
Abstract
The study analyses factor structure and psychometric properties of the Italian version of the Fertility Problem Inventory–Short Form. A sample of 206 infertile couples completed the Italian version of Fertility Problem Inventory (46 items) with demographics, State Anxiety Scale of State-Trait Anxiety Inventory (Form Y), Edinburgh Depression Scale and Dyadic Adjustment Scale, used to assess convergent and discriminant validity. Confirmatory factor analysis was unsatisfactory (comparative fit index = 0.87; Tucker-Lewis Index = 0.83; root mean square error of approximation = 0.17), and Cronbach’s α (0.95) revealed a redundancy of items. Exploratory factor analysis was carried out deleting cross-loading items, and Mokken scale analysis was applied to verify the items homogeneity within the reduced subscales of the questionnaire. The Fertility Problem Inventory–Short Form consists of 27 items, tapping four meaningful and reliable factors. Convergent and discriminant validity were confirmed. Findings indicated that the Fertility Problem Inventory–Short Form is a valid and reliable measure to assess infertility-related stress dimensions.
Introduction
Infertility is clinically described as a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse (Zegers-Hochschild et al., 2009) affecting 9%–15% of couples worldwide (Boivin et al., 2007) and 10%–12% of couples in Italy (ISTAT, 2015). Several studies highlighted that infertility is a deeply distressing experience affecting quality of life (Aarts et al., 2012; Huppelschoten et al., 2013; Monga et al., 2004; Onat and Beji, 2012; Ozkan et al., 2015; Shindel et al., 2008), self-esteem (Daniluk and Hurtig-Mitchell, 2003) and quality of marital and sexual relationships (Nelson et al., 2008; Repokari et al., 2007; Wischmann and Thorn, 2013; Yazdani et al., 2016), and inducing mood disorders, anxiety and depression (Luk and Loke, 2015; Peterson et al., 2013; Williams et al., 2007; Wischmann et al., 2001).
Referring to Lazarus and Folkman’s (1984) transactional model of stress process, in the last decades, several studies developed different measures to explore stress dimensions in infertile patients (Abbey et al., 1991; Bernstein et al., 1985; Collins et al., 1992; Glover et al., 1999).
The Infertility Questionnaire (IFQ; Bernstein et al., 1985) consists of 21 items and was the first method developed to assess the psychological dysfunctions related to infertility with particular reference to three major areas, that is, self-esteem, blame and guilt, and quality of sexual life. Further tools examined specific life domains associated with the infertility experience. In particular, the Fertility Problem Stress Inventory (FPS; Abbey et al., 1991) consists of 14 items evaluating infertility-related stress covering the three dimensions of personal, social (i.e. family, friends and colleagues) and marital stress in infertile couples; the Infertility Reaction Scale (IRS; Collins et al., 1992) consists of 15 items and aimed at exploring the emotional reactions to infertility in terms of social pressure and sexual relationship. Finally, The Fertility Adjustment Scale (Glover et al., 1999) consists of 12 items aimed at assessing psychological reactions to fertility-related problems, mainly focusing on need for parenthood (e.g. importance to have a child) and the rejection/adjustment to a future life without a child, with only one item assessing the quality of couples’ relation in terms of communication.
All measures described has been considered adequate in terms of patients’ burden, due to the number of items included; nevertheless, each of them focused only on some specific dimensions of infertility-related stress.
In this perspective, the Fertility Problem Inventory (FPI; Newton et al., 1999) has been conceived as the first multidimensional questionnaire to assess all dimensions previously emphasized, that is, personal concern related to need for parenthood and rejection/adjustment to a future without a child; social concern related to perceived stress in relationships with family, friends and colleagues; and sexual and couple relationship concern.
The original version of the FPI was obtained by following a sequential strategy of scale construction and selecting all items able to enhance convergent and discriminative validity. The final 46-item questionnaire consisted of five scales identified as Sexual Concern (Sex; that is, diminished sexual enjoyment or sexual self-esteem, and sexual relations difficulties); Social Concern (Soc; that is, sensitivity to comments and reminders of infertility, feelings of social isolation and alienation from family or peers); Relationship Concern (Rel; that is, difficulty talking about infertility and concerns about the impact of infertility on the relationship); Need for Parenthood (Need; that is, perception of parenthood as primary or essential goal of life and close identification with role of parent); Rejection of Childfree Lifestyle (Rej; that is, perception of future satisfaction or happiness as dependent on having a child and negative view of childfree lifestyle). A composite measure of Global Stress was derived by summing the scores of all five scales. All five scales and the composite total scale revealed adequate levels of internal consistency, test–retest reliability, convergent validity (e.g. significant correlations with perceived anxiety, depression and dyadic adjustment) and discriminative validity (i.e. significant and low intercorrelations between the five scales). Finally, the authors of the test demonstrated that patterns of infertility-related stress assessed by the five scales of FPI differed depending on demographic and infertility-related characteristics.
The FPI identifies and measures significant domains of infertility-related stress. Research revealed that personal and marital stress dimensions significantly associated with treatment outcomes (Boivin and Schmidt, 2005; Cooper et al., 2007); moreover, it emerged significant gender differences concerning the effects of self-related stress dimensions on perceived levels of anxiety and depression (Lykeridou et al., 2009; Peterson et al., 2007), marital satisfaction (Peterson et al., 2003) and resilience processes (Herrmann et al., 2011; Sexton et al., 2010).
Validation studies of FPI have been proposed in different countries such as Greece (Gourounti et al., 2011), China (Peng et al., 2011), Portugal (Moura-Ramos et al., 2012) and Korea (Kim and Shin, 2014), substantially confirming the original structure of the questionnaire.
In Italy, the first validation study (Donarelli et al., 2015) didn’t confirm the original multidimensional structure of the test, and post hoc explorative factor analysis, conducted to determine the model of best fit, extracted two factors explaining 25% of variance. The first factor contained 29 items merging all the items from Relational Scale, Sexual Scale and most of the items from Social Scale of the original version, and it has been labelled Infertility Life Domain (α = 0.85). The second extracted factor consisted of 14 items merging the original scale of Rejection of Childfree Lifestyle and Need for Parenthood, and it has been labelled Importance of Parenthood (α = 0.80). Therefore, the original factor structure of the FPI has been only partially supported by this study, which reduced the dimensions explored by the test merging them into two factors.
In this perspective, this study moved both from the interest in the multidimensional structure of the FPI and from the consideration of the great burden of the 46-item original questionnaire. Therefore, it aimed to re-examine psychometric properties and factorial structure of the Italian version of the test in order to develop a valid and reliable Fertility Problem Inventory–Short Form (FPI-SF).
Methods
Study design and participants
The study protocol was approved by the Ethical Committee of the University were this study took place, and research was performed in accordance with the Declaration of Helsinki.
A cross-sectional study was conducted with the aim to re-examine psychometric properties and factor structure of the Italian version of FPI and to validate a short-form, comparing infertility-related stress dimensions emerged with respect to both individual characteristics of patients (gender, age and educational level) and infertility-related characteristics (type of diagnosis, presence of previous treatments and infertility treatment period).
The study was conducted between April 2015 and September 2016. Chairman of different Italian Centres of Assisted Reproduction of Naples (six centres), Udine (one centre) and Brescia (two centres) were contacted to enlist their participation to the project and gave the authorization for submitting a questionnaire to the infertile couples undergoing treatments in their centres. Inclusion criteria were as follows: (a) couples who had been diagnosed with infertility (Male Factor; Female Factor; Combined Male and Female Factor; and Unexplained); (b) couples who were undergoing an infertility treatment of intrauterine insemination (IUI) or in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI); c) the agreement by both members of the couple to participate in the study in order to consider couple sharing infertility problems as research unit. About 500 subjects (both partners of 250 couples) were asked by their physician to participate in the study before their appointment. If one or both partners refused to complete the survey, they were not included in the final data set; therefore, 12 couples with males not responding and 32 couples with no response from either partners were excluded. Overall, 206 couples (206 male, 206 female) completed the questionnaire (response rate = 82.4%).
The questionnaire lasting 20–25 minutes (one session) was submitted individually to both members of the infertile couples in a quiet room setting in the medical centre, and one of the authors was always present to answer any queries raised by participants. The respondents were informed of the objectives of the study, and informed consent was obtained from all participants. The couples voluntarily and anonymously participated in the survey, and received no compensation for their collaboration.
Measures
A questionnaire composed of five sections was submitted. Section 1 included items pertaining to socio-demographics (age, sex, educational level) and data on type of diagnosis (Male Factor; Female Factor; Combined Male and Female Factor; and Unexplained), presence of previous treatments (No/Yes) and infertility treatment period (≤ 1 year/>1 year). Data provided by the participants were double checked with those reported by the physicians. Section 2 consisted of the Italian version of the FPI (Donarelli et al., 2015), a self-administrated measure composed of 46 items on a 6-point Likert scale ranging from one (Strongly disagree) to six (Strongly agree), which provides a Global Stress score of perceived infertility-related stress ranging from 46 to 276. Section 3 consisted of the State scale of the State-Trait Anxiety Inventory (State-Trait Anxiety Inventory (Form Y) (STAI-Y); Spielberger, 1972), used to assess perceived levels of State Anxiety related to infertility in accordance with the literature (Csemiczky et al., 2000; Donarelli et al., 2015; Newton et al., 1999). The scale consists of 20 items rated on a 4-point scale ranging from one (Not at all) to four (Very much); total score ranges from 20 to 80. The STAI-Y has been adapted to Italian (Pedrabissi and Santinello, 1989) and has been found to have satisfactory psychometric properties (Cronbach’s α = 0.91) and construct validity; the cut-off point for the Italian version of State Anxiety Scale were, respectively, 36.00 for male patients and 39.93 for female patients. Section 4 included the Edinburgh Depression Scale (EDS; Murray and Cox, 1990) which consists of 10 items rated on a 4-point scale ranging from zero (Not at all) to three (Most of the time); total score ranges from 0 to 30. The EDS has been adapted to Italian (Benvenuti et al., 1999) and has been found to have satisfactory psychometric properties (Cronbach’s α = 0.78) and construct validity; the cut-off point for the Italian version was 9. Section 5 included the Dyadic Adjustment Scale (DAS; Spanier, 1976) which consists of 32 items rated on a 6-point scale ranging from zero (Always disagree) to five (Always agree); total score ranges from 0 to 160. The DAS has been adapted to Italian (Gentili et al., 2002) and has been found to have satisfactory psychometric properties (Cronbach’s α = 0.93) and construct validity; the cut-off point for the Italian version was 115.7.
Statistical analysis
Descriptive statistics, factor analysis, Pearson’s correlations and analyses of variance (ANOVAs) were tested using SPSS version 21. Confirmatory factor analysis (CFA) was carried out using AMOS version 21. We considered different parameters of model fit: χ2 non-significant (p > 0.05), Tucker-Lewis Index (TLI > 0.95), root mean square error of approximation (RMSEA < 0.08) and comparative fit index (CFI > 0.95) (Hu and Bentler, 1998).
On the basis of data emerged, an exploratory factor analysis (EFA) using principal axis factoring analysis with oblique promax rotation was performed to improve the fit of the model with our data. The choice of non-orthogonal rotation was justified on the hypothesis that the factors would be correlated. The factorability of the correlation matrix of the FPI was evaluated by Kaiser–Meyer–Olkin (KMO) measure and Barlett test of sphericity. Criteria for extraction and interpretation of factors were as follows: eigenvalues >1.0, Cattell’s scree test and inspection of scree plot, communality ≥0.30 for each item and factor loading >0.32 for each item loading on each factor (Costello and Osborne, 2005). CFA was performed to assess the robustness of the structure of the FPI-SF derived from the EFA. Moreover, Mokken scale analysis was carried out using the R package ‘Mokken’ to further validate the emerged version of FPI-SF verifying the items homogeneity within the reduced subscales of the questionnaire. The scale’s and items’ Loevinger’s scalability coefficients (H and Hi, respectively) were considered adequate if H > 0.30 (high degree of homogeneity of the set of items) and Hi > 0.30 for all items (item consistent with the set of items) (Sijtsma and Van der Ark, 2017; Stochl et al., 2012).
Finally, Convergent validity was assessed by analysing the correlations of FPI-SF subscales and Global Stress scores with the standardized scales scores of STAI-Y, EDS, and DAS. Discriminant validity was evaluated by exploring the intercorrelations between the subscales, and ANOVA tests were used to analyse differences in FPI-SF subscales and Global Stress mean scores between subgroups of infertile patients divided by sex, age (the mean age of 34 years was used as a cut-off point), educational level (Junior Middle School; Senior School; College), type of diagnosis (Male Factor; Female Factor; Combined Factor; Unexplained Factor), previous treatments (No/Yes) and infertility treatment period (1 year has been considered as a cut-off point in accordance with the literature; Kim and Shin, 2014).
Results
Characteristics of participants
The study was carried out in a sample of 206 Italian infertile couples. The ages of participants ranged from 22 to 48 years (Mean = 34.40, standard deviation (SD) = 3.85). All the 206 couples recruited had a diagnosis of primary infertility and 119 (57.7%) of them have undergone previous treatments. All demographic and infertility-related characteristics are provided in Table 1.
Demographic and infertility-related characteristics of participants (N = 206 couples).

IVF: in vitro fertilization; ICSI: intracytoplasmic sperm injection; IUI: intrauterine insemination.
Item analysis of the original version of FPI
Preliminarily, the symmetrical distribution of item scores (skewness and kurtosis values) and the internal consistency (Cronbach’s α) were evaluated. The analysis produced values of skewness, and kurtosis for all items between −1.5 and 1.5, showing a normal distribution of scores.
The FPI revealed a very high Cronbach’s α (0.95), suggesting a redundancy of the items of the full questionnaire (Briggs and Cheek, 1986); indeed, a maximum α value of 0.90 is recommended (Tavakol and Dennick, 2011). Therefore, concerning the five subscales, two subscales had good internal consistency: that is, Rejection of Childfree Lifestyle (α = 0.87) and Need for Parenthood (α = 0.89), and three had poor internal consistency: that is, Social Concern (α = 0.50), Sexual Concern (α = 0.47) and Relationship Concern (α = 0.43).
CFA
The theoretical model of the FPI (Newton et al., 1999) was tested by CFA, which indicated a low fit between data collected and the theoretical model: χ2 value statistical significant (p < 0.05), CFI = 0.87, TLI = 0.83, RMSEA = 0.17. These results of CFA, the redundancy of items revealed by the high Cronbach’s α of the questionnaire and the low Cronbach’s α of three subscales of FPI suggested to carry out some modifications of the model in an attempt to improve it. In these cases, the procedure recommended is exploratory rather than confirmatory analysis (Browne, 2001). Consequently, an EFA was conducted to assess the structure of FPI and to improve its validity, internal consistency and discriminative capacity by removing redundant items.
EFA
The EFA was conducted using principal axis factoring analysis with oblique promax rotation. The assessment of factorability showed that the Kaiser–Meyer–Olkin measure was 0.83 and Barlett’s test of sphericity was significant (p < 0.001) indicating that the data were adequate for the factor analysis. The examination of the scree plot produced a departure from linearity corresponding to a four-factor result; the scree test also confirmed that our data should be analysed for four factors. The first four eigenvalues were 7.74, 4.04, 2.81 and 1.34. The four-factor solution explained a variance of 35% from a total of 46 items, with 6 items having cross loadings (items 4, 7, 13, 20, 24, 38) and 13 items having communality <0.32 (items 1, 2, 3, 8, 9, 11, 12, 14, 18, 26, 32, 33, 37). After eliminating these 19 items, a re-run of the model produced a cleaner solution with 27 items and four factors which had an explained variance of 44%. The first four eigenvalues were 5.87, 3.17, 1.90 and 1.0. The scree test supported that our data should be examined for four factors. With a KMO of 0.85, the overall fit of the model was found to be adequate (χ2 = 4.406.144, df = 351, p < 0.001). The first factor (10 items, explained variance = 21.76%, Cronbach’s α = 0.88) was loaded by items referred to sensitivity to comments and reminders concerning infertility and feelings of social isolation. This factor corresponded to the scale of Social Concern of the original version. The second factor (six items, explained variance = 11.75%, Cronbach’s α = 0.78) was loaded by items referred to the perception of parenthood perceived as an essential goal in life. We labelled this scale Need for Parenthood as in the original version of the test. The third factor (six items, explained variance = 7.03%, Cronbach’s α = 0.77) was loaded by items concerning negative view of childfree lifestyle and perception of future happiness as dependent on having a child. This factor corresponded to the scale of Rejection of Childfree Lifestyle of the original version. The fourth factor (five items, explained variance = 3.45%, Cronbach’s α = 0.70) was loaded by items referred to difficulties in talking about infertility, concerns about the impact on couple relationship and sexual relations difficulties. This factor grouped the two scales (Relationship Concern and Sexual Concern) of the original version of FPI (Newton et al., 1999); consequently, we labelled it Couple’s Relationship Concern (Table 2). The Confirmatory Factors Analysis revealed satisfactory fit of the data structure emerged with the model (χ2 is not significant p > 0.05; CFI = 0.97; TLI = 0.96; RMSEA = 0.05). Moreover, the Mokken scale analysis revealed adequate scalability for all items and subscales of the test, highlighting that the scale level Loevinger’s coefficients were higher than 0.30 for all the four subscales (Social Concern H = 0.46, Need for Parenthood H = 0.39, Rejection of Childfree Lifestyle H = 0.38, Couple’s Relationship Concern H = 0.39) and that item level Loevinger’s coefficients were higher than 0.30 for all the 27 items.
Factor structure of the 27-item Fertility Problem Inventory–Short Form (FPI-SF).
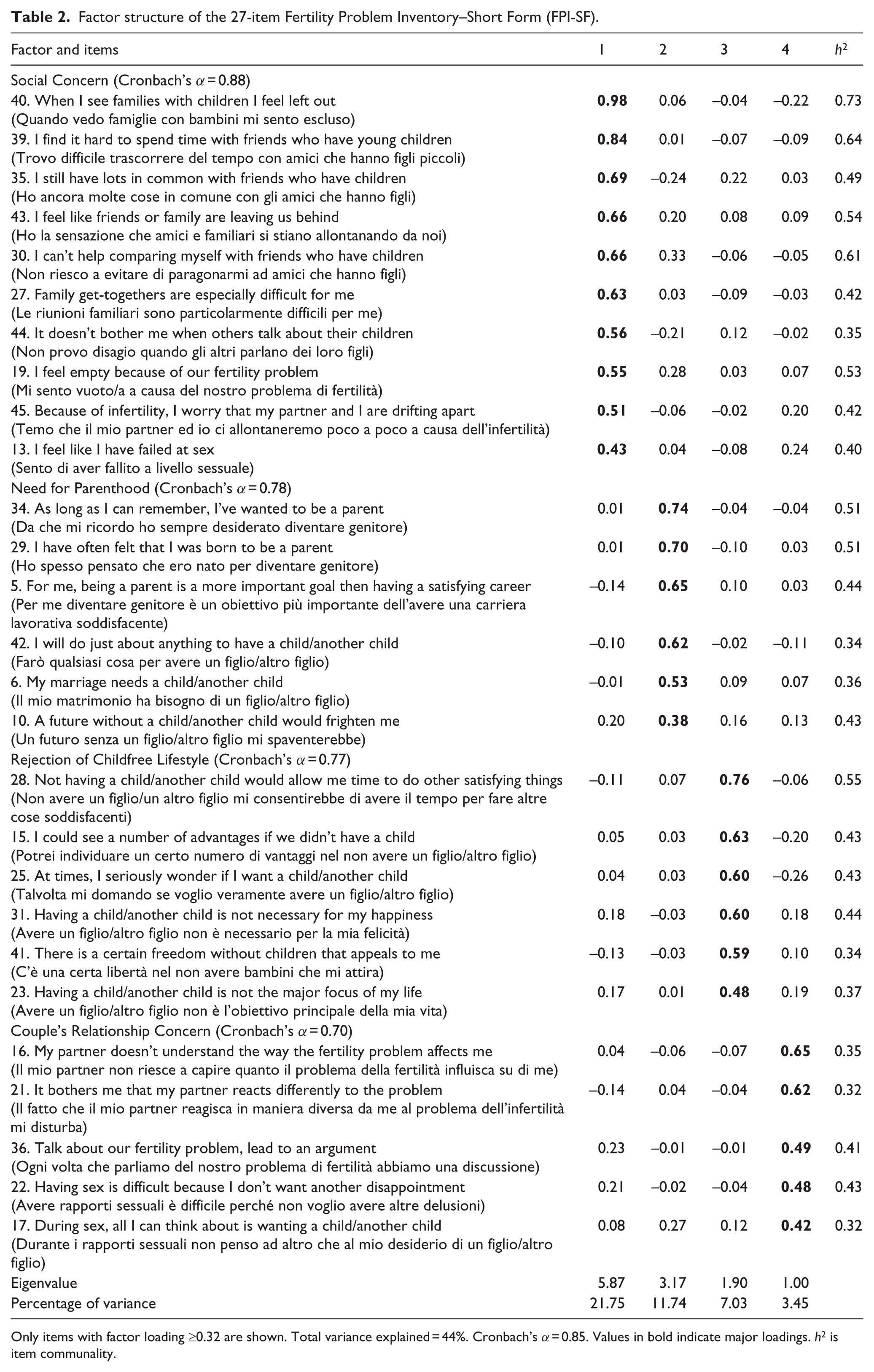
Only items with factor loading ≥0.32 are shown. Total variance explained = 44%. Cronbach’s α = 0.85. Values in bold indicate major loadings. h2 is item communality.
Table 3 illustrates items, means, SD and ranges of the FPI Short-Form subscales and the total scale (Global Stress), useful to achieve normative scores. Considering that high levels of infertility-related stress can be indicated by scores that are 1 SD above the mean (e.g. the 84th percentile) and low levels of stress can be indicated by scores that are 1 SD below the mean (e.g. the 16th percentile) of the normal distribution of the FPI-SF scores, we can affirm that scores of 72 or below indicate low infertility-related stress, scores of 73–111 indicate average infertility-related stress and scores of 112 or more indicate high infertility-related stress.
Items, mean, SD and range scores of Fertility Problem Inventory–Short Form scales.

FPI-SF: Fertility Problem Inventory–Short Form.
Item analysis of the FPI-SF
Following the analysis of the factor structure of the FPI, the emerged new short version of the questionnaire has been submitted to item analysis. Mean scores for the single items varied from a maximum score of 4.78 (Item 5: ‘Being a parent is a more important goal than having a satisfying career’) to a minimum of 1.81 (Item 22: ‘Having sex is difficult because I don’t want another disappointment’). SDs for the single items varied from 2.02 (Item 44: ‘It doesn’t bother me when others talk about their children’) to 1.26 (Item 22: ‘Having sex is difficult because I don’t want another disappointment’). The skewness and kurtosis varied from −1.5 to 1.5, indicating a normal distribution of the scores. Item total correlation was significant for all items (0.20 < r< 0.74; p ≤ 0.001), and the mean inter-item correlation 0.18 was satisfactory (Clark and Watson, 1995). Cronbach’s α of the total scale was 0.85. The overall findings of item analysis accounted for adequate reliability of the Italian FPI-SF.
Convergent and discriminant validity
Correlations with measures of State Anxiety (STAI-Y), Depression (EDS) and Dyadic Adjustment (DAS Tot) were carried out to test convergent validity, showing that all FPI-SF subscales and Global Stress scores were significantly related in the expected directions (Table 4).
Correlations of Fertility Problem Inventory–Short Form scales with State Anxiety, Depression and Dyadic Adjustment scales.

p < 0.05; **p < 0.01.
Concerning discriminant validity, intercorrelations between the scales of FPI-SF and correlations between the four subscales and the Global Stress scores were calculated (Table 5). Intercorrelations ranged from 0.04 to 0.46, showing low to moderate levels (Cohen, 1988) and correlations of all FPI-SF subscales with Global Stress scores were high in size and significant, indicating that the questionnaire assessed different but related dimensions.
Intercorrelations between Fertility Problem Inventory–Short form (FPI-SF) scales.

p < 0.05; **p < 0.01.
Moreover, ANOVA tests (Table 6) showed, concerning demographic characteristics, that female infertile patients perceived significantly higher levels of Need for Parenthood and Global Stress; both male and female infertile patients >34 years reported higher levels of Need for Parenthood and Global Stress, and both male and female infertile patients with higher educational levels revealed higher levels of Social Concern and lower levels of Need for Parenthood and Rejection of Childfree Lifestyle. Moreover, concerning infertility-related characteristics, Male Factor was associated with higher levels of Social Concern, Need for Parenthood, Couple’s Relationship Concern and Global Stress in male patients; Female Factor was associated with higher levels of Need for Parenthood, Rejection of Childfree Lifestyle, Couple’s Relationship Concern and Global Stress in female patients; and Combined Factor was associated with higher levels of all subscales and Global Stress in both male and female patients. Finally, infertility treatment period >1 year was associated with higher levels of Social Concern, in male patients, with higher levels of Couple’s Relationship Concern, in female patients and with higher levels of Need for Parenthood, Rejection of Childfree Lifestyle and Global Stress both in male and female patients.
Differences in the Fertility Problem Inventory–Short Form scales scores by gender, age, educational level, type of diagnosis, presence of previous treatments, infertility treatment period.

p < 0.05; **p < 0.01.
Discussion
Findings highlighted that the proposed Italian FPI-SF possessed adequate factor validity and reliability, tapping four meaningful and reliable factors which allowed to substantially confirm the original multidimensional structure of the FPI (Gourounti et al., 2011; Kim and Shin, 2014; Moura-Ramos et al., 2012; Newton et al., 1999; Peng et al., 2011). Three dimensions of the original version, that is, Social Concern, Need for Parenthood and Rejection of Childfree Lifestyle, were confirmed in the FPI-SF, and two dimensions, that is, Relationship Concern and Sexual Concern scales, merged in one factor, consequently labelled Couple’s Relationship Concern, overall highlighting a structure of FPI-SF which agrees with the four-factor structure emerged from the Greek validation study of the FPI (Gourounti et al., 2011).
The final 27-item version of FPI-SF showed a satisfactory fit of the data structure with the theoretical model of the test and an excellent internal consistency, offering the further relevant advantages of being a synthetic and abbreviated valid version of FPI for use in clinical practice and research. In this perspective, the analysis of convergent validity of FPI-SF revealed significant associations of all its subscales scores with perceived levels of State Anxiety, Depression, and Dyadic Adjustment in the expected directions, and the discriminant validity analyses confirmed that all scales assessed different but connected dimensions of infertility-related stress. Finally, the FPI-SF allowed the assessment of all infertility-related stress dimensions of the construct differentiated by individual characteristics of gender, age, educational level, and by infertility-related characteristics of type of diagnosis and duration of infertility.
In particular, data provided important information from a clinical point of view, highlighting several differences in stress dimensions by gender and type of diagnosis, the protective role of educational level and the duration of infertility treatment period as significant risk factor. In this perspective, the FPI-SF could be usefully applied to assess risk and protective factors and to define more focused interventions.
Despite these merits, some limitations need to be underlined. First, the test–retest reliability of the FPI-SF was not covered in this study, so that actually it is not possible to evaluate the temporal stability of our measures. Second, the study revealed some significant effects of individual characteristics and infertility-related characteristics that should be object of further analysis and investigations. Moreover, further studies should be developed to better explore the effects of responsiveness to treatments (i.e. success or failure of treatments) on infertile patients’ perceived levels of stress. Finally, considering that cultural and social variables may influence quality and intensity of infertility-related stress dimensions, future studies should be conducted using the FPI-SF with different infertile populations.
Despite these limitations, the FPI-SF constitutes a synthetic, reliable and valid multidimensional measure to assess stress dimensions among infertile patients in clinical practice and research, to define evidence-based interventions aiming to reduce infertility-related stress, non-compliance and discontinuation in Assisted Reproduction Treatment, and to promote individual and couples’ psychological health in infertile patients.
Footnotes
Acknowledgements
The authors wish to thank all the study participants for completing the questionnaire.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.