consists of 20 items and assesses the perceived spiritual life quality in a 6-point Likert-type scale from 1 (strongly disagree) to 6 (strongly agree). The SWBS measures spiritual health in two aspects including religious well-being (RWB) and existential well-being (EWB). Higher scores indicate higher levels of well-being and spiritual satisfaction (Utsey et al., 2007). Several studies have supported psychometric properties of the SWBS (Bufford et al., 1991; Genia, 2001). Cronbach’s alpha coefficients were .91 for RWB and .87 for EWB in this study.
Results
The means and SDs for the research variables including adjustment to heart disease, religious health, existential health, and ego-strength are presented in Table 1.
Mean scores and standard deviations on each variable of the adjustment to heart disease, religious well-being, existential well-being, and ego-strength for men, women, and the total sample.

SD: standard deviation.
Bivariate correlation coefficients between variables are presented in Table 2. The significant associations provide support for the correlational hypotheses (p < .01).
Zero-order correlations between adjustment to heart disease, religious well-being, existential well-being, and ego-strength for the total sample.
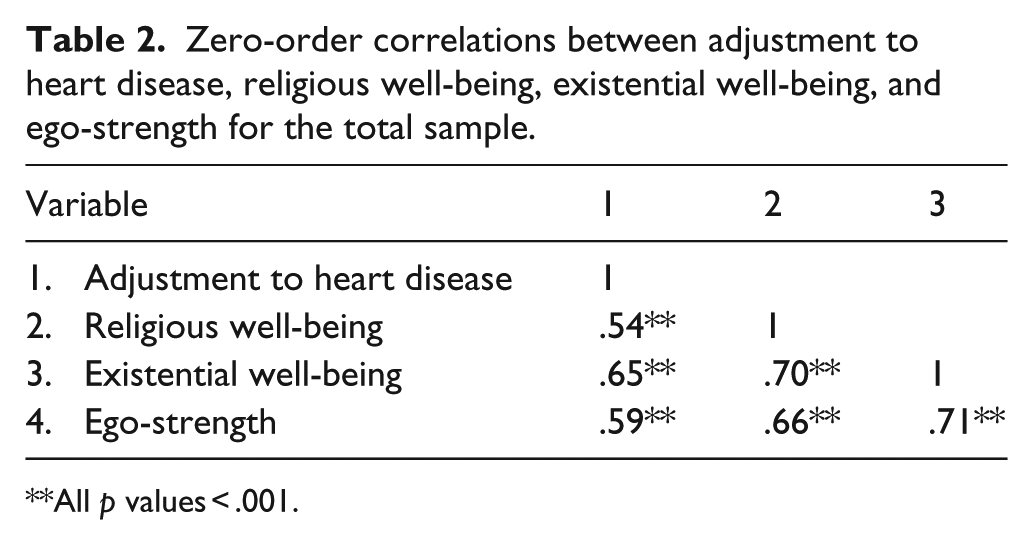
All p values < .001.
In order to investigate the mediating role of spiritual well-being in the relationship between ego-strength and adjustment to heart disease, path analysis was performed. It was assumed that the relationship between ego-strength and adjustment to heart disease is moderated by spiritual well-being components, that is, existential and religious health. Figure 1 shows standardized path coefficients for the hypothesized model. According to the results of path analysis, the coefficients of all paths were significant.

Standardized path coefficients on the mediating role of spiritual health in the relationship between ego-strength and adjustment to heart disease.
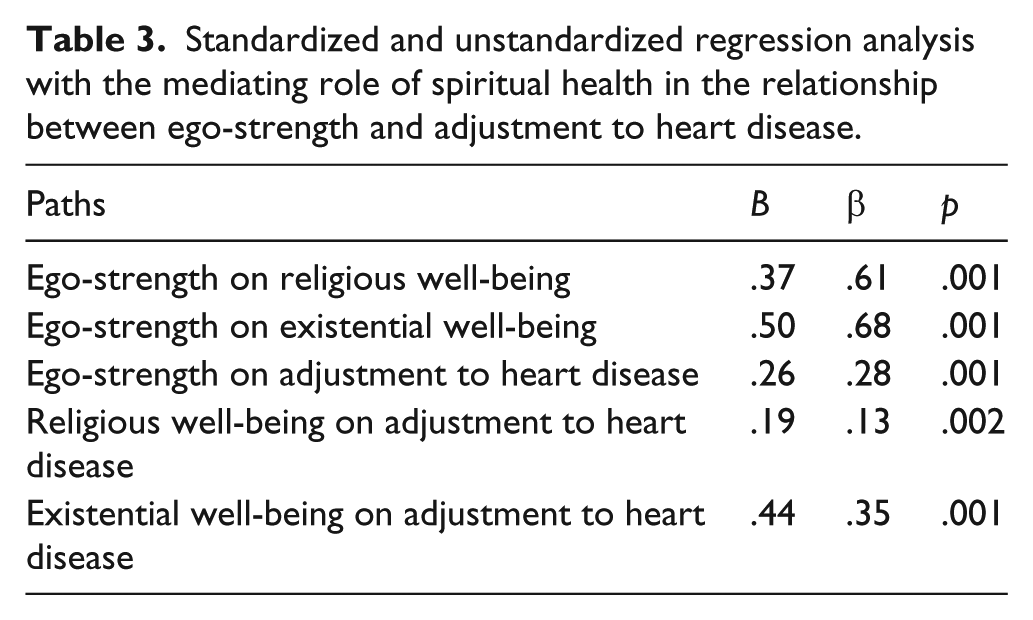
Standardized and unstandardized direct path coefficients of the hypothesized model are presented in Table 3. The indirect effect of ego-strength on the adjustment to heart disease was statistically significant (β = .31, p < .01).
Standardized and unstandardized regression analysis with the mediating role of spiritual health in the relationship between ego-strength and adjustment to heart disease.
Fit indices of the hypothesized model are presented in Table 4. The Chi-square and the Chi-square over degrees of freedom (χ2/df) are not statistically significant. Lower values of χ2/df are indicative of better fit (<4 is considered to be acceptable). The root mean square error of approximation (RMSEA) value close to .06 is indicative of good fit. The goodness-of-fit index (GFI), adjusted goodness-of-fit index (AGFI), comparative fit index (CFI), and normed fit index (NFI) values are desirable.
Fit indices of the mediating role of spiritual health in the relationship between ego-strength and adjustment to heart disease.

RMSEA: root mean square error of approximation; AGFI: adjusted goodness-of-fit index; CFI: comparative fit index; NFI: normed fit index.
Discussion
Ego-strength is considered as a set of psychological abilities to resolve intrapsychic conflicts and environmental demands (McCrae and Costa, 2005). The strength of ego would, therefore, help one cope with stressful situations such as struggling with a heart disease. Examining the power of ego with regard to patient adjustment to heart disease was the first aim of this study. This study also aimed to find out whether the relationship between ego-strength and adjustment to heart disease is mediated by spiritual health.
This study presented a hypothetical model to examine the mediating role of spiritual health in the relationship between ego-strength and adjustment to heart disease. The results of this study showed that ego-strength had a significant positive correlation with adjustment to heart disease. This result is in line with the findings of previous research concerning the relationship between ego-strength and adjustment to infertility (Teimourpour et al., 2015), irritable bowel syndrome (Koochaaki-Ravandi et al., 2015), hemodialysis (Settineri et al., 2012), and multiple sclerosis (Hyphantis et al., 2008) and could be explained according to several possibilities. Levels of ego-strength are determined by a collection of one’s psychological abilities for resolving intrapersonal as well as interpersonal conflicts (McCrae and Costa, 2005) including ego control, ego resiliency, defense mechanisms, and coping strategies (Bellak et al., 1973; Besharat, 2016). Each of these characteristics helps an individual somehow cope with problems, resolve the problems, preserve sense of integrity, and above all achieve a higher level of development. Accordingly, the main function of ego-strength is providing one’s intra- and interpersonal facilities to cope with stresses and environmental demands (Besharat, 2016; Kim and Park, 2016; Settineri et al., 2012; Singh and Anand, 2015; Symister and Friend, 2003). Should we consider a heart disease as one of the stress factors and environmental demands (De Ridder et al., 2008; Marin et al., 2009) then ego-strength can help a patient be better adjusted to disease process and recovery through proper levels of ego control (Baumeister et al., 2007; Besharat, 2016; Block and Block, 1980) and ego resiliency (Besharat, 2016; Block and Block, 1980; Cramer, 2012). These characteristics may help the patient using more efficient coping strategies (Besharat, 2016; Carver and Scheier, 2016; Folkman, 2008; Obegi and Berant, 2010) as well as more mature defense mechanisms (Besharat, 2016).
The results of this study showed that spiritual health had a significant positive correlation with adjustment to heart disease. This result is in line with the findings of previous research confirming the role of spirituality and its importance in physical and mental health (Ballew et al., 2012; Beery et al., 2002; Bonelli and Koenig, 2013; Heydarzadegan and Koochaakzaei, 2015; Koenig, 2009; Koenig et al., 2012; Liu et al., 2011; Morris, 2001; Nadarajah et al., 2013; Warber et al., 2011). There are several possible explanations clarifying these results. Spirituality and spiritual well-being help an individual achieve more biological, psychological, and social balance by the power of integrating one’s relationship with different life aspects (Fisher, 2010; Young and Koopsen, 2010). This integration increases the person’s strength of acceptance and adaptation to serious life-threatening conditions such as heart disease and will result in the person’s more adjustment to the illness. Spirituality improves the strength of adjustment to disease and recovery speed through relaxation (Pargament et al., 2000). It also leads to improvement in patient’s strength in simplification of negative emotion regulation (McCullough and Willoughby, 2009), making coping strategies with disease efficient (Sacco et al., 2014; Unantenne et al., 2013; Walton, 1999), and preventing from expanding negative emotions such as depression and frustration (Miller et al., 2012; Sacco et al., 2014).
The path analysis results showed that spiritual health had a mediating role in the relationship between ego-strength and adjustment to heart disease. According to personality model of adjustment to disease (Adler and Matthews, 1994), it can be predicted that ego-strength as one of the personality determinants (Besharat, 2016; Besharat et al., 2015) may increase both the person’s strength in environmental management (Singh and Anand, 2015) and adaptability (Symister and Friend, 2003). These abilities may in turn provide the individual with a higher level of adjustment (Besharat, 2016; Bonanno, 2004; Richardson, 2002; Settineri et al., 2012). This collection of components and functions of ego-strength equals the individual’s ability to maintain ego identity as well as self-fulfillment and self-actualization (Markstrom and Marshall, 2007), apart from the existence of mental sadness, pain, and conflict between inner needs and outer demands (Frederick, 2013). Accordingly, a sense of spirituality may be developed and/or increased by ego-strength, a sense that can bring the person about feelings of peace and consistency with her/himself, God, others, and the environment (Fisher, 2010). Such feelings might also function as an integrative power ending in physical, psychological, and social balance (Young and Koopsen, 2010). Therefore, ego-strength may improve the levels of adjustment to disease through reinforcement, formation, and continuity of spiritual health.
This study has several limitations. First, the cross-sectional design of the study prevents an understanding of the exact nature of the relationships, particularly with respect to directionality. Second, the sampling method was based on volunteer participation and limited to one hospital. Therefore, one should exercise caution when generalizing the findings. Third, lack of comprehensive control over patients’ demographic variables, life styles, daily stresses, food diets, and weights may have a confounding influence on the study results.
In summary, the results of this study provided preliminary support for the ego-strength model of adjustment. Ego-strength characteristics including ego control, ego resiliency, coping strategies, and defense mechanisms (Besharat, 2016) highlighted the role of personality and coping in adjustment to heart disease. Insertion of the main components of ego-strength in treatment schedules of medical patients, which based on research evidence (Baumeister et al., 2007; Besharat, 2016; Block and Block, 1980; Carver and Scheier, 2016; Cramer, 2012; De Ridder et al., 2008; Folkman, 2008; Marin et al., 2009) improves speed, quality, and quantity of the recovery, is considered as one of the achievements of this study. The findings can also help personality as well as stress and coping models (Adler and Matthews, 1994) incorporating such variables into the treatment and adjustment to heart disease. The mediating results of this study lend support to the biopsychosocial–spiritual model of care (Beng, 2004; Sulmasy, 2002) as well as the palliative care model (Long, 2011; Richardson, 2014), emphasizing the importance of spirituality in health care system. Ego-strength can help people through integrating psychological and spiritual well-being, either religious or existential, leading to meaning in life, peace of mind, hope, happiness, and enlightenment. The results of this study require health care professionals to recognize spiritual and religious concerns as well as attention to spiritual needs in order to help patients a better adjustment to heart disease.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the financial support of University of Tehran for this research under grant no. 5106003/1/65.