
Abstract
This study examines the importance of four psychosocial factors—personality, cognitive appraisal of quality of life, social support, and current reserve-building—in predicting treatment burden in chronically ill patients. Chronically ill patients (n = 446) completed web-based measures. Structural equation modeling was used to investigate psychosocial factors predicting treatment burden. Reserve-building activities indirectly reduced treatment burden by: (1) reducing health worries appraisals, (2) reducing financial difficulties, (3) increasing calm and peaceful appraisals, and (4) increasing perceived social support. These findings point to key behaviors that chronically ill people can use to attenuate their treatment burden.
Introduction
People with chronic health conditions experience burden not only from their illness, but also from their ever-expanding healthcare regimens required for self-management. These regimens can include taking medication, keeping medical appointments, as well as monitoring health, diet, and exercise (Gallacher et al., 2011; May et al., 2009). This workload of healthcare and its impact on patient functioning and well-being is known as “treatment burden” (Eton et al., 2015). It can trigger a spiral of negative consequences, such as non-adherence to prescribed treatments and poor self-care (Durso, 2006; Graves et al., 2007; Haynes et al., 2002; Karamanidou et al., 2014; Kunt and Snoek, 2009; Vijan et al., 2005). Non-adherence to necessary care can lead to worse clinical outcomes (e.g. more hospitalizations and higher mortality (Ho et al., 2006; Rasmussen et al., 2007) and poor quality of life (QOL) (Anderson et al., 2004; Boyd et al., 2014; Brod et al., 2009; Jowsey et al., 2012; Pifferi et al., 2010). The conceptual model of treatment burden comprises the work patients must do to care for their health, the challenges and stressors that exacerbate the felt burden, and the impacts of burden (Eton et al., 2015). These impacts of burden include behavioral, cognitive, physical, and psychosocial well-being (Eton et al., 2012).
While treatment burden is relevant to people with one chronic illness, it is even more significant in the context of having multiple chronic conditions. Current estimates suggest that one in four American adults have multiple chronic conditions (Anderson, 2010; Ward and Schiller, 2013), a prevalence that has risen in the past decade and is projected to continue rising by >1 percent per year until 2030 (Centers for Medicare and Medicaid Services, 2012; Freid et al., 2012; Yoon et al., 2014). Cost implications are profound. About 66 percent of total healthcare spending in the United States is directed at the 27 percent of Americans with multiple chronic conditions (Anderson, 2010). People with multiple chronic conditions account for 96 percent of all Medicare spending (Anderson, 2010). Individuals with multiple chronic conditions pay more for prescription drugs and have higher out-of-pocket healthcare costs (Anderson, 2010), in addition to reporting generally worse health-related QOL compared to people with only one chronic condition (Rothrock et al., 2010).
People with multiple chronic conditions are especially vulnerable to feeling treatment burden as they are often required to engage in a complex array of self-care activities to maintain health (May et al., 2009). Older adults with five or more conditions must fill an average of 50 prescription medications, see 14 different physicians, and make 37 physician office visits every year (Warshaw, 2006). Older multimorbid adults (≥65 years) who report greater difficulty performing prescribed healthcare tasks experience lower mental and physical well-being and have less confidence in their ability to self-manage their conditions (Boyd et al., 2014). Care demands may increase in intensity with each new diagnosis: management protocols add more medications, tests, and medical appointments to the self-care regimen, thereby further straining personal resources and capacity (Bayliss et al., 2003; May et al., 2009). Demands are amplified if the various health conditions require specialized care from multiple providers (Boyd and Fortin, 2010; Sav et al., 2013a, 2013b; Vogeli et al., 2007b). People with multiple chronic conditions report receiving conflicting medical advice from different providers, duplication of medical tests, and more services. Hence, care for this population is often fragmented and poorly coordinated (Benjamin, 2010; Vogeli et al., 2007; Wolff et al., 2002). All of these complex demands have substantial impacts on patients’ behavioral, cognitive, physical, and psychosocial well-being.
It would be useful to understand what individual patients can do to reduce their treatment burden impact. For example, do psychosocial factors influence treatment burden impact? If so, are they modifiable behavioral factors? How much of treatment burden impact is due to stable characteristics of the individual that are less amenable to behavioral intervention? Such an understanding might not only help providers to improve the QOL for individuals living with multiple chronic illnesses. It may also indirectly reduce treatment costs by stopping a negative feedback loop whereby patients who have substantial treatment burden adhere less well to their (multiple) treatment regimens, thereby having more hospital admissions, worse clinical outcomes, and higher mortality rates (Eton et al., 2015).
In considering what psychosocial factors might influence treatment burden impact, it is worthwhile to consider those factors that have been found to be relevant to health outcomes more generally. Such factors would likely be pertinent since treatment burden impact is the QOL impact of the work related to treatments. A growing evidence base suggests that four domains of psychosocial factors have notable relevance to health outcomes. Personality has been shown to have direct relevance to how people deal with symptoms (Malouff et al., 2005) and what coping strategies they employ to deal with illness, treatment side effects, and prognostic estimates (Connor-Smith and Flachsbart, 2007). For example, people with high neuroticism scores tend to report more physical (Costa and McCrae, 1987) and mental health symptoms (Campbell-Sills et al., 2006) and to fare more poorly with the healthcare system (Singh et al., 2010). In contrast, people high in conscientiousness tend to be more adherent to treatment regimens (Christensen and Smith, 1995) and thus have better health outcomes (DiMatteo et al., 2002; Hill and Roberts, 2011). It is unknown how personality relates to treatment burden.
Cognitive appraisal processes refer to differences in the ways people think about QOL, including frame of reference, standards of comparison, sampling of experience, and combinatory algorithm (i.e. patterns of emphasis). These differences in QOL appraisal have been found to be relevant to adapting to illness, both in cross-sectional comparisons and over time (Li and Rapkin, 2009; Rapkin and Schwartz, 2004; Schwartz et al., 2017a). QOL outcomes tend to be better among people who emphasize more positive and personally controllable aspects of their circumstances (Finkelstein et al., 2017; Li and Rapkin, 2009; Schwartz et al., 2013b), such as focusing on the positive, downplaying negative experiences, emphasizing independent problem-solving, and avoiding comparing oneself to others (Schwartz et al., 2013b). Recent work has documented that resilient people employ different appraisal processes than non-resilient people, and these processes differ for physical and emotional outcomes (Schwartz et al., 2017b).
A third relevant domain is social support. A large body of research has documented the positive association of social support and health outcomes (Berkman and Glass, 2000; Uchino, 2006), such that people who enjoy companionship are happier and have better marriages when they share companionship with their spouse (Crawford et al., 2002). People who have more instrumental and emotional support fare better with adversity in health or other vicissitudes in life circumstances (Penninx et al., 1998; Thoits, 1986). Given its relevance to health outcomes in general, any investigation of psychosocial factors relevant to treatment burden should at a minimum consider social support.
Less well understood but equally plausible, a fourth domain that may be important for treatment burden is reserve-building activities. A recent report from the National Academy of Sciences’ Institute of Medicine (2015) noted that people who maintained cognitive acuity into old age were physically active, socially engaged, and got enough sleep, while managing chronic conditions such as diabetes and high blood pressure. Building on work with leading neuroscientists, psychiatrists, and brain health experts, the report notes that cognitive decline is not inevitable with aging, even in the context of multiple chronic conditions. Thus, in order to survive and thrive despite the stress of illness, people remain engaged in life by having enjoyable and stimulating leisure activities, such as reading, singing in a choir, or going for walks.
Early research was limited to a focus on cognitive reserve (Stern, 2002), measured as pre-morbid educational attainment and cognitive performance (e.g. processing speed and memory) (Stern, 2007). However, more recent work indicates that reserve-building activities—personally enriching activities spanning intellectual, cultural, hobby, physical, and spiritual pursuits—may build and maintain brain health (Schwartz et al., 2016a, 2016b). Support for this notion comes from cross-sectional associations with better physical and mental health and neurocognitive function (Schwartz et al., 2013c), and longitudinally with lower levels of disability progression (Schwartz et al., 2013a). While both past and current reserve-building activities contribute to these outcomes, evidence suggests that current rather than past activities are more strongly associated with these outcomes, both cross-sectionally and over time (Schwartz et al., 2013c, 2017a). Hence, enhancing the frequency of these activities could shore up personal resilience in dealing with chronic illness (Schwartz et al., 2016a, 2016b).
Qualitative work suggests that engaging in reserve-building activities may help multi-morbid patients lessen their perception of treatment burden (Ridgeway et al., 2014). Several people noted that they do things to “keep their spirits up” like participating in hobbies, spending time outdoors, spending time with family/friends, and turning to spirituality and faith (Ridgeway et al., 2014). Thus, while it would be easy to assume that people with multiple conditions who experience treatment burden do not have time for reserve-building activities, our qualitative evidence would suggest that this is not the case. Furthermore, such activities were reported by people with high and low formal educational attainment, and by Whites and non-Whites alike.
This study seeks to examine predictors of treatment burden in a heterogeneous sample of people with chronic illness. We sought to evaluate the relationship between treatment burden impact and the following psychosocial factors: personality, appraisal processes, social support, and current reserve-building activities. It was hypothesized that appraisal variables would mediate the relationship between reserve-building activities and treatment burden impact. It was also expected that the treatment burden impact would be greater for people with more comorbidities rather than one particular medical condition. This expectation is based on the qualitative research that suggests that juggling multiple and diverse treatment regimens for multiple chronic conditions leads to the greatest perceived treatment burden and impact (Eton et al., 2015, 2017).
Methods
Sample
Eligible participants were 18 years of age or older, and able to complete an online questionnaire. Participants were recruited from panels that include patients and caregiver panelists from a heterogeneous grouping of chronic health conditions (Rare Patient Voice) and cancer (WhatNext). The panel participants were recruited in-person at conferences and gatherings of disease-specific organizations, and were screened to have the disease or be a caregiver of someone with the identified index condition (Rapkin et al., 2017).
Procedure and design
A web-based survey was administered using the Health Insurance Portability and Accountability Act (HIPAA)-compliant, secure SurveyGizmo engine (www.surveygizmo.com). Email invitations were sent to panel members using their standard protocol for notifying panel participants of study opportunities. We followed study procedures described by Dillman’s Tailored Design Method (Dillman et al., 2014). The survey began with an informed consent form that participants endorsed prior to completing the questionnaires. The study was reviewed and approved by the New England Review Board (NEIRB#15-254).
Measures
Treatment burden was assessed using the role activity limitations (6 items) and physical/mental exhaustion (5 items) scales of the Patient Experience with Treatment and Self-management (PETS) (Eton et al., 2017). These scales have been found to be reliable and valid in a diverse patient sample with multiple chronic conditions (Eton et al., 2017) (α = 0.94 and 0.92 in the current sample, respectively). Cognitive appraisal processes using the Brief Appraisal Inventory (Rapkin et al., 2017), a 23-item Likert-type-scale measure that describes individual differences in what respondents think about when completing a QOL measure. This measure yields five component scores based on principal components analysis: health worries; independence and interpersonal; accomplishing goals and problem-solving; and calm peaceful active; and spirituality and altruism (Rapkin et al., 2017). Personality was measured using the
Statistical analysis
Reducing the number of predictors in structural equation model
Prior to conducting structural equation model (SEM) analysis, we sought to reduce the number of variables in the SEM. We thus examined Pearson’s correlations among the PETS scales and the above-mentioned measures and removed scales that were uncorrelated with the PETS.
A bifactor model of treatment burden impact
We began by examining the factor structure of the two PETS scales to evaluate the feasibility of using a single latent variable to represent treatment burden impact. Treatment burden impact was operationalized using a bifactor methodology (e.g. Gibbons and Hedeker, 1992; Holzinger and Swineford, 1937). In a bifactor model, factor loadings on the single general factor reflect the magnitude of relationships between all the variables (e.g. role and activity limitations items; and physical and mental fatigue items) and treatment burden impact. The shared content between subsets of variables is captured by a second loading on a content-specific factor. The specific-factor loading is conceptually similar to capturing the residual correlation between items with similar content. For example, how much a person’s self-management interfered with work responsibilities and family responsibilities may be captured by the specific factor role and activity limitations. Similarly, the shared-content between two items measuring how much self-management made the person worn out or preoccupied is captured by the specific factor physical and mental fatigue. In this manner, the bifactor model accounts for dependencies between items when establishing a total treatment burden impact score.
A SEM explaining treatment burden impact
Mediation models were conducted within a SEM framework. It was hypothesized that appraisal variables would mediate the relationship between reserve-building activities and treatment burden. In mediation analyses there are two types of relationships (pathways) to consider. There is the direct effect from reserve-building activities to treatment burden, and there is the indirect effect from reserve-building activities to treatment burden through both variables’ relationship with appraisal processes, social support, personality, and difficulty paying bills (the mediators). In this instance, mediation occurs when some (partial) or all (full) of the direct effect between reserve-building activities and treatment burden is accounted for by the indirect effect through appraisal or other processes.
SEM mediation analyses were conducted using Mplus version 7 software (Muthén and Muthén, 1998–2015) and accounted for the categorical nature of some items using the inter-item polychoric correlations with mean- and variance-adjusted weighted least squares. Model fit was evaluated using the following indices: root mean square error approximation (RMSEA) ≤ 0.08, Tucker–Lewis index (TLI) ≥ 0.95, and comparative fit index (CFI) ≥ 0.95 (Hu and Bentler, 1999; Browne and Cudeck, 1993). Analyses of observed variables were conducted using Stata 15 (StataCorp, 2017) and SPSS 24 (2016).
Results
Sample
The study sample included 446 patients. Table 1 provides the sociodemographic characteristics, ICD-10 categories, and reported comorbidities of this heterogeneous sample. The sample had a mean age of 49, and 85 percent was female. Most respondents were married and living with spouse and/or family members. The most prevalent ICD-10 index health conditions were diseases of the nervous system (e.g. multiple sclerosis) followed by neoplasms (e.g. breast cancer) and endocrine diseases. The most prevalent comorbidities were back pain, depression, and insomnia. A majority of participants reported that it was somewhat, very, or extremely difficult to pay bills.
Sample characteristics.

May add up to more than 100 percent because respondents were allowed to check all that apply.
Correlates of treatment burden
Table 2 shows Pearson’s correlations among the two PETS scales and the five sets of psychosocial factors examined in this study. The PETS scales had a large intercorrelation (r = 0.69) and they had small correlations with four reserve-building activities: active in the world, outdoor, exercise, and inner life. They were also similarly correlated with reported current and past social support, neuroticism, and four appraisal composite scores (health worries, independence and interpersonal concerns, accomplishing goals and problem-solving, and calm peaceful active). Demographic correlates of the PETS scales included age, difficulty paying bills, and comorbidity load.
Pearson’s correlations among variables considered for SEM.

SEM of treatment burden
Latent variables within the SEM for treatment burden, reserve-building, and social support
The key outcome, treatment burden, was modeled as a bifactor model with all items loading on the general factor (i.e. treatment burden impact) and items within the role activity limitations and physical and mental fatigue scales modeled as orthogonal specific factors. The SEM modeling framework treats treatment burden impact as the outcome of interest, with the specific factors accounting for residual covariance. All of the general factor loadings were large (>0.60; see Supplementary Table 1) and the specific factor loadings were also high (mostly >0.49), suggesting that unique variance is being explained by each specific factor. Social support was also modeled as a latent variable, which was supported by all five scale items having high loadings (>0.80). Finally, the reserve-building factor was also modeled as a latent variable comprising the four reserve-building subscales of note from Pearson’s correlation analysis: active in the world, outdoor, exercise, and inner life. These factor loadings were somewhat lower (range 0.28–0.51), which is to be expected since the subscales assess diverse aspects of reserve-building (Schwartz et al., 2017c). The appraisal scores were kept as weighted sums and standardized scores based on principal components analysis with orthogonal rotation reported in earlier work (Rapkin et al., 2017). Figure 1 shows the full SEM with all direct and indirect effects between the above-mentioned latent variables.

Empirical results predicting treatment burden. Reserve-building activities indirectly reduced treatment burden by: (1) reducing health worries appraisals, (2) reducing financial difficulties, (3) increasing calm and peaceful appraisals, and (4) increasing perceived social support. Note: All coefficients are standardized (mean = 0, standard deviation = 1). Latent variables are represented with ovals. Observed variables are represented with rectangles. For illustrative purposes, factor loading schematics and values have been omitted. “Treatment Burden Impact” is the general factor from a bifactor model comprising also the specific factors Role and Activity Limitations and Physical and Mental Fatigue.
SEM direct effects on treatment burden
The final, most parsimonious SEM accounted for 47 percent of the variance in treatment burden impact and closely fit the data (χ2 = 820, df = 326, p < 0.01; RMSEA = 0.06, CFI = 0.98, TLI = 0.98). The model estimated a series of direct and indirect effects on treatment burden impact from reserve-building and through appraisal and other covariates (for all model parameters, see Table 3). In order of magnitude, the strongest direct effects on treatment burden impact were from interpersonal/independence, neuroticism, health worries, age, difficulty paying bills, and comorbidity load.
Direct, indirect, and total effects from reserve building to treatment burden impact.
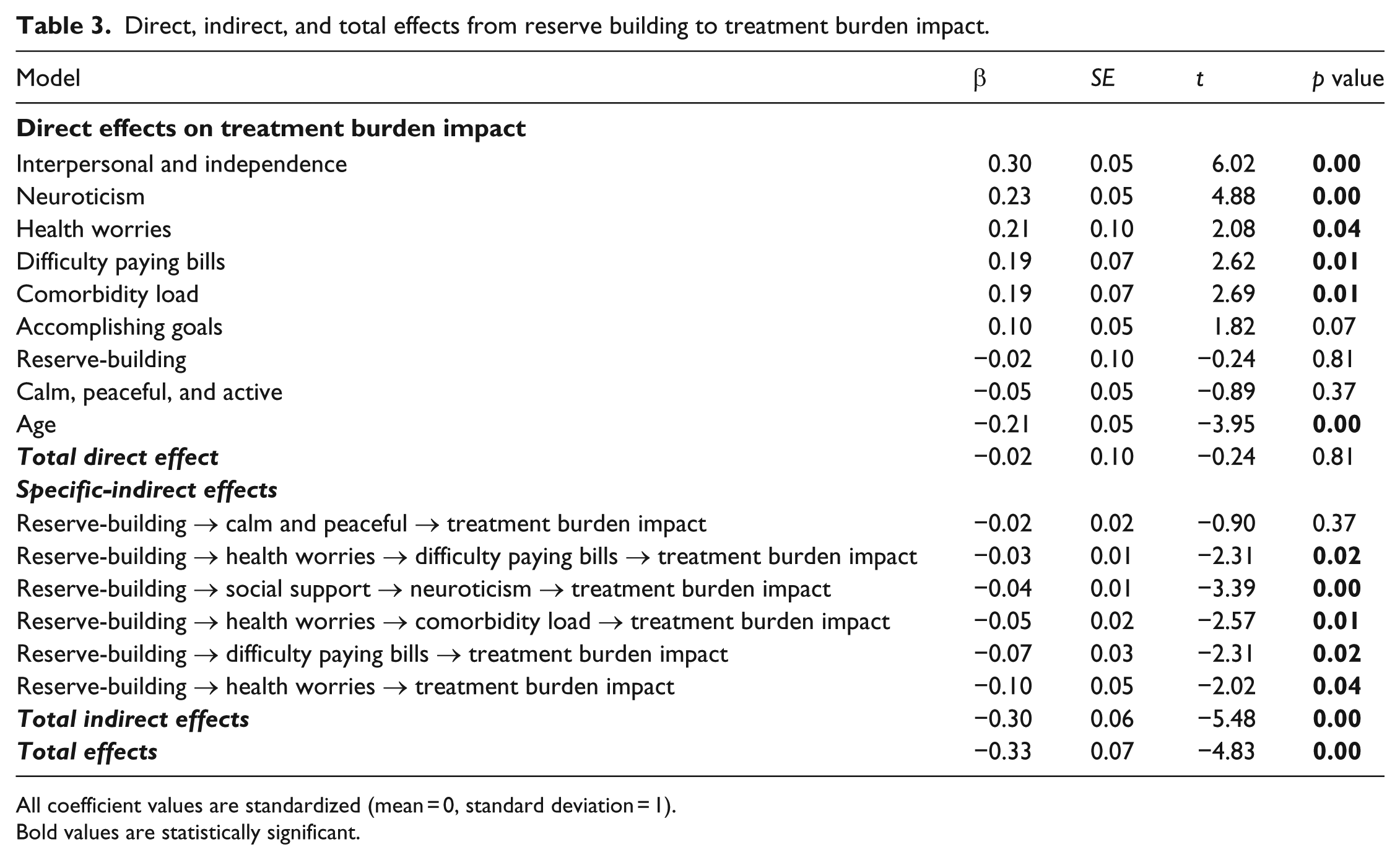
All coefficient values are standardized (mean = 0, standard deviation = 1).
Bold values are statistically significant.
SEM indirect effects on treatment burden
The SEM considered multiple indirect effects on treatment burden impact (Table 3). Importantly, the total effect of reserve-building on treatment burden comprised mainly indirect effects through other model variables and only weakly by the direct effect, suggesting complete mediation of reserve-building. Simple mediation of reserve-building on treatment burden impact was found through the specific mediators, health worries and difficulty paying bills. More complex mediation was found between the health worries and comorbidity load, social support and neuroticism, and health worries and difficulty paying bills.
Furthermore, health worries impacts treatment burden directly, via its relationship with comorbidity load (Table 3). Reserve-building is also closely related to (lesser) difficulty paying bills, but there is also a weak relationship through health worries (Table 3). Reserve-building has a significant indirect effect on treatment burden impact through difficulty paying bills, via a relationship between health worries and bills, via a relationship between health worries and comorbidity load, and via a significant relationship between (more) social support and (lesser) neuroticism.
Thus, after accounting for all of these indirect effects, reserve-building does not directly predict treatment burden. Rather, reserve-building leads to other factors that reduce treatment burden (i.e. full mediation).
Discussion
The results of this study suggest that engaging in reserve-building activities is associated with reduced treatment burden by distracting from health worries and by promoting appraisals related to being calm and peaceful. These findings support our hypothesis that appraisal mediates the relationship between reserve-building and treatment burden. They suggest that engaging in reserve-building activities is associated with differences in how one thinks about QOL, and what one thinks about.
Reserve-building activities are also associated with improved social support, which is associated with lesser treatment burden. It is possible, for example, that engaging in reserve-building activities helps people to create and maintain relationships with others and that these relationships also buffer them from the negative impact of attending to their own medical care. For example, by attending lectures or other cultural activities (active in the world), one may meet other people with similar interests and expand one’s social network. Similarly, by engaging in outdoor pursuits and/or exercise, one may meet new friends or deepen existing relationships.
Our model also suggests that improved social support is associated with reduced neuroticism in individuals, which thereby also attenuates treatment burden. In other words, people with better social support may be less likely to find fault with others or to get nervous easily (the two neuroticism items in the personality measure used), both of which would make the work of self-management less draining and tiresome. While personality characteristics are thought of as static characteristics, these items seem more mutable depending on the environment in which one finds oneself (i.e. friends, shared activities). These findings suggest that reserve-building activities and the accompanying social support could reduce tendencies of focusing on negative ways for interacting in the world.
Engaging in reserve-building activities is also associated with reduced treatment burden by reducing financial worries. The reserve-building activities that were kept in our model are not necessarily dependent on finances, although there are certainly versions of them that are costly. For example, exercise and outdoor activities can be accessible without pay if one lives near parks or safe places to walk or ride a bike. Cultural and intellectual activities (active in the world) can also be low-cost if one lives near a university or community center where lectures, exhibits, and films can be inexpensive or free.
Thus, our findings suggest that reserve-building activities may lead to a positive feedback loop whereby these activities reduce worrisome appraisals, enhance calm appraisals, and build social support networks and thereby reduce treatment burden. This positive loop might then lead to reduced treatment burden despite growing older or having more comorbidity load.
As with any cross-sectional study, an important caveat is that we cannot distinguish correlational and causal relationships based on this work. Although we present findings in terms of “associations,” it is sometimes hard to resist using language that implies that the relationships are causal. For example, people may have less treatment burden because they are healthier and thus able to engage in reserve-building activities. Similarly, people with fewer health worries would likely have lower comorbidity load and thus less difficulty paying bills. Low resources may also impact the accessibility of salutogenic reserve-building activities. There is some evidence that people of higher socioeconomic status are more likely to engage in reserve-building activities that are intellectually stimulating, involve outdoor pursuits, and include physical exercise (Schwartz et al., 2018). Frequent strife may also influence which appraisal processes are predominant, as well as expressed personality.
These suggested findings might thus be better phrased as “hypotheses” for future research using designs that can support causal inference. For example, a longitudinal observational study might be able to show change over time and relationships between changes in reserve-building, social support, appraisal, and treatment burden. Even better would be a randomized trial comparing an intervention aimed at increasing reserve-building activities to standard practice and evaluating effects over time. Such an intervention might employ motivational interviewing to help individual patients identify reserve-building activities they would like to do and discuss current barriers to engaging in them. With help, individuals might identify ways to combat the barriers so that they can bring reserve-building activities into their daily lives. Since these implicated activities are not necessarily costly to pursue, it would seem possible that they be accessible across the socioeconomic continuum.
Helping people to increase their engagement in reserve-building activities may help them to feel more calm and peaceful and to worry less. In the short term, these activities might not only reduce perceived treatment burden but also lower the risk of treatment intensification, because the activities are themselves health-enhancing. In the long term, more reserve-building activities might result in a compression of morbidity (Fries, 2005), that is, a longer time to functional deterioration due to reduced health risk behaviors. A growing research base suggests that having a better health-risk-behavior profile (e.g. not smoking, not overweight; Hubert et al., 2002), regular exercise habits (Hubert et al., 2002), and having an active cognitive lifestyle (Marioni et al., 2012) are linked with a compression of morbidity in late life. A host of relatively simple interventions may be implemented to improve the health and well-being of individuals with multiple chronic conditions, and reduce suffering and healthcare costs.
While this study has advantages of a large and heterogeneous sample with multiple chronic conditions, its limitations must be acknowledged in addition to the above-mentioned caveat. It predominantly comprises White females who are married or living with family members. Thus, the participants may be more representative of people with higher levels of social support. This sample characteristic could constrain the correlations between treatment burden and social support. In addition, use of a very brief personality measure renders the variables less reliable than a longer measure of the constructs.
In summary, this research might provide a roadmap for helping patients to manage their illness. It suggests that reserve-building activities may impact treatment burden by affecting ways of thinking—reducing worrying and increasing a sense of calm. They may also enhance perceived social support and reduce neuroticism. Our findings point to key behaviors that chronically ill people can use to attenuate treatment burden.
Supplemental Material
Supplementary_table_PROOFS – Supplemental material for Reserve-building activities attenuate treatment burden in chronic illness: The mediating role of appraisal and social support
Supplemental material, Supplementary_table_PROOFS for Reserve-building activities attenuate treatment burden in chronic illness: The mediating role of appraisal and social support by Carolyn E Schwartz, Jie Zhang, Wesley Michael, David T Eton and Bruce D Rapkin in Health Psychology Open
Footnotes
Acknowledgements
We are grateful to Brian Stucky, PhD, for his helpful input during data analysis and on earlier drafts of this manuscript. We are grateful to the patients who participated in this study. All authors declare that they have no potential conflicts of interest and report no disclosures.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.