
Abstract
Growing evidence indicates that self-compassion is associated with better physical health, but the pathways that mediate this relationship are not well understood. This study tested a serial mediation model that linked self-compassion, perceived stress, health behaviors, and a comprehensive index of physical health. A sample of 176 individuals completed an online survey posted on Amazon’s Mechanical Turk. Self-compassion had an indirect effect on physical health via both mediators and through the sequential pathway, suggesting that taking a kind, accepting and mindful stance toward one’s flaws and failures may have benefits for reducing stress and promoting health behaviors.
Introduction
In the past decade, self-compassion has emerged as an important quality for mental health and well-being. This construct, defined as treating oneself with kindness and nonjudgmental acceptance in response to perceived challenges and failures (Neff, 2003), shows consistent relationships with a wide range of desirable psychological attributes (MacBeth and Gumley, 2012; Neff et al., 2007a). Growing evidence indicates that self-compassion is also associated with several key health-related outcomes including lower perceived stress (Allen and Leary, 2010; Sirois et al., 2015b), attenuated physiological responses to stress (Arch et al., 2014; Breines et al., 2014), the practice of health-promoting behaviors (Dunne et al., 2016; Sirois et al., 2015a; Terry et al., 2013), and better physical health (Brown et al., 2016; Dunne et al., 2016; Hall et al., 2013). However, the evidence base demonstrating the benefits of self-compassion for health is outpacing research into the pathways and processes that might account for this association. The limited evidence to date suggests that engagement with health-promoting behaviors may explain why self-compassionate people experience better physical health (Dunne et al., 2016), and that lower levels of negative affect account for the link between self-compassion and better health behaviors (Sirois et al., 2015a). In light of the consistent relationships between perceived stress and physical health (Cohen et al., 2007; McEwen, 2007), and between stress and poor health behaviors (Cohen et al., 1983; Sirois, 2007), it is plausible that lower perceived stress is involved in the pathway connecting self-compassion to health behaviors and physical health. The purpose of this study was to test this idea.
Self-compassion and stress
Self-compassion is commonly conceptualized as including three key components (Neff, 2003), each of which can have benefits for reducing stress. Self-kindness refers to responding to perceived inadequacy or disappointment with understanding, patience, and acceptance, rather than with harsh self-criticism. This response presumably defuses negative emotions and helps the individual to reinterpret stressful events in a self-supportive way. Common humanity refers to the recognition that all people are imperfect, make mistakes, and experience failure. As a result of this recognition, self-compassionate people do not feel isolated by the experience of failure or struggle, but recognize that stressful events are part of the human experience. Appraising difficult events from this perspective would likely reduce the perception of threat that contributes to stress, as well as reduce the barriers to seeking help when in times of need (Allen and Leary, 2010; Sirois et al., 2015b). Finally, mindfulness refers to not becoming over-identified with the negative feelings that can arise after failure or during struggles, but maintaining a balanced sense of awareness of those feelings. This mindset can help reduce stress by minimizing rumination over the negative aspects of events. Together, the components of self-compassion are posited to reduce stress by enhancing the self-regulation of negative emotions that can result from failures and unexpected events (Neff et al., 2007a).
Substantial evidence supports the idea that self-compassion can reduce perceived stress. The link between self-compassion and lower stress has been well documented based on self-report measures (Allen and Leary, 2010; Brion et al., 2014; Finlay-Jones et al., 2015; Pinto-Gouveia et al., 2014; Sirois, 2014; 2015b), and interventions designed to increase self-compassion produce simultaneous decreases in perceived stress (Neff and Germer, 2013). Studies employing physiological measures have also supported this relationship. For example, persons with higher self-compassion show lower sympathetic nervous system activation and reduced inflammatory response following exposure to a lab stressor, even after accounting for demographics, depressive symptoms, and distress (Breines et al., 2014, 2015). They also demonstrate greater heart rate variability, an index of parasympathetic influence on the heart which reflects greater ability to return to a resting state following acute stress (Svendsen et al., 2016). Finally, an experimental study found that brief training in self-compassion dampened young women’s psychobiological responses to a social evaluative threat relative to two control conditions (Arch et al., 2014). Specifically, women who listened to a 10-minute recording encouraging self-compassionate attitudes once a day for 4 days showed reduced sympathetic nervous system reactivity (salivary alpha amylase), greater heart rate variability, and lower self-reported anxiety. Because chronic activation of the physiological stress response has been shown to have a detrimental effect on health (Cohen et al., 1983, 2007; McEwen, 2007), these findings suggest that both dispositional self-compassion and induced state self-compassion can protect health by mitigating this activation.
In addition to having a direct influence on physical health through psychophysiological pathways (Cohen et al., 1983; McEwen, 2007), stress can influence health indirectly through its effects on health behaviors. As people attempt to cope with stress, they may engage in behaviors that bring short-term relief, such as smoking, drinking alcohol, or consuming high-calorie, highly processed foods (Ng and Jeffery, 2003; Pak et al., 1999; Steptoe et al., 1998). They also are likely to neglect health-promoting behaviors, such as exercise (Ng and Jeffery, 2003; Stults-Kolehmainen and Sinha, 2014), or careful adherence to other medical regimens (e.g. Bottonari et al., 2010). Similar to the direct pathway, this indirect pathway is most detrimental to health when stress is prolonged and the behavioral responses occur over an extended period of time (World Health Organization (WHO), 2014).
Self-compassion, health behaviors, and health
A nascent body of evidence indicates that self-compassion facilitates the practice of a range of important health behaviors. For example, self-compassion is associated with healthy eating behaviors (Adams and Leary, 2007; Schoenefeld and Webb, 2013), exercise behavior (Magnus et al., 2010), smoking cessation (Kelly et al., 2010), dietary adherence (Dowd and Jung, 2017), medical adherence (Brion et al., 2014; Sirois and Hirsch, forthcoming), seeking medical care (Terry et al., 2013), and indices of general health-promoting behaviors (Dunne et al., 2016; Sirois et al., 2015a). The association of self-compassion with health behaviors has been explained in terms of its links to self-regulation (Terry and Leary, 2011), and adaptive regulation of emotions in particular (Sirois, 2015; Sirois et al., 2015a). Self-compassionate people respond to the inevitable failures and setbacks that can occur when trying to change their health behaviors with acceptance rather than judgment (self-kindness) and view their mistakes as something everyone experiences (common humanity) rather than becoming immersed in negative feelings or stressing about their situation (mindfulness; for example, Adams and Leary, 2007). Because negative affect is known to interfere with self-regulation (Sirois, 2015; Wagner and Heatherton, 2015), self-compassionate responding can help people to maintain the practice of health behaviors by tempering negative emotions that may arise in response to health behavior goal setbacks. Evidence supporting this proposition comes from a meta-analysis that found self-compassion was consistently and positively associated with more frequent practice of variety of health-promoting behaviors, such as regular exercise, healthy eating, healthy sleep behaviors, and stress management in 15 samples involving more than 3000 participants (Sirois et al., 2015a). As described previously, self-compassion can also reduce perceived stress, which typically has a substantial subjective distress component and tends to correlate with negative affect (Dohrenwend and Shrout, 1985). For this reason, this study posited that self-compassion would convey a similar positive effect on health behavior through reduced perceived stress.
Self-compassion also appears to be beneficial for physical health. Several studies have linked self-compassion to measures of physical well-being (Hall et al., 2013), physical symptom scores (Dunne et al., 2016), and a composite measure of physical health (Brown et al., 2016). However, aside from one study (Dunne et al., 2016), there has been little research into the reasons why self-compassion is linked to better physical health. Dunne et al. (2016) found that health-promoting behaviors partly explained the association between self-compassion and fewer physical symptoms, but a potential limitation of this finding is that self-reported symptoms tend to be influenced by negative affect. Specifically, although negative affect is consistently related to health complaints as measured by symptom checklists, it is unrelated to many other indices of health, such as frequency of illness, usage of health care, role limitations due to physical health, pathology, or overall mortality (Watson and Pennebaker, 1989). Because self-compassion is consistently associated with lower levels of negative affect (Neff et al., 2007a; Sirois et al., 2015a), it is important to use measures that assess physical health with a range of indicators to avoid artificially inflated estimates of the association between self-compassion and health.
This study
The aim of this study was to test a serial mediation model in which the health-beneficial effects of self-compassion are conveyed through reduced perceived stress and increased health behaviors. A diagram of our proposed model is presented in Figure 1. We hypothesized that self-compassion would be inversely associated with perceived stress, and positively associated with more frequent health behaviors and better physical health. We further predicted that perceived stress would be inversely associated with frequency of health behaviors and physical health, and frequency of health behaviors would show a positive association with physical health. In regard to mediation, we expected that self-compassion would have significant indirect effects on both health behaviors and physical health through perceived stress. Of primary interest, we hypothesized that self-compassion would have a positive indirect effect on physical health through the serial pathway involving reduced perceived stress and increased health behaviors. Importantly, we used a well-validated composite measure of physical health, the RAND-36 (Hays and Morales, 2001), that included not only physical symptoms but also physical functioning, role limitations, and general health.

Proposed serial mediation model linking self-compassion and physical health through perceived stress and health behaviors.
In addition, we tested an alternate model in which the causal ordering of perceived stress and health behaviors was reversed. Previous work has shown that reduced negative affect mediates the relationship between self-compassion and health behaviors (Sirois et al., 2015a), and this finding formed the basis for our original serial mediation model. However, it is also plausible that health behaviors mediate the relationship between self-compassion and perceived stress. In this conceptualization, self-compassion will show a positive association with health behaviors, and in turn, health behaviors will show an inverse relationship with perceived stress. If this model is correct, we expected that self-compassion would have a significant indirect effect on perceived stress through health behavior. However, if this model is incorrect, we expected to see no mediating effect of health behavior.
Methods
Participants and procedure
All procedures were approved by the Institutional Review Board and all participants were treated according to ethical guidelines established by the American Psychological Association. A brief description of the study, including estimated duration and compensation, was posted on Amazon’s Mechanical Turk website. MTurk is a website that provides online “workers” with opportunities to complete online tasks for monetary compensation. It is recognized as a source of quality data for social science research, and tends to provide greater diversity than college samples (Buhrmester et al., 2011). Interested participants were directed to a survey link. Before proceeding, participants were required to indicate that they understood the informed consent information and that they agreed to participate. Following acknowledgment of informed consent, the measures described below were presented in random order. Two attention checks were embedded in the survey (e.g. “To make sure you are paying attention, please answer strongly disagree”), and those who failed either check were not included in the data set. Participants were paid US$2.50 for completing the survey.
The final sample consisted of 176 participants (44.9% female) with an average age of 31.6 years (standard deviation (SD) = 10.1). The majority identified as White (76.9%) with the remaining identifying as Asian-American (11.0%), African-American (8.2%), Latin-American (2.8%), or multiracial (1.0%). In regard to relationship status, 47.4 percent were single, 46.3 percent were in a long-term relationship, and 6.3 percent were divorced. In regard to education level, 57.1 percent had a high school degree or some college, and 42.9 percent had a college degree or higher.
Measures
Self-compassion
The 12-item Self-Compassion Scale–Short Form (Raes et al., 2011) was used to measure self-compassion (e.g. “I try to be understanding and patient towards those aspects of my personality I don’t like”). Items are rated on a 5-point response scale ranging from 1 (almost never) to 5 (almost always). The short form correlates almost perfectly with the original, longer version of the scale and showed good internal consistency among Dutch and American undergraduate students (Raes et al., 2011). Recent psychometric analysis of this instrument has supported the use of the overall score as a general measure of self-compassion (Neff et al., 2017). Items were reversed where necessary and added to create a single self-compassion score. Cronbach’s alpha for this study was .82.
Health outcomes
The RAND 36-Item Health Survey 1.0 (RAND-36; Hays and Morales, 2001) was used to assess physical health. The 36-item scale is made up of eight multi-item scales assessing physical function, role limitations due to physical health problems, pain, general health, vitality, social functioning, role limitations due to emotional problems, and emotional well-being. Scores on the subscales range from 0 to 100, with higher scores indicating greater freedom from disability. The eight subscales can be standardized and weighted to produce two summary measures: the physical component summary (PCS) and mental component summary (MCS) scores (Farivar et al., 2007; Hays and Morales, 2001). Only the PCS was used in this study. The RAND-36 was first developed and tested for the Medical Outcomes Study (MOS), a 2-year study of chronic medical conditions (Ware and Sherbourne, 1992), but it has subsequently been used in numerous studies involving thousands of participants (Hays and Morales, 2001). Ample evidence supports the reliability and validity of the RAND SF-36 (Vander Zee et al., 1996). Internal consistency for the eight subscales that were used to create the weighted PCS ranged from .81 (pain) to .89 (mental health) in this study.
Perceived stress
The 10-item Perceived Stress Scale (PSS; Cohen and Williamson, 1988) was used to assess the perceived stressfulness of events experienced within the past month. Items tapping the degree to which respondents found their lives unpredictable, uncontrollable, and overwhelming (e.g. “In the last month, how often have you felt nervous and stressed”) are rated on a 5-point scale ranging from “Never” to “Very often.” A total perceived stress score was calculated by averaging the items after reverse coding the negative items. The PSS has demonstrated good reliability and validity (Cohen and Williamson, 1988). In this study, Cronbach’s alpha was .92.
Health behavior
General health protective practices were assessed using four subscales from the Health Promoting Lifestyle Profile II (HPLPII; Walker et al., 1995). The 9-item Health Responsibility subscale assesses the extent to which participants assume accountability for their own well-being (e.g. “I discuss my health concerns with health professionals”). The 8-item Stress Management subscale assesses the individual’s efforts to control or reduce tension (e.g. “I pace myself to prevent tiredness”). The 9-item Nutrition subscale asks about healthful eating habits (e.g. “I read labels to identify nutrients in packaged food”) and the 8-item Physical Activity subscale asks about engagement in light, moderate, and/or vigorous physical exercise (“I take part in light to moderate physical activity such as sustained walking five more times a week”). Participants indicate their frequency of each behavior on a 4-point scale (1 = never, 4 = routinely). The HPLPII has good psychometric properties including test–retest reliability, good internal consistency, and validity as evidenced by moderate to large correlations with other measures of lifestyle and perceived health (Walker and Hill-Polerecky, 1996). For this study, all items were averaged to create an overall health behavior composite with higher scores indicating more frequent practice of health-promoting behaviors.
Results
First, data were examined for missing values. One case was deleted due to excessive missing data (more than 20%). Missing data for the remaining cases was very low (<5%). Skew and kurtosis were within recommended limits for regression analysis (i.e. less than 3.0 for skew and less than 10.0 for kurtosis; Kline, 2010). Descriptive statistics for the major study variables and their intercorrelations are presented in Table 1. Self-compassion was positively and significantly correlated with health behavior and physical health and negatively correlated with perceived stress. Perceived stress showed a significant inverse relationship with physical health, and health behavior showed positive associations with health.
Descriptive statistics and intercorrelations for main study variables.
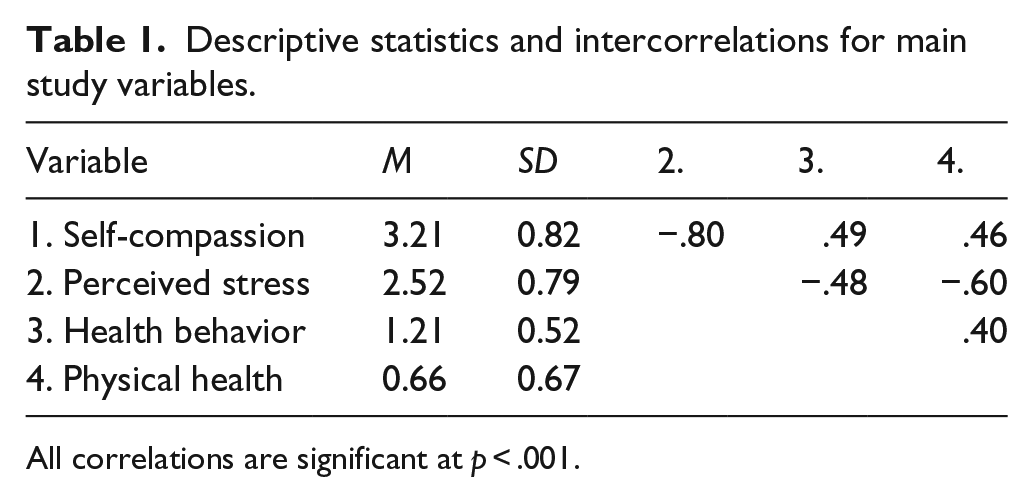
All correlations are significant at p < .001.
The PROCESS macro for SPSS (Hayes, 2013) was used to determine total, direct, and indirect effects of self-compassion, perceived stress, and health-promoting behavior on physical health. A conceptual diagram of the serial mediation model is presented in Figure 2, along with path coefficients. Participant’s sex and age were entered as covariates. Values for the standardized indirect, direct, and total effects of self-compassion on health outcomes are presented in Table 2. The significance of indirect effects was tested using 95 percent confidence intervals based on 5000 bias-corrected bootstrap samples and confidence intervals that did not contain zero were regarded as significant. This procedure is now recommended for testing the significance of indirect effects because it does not require the assumption of normality for the sampling distribution of indirect effects (Hayes, 2009).

Conceptual diagram linking self-compassion and physical health through perceived stress and health behaviors. Values presented are standardized path coefficients with bootstrap standard errors in parentheses.
Summary of serial mediation model linking self-compassion and physical health through perceived stress and health-promoting behavior.

CI: confidence interval; SE: standard error; SC: self-compassion; PS: perceived stress; HB: health-promoting behaviors; PH: physical health.
p < .001.
Consistent with previous work, self-compassion had a significant indirect effect on health behaviors through perceived stress (Sirois et al., 2015a). There was a strong inverse association between self-compassion and perceived stress, and lower stress was associated with more frequent health behaviors. Self-compassion had significant indirect effects on physical health through both perceived stress and health behaviors. People with higher self-compassion tended to perceive lower levels of stress and also tended to engage in more frequent health-promoting behaviors; both of these pathways were related to better physical health. The serial path from self-compassion to physical health via both perceived stress and health behaviors was also significant, supporting the idea that self-compassion leads to lower levels of perceived stress, and lower perceived stress leads to increased frequency of health behaviors. The complete model explained 38 percent of the variance in physical health.
Finally, we tested an alternate model that reversed the order of perceived stress and health behavior (i.e. health behavior was entered as the first mediator and perceived stress was the second; Figure 3). Results are summarized in Table 3. As was the case with the original model, the serial pathway through these two mediators was significant and the magnitude of this serial pathway did not differ substantially between the two models. The specific indirect effects through each of these two mediators were very similar to those observed in the original model. The primary difference in the two models involved the simple mediation model embedded within the full alternate model (i.e. self-compassion to health behaviors to perceived stress; see top part of Table 3). In the alternate model, nearly all of the total effect of self-compassion on perceived stress was direct, with only a small indirect effect through health behaviors. In contrast, in the original model, self-compassion had a substantial indirect effect on health behavior through perceived stress.

Conceptual diagram of alternate model linking self-compassion and physical health through health behaviors and perceived stress. Values presented are standardized path coefficients with bootstrap standard errors in parentheses.
Summary of serial mediation model linking self-compassion and physical health through health-promoting behavior and perceived stress.

CI: confidence interval; SE: standard error; SC: self-compassion; PS: perceived stress; HB: health-promoting behaviors; PH: physical health.
p < .001.
Discussion
This study tested a serial mediation model linking self-compassion with physical health via perceived stress and health behaviors. Consistent with previous research (e.g. Brion et al., 2014; Dunne et al., 2016; Sirois et al., 2015a), we found that self-compassionate people reported lower stress, more frequent health behaviors, and better overall physical health. Importantly, both lower stress and more frequent health behaviors explained the association with physical health individually, and the full pathway through stress and health behaviors was also significant.
Although our alternate model showed that health behavior did mediate the relationship between self-compassion and perceived stress, this indirect effect was small, suggesting that our original model was the more plausible of the two. Specifically, nearly all of the total effect of self-compassion on perceived stress was direct, with only a small indirect effect through health behaviors. In contrast, in the original model, there was a substantial mediating effect, with nearly half of the total effect of self-compassion on health behavior occurring through perceived stress. Because self-compassion has such a strong inverse relationship with perceived stress, we reasoned that this reduction in perceived stress was more likely to affect a person’s propensity for engaging in health-promoting behavior than vice versa.
Overall, our findings extend our understanding of self-compassion and physical health in several important ways. First, although previous research has shown that self-compassion is associated with lower levels of perceived stress, this study was the first to test perceived stress as a mediator of the relationship between self-compassion and physical health. Indeed, this pathway accounted for most of the total effect of self-compassion on health. Second, whereas previous research has noted that self-compassion is linked to physical symptoms via the practice of health behaviors (Dunne et al., 2016), this study replicated these findings using a comprehensive index of physical health that included symptoms, functioning, and a global rating of overall health. In addition, negative affective states have been shown to account for why self-compassionate people may be better able to regulate their health behaviors (Sirois, 2015; Sirois et al., 2015a). The current results extend these previous findings by demonstrating that lower stress, arguably a negative affective state, explains the association between self-compassion and health behaviors. Finally, our test of the full path model linking self-compassion to stress, health behaviors, and physical health provides the first test of the combined pathways from previous research on self-compassion and health (Dunne et al., 2016; Sirois, 2015; Sirois et al., 2015a), and indicates that self-compassion may relate to physical health through multiple routes.
The stress pathway accounted for most of the indirect and total effects of self-compassion on physical health, suggesting that it is the most salient route connecting self-compassion and health benefits. This result underscores the direct and immediate beneficial effects of self-compassion on the psychophysiological experience of stress (alpha-amylase activity, heart rate variability, and interleukin-6 response) found in other research (Arch et al., 2014; Breines et al., 2014, 2015). Although this physiological activation of the stress systems can be most damaging when prolonged (Cohen et al., 2012; McEwen, 2007), even short-term acute activation can take a toll on immediate health by suppressing immune functioning and creating vulnerability for infections, and other acute conditions (Taylor and Sirois, 2014). In contrast, health behaviors can be conceptualized as distal or indirect predictors of physical health, as the effects of poor health behaviors on health status tend to be cumulative over time (WHO, 2014). Although our results showed that the stress pathway accounted for most of self-compassion’s effect on health, it is important to note that self-compassion was linked with increased engagement in health behaviors both directly and indirectly (via reduced stress). It is likely that self-compassion and the reduction in perceived stress that accompanies it have small but cumulative effects on other processes that influence health, such as increased positive affect (Stellar et al., 2015) or satisfying social relationships (Holt-Lunstad et al., 2010). Future research is needed to test this idea.
Growing evidence indicates that self-compassion is malleable and can be enhanced through training (Jazaieri et al., 2013; Neff and Germer, 2013). For example, Neff and Germer (2013) developed an 8-week program aimed at increasing mindful self-compassion. While this program produced significant increases in self-compassion, there were concomitant decreases in perceived stress. In light of the well-documented health benefits of stress management (Taylor and Sirois, 2014), it is reasonable to think that this type of program would also have a positive impact on health. Our findings also suggest that self-compassion could play a role in interventions directly aimed at improving health behaviors. For example, several studies have now found that promoting self-compassionate responding to health behaviors failures can be effective for reducing health risk behaviors such as overeating (Adams and Leary, 2007), smoking (Kelly et al., 2010), and alcohol misuse (Brooks et al., 2012). It is possible that techniques designed to elevate self-compassion may be equally beneficial for increasing health-promoting behaviors, and subsequent physical health. Future research using experimental and longitudinal methods is needed to provide more rigorous tests of these ideas.
An important limitation of this study was its cross-sectional, correlational design. Given this design, it is not possible to confirm the proposed directionality of the relations among self-compassion, stress, health behaviors, and physical health. The models we tested implied that self-compassion exerted causal effects on both perceived stress and health behaviors; although this idea could not be confirmed in this study, it is consistent with experimental work that has demonstrated that increases in self-compassion can produce changes in perceived stress and health behaviors (Adams and Leary, 2007; Kelly et al., 2010; Neff and Germer, 2013). We tested an alternate model that placed health behavior as antecedent to perceived stress, but concluded that our original model was the more plausible of the two based on the strong relationship between self-compassion and perceived stress. Furthermore, our original model was informed by previous theory and research on self-compassion and health (Dunne et al., 2016; Sirois, 2015; Sirois et al., 2015a; Terry and Leary, 2011). Nevertheless, further prospective and experimental research is needed to assess the temporal precedence of our serial mediation model, particularly because recent evidence suggests that these relationships are dynamic and complex. Specifically, a longitudinal study examined how stress and health behaviors were related using ecological momentary assessment over a period of 12 months (Burg et al., 2017). The authors found that stress and exercise behaviors were inversely related but that this association was both unidirectional (stress to exercise) and bi-directional (stress to exercise to stress). Daily diary studies and similar ecologically valid methodological approaches are therefore needed to further clarify the nature of the pathways between self-compassion and health suggested by this study.
Conclusion
Although self-compassion has been firmly established as an asset for a wide range of desirable psychological outcomes (MacBeth and Gumley, 2012; Neff et al., 2007b), this study adds to the growing evidence that it also has benefits for physical health. These benefits appear to accrue primarily through the reduction in perceived stress that occurs when people respond to their personal failures, struggles, and difficult circumstances with a kind and forgiving attitude, and secondarily through increased engagement in health-promoting behaviors. Given the malleability of self-compassion, our results suggest that interventions cultivating self-compassion may be a fruitful direction for future research seeking to identify ways to reduce stress, increase health-promoting behaviors, and ultimately, improve health.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a JMM institutional grant at Grove City College.