
Abstract
Growing evidence suggests that the arts may be useful in health care and in the training of health care professionals. Four art genres – novels, films, paintings and music – are examined for their potential contribution to enhancing patient health and/or making better health care providers. Based on a narrative literature review, we examine the effects of passive (e.g. reading, watching, viewing and listening) and active (e.g. writing, producing, painting and performing) exposure to the four art genres, by both patients and health care providers. Overall, an emerging body of empirical evidence indicates positive effects on psychological and physiological outcome measures in patients and some benefits to medical training. Expressive writing/emotional disclosure, psychoneuroimmunology, Theory of Mind and the Common Sense Model of Self-Regulation are considered as possible theoretical frameworks to help incorporate art genres as sources of inspiration for the further development of health psychology research and clinical applications.
We tell ourselves stories in order to live. Not disclosing our thoughts and feelings can be risky for our mental and physical health. Divulging them can be healthy.
‘Do art lovers make better doctors?’ was the title of a preliminary examination of whether reading novels and poems, watching films, listening to music, and studying paintings helps medical students and health care professionals be ‘better’ in their work with patients (Kaptein et al., 2013). Defining ‘better’ is the major issue, of course. As stated by Ousager and Johannessen (2010), ‘the ultimate question is whether it can be documented that students who are exposed to the humanities eventually become better doctors to the benefit of themselves, their practice, and their patients’ (p. 993).
Authorities and organisations responsible for the education and training of health care professionals invariably emphasise the value of incorporating medical humanities into the medical curriculum (Jones et al., 2014; USA guidelines: American Society for Bioethics and Humanities (ASBH), 2009; Canada guidelines: Frank et al., 2015; UK guidelines: General Medical Council (GMC), 2009; NFU Dutch guidelines: Medical Education, 2009; State of the Field Committee, 2009; Thompson et al., 2016). However, there continue to be debates over the benefits of exposing medical students and other trainee health professionals to novels, films, paintings and music in an attempt to ‘humanise’ and/or otherwise improve the quality of medical care (e.g. Heath, 2016; Perry et al., 2011). Reviews of the effects of medical humanities on various outcomes range from the cautiously optimistic (e.g. Ousager and Johannessen, 2010) to the outright negative (e.g. Bignall, 2001). Quite often in this debate, emotional reactions seem to dominate scientific reasoning; sometimes, raising the question about the effects of medical humanities in itself elicits fierce criticism (e.g. Belling, 2010; Charon, 2010).
Reviewing such a vast topic, particularly one characterised by rather diverse methods and uneven – and, not seldomly, low – methodological rigour is complex and may easily be contentious. Our goal is to attempt to provide some preliminary structure around this broad issue; in particular, we focus on three elements. First, we focus on (future) health professionals and on patients. Second, we distinguish between ‘active’ (e.g. writing, producing, painting and performing) versus ‘passive’ (e.g. reading, watching, viewing and listening) exposure to the four art genres that we discuss, that is, novels, films, paintings and music (cf. Väänänen et al., 2009). Third, we use high-quality empirical studies – where available – in assessing the effects, that is, preferably experimental design, randomised controlled, with more than only self-reported outcomes.
Novels are an almost endless source of description of how patients, their family and friends, health care providers and society make sense of illness (e.g. Nádas (2002) on cardiovascular diseases; Solzhenitsyn (1971) on cancer). Films portray how a society and its citizens respond to epidemics and various illnesses (e.g. Darbyshire and Baker, 2012). There is evidence that paintings can be used to teach students to improve their observational skills – for example, supervised studying by medical students of naked bodies on a painting resulted in better observational skills of real patients with skin conditions (Naghshineh et al., 2008). Music has been used in teaching medical students about love, death and mourning (e.g. Butler, 2009). In the area of health humanities, virtually all conceivable art genres are relevant. In this article, we focus on four genres, given the body of empirical knowledge: novels, films, paintings and music (opera, theatre and poems are excluded but see Bernard et al. (2015), and Seymour and Murray (2016)).
Each genre can be experienced both passively (receptively) and actively (generatively). For example, health care providers can prescribe ‘reading novels’ (bibliotherapy, McCulliss, 2012) to patients to help them make sense of their predicament. In the active writing mode, patients are encouraged to apply expressive writing to facilitate adaptive coping and an improved medical and psychosocial outcome, supported by evidence about the positive effects of such activity (Pennebaker and Smyth, 2016; Smyth and Greenberg, 2000). Medical students report positive effects from reading novels: self-reported levels of empathy and satisfaction with the clinical encounter (Bate and Schuman, 2016; McLellan, 1996; Myers and George, 2012). Regarding films, patients living with a certain medical condition may benefit from watching films about that condition (e.g. diabetes, in the film ‘Steel Magnolias’; Ross, 1989) which may be instrumental in improving knowledge and self-management behaviour. In the active mode, patients make films about their own illness and can use ‘photo voice’ (Catalani and Minkler, 2010; Dassah et al., 2017) as a means to depict their illness in pictures. Physicians watching movies with themes which are highly relevant for health care providers (e.g. the film ‘The Doctor’, 1991) report a greater understanding of patients’ concerns (Darbyshire and Baker, 2012). Patients can paint and depict their illness (art therapy is a broad encompassing label often used in this domain; Archer et al., 2015). Some physicians have expressed in paintings the emotional aspects of their work and its effects on them (e.g. Calne, 1996). Patients may turn to music to help cope with their illness, for example, during chemotherapy; researchers have found positive effects of listening to music by patients on physiological and psychological variables (e.g. Hole et al., 2015). In addition, patients use music to express their coping with illness (e.g. Panigrahi et al., 2014); physicians seem to benefit from listening to or performing music (Wong, 2012).
Art in health care is a rapidly developing field. In the past decade, journals, books, conferences, professional societies and university departments devoted to the field labelled ‘Medical Humanities’ have sprung up and been established; the field has recently been relabelled Health Humanities for reasons health psychologists understand only too well (Jones et al., 2014). The greatly increased attention paid to patient-reported outcomes, biopsychosocial medicine, health psychology, shared decision making and self-management, has facilitated this development. A growing body of empirical evidence supports the clinical and research base of ‘health humanities’. The references to the clinical and research applications in this article give an impression of the sources for the empirical basis of the area. The theoretical basis of the area seems somewhat lagging, however – which is why we also attempt to discuss some theoretical concepts that seem relevant and give some suggestions about incorporating those concepts into a theoretical framework relevant for health psychology. A few core concepts are available for developing such a framework. We briefly outline these theoretical concepts, which can be viewed as potential mechanisms linking passive and active involvement with art and various outcomes (psychological, social, medical).
Expressive writing/emotional disclosure
Expressive writing, typically consisting of some (at least semi-structured) writing about emotionally meaningful topic(s), is one way for active involvement in writing; expressive writing may also, to some degree, reflect a broader method of creative and expressive active involvement (e.g. painting or dancing about emotionally meaningful topics). According to Pennebaker and Smyth (2016) in their recent review of research on this topic, expressive writing (and creative/expressive activities more generally) may help produce structure (e.g. a coherent narrative, temporal structure) and facilitate insight, meaning and categories that help the patient make sense and accommodate/assimilate the experience; notably, this view is broadly consistent with many elements from the Common Sense Model of Self-Regulation (Leventhal et al., 2016). The health benefits of expressive writing have been documented and are quite diverse – including (but not limited to) improvements in clinical disease status, enhanced psychological well-being, better physiological (e.g. immunological) function, improved interpersonal relationships and better cognitive function (Pennebaker and Smyth, 2016, esp. pp. 155–156; cf. Smyth, 1998; Smyth et al., 1999).
The authors warn that ‘no single explanation or straightforward theory of disclosure has emerged’ and note that multiple mechanisms are likely involved (and/or different mechanisms in different people and/or contexts; Pennebaker and Smyth, 2016: 155; see also Smyth and Pennebaker, 2008). Nevertheless, the mechanisms sketched above do place the field of ‘art in medicine’ in a (health) psychology context, especially given its link to the Common Sense Model, and thereby the potential link of expressive writing to research about clinical interventions in the areas of self-management, adherence, illness perceptions and quality of life (Hagger et al., 2017).
Extending earlier theoretical and empirical work (e.g. Pennebaker, 1993; Smyth, 1998), Frattaroli (2006) in her meta-analysis of expressive writing and emotional disclosure found beneficial effects of experimental disclosure on psychological health, physical health and overall functioning. Moreover, she reviewed evidence for a set of mechanisms and mediators that may help explain the effects of experimental disclosure. Five theoretical approaches are reviewed: inhibition theory, cognitive processing theory, self-regulation theory, social integration model and exposure model. In a systematic review of expressive writing in patients with cancer, Merz et al. (2014) identified four mechanisms they saw as potentially involved in explaining the benefits of expressive writing in cancer patients (again, broadly consistent with earlier work): expressive writing has a benefit through the expression itself (in an otherwise potentially constrained context), it may stimulate cognitive restructuring of a trauma and habituation to the emotions associated with that trauma, it may boost personal mastery and self-regulation, and expressive writing may help restoring a sense of perceived control (p. 340).
Theory of mind
The concept of ‘Theory of Mind’ (ToM) is the second theoretical framework that could help explain the mechanisms between reading literary fiction, on one hand, and ‘the capacity to identify and understand others’ subjective state’ – ToM defined – on the other hand (Kidd and Castano, 2013: 377; Pino and Mazza, 2016). In a series of experimental studies, these authors have demonstrated how levels of affective ToM (the ability to detect and understand others’ emotions) and cognitive ToM (the inference and representation of others’ beliefs and intentions) increased as a consequence of reading literary fiction. ToM seems to be a useful theoretical concept, explaining the link between reading novels and poems, and levels of empathy. Mar and colleagues incorporated ToM into their research on reading and combined this with neurological work where MRIs were utilised to examine if and which areas in the brain might be associated with ToM and with attempts to influence ToM by reading literary works (e.g. Mar, 2011). In their recent research, this group included ‘personality’ (NEO) as a concept in explaining effects of reading and ToM (Maslej et al., 2017). In a refinement of the area, Kidd and Castano (2017) recently discovered how literary fiction (‘high literature’) and ‘genre fiction’ have different effects on ToM: ‘exposure to literary but not genre fiction positively predicts performance on a test of ToM’ (p. 474).
ToM is not simply a purely cognitive process rather one which is located in our everyday social interaction. Thus, it could be argued that through developments in our linguistic repertoire, we can increase our sophistication in understanding other minds (Hughes and Leekam, 2006). Furthermore, a social constructionist approach to mental activity argues that it is constituted through text and talk which are situated in a cultural and historical context (Shi-Xu, 2006). Anthropologists such as Luhrmann (2011) have explored how cultural variations in theories of mind are connected with how people conceptualise and experience illness. Gentner and Grudin (1985) have explored historical changes in mental metaphors. Thus, it would be expected that encounters with various art forms would be reflected in how both health professionals and patients conceptualise illness.
Psychoneuroimmunology
Psychoneuroimmunology (PNI) is a third theoretical concept or mechanism that may be involved in explaining associations between being involved with reading, writing, films, music and painting(s) – passively or actively – on one hand, and (changes in) coping strategies and outcomes, on the other hand. Broadly put, PNI is an umbrella term referring to the intra-individual interactions between psychological events and the nervous and immune systems. As such, the assertion that aesthetic experience can have consequences for physical systems gains plausibility within a psychoneuroimmunological frame of reference. Research into the effects of music, for example, on physiological systems has a long history. In the early 20th century, Hyde and Scalapino (1918) studied the effects of music listening on cardiovascular function. They found that listening to ‘stirring’ music appeared to increase both blood pressure and heart rate. This might be accounted for by the way external rhythms influence an individual’s respiration and thus produce downstream cardiovascular effects. However, one of Hyde and Scalpino’s more intriguing findings is harder to explain. They found that listening to minor tones appeared to elevate heart rate and dampen blood pressure when compared to listening to major tones. Such a finding implies that the aesthetic–perceptual aspects of music listening, as well as the mechanics of respiration, may result in direct physiological impacts.
Fancourt et al. (2014), having reviewed the literature on music and PNI, present a conceptual framework that can serve for multiple artistic forms. They helpfully seek to distinguish different aspects of artistic experience that appear to influence the extent and nature of physiological responses. These comprise the physical properties of the art (e.g. the tempo or pitch of music, or the colours of a painting), the physical involvement required by the art (e.g. the bodily actions required to produce or consume the art), the social engagement required to by the art, and the personal response to the art (including feelings of familiarity vs novelty; liking vs disliking of pieces or genres; perceived positive vs negative emotionality). When seeking to identify the impact of passive or active engagement in the literature, films, paintings, or music, the PNI research to date suggests that it would be useful to consider such dimensions separately (Brattico and Pearce, 2013).
There is little consensus on what specific biomarkers should be given greatest priority when developing research – or interventions – relating to the psychoneuroimmunological effects of these different artistic forms. Several studies have identified an impact of artistic experience on measures of immunoglobulin A (IgA), an antibody active in mucous membranes that is implicated in susceptibility to infection. Another body of work has considered the impact on the stress hormone cortisol. By and large, the research has suggested positive effects for music, namely, increases in IgA and decreases in stress-related cortisol. However, some caveats need to be borne in mind. First, these measures are among the most researched, but this does not mean they are the most important. Simply put, part of the focus on IgA and cortisol stems from the fact that they are relatively cheap and practical to incorporate into a laboratory procedure. As such, researchers are encouraged to broaden the range of physiological measures and systems that are to be considered. Second, while it is tempting to interpret fluctuations in IgA and cortisol as though their implications for well-being are linear, in reality the endocrinal and immune systems are complex and sometimes ambiguous. For example, elevations in IgA may be interpreted as evidence of an efficient immune response (and thus good health) or of a current infection (and thus poor health). As such, the risk of confirmation bias in PNI research is high. In summary, while PNI offers a comprehensive framework within which to demonstrate and explore the biological mechanisms linking art to health, the range of possible approaches is extensive. However, given the recurring patterns in research to date, there is clear justification for continuing to investigate the impact of art on these physiological systems.
Common sense model of self-regulation (CSM)
Expressive writing/emotional disclosure, ToM and PNI may be helpful in explaining how the passive and active exposure to novels, film, painting(s) and music is associated with benefits in the levels of empathy in health care providers, and QOL and physiological measures in patients with a somatic disease. Incorporating these three theoretical concepts into the CSM (Figure 1) may be a useful step in developing a theoretical model regarding arts and health psychology.
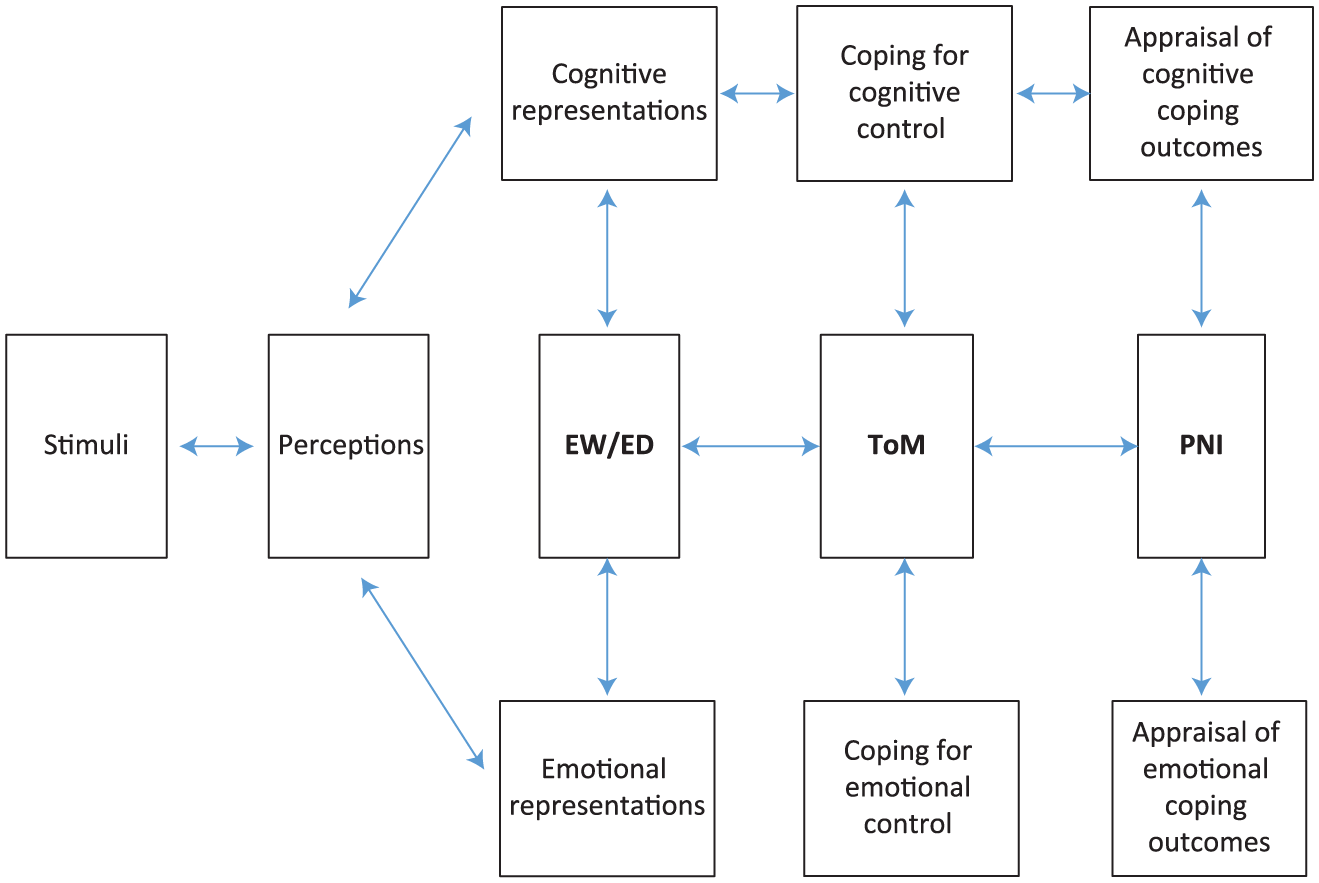
Expanded version of the Common Sense Model of Illness (from Hagger et al., 2017).
Several possible processes follow from the suggested expanded common sense model of self-regulation. These include expressive writing/emotional disclosure (EW/ED) effects illness representations, thereby affecting coping and outcomes; EW/ED impacts on ToM, leading to more adaptive coping; EW/ED impacts outcomes via ToM. Or a study that uses bibliotherapy as the intervention leads to improved coping, mediated by more stable, ‘healthy’ PNI status and thereby to a more adaptive outcome of cancer. Expressive writing improves PNI, thereby improving QOL. Patients with cancer performing music score higher on ToM. These processes will be considered in our review.
Methods
Several approaches were applied in identifying relevant research on the effects of reading or writing novels, watching or making films, watching or making paintings, and listening to or making music, in patients and health care providers.
PubMed searches were conducted using ‘medical humanities AND novels’, ‘medical humanities AND films’, ‘medical humanities AND paintings’ and ‘medical humanities AND music’ as key terms.
Articles were identified in a selection of key journals which specifically focus on ‘medical humanities’, that is, Academic Medicine, Hektoen International, Journal of Medical Humanities, Journal of Poetry Therapy, Medical Anthropology Quarterly, Medical Humanities, Psychology of Aesthetics, Creativity, and the Arts.
Sections in (medical) journals that focus specifically on medical humanities were studied, that is, American Journal of Psychiatry, Annals of Internal Medicine, Bellevue Literary Bulletin, British Journal of Psychiatry, Chest, Canadian Medical Association Journal, Family Medicine, Journal of Clinical Oncology, Poetics Today.
Relevant websites, that is, www.medhum.med.nyu.edu; www.literatuurengeneeskunde.nl; www.blogs.bmj.com/medical-humanities, were reviewed.
Files from the authors of the current paper. All are active in the area and publish in the field of ‘literature and medicine’ and ‘medical humanities’ (e.g. Kaptein et al., 2015; Murray, 2000; Murray and Gray, 2008; Sesker et al., 2016; Smyth et al., 1999).
Results
Novels
The paper ‘A chapter a day: Association of book reading with longevity’ (Bavishi et al., 2016) concludes ‘… the benefits of reading books include a longer life in which to read them’ (p. 44). Do patients benefit from reading novels (‘bibliotherapy’): will it give them ‘a longer life’? Various publications encourage teachers of health professionals to use novels in order to increase their empathic behaviour towards patients and to promote adaptive coping in patients (e.g. Myers and George, 2012). Do patients benefit from reading novels about their affliction? Do they benefit from expressive writing; will it make their wounds heal more quickly? Do physicians become better doctors when they write about their professional experiences? Only relatively recently are empirical papers on these topics available, some with quite stringent designs, adequate sample sizes and sophisticated methodology.
Patients – passive exposure to novels
Bibliotherapy is the term used to describe the reading of novels and other literature by patients as a means to help them get better. Defined as ‘the use of selected reading materials as therapeutic adjuncts in medicine and psychiatry; also, guidance in the solution of personal problems through directed reading’ (McCulliss, 2012: 23), bibliotherapy has been applied to an extensive list of health problems ranging from cancer, depression and migraines to sexual dysfunction. Outcome studies report consistent positive, albeit modest, effects on measures such as depression, self-efficacy, sense of belonging and finding workable solutions to the identified problems (McCulliss, 2012).
Latchem and Greenhalgh (2014) conducted a systematic review of the effects of reading on health and well-being of people with neurological conditions. They concluded that some positive effects are discernible, although they caution against excessive optimism due to the small number of high-quality studies. Some studies in this domain are quite striking. For example, in the cleverly titled study, ‘A “novel” intervention’, reading age-appropriate fiction by girls of 9–13 years of age with obesity resulted in significant decreases in BMI (Bravender et al., 2010). A large prospective study with a 12-year follow-up concluded that ‘book readers experience a 20% reduction in risk of mortality’ (Bavishi et al., 2016: 44). Negative side-effects of reading appear to be scarce, which – given the emerging evidence that reading is associated with, and may be causally related to, good health in both ill and healthy persons – suggest the uptake of reading is warranted in patients and health care providers. A recent systematic review of randomised clinical trials in depression treatment concluded that ‘bibliotherapy could play an important role in the treatment of a serious mental health issue’ (Gualano et al., 2017: 49). A recent study by Billington et al. (2017) compared a structured group reading programme of various novels with a CBT intervention for patients with chronic pain. Although this was a small study, they found evidence that the reading programme was more effective than the CBT intervention in improving patient mood. With reference to our ToM hypothesis, one of the reading group participants said after a reading session: From a poem or story you get these pictures in your mind sometimes that you wouldn’t normally get. You can sort of take them away … if you try to relax or when you go to bed at night-time, you can have that picture in your mind that you got from the poem or story. What you have tried to absorb can come out later or help you as a distraction from all these things spinning around in your mind that you want to get rid of (p. 161).
Reading illness narratives was applied in an experiment to study the effects on (self-reported) HPV vaccination (Krakow et al., 2017). The publication of this study in Health Psychology seems testament to the increasing interest and relevance of health humanities in health psychology.
Patients: active exposure to novels
Although reading books is usually a solitary and more passive form of mental activity (but note the activity involved in book reading clubs as in the study of Billington et al., 2017), expressive writing is an active counterpart – sometimes referred to as ‘scriptotherapy’. In many forms of expressive writing, a person writes about stressful or otherwise emotionally significant experience; such writing is typically done without regard to style or format and is largely kept private with the goal of facilitating understanding and reflection. Reviews of the topic point at various beneficial effects. In his review of the subject, Smyth (1998) distinguished five categories of outcomes, that is, reported health, psychological well-being, physiological functioning, general functioning and health behaviours. In healthy respondents, expressive writing led to positive effects on most of these outcomes (Pennebaker and Smyth, 2016; Smyth, 1998). In a later study, positive effects were also found in patients with chronic disease (asthma and rheumatoid arthritis (RA); Smyth et al., 1999). The patients in that study wrote about the most stressful event of their lives and, 4 months following writing, demonstrated clinically significant improvements in pulmonary function (in asthma) or overall disease activity (in RA).
Expressive writing has now been studied, often in an experimentally and clinically sound fashion, for over three decades. Much of this work extended writing to new patient samples and new contexts (see Pennebaker and Smyth, 2016, for more comprehensive review). In some contexts, such as getting patients who have cancer to write, results were not as straightforward. Two major systematic reviews and meta-analyses (in patients with cancer) led to more cautious conclusions. Merz et al. (2014) reviewed 13 articles and concluded that ‘the majority of the intervention effects were null, although there were several main effects … on sleep, pain, and general physical and psychological symptoms’ (p. 339). Similarly, Zachariae and O’Toole (2015) reported no major effects on psychological or physiological outcomes. Both research groups, however, stressed the importance and potential value of further study, given the practical and inexpensive nature of the intervention.
Health care providers: passive exposure to novels
What are the effects of reading novels by medical students (soon to be health care providers) on their professional behaviour? Is the quality of medical care given to a patient with cancer by a physician who has studied ‘Cancer Ward’ better than the care from one who did not read the novel? A review of empirical studies addressing this issue concluded that the evidence is weak, but this conclusion appears based on a relatively small number of studies, with the majority of studies focusing on effects of training courses on medical ethics and patient–physician interaction (Ousager and Johannessen, 2010; Perry et al., 2011). The dependent variables in most studies were self-reported, not patient-reported or observations of clinical practice. Despite this, medical journals continue to publish papers on ‘novels doctors should read’ (e.g. Lancet: McLellan, 1996). A study of Finnish medical students demonstrated how reading novels may not always attain the intended effect: they found a negative effect of reading The Black Swan by Thomas Mann which considers a fatal episode of ovarian cancer (Lahtinen and Torppa, 2007): the students were very interested in how to diagnose ovarian cancer rather than in how to explore the psychosocial impact of a fatal disease.
Health care providers: active exposure to novels
The impact of expressive writing by physicians, nurses and health students, sometimes part of courses in Literature & Medicine or Medical Humanities, has not been studied empirically. At the same time, a large number of physicians write novels and poems about their clinical work (e.g. Mikhail Bulgakow, Richard Selzer, Lev Tolstoy, Abraham Verghese, William Carlos Williams). More recently, there are examples of health care providers writing ‘online’ about their encounters with patients (e.g. ‘Pulse – voices from the heart of medicine’ (www.pulsevoices.org)).
The scoping review and narrative synthesis of quantitative outcome studies in medical humanities by Dennhardt et al. (2016) offer suggestions about how different types of humanities may work: ‘art as expertise, as dialogue, and as a means of expression and transformation’ are suggested by the authors as theoretical frameworks.
Films
‘Cinemeducation’ (Alexander et al., 2005) is the title of a book on how films may be used in medical education, with a view to encouraging medical students to reflect on the responses of patients, their social environment and their physicians to illness. ‘The Doctor’ (Haines, 1991), ‘One flew over the cuckoo’s nest’ (Forman, 1975) and ‘The seventh seal’ (Bergman, 1957) are a few of the classic films recommended. They depict, respectively, a highly successful physician who becomes a patient, life in a psychiatric ward, and the social representation of a contagious disease. Alexander et al. (2005) have organised the potential films according to themes relevant in medicine, for example, chronic illness, family violence, eating disorders. The book The Picture of Health by (Colt et al., 2011) has a similar objective, with an emphasis on movies that illustrate issues in medical ethics, for example, ‘autonomy, justice, and informed consent’, ‘communication and provider-patient relationships’ or ‘end of life and right to die’. Ferguson (2010) reviewed films about living with diabetes and identified the concept of ‘control’ as a central theme – consistent with a central theme in health psychology research about people with diabetes (e.g. Kaptein et al., 2017).
Patients: passive exposure to films
A study investigating the impact of viewing films in a setting was conducted by (Jones et al., 2016). Patients recovering from an acute coronary syndrome were randomised to an intervention group and a control group, where the intervention entailed observing a brief animated film representation of ‘the pathogenesis of acute coronary syndrome and the resulting effects’ (p. 110). Similar animations were presented illustrating the potential beneficial effects of adhering to statin treatment. Illness perceptions and medication beliefs, satisfaction with the intervention and behavioural outcomes (days taken to return to work, exercise) were studied as dependent variables. Overall, the intervention resulted in meaningful positive effects on illness perceptions, treatment beliefs, symptoms, return to work and exercise behaviour.
Health care Patients: active exposure to films
Patient-directed or initiated films are not directly identified by PubMed searches; high level evidence reviews, therefore, are unavailable. Photovoice is an approach with a quite large evidence base. Photovoice was developed ‘to promote empowerment and give voice to populations experiencing a variety of health problems and health care contexts’ (Evans-Agnew and Rosemberg, 2016: 1019). Usually, patients (or participants) are provided with a camera and then encouraged to take pictures and make a film of situations, persons and objects that are meaningful to them and their (medical) condition. Two reviews on the effects of photovoice were identified (Catalani and Minkler, 2010; Evans-Agnew and Rosemberg, 2016). The outcome criteria used pertain mainly to whether participants were involved in developing and improving relationships between the participants and the community where the study was conducted. In their review of 37 articles on photovoice about public health, Catalani and Minkler (2010) concluded that ‘photovoice appears to contribute to an enhanced understanding of community assets and needs and to empowerment’ (p. 424).
Frith and Harcourt (2007) discuss how women’s experiences with chemotherapy are reflected in photographs that the women themselves took. The authors maintained that keeping a photographic record of their experiences of chemotherapy treatment for breast cancer helped the women considerably in adjusting to and mastering their situation. The use of photovoice in mental illness has been reviewed by Han and Oliffe (2016).
Health care providers: passive exposure to films
Films like ‘Wit’ (Nichols, 1999, based on the novel by Edson, 1993) or ‘The Doctor’ (Haines, 1991) are a potential means of teaching health students and health care providers about how they might respond to human suffering. Darbyshire and Baker (2012) reviewed the subject and present a thematic analysis of the use of cinema in medical education. They concluded that the field is still in its infancy. The Journal of Medicine and Movies is a Spanish journal that publishes articles with English summaries. It reviews films about illness and discusses the use of films in the training of health care providers.
Health care providers: active exposure to films
Rabow et al. (2010) describe a documentary made by physicians about how persons with brain tumours and their families try to live with the illness, wherein the patients helped provide content for the documentary. A pre-post survey among neurosurgeons, neuro-oncologists and medical students who watched the film revealed increased positive attitude towards the film and its objectives.
Paintings
Illness is a theme which figures prominently in the world of painting. One only has to look at the work by Munch (e.g. ‘The sick child’), Picasso (e.g. ‘Science and Charity’) or Rembrandt (e.g. ‘Bathsheba at the bath’) to grasp how artistic portrayals of illness and dying can impact the viewer (Dequeker, 2006). Research has considered the impact of passive and active participation in artwork by both patients and health care providers.
Patients: passive exposure to paintings
Research of the impact on patients viewing paintings and comparable objects is limited. In an observational study, patients and visitors in a hospital emergency department were observed before and after new still and video art was installed (Nanda et al., 2012). There was a reduction in the number of queries and increased social interactions by patients and visitors after the intervention. Quan et al. (2016) found that paediatric patients exhibited less stress and more positive attitudes to radiographic procedures in a condition where lighting, colour and movement in the radiography room changed compared to a standard condition.
Patients: active exposure to paintings
There is substantial research literature on the impact that active participation in art making has on patients. This research can be traced back to earlier work where clinicians attempted to use children’s drawings as diagnostic instruments. More recently, adult patients with somatic illnesses were encouraged to draw their illness (e.g. Broadbent et al., 2006). Illnesses depicted in the drawings range from myocardial infarction to sickle cell disease to Cushing’s disease (see Van Leeuwen et al., 2015, for a recent concise review). Drawings reflect not only medical severity but also perceived severity. Drawings have been found to predict illness outcome in terms of resumption of work, sexual activities and reductions in pain. A particular feature of the latter research is the connection with work on illness perceptions, medication beliefs, coping and quality of life (e.g. see Courtney et al., 2017, which adopted a narrative approach to explore the pain experience of the painter Frida Kahlo; also Kirkham et al., 2015, which adopted an interpretative phenomenological approach to the analysis of drawings of chronic pain).
Archer et al. (2015) conducted a systematic review of randomised controlled trials on the effects of creative interventions on psychological outcomes in adult patients with cancer. They identified four papers on the use of art therapy, which reported improvements in various psychological outcome measures. Art therapy in these papers consisted of drawing a life-size body outline and drawings of the participants’ own choice. Assessments of the effects were self-report measures regarding quality of life, which generally improved as a consequence of the intervention.
Other researchers have explored how mental illness images are associated with artistic representations by the patients. Women’s mental images of their breast cancer were explored in a qualitative interview study (Harrow et al., 2008). The patients used, among other approaches, clay to represent their illness. Results indicated that these clay representations reflected the illness perceptions of the women. In another study by Lawson et al. (2017), it was found that painting a tile during an invasive medical treatment (blood and marrow transplantation) was a highly appreciated experience by the patients.
Graphic medicine is a new development in the area of representing living with illness (www.graphicmedicine.org). Blogs, websites and related social media give patients (and their relatives) new opportunities to express their ideas and emotions about their illness (e.g. Al-Jawad, 2015; Fies, 2006: Mom’s Cancer; Marchetto, 2006: Cancer Vixen – see McMullin, 2016).
Paintings by patients who have been institutionalised in (psychiatric) hospitals have also attracted research interest. An example is the study by Allegaert et al. (2010) of the work by the painter and graphic artist Willem Van Genk who spent time in hospital as a result of a range of mental health problems. He is considered as an exponent of ‘outsider art’, which is a term used to describe work by people working outside the usual confines such as those in psychiatric institutions.
Health care providers: passive exposure to paintings
Some research has explored the impact on medical students and physicians from viewing paintings. Naghshineh et al. (2008) observed the impact on medical students who were instructed by museum experts on how to examine the skin of naked bodies in paintings. Afterwards, these students examined the skin of ‘real’ patients. Compared to students in the control condition, the students who visited the museum scored better on ‘sophistication in their descriptions of artistic and clinical imagery’ (p. 991). A similar study with general practitioners and primary care nurses obtained similar results (Kirklin et al., 2007).
Health care providers: active exposure to paintings
There has been limited research on the character of artwork by health care providers. Some clinicians have written about their own artwork. For example, Calne (1996) has written about his paintings of transplantation surgery which has had a broader influence on clinical education.
Music
Opera: Desire, Disease, Death (Hutcheon and Hutcheon, 1996) is an attractively titled book that explores the literary and musical relationship between operas and various illnesses. AIDS, cholera, plague, syphilis and tuberculosis each play quite significant roles in major operas. Music and libretto are often deployed to portray the dimensions of various (infectious) diseases, reflecting their cultural depiction over time and across cultures (with prominent examples to be found in such works as La Traviata and Oedipe Re). Ultimately, music plays a crucial role in the lives of many. This, therefore, holds true for patients as well.
Patients: passive exposure to music
One systematic review indicates that having patients listen to music while they are in the operating room appears to reduce their stress levels, leading to a reduction in analgesia and sedation requirements (Moris and Linos, 2013). The effect applies to children as well as adults. That pain and distress are both reduced in children undergoing intravenous placement in the paediatric emergency department has been demonstrated in a randomised clinical trial (Hartling et al., 2013). In a systematic review and meta-analysis of such trials, the authors concluded that ‘music interventions may have a statistically significant effect in reducing post-operative pain, anxiety and distress in children undergoing a surgical procedure’ (Van der Heijden et al., 2015: 2). Recovery post-surgery is also enhanced. A recent systematic review and meta-analysis by Hole et al. (2015) indicated that music improves recovery after surgical procedures (in adults), and that ‘music could be offered as a way to help patients reduce pain and anxiety during the postoperative period’ (p. 1659).
Music interventions have been attempted for several chronic and severe illness conditions. (Lai et al., 2011) randomised cancer patient caregivers to experimental or control conditions. In the experimental condition, recorded music was combined with a visit by a nurse who took care of patients with cancer in their homes. The control condition was similar but with no music. The authors found that patients in the experimental condition exhibited enhanced well-being as measured by anxiety and depression scores, as well as blood volume pulse amplitude, compared to patients in the control condition.
Patients undergoing haemodialysis, an invasive and frequent medical procedure, appear to benefit from listening to music, at least in terms of reduced scores for anxiety and pain (Pothoulaki et al., 2008). Patients undergoing bronchoscopy also appear to benefit: a recent meta-analysis suggests that listening to music during bronchoscopy helps to reduce patients’ blood pressure and heart rate (Tam et al., 2016).
For broader mental health outcomes, the effects of music seem more pronounced. Among patients with cancer, such interventions appear particularly useful in improving psychological (and some physical) outcomes, according to a Cochrane Collaboration review; the authors conclude that ‘music interventions may have beneficial effects on anxiety, pain, mood, and QoL’ in such patients (Bradt et al., 2011). Similar conclusions were presented by Zhang et al. (2012) for patients with cancer, and by Kamioka et al. (2014) and Staricoff and Clift (2011) for patients in all diagnostic categories including cancer. The assessment by Kamioka et al. is particularly notable for focusing on systematic reviews based on randomised controlled trials. The positive effects of music on psychological and physiological outcomes seem to extend to family members of patients as well (e.g. Gallagher et al., 2017).
Patients: active exposure to music
Teaching patients with COPD to sing or play music appears to improve their quality of life, as inferred from quality of life indices and some physiological outcomes (Panigrahi et al., 2014). The empirical basis for this topic, however, seems rather limited.
Health care providers: passive exposure to music
The benefit from music in health care is not restricted to patients. A systematic review by Moris and Linos (2013) suggests that surgeons’ heart rate, blood pressure and muscle effort are also enhanced by music in the operating theatre, and that ambient music serves to increase the accuracy with which surgical tasks are performed. Another potential application is exemplified by Butler (2009), who showed how medical students, not usually very experienced in dealing with grief and mourning, can be assisted in learning about these subjects by listening to and discussing relevant rock ‘n’ roll songs (such as Dead man’s curve by Jan and Dean).
Health care providers: active exposure to music
Moris and Linos (2013) report two studies showing how playing musical instruments facilitates surgeons in learning and performing surgical tasks. Similarly, a study by Boyd et al. (2008) shows how surgeons’ experience of playing musical instruments is associated with improved quality of laparoscopic skills.
In her book Scales to Scalpels: Doctors Who Practice the Healing Arts of Music and Medicine, Wong (2012) discusses an orchestra comprising health care providers. She argues that a passion for music impacts the orchestra members’ clinical work in positive, ‘healing’ ways. Another fascinating publication in this domain is Rueger’s (1991) The Musical House Apothecary, in which the author categorises classical music into ‘recipes for body, soul and mind’, and suggests appropriate music for clinicians to prescribed for conditions ranging from anxiety to depression, loneliness, mourning, spleen conditions and suicide.
Discussion
Our review focuses on an emerging area of study, but allows a number of clear, albeit cautious, conclusions. First, the area is developing at an accelerating rate, with higher quality evidence (such as extensive systematic reviews and meta-analyses) appearing in more recent publications. In addition, these publications pertain to all four art genres, and to both categories of respondents, in active and passive roles. The least well-developed category is ‘health care providers, active’; medical students, physicians and other health care providers have not yet been targeted by research on expressive writing, photovoice/film making, painting or music making to any substantial extent. We suggest that this lag reflects a prevailing biomedical view on health and illness in these circles.
By and large, the evidence supports the cautious conclusion that patients involved, either actively or passively, in reading and writing novels, watching and directing films, painting and observing paintings, and consuming or producing music, experience beneficial effects in various domains. The evidence to date justifies further research in these areas. It is widely acknowledged that health care requires more than undergoing or ordering tests, swallowing or prescribing medication, and being subjected to or performing invasive procedures. We suggest that comprehensive health care should also involve talking, reading, writing, watching films or expressing illness in photos, observing paintings or painting one’s medical situation and listening to music or performing it.
Our paper consolidates previous work by, for example, Ousager and Johannessen (2010), who broadly present similar conclusions. However, our review is somewhat more ambitious in focusing not only on medical students but also on other categories of health care providers, and in examining four art genres.
One significant challenge in this area, as previously raised by some critics, will be in effectively operationalising ‘benefit’. The attempt to do so occasionally elicits accusations of antiscience, especially from critics of the ‘narrative medicine’ fields, who claim that fields such as narrative medicine lack value (e.g. O’Mahony, 2013; Strawson, 2004). Other scepticism appears to arise from ardent attachment to the biomedical tradition. For example, in criticising one LitMed paper, an editorial by Schneiderman and Schneiderman (1995) bemoaned the fact that ‘only two of its seven authors are physicians’ (p. 618). They also argue that ‘Literature can be intimidating to anybody, certainly to those of us (sic) whose backgrounds are largely scientific (sic)’ (p. 618), as though literary scientists are dispositionally ill-equipped to appreciate empirical research. This seems to strongly imply an a priori assumption that the aesthetic dimensions of the literature are alien and, therefore, of little value, to medicine.
We limited ourselves to four art genres and did not include poetry or drama (see, for example, Boydell et al., 2012, for work on drama, photo and theatre). There are even studies of how certain medical conditions are represented in stamps and posters (e.g. Lefrère and Danic, 2009), reminding us that artistic depictions of illness in wider culture may also affect patients, even outside the direct context of a structured intervention.
Further development of this area will benefit from the more elaborate embedding of empirical studies within strong theoretical models and theories. Suggestions can be derived, for example, from the Common Sense Model of Self-Regulation. For example, drawing on this model, De Brún et al. (2015) used newspaper articles, radio discussions and online news articles to frame their study of portrayals of overweight. They maintain that such analyses are particularly useful in research and interventions aimed at reducing overweight and obesity. In a similar vein, the novel The Breath: A Decision by Thomas Bernhard was analysed in an effort to study the literary portrayal of respiratory illness (Kaptein and Lyons, 2010). Kidd and Castano’s (2013) ‘ToM’ seems helpful in considering findings on the beneficial effects of various art activities in medical settings. Mar (2011) discusses the neural bases of social cognition of story comprehension, exploring whether and where regions in the human brain are involved with ‘ToM’. McCrae et al. (2013) offer their Five-Factor model as a paradigm to consider personality factors in both fictional and factual contexts. And Murray is a long-time proponent of health psychology theory in research on the subject of art and narrative psychology (Murray, 2000; Murray and Gray, 2008). Hughes (2016) in his Rethinking Psychology emphasises the need for using high-quality research in this area.
Clinical implications of our review can also be considered. One suggestion is to draft training syllabi for teaching and professional development of both professionals-to-be (i.e. students in health and medicine) and practising health care professionals, detailing research about how novels, films, paintings and music can be helpful in clinical care. Applying the four art genres to patients with various medical conditions might help them and their relatives to live with illness. One can only hope that imagination, art and compassion will find their way into mainstream medical care in the end – health psychology appears to be able to contribute to the field, in content, methodology and theoretical considerations. The Common Sense Model (Figure 1) with the addition of EW/ED, ToM and PNI offers a wealth of research and clinical opportunities. Health psychology, in particular, with its potential of solid theoretical and empirical work, seems perfectly suited to play a major role in the further development of health humanities.