
Abstract
This study investigates couples’ adjustment to rectal cancer and a colostomy using the ‘Classification System of Couple Adjustment to Cancer’, a framework delineating fluctuations in couples’ sense of ‘I’ and ‘We’ in response to cancer. Nine couples affected by rectal cancer and adjusting to life with a colostomy were interviewed. A theoretical thematic analysis of the transcripts was conducted; nearly all ‘I–We’ shifts of the Classification System of Couple Adjustment to Cancer were observed – often in unique ways in response to rectal cancer–specific challenges – and one new shift was described. The results provide a novel and experientially grounded means of conceptualizing complex dyadic coping processes.
Introduction
Colorectal cancer (CRC) is the third most diagnosed cancer in North America (American Cancer Society, 2014; Canadian Cancer Society, 2014). It is the second leading cause of death by cancer in men and the third leading cause of death by cancer in women. When malignant tumours are located in the lower portion of the rectum, patients may undergo an abdominoperineal resection (APR), a procedure in which a patient’s distal colon, rectum and anal sphincter complex are removed and the anus sewn closed (Perry and Connaughton, 2007). A colostomy is needed following such sphincter-sacrificing procedures (Sprangers et al., 1995). While medical advancements have reduced the number of patients requiring permanent ostomies as part of their treatment (Butler et al., 2013), it is estimated that approximately 15 per cent of patients diagnosed with CRC (usually rectal cancer (RC)) will need a permanent colostomy (Cancer Care Ontario, 2004). Given the invasive nature of the colostomy, it is not surprising that patients with CRC and permanent colostomies report poorer quality of life than patients with CRC living without permanent colostomies (Sprangers et al., 1995). Those with stomas may experience disruptions in bowel function (Burch, 2005; Nugent et al., 1999; Sprangers et al., 1995; Sun et al., 2013), changes to their diet (Nugent et al., 1999; Sprangers et al., 1995; Sun et al., 2013), lowered self-esteem and body image (Burch, 2005; Danielson et al., 2013; Persson and Hellstrom, 2002; Sprangers et al., 1995), feelings of loss of control and depression (Burch, 2005; Emslie et al., 2009; McVey et al., 2001), and diminishment in sexual functioning and decreased desire to engage in sexual activity (Burch, 2005; Cohen, 1991; Nugent et al., 1999; Salter, 1992; Sprangers et al., 1995; Sprunk and Alteneder, 2000) – changes with significant implications for intimate relationships.
Dyadic coping with CRC and a permanent colostomy
Despite identifying several significant challenges imposed by the colostomy, relatively little is known about how couples cope with CRC, and more specifically their adjustment to the colostomy. Well-partners may support patients by helping them seek medical care, taking an active role in the care of the colostomy, minimizing their ill-partners’ concerns or fears, concealing their own worry, prioritizing the needs of the patient, providing assurances of normalcy and continued attractiveness and taking on added household responsibilities (Altschuler et al., 2009; Dyk and Sutherland, 1956; Emslie et al., 2009; Northouse et al., 1999; Ohlsson-Nevo et al., 2011). In some cases, partners have expressed feeling unprepared for these new demands – some feeling limited in their social activities or forced into early retirement as a result (Ohlsson-Nevo et al., 2011). In turn, patients have expressed difficulty in surrendering former responsibilities or accepting personal caregiving from their partner (Dyk and Sutherland, 1956; Emslie et al., 2009). Moreover, while some couples are able to return to their pre-surgery sexual relationship, many describe having a different sexual relationship post-surgery (e.g. establishing new forms of intimacy/sexuality, new ways of relating to one another) with some failing to resume any sexual relationship (Dyk and Sutherland, 1956; Emslie et al., 2009; Ohlsson-Nevo et al., 2011).
‘We’-ness as a form of couple resilience
Research supports the notion that a couple’s sense of ‘We’-ness allows them to be resilient in the face of cancer-related challenges (Berg et al., 2008; Fergus, 2011; Kayser et al., 2007; Skerrett, 1998, 2003). Skerrett (2015) proposed that a sense of ‘We’-ness promotes resilience because it encourages partners to take responsibility for their reciprocal influence within the relationship, safely share vulnerabilities, co-construct meaning of their experience with adversity and develop strong relational skills over time. In taking a ‘We’-orientation, couples conceptualize the stressor as occurring to ‘us’ and as a common responsibility to be tackled by the couple, thus leading them to engage in dyadic or ‘communal coping’ (Lyons et al., 1998; Skerrett, 2015).
While the literature suggests that couple resilience in reference to cancer is strengthened through a fostering and awareness of ‘We’-ness, this may be an oversimplification of couples’ dynamic response and adjustment to illness. As adjustment to cancer is a variable process, it is conceivable that a couple’s sense of cohesion may be more accurately conceptualized as fluid, undergoing fluctuations between a sense of ‘We’ and ‘I’ as couples adapt to new challenges. In one analysis of the illness experience as conveyed by a sample of breast and prostate cancer patients and their spouses, couples’ fluctuations between a sense of ‘We’ and ‘I’ and vice versa were identified throughout the cancer journey (Fergus et al., 2012). These could be discrete instances or slowly evolving alterations in the couple’s sense of togetherness that reflect a change in the couple’s normative way of being. Such ‘I–We’ ‘shifts’ often have to do with the erection or dissolution of a personal boundary by one or both partners, in order to accommodate the challenges posed by the illness (e.g. shock and devastation of diagnosis, disabling treatment effects, challenges to personal care, existential fears). It was noted that such shifts, or instances in which one partner imposed a personal boundary resulting in a greater sense of ‘I’ or separateness in response to the cancer experience, were not necessarily damaging to the couple’s maintenance of ‘We’-ness and in fact could also be an indication of resiliency and a strong collective identity (Fergus et al., 2012). For instance, a patient who reacts to news of the prostate cancer diagnosis by withdrawing from others for a few days to process his situation is effectively inserting a boundary between himself and his partner. On the surface, this change in relational dynamic may appear distancing between patient and partner. However, in an otherwise high-functioning relationship where the well-partner is attuned to, and respecting of the patient’s emotional boundaries or need for personal space, the partner is likely to grant the patient the emotional and/or physical space he is needing (or indirectly ‘requesting’) through the erection of the boundary. The partner’s recognition of the patient’s individual needs – which may include a degree of ‘separateness’ from the other – within the context of the relationship bolsters the couple’s ‘We’-ness by virtue of the well-partner demonstrating understanding, acceptance and love for the patient, which in turn is stabilizing for the patient (i.e. provides a sense of security that is also regulating of his emotional distress) and thus strengthening of the patient’s identification with the relationship (Fergus, 2011).
These observations led to the development of the Classification System of Couple Adjustment to Cancer (CSCAC; Fergus et al., 2014), a paradigm or taxonomy delineating specific types of fluctuations in togetherness or ‘We’-ness, and separateness or ‘I’-ness. ‘I–We’ processes that strengthen the couple’s sense of ‘We’ are termed ‘We’-affirming processes and are generally characterized by a ‘coming together’ or dissolution of a boundary between partners (see Table 1). For example, the code, Doing Everything We Can, entails partners banding together to learn about the cancer and make treatment decisions as a team. In contrast, ‘I–We’ processes that weaken the couples’ sense of ‘We’ are termed ‘We’-eroding processes and are characterized by a distancing between partners, often due to a boundary being erected between self and other. For instance, the code, Dealing with It on My Own, captures the patient’s reactive assertion of autonomy to the point of shutting out the caregiving spouse. Finally, those ‘I–We’ processes that have the potential to either strengthen or weaken the ‘We’, depending on the relational context and the other partner’s individual reactions in response to the shift or boundary creation/dissolution, are termed ‘We’-differentiating processes. An example of a ‘We’-differentiating process is in the code, My Body, My Personal Space, in which the patient erects a boundary at the level of the body. In turn, the partner may feel shut out or rejected, ultimately leading the shift to be a ‘We’-eroding process, or alternatively, the partner may be respectful and accepting of the patient’s need for privacy/space, ultimately leading the shift to affirm the ‘We’. It is believed that couples may freely fluctuate between ‘We’-affirming, ‘We’-differentiating and ‘We’-eroding processes in response to cancer-related challenges and that such fluctuations are not unidirectional or sequential. The fluctuations between ‘I’ and ‘We’ are also classified more broadly according to the nature or theme of the challenge faced by the couple (i.e. existential fears, emotional burden of illness, physical or treatment concerns) (see Table 1).
‘I–We’ classification of couple coping and adjustment processes.

Originally labelled Feeling/Thinking the Unspeakable.
Newly identified ‘I–We’ process Code in current sample of rectal cancer (RC) patients and their partners.
This study
The aim of this study is to (a) validate the CSCAC using a sample of couples adjusting to RC and a permanent colostomy and (b) further refine the framework based on emerging data from the RC sample. RC patients were chosen – as a sub-group of the CRC patient population – to study given the paucity of research in the area of dyadic coping with permanent colostomies in relation to CRC in general and RC specifically. The literature that does exist often includes the single perspective of either the patient or the well-partner, tends to focus more on physical and practical adjustments and falls short of identifying patterns in couples’ psychological adjustment to the illness (e.g. Altschuler et al., 2009; Emslie et al., 2009; Ohlsson-Nevo et al., 2011). This study, in contrast, approaches the couple as a dyadic entity, seeking to understand couple coping dynamics with RC and a permanent colostomy as observed through the lens of the CSCAC.
Method
Procedures
Participant recruitment
This study was reviewed by the Sunnybrook Health Sciences Centre Research Ethics Board (#071-2013) and the York University Human Participants Review Sub-Committee (#2013-114), and written approval was granted prior to commencing recruitment. The sample was collected in collaboration with the Ostomy Advanced Practice Nurse at the host hospital. Eligible patient participants had received a diagnosis of RC, underwent an APR and had a permanent colostomy as a result of their treatment. Furthermore, in order to study dyadic adjustment from diagnosis to present, eligible patient participants were required to have begun their current relationship prior to their diagnosis and first course of active treatment. Recruitment was open to patients and partners aged 18–80 years inclusive, with the ability to read and speak English. Couples could be heterosexual or same-sex and did not need to be legally married. While efforts were made to balance recruitment by patient gender, the final sample consisted of seven male and two female patients and their partners.
Interview structure
The interviews were conducted with both patient and partner present. The interview was semi-structured, consisting of open-ended questions designed to elicit information about the couples’ experiences in adjusting to RC and the permanent colostomy. The semi-structured format encouraged participants to share their experiences to the degree that they felt comfortable while allowing the interviewer the freedom to pursue unanticipated avenues of interest relevant to the study objectives as they arose during the interview. Following the interview, both patients and partners completed a basic demographic form including treatment-related questions, as well as a relationship satisfaction questionnaire in order to individually gauge partners’ perceived quality of relationship. Gathering information about couples’ relationship satisfaction was undertaken in order to provide an additional index of the couples’ degree of functioning and adjustment.
Materials
Kansas Marital Satisfaction Survey
This three-item self-report measure was designed to quickly assess relationship satisfaction (Schumm et al., 1983). Respondents must rate their level of satisfaction with regard to their marriage/relationship, their relationship with their partner and their spouse as a partner, using a 7-point scale (1 = extremely dissatisfied, 7 = extremely satisfied). Individual scores can range from 3 to 21, where higher scores indicate greater relationship satisfaction (Crane et al., 2000). Couple scores of satisfaction can also be calculated by averaging each partner’s individual score. Crane et al. (2000) identified 17 as the cut-off score that distinguishes distressed from non-distressed couples. The scale has demonstrated high internal consistency (Schumm et al., 1983) and an adequate degree of concurrent validity with both the Dyadic Adjustment Scale and the Quality of Marriage Index (Schumm et al., 1986).
Methodology
Despite the fact that quantitative and qualitative methods of inquiry are grounded in different epistemological assumptions and attempt to answer different types of questions (i.e. why vs how, respectively), the value and rigour of their results are often compared to one another (Marecek, 2003). Quantitative analysis, based on positivism, is often regarded as objective, concrete and scientific. In contrast, qualitative inquiry is cast as subjective, ‘soft’ and unscientific. Most commonly, qualitative research is criticized for an inadequate ability to generalize and for scepticism over the validity or trustworthiness of data and the interpretations drawn from them (Lather, 1986; Marecek, 2003; Polit and Beck, 2010). The consensus among most qualitative researchers is that there is a need to implement safeguards for enhancing analytic integrity (Creswell and Miller, 2000; Lather, 1986; Marecek, 2003). In recognition of the importance of credibility (Glaser and Strauss, 1967) or validity in qualitative research, the focus of this study is to validate a new classification system for understanding couple adjustment to cancer based on partners’ ongoing negotiations of self-other boundaries in relation to the stressor (Fergus et al., 2014).
We employed different approaches to ascertaining the validity of the ‘I–We’ classification of couple adjustment to cancer. First, interview transcripts from this study were subjected to an analysis focused on gathering evidence that supported or disconfirmed the theory of adjustment; specifically, we reviewed the transcripts in order to identify which of the 32 types of ‘I–We’ process codes within the classification system as reported by Fergus et al. (2012) were observable in the RC sample. This approach is consistent with Stiles’ (1993) description of replication, in the sense that a previous interpretation was applied to new information. As is detailed in the analysis section below, our goal was to identify fluctuations that occurred in relation to ‘I’-ness versus ‘We’-ness over the course of couples’ adjustment to RC. Furthermore, we attempted to remain reflexive during the analysis (Creswell and Miller, 2000), acknowledging our predisposition for recognizing ‘I–We’ process codes due to our involvement in creating and refining the classification system. Therefore, beyond acknowledging our own biases, we also remained open to adapting the existing framework based on new information and/or observations from the current dataset, a process Stiles (1993) terms ‘reflexive validity’. When we found that an observed ‘I–We’ shift in the current investigation did not fit the existing ‘I–We’ process codes, we revised the classification system through the addition of a new ‘I–We’ code, a rearrangement of the existing ‘I–We’ process codes or the further refinement of the original ‘I–We’ process code definitions. Thus, the classification evolved in response to new observations. In order to ensure the integrity of the current analysis, ongoing consultation between members of the research team and maintenance of an audit trail (i.e. memoing) were undertaken throughout the study (Creswell and Miller, 2000; Lincoln and Guba, 1985; Stiles, 1993).
In a further effort to validate the classification system, a methodology based largely on a transactional approach to validity was developed and then employed during the second part of the interview. A transactional approach to validity involves an interaction between the data, the researcher and the participants with the goal of improving agreement and accuracy of interpretations (Cho and Trent, 2006). One form of transactional validity is known as ‘member checking’. This procedure involves taking the qualitative information and interpretations back to the participants to consult with them about their accuracy (Cho and Trent, 2006; Creswell and Miller, 2000; Lincoln and Guba, 1985). It is important to note that this study adapted the commonly used approach to member checking. Specifically, the conceptualization of adjustment as fluctuations and negotiations in ‘I–We’ boundaries originally developed based on an analysis of couples coping with breast and prostate cancer was presented to this study’s participants, couples adjusting to RC. The decision to conduct a member check with a new sample of RC patients and their partners rather than the original sample of couples adjusting to breast and prostate cancer was born out of the idea that this novel method of member checking held the potential to validate the ‘I–We’ conceptualization, while expanding and enriching the original ‘I–We’ process codes based on the unique challenges associated with couples coping with RC, and provide an opportunity to learn about an understudied oncology population.
It can also be argued that replicating the classification system with a different yet related sample – that is patients and partners adjusting to a third type of cancer – is a form of triangulation. Triangulation is an approach to validation conducted by gathering information from multiple sources (i.e. participants, theories, methods) and assessing their agreement (Cho and Trent, 2006; Creswell and Miller, 2000). Couples adjusting to RC as opposed to breast or prostate cancer represent an additional data source with which the classification system may be replicated. Inclusion of multiple data sources reduces the likelihood of misinterpretation and convergence between multiple data sources suggests stronger validity (Stiles, 1993). In other words, if couples adjusting to RC are able to consciously identify with the concept of there being ‘I–We’ fluctuations in relation to their own experience with cancer, or such shifts are implicit in their descriptions of their experience, such observations help to support the validity of the framework being investigated.
Analysis
The interviews were recorded and transcribed verbatim and NVivo software was used to organize data and assist with managing the analysis. The goal of the analysis was to identify fluctuations that occur between respective partners’ sense of ‘I’ and ‘We’, or vice versa, during their adjustment to RC and the permanent colostomy in reference to the existing CSCAC coding scheme. The analysis can therefore be described as a theoretical thematic analysis (Braun and Clark, 2006) as it was conducted with a theoretical lens focused on shifts between ‘I’ and ‘We’. In other words, the theoretical or deductive portion of the analysis entailed classifying the observed shifts using the existing ‘I–We’ process codes. However, as opposed to making strictly deductive inferences, the current analysis also employed inductive reasoning in order to avoid ‘forcing’ (Glaser, 1992) the data into the pre-existing classification system (i.e. the framework was modified based on new information from the current sample by adding or reorganizing the codes or ‘fine-tuning’ their definitions). In other words, the goal of the current analysis was not only to validate the ‘I–We’ framework in RC patients but also to refine the existing classification system in response to emerging data from the RC patients and their partners.
The analysis was a two-step process and a replication of the steps taken in the original study (Fergus et al., 2012). Transcripts were reviewed in order to identify portions of text for analysis. This was the first phase of the analysis and involved identifying passages of text from each transcript that were relevant to the study goals. A data extraction rule was developed based on whether the excerpt was considered ‘episodic’, ‘reflective’ or ‘linguistic’ in order to guide this process. Transcripts were then coded according to the relevant ‘I–We’ process code(s) (see Table 1) (Fergus et al., 2014). Where applicable, interview excerpts were assigned more than one code (in the end, no more than three categories were assigned for any given interview excerpt). When new information emerged from the interview content based on this sample, the original coding definitions were expanded or adapted accordingly.
Participants
The sample consisted of nine patients and their well-partners (N = 18) from the Greater Toronto Area. All were in heterosexual relationships. The average age of patient participants (n = 9) was 60 years (range: 42–80 years). Seven of the patients were male and two were female. Patient participants were diagnosed with RC, either primary (n = 6) or recurrent (n = 3), and on average were 57 years at time of diagnosis (range: 40–76 years). On average, patients were 33 months past their date of diagnosis at the time of the interview. All patients underwent neoadjuvant chemotherapy and radiation treatment followed by an APR and permanent colostomy. Six patients also received adjuvant chemotherapy as part of their treatment. The average length of the relationships was 30 years (range: 4–55 years). Except for one co-habiting couple, all other couples were married. The average age of participating partners (n = 9) was 57 years (range: 37–76 years). The majority of couples (nc = 5) 1 had children as a result of their current relationship. One patient had children from a former relationship. In most cases, the children were of adult age. Refer to Table 2 for additional patient medical information as well as ethnic, educational and employment demographics. The results from the Kansas Marital Satisfaction Survey revealed that both individual partners (M = 20.50, standard deviation (SD) = 1.15, range = 18–21) and couples (M = 20.50, SD = 1.06, range = 18–21) were satisfied in their relationship. As all the couple scores were above the cut-off score of 17, all couples were characterized as non-distressed (Crane et al., 2000).
Participant ethnic, educational, employment and medical information.

Results
To varying degrees, all couples described fluctuations between a sense of ‘I’ and ‘We’ in their adjustment to RC and the colostomy (see Table 3). All of the previously identified ‘We’-affirming and ‘We’-differentiating processes were identified in the current sample, while not all ‘We’-eroding processes were observed. Codes illustrating the ways in which ‘I–We’ shifts uniquely manifested within the RC patient population with their partners are presented below.
Frequency of endorsement of ‘I–We’ process codes in rectal cancer sample.
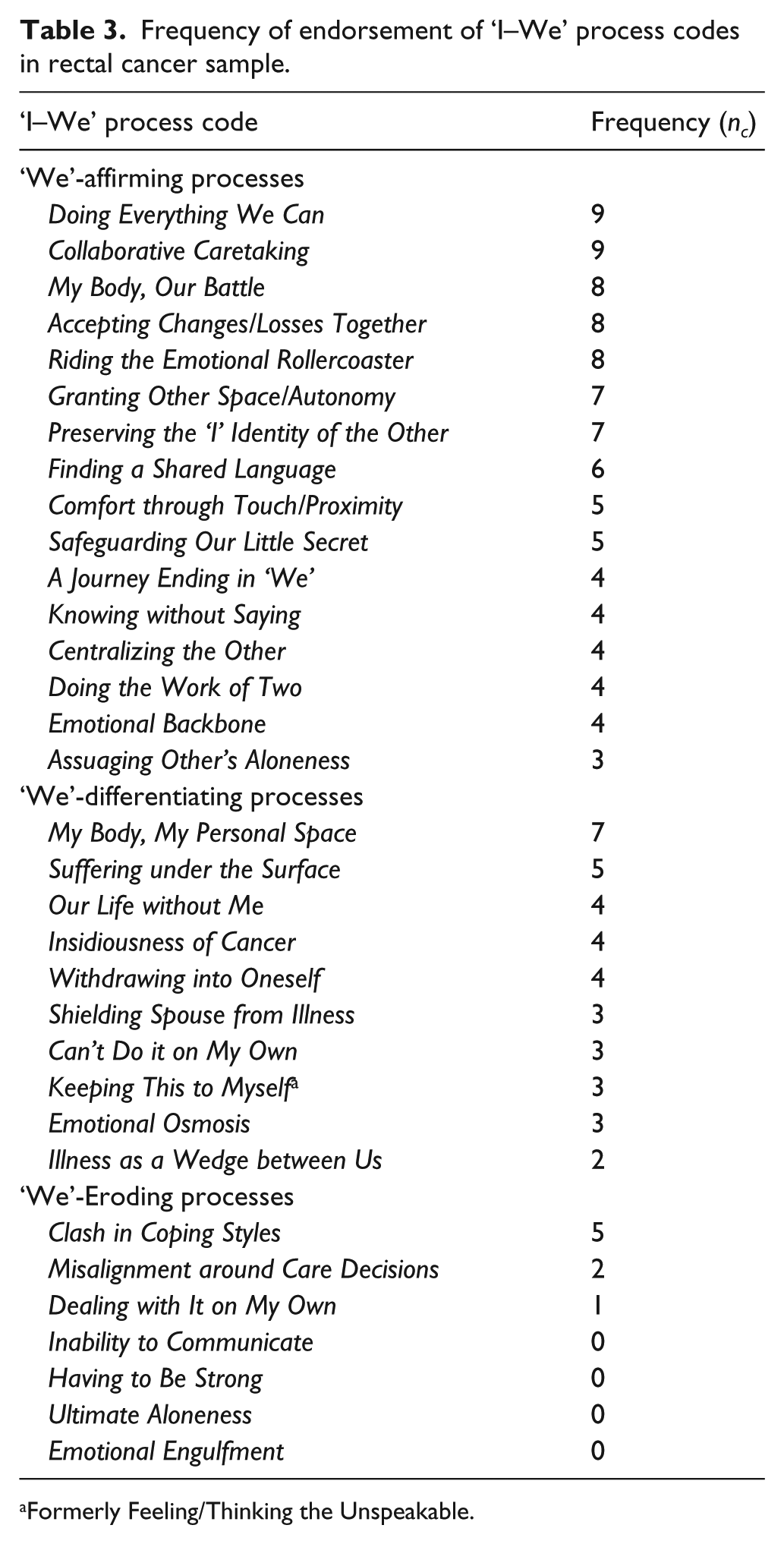
Formerly Feeling/Thinking the Unspeakable.
Participant reactions to ‘I–We’ conceptualization of adjustment
While ‘I–We’ process codes were identified in the discourse of all couples, participants had varying reactions when presented directly with the ‘I–We’ conceptualization of dyadic adjustment to cancer. Just under half of the couples (nc = 4) overtly agreed with the ‘I–We’ conceptualization of adjustment and were able to clearly identify shifts within their cancer experience that were consistent with the notion that a couple’s sense of togetherness and separateness fluctuates over the course of adjusting to cancer. One-third of the couples (nc = 3) had a more mixed reaction towards the presented conceptualization of adjustment to cancer. Specifically, these couples were initially less eager to describe their experience as fluctuating between ‘I–We’ because, while they often agreed that they became closer throughout the illness, they did not resonate with the notion of there being a boundary between themselves and the other, or requiring space from the other. However, following further discussion of the ‘I–We’ conceptualization of adjustment, they were able to offer examples of instances that were characterized by a movement towards ‘I’ and consistent with the ‘I–We’ process codes, although they did not consciously identify them as such. Moreover, it was noted by couples in both groups that a mutual respect for one another’s individual needs and privacy was practised prior to the cancer experience. In other words, this was not something ‘new’ for the couples.
Shifts explicitly identified by couples during this portion of the interview varied. A commonly reported shift for couples was a request for personal physical space or privacy around the colostomy and its related activities. Needs for emotional space following diagnosis, treatment or a particularly stressful cancer-related event were also expressed. Others described a feeling of coping separately as one male patient, Gerry, 2 described feeling ‘in the same space but not connected’ to his partner Julia. Some couples discussed absorbing the news of diagnosis, exploring treatment options and discussing existential fears together. One patient, Matthew, described individually pursuing alternative treatments, against the wishes of his spouse, as he was resistant to receiving the colostomy. Couples also recalled times when they found comfort through being near one another or touching, or times when they were so in tune with one another that they knew what the other was thinking without saying a word. The redistribution of the patient’s responsibilities, both practical and physical, to the partner was also a shift identified by several couples. While couples agreed with the conceptualization of their adjustment as a fluctuation between ‘I’ and ‘We’, they also stated that the experience solidified their sense of togetherness.
Two of the nine couples were more hesitant to describe their experience as consistent with the ‘I–We’ conceptualization of adjustment. These couples denied feeling a need for separateness during their experience. They characterized their experience as having a stable sense of ‘We’-ness or togetherness throughout the diagnosis and treatment trajectory including living with the ostomy. In these cases, proposing the ‘I–We’ conceptualization of adjustment led couples to reveal ‘We’-affirming processes, for example, their ways of communicating around the stoma or a new appreciation for their relationship.
‘We’-affirming processes
Doing everything we can (nc = 9)
This process represents partners’ uniting in their efforts to tackle the cancer by, for example, learning about RC and treatment avenues and jointly making treatment decisions. Essentially, couples are taking a ‘We’-orientation to the cancer and perceiving it as ‘our’ problem to solve, as illustrated by Julia’s recollection of hearing the news of Gerry’s RC diagnosis:
…in the doctor’s room [I] was to be some kind of a strength to him and then definitely when we got back to our cars after we’d been at the hospital almost all day – it was horrible day, obviously – and just hugging each other and knowing that we were together. He wasn’t going through this alone, I wasn’t going through this alone – we were together, we’re doing this together.
This united approach was specifically apparent in this sample in the ways that couples researched colostomy care and ostomy products together. Some couples expressed hearing the word ‘colostomy’ or ‘stoma’ for the first time as they were told that the patient would be receiving one as a permanent consequence of his or her treatment. Helen, partner to patient Richard, recalled the couple’s first experiences in learning about the colostomy and its supplies:
We got pamphlets … I went on the Internet …. But in the beginning it was not easy because you have so many things … to choose from that you go ‘oh my God’ and in the beginning you even order the wrong things. But now we know.
In some instances, partners took on the role of advocate or speaker for the patient in relation to treatment. For example, one patient, Daniel, recalled his wife, Margaret, advocating for him following a misunderstanding with medical staff:
Using her managerial skills Margaret told them, ‘Look it – you guys are supposed to let us know what’s happening so we can do [it]. We were supposed to be here at two o’clock to get the PICC line done’. Margaret gave them heck, told them that we weren’t leaving until the PICC line is in.
Collaborative caretaking (nc = 9)
This code entails couples collectively taking responsibility for tending to the patient’s often deeply private physical needs. As the colostomy imposed the most significant changes to the patients’ daily physical needs, in this sample Collaborative Caretaking was overwhelmingly related to partners’ assistance with colostomy care. Partners’ degree of involvement in caring for the colostomy varied from direct care of the colostomy (e.g. changing pouching system, assisting in irrigation), as Margaret shared, ‘Daniel has had his colostomy for what, how many years? Five years, honey? [turning to Daniel]. He did his first colostomy change by himself when he went with our son out west this summer’, to indirect care of the colostomy (e.g. purchasing colostomy supplies, monitoring foods that disrupt or help the functioning of the colostomy, checking in about characteristics of stoma output, cleaning soiled linens), as one patient, Cathleen, describes her experience with her husband, Samuel:
Oh my gosh, I mean there is output, there is no output …. And there is gas and there is no gas, and there is pain and there is no pain. And I had two [obstructions] and I was dying in pain, which I resolved both at home with his help.
Certainly, caring for the patient can also be burdensome for the well-partner who may experience a feeling of confinement themselves based on the need to be near to the patient in the event of physical care needs. Having been responsible for the majority of her ill-partner’s direct care needs, Sophia noted her renewed sense of freedom when her husband, Ali, became more physically independent:
… for five or six months, I can say like we don’t have to worry about being with each other all the time. Like he can take care of himself, except changing the flange, he knows whenever it’s time he will tell me … so that’s the good part, like you have the freedom and also the peace of mind that if he’s alone or going to the public washrooms or things where you cannot just go with him, then he can manage the things on his own.
My body, our battle (nc = 8)
This process entails couples taking collective ownership of the cancer itself. It is commonly characterized by partners expressing themselves in a way that conveys that both the patient and well-partner were undergoing and experiencing the illness at its various stages (i.e. diagnosis, chemotherapy, surgery) and is most often apparent in the couple’s use of ‘We’ language. While recalling her course of treatment, Cathleen remarked, ‘… and then we start doing chemotherapy for 4 months’; her use of ‘we’ versus ‘I’ in describing her cancer treatment implies that she was not going through the treatment alone, although only she received the chemotherapy medications. Additionally, both members of the couple often made reference to the ill-partner’s body and adjustment to the colostomy, as though it was the couple’s shared body. When describing the couple’s routine in caring for the stoma, patient Daniel recalled, ‘early on we had a rash, quite a severe one, we even took pictures of it’. In reality, the rash was restricted on a physical level to the skin of the patient; however, the language use points to the collective experiencing and sharing of the physical burden of the colostomy. Sophia poignantly captured this ‘I–We’ process of sharing the cancer experience as a caregiver when she stated, ‘It’s not only your suffering, it’s my suffering’.
Accepting changes and losses together (nc = 8)
Most often, this process referred to changes to sexual intimacy as a result of the patient’s compromised sexual function or body image due to the radiation, chemotherapy, surgery and/or the pouching system. Natalie struggled with having intercourse with her husband following her cancer treatments as she experienced pain during penetration. She described, ‘I’d be like, oh you know, “Oh here we go, we’ve got to do it now” … So now we’ve almost come back to the way we were before we were married [laughs]. We just rub’. In fact, when faced with these changes in their sexual relationship, many couples reported experimenting with alternative sexual activities like masturbation, oral sex, use of toys or changes in sexual position. Many couples also remarked that their sexual relationship was not the focal point of their relationship as a couple, as one partner described, ‘it’s just enough to be together … just clinch together and feel warm side by side. That experience is really the important thing in the relationship’.
Preserving the ‘I’ identity of the other (nc = 7)
This change relates to well-partners’ efforts to support the dignity of the patient and not draw attention to the losses, damages or disabilities imposed by the illness. This includes partners’ efforts to maintain normalcy; working towards minimizing change in the patients’ routines, abilities and sense of self; or reassuring patients about the acceptability of their physical appearance (e.g. attractiveness, pouching system not visible when dressed). Richard described how his partner did not perceive him as weak or incapable of maintaining healthy habits following his treatment:
She supports me in everything … for example one way she supports me is that she knows that I am lazy. I don’t do exercise. I like to eat and to drink. So she comes home every day from work and one of the first things she does is to force me to walk … I know that that’s good for me to keep in better shape.
In another example, Natalie purchased ostomy-specific apparel to cover her stoma while being intimate with her partner, Bernard. However, his reaction to her concealing the stoma helped instead to re-assure her of her physical attractiveness in his eyes. Together, they described this interaction:
I got on the Internet right away and I found this website called Ostomy Secrets. So it’s like Victoria Secrets … they also showed a ‘vixen belt’ that you could wear for when you’re having sex […] It was the prettiest little lace belt that I ordered right away. You know with visions that we, you know … [laughs]
So here’s the deal, here’s the deal. So the first time here’s the thing, it’s like ‘Ya, ya that’s cool’ whatever and all that. So then about like the [third] time and whatever. And then it’s like …
[imitating Bernard] ‘Don’t even wear it!’
Other partners helped patients maintain their dignity in public settings. One partner monitored when an odour could be detected and reminded the patient to change his pouch. Another partner acted as a trusted ‘second eye’ about the visibility of the colostomy pouch before the couple left the house.
Finding a shared language (nc = 6)
This shift entails the couples’ process of developing an idiosyncratic way of communicating about cancer and its related struggles. Many couples, for example, used humour as part of their regular interaction when facing the ‘lows’ of the cancer experience. For example, well-partner Bernard commented, ‘It would be the worst […] and I’d like say something silly like “Rectum/Wrecked ‘em? Darn near killed ‘em!” And then we’d laugh […] if you’re not laughing, you’re crying’. Unique ways of speaking about the cancer experience were also supportive of couples’ coping, as Samuel described the positive impact of Cathleen’s creative approach to framing and communicating about her radiation treatment:
She said ‘I think I’m talking with God … that He’s putting his special finger in that spot to kill the [cancer]’. And it was very, it was very remarkable how [she was able] to condense all of the difficulties she goes through, just isolated from the fact that really radiation is bad; just how you translated that into a positive thing … I mean that’s the kind of thinking she has.
Idiosyncratic language was also evident in how partners communicated about colostomy-related activities. Bernard described his dialogue with Natalie around her irrigation: ‘Well when we talk I say, “Are you doing your thing?” That’s what we call it’. Couples also commonly named the stoma or pouch. One partner stated, “We’ve named him Bob,” while another patient revealed, “Her name is Bertha … crazy Bertha’. Naming the stoma or pouch allowed couples to covertly discuss it in public free from fear of embarrassment.
Safeguarding our little secret (nc = 5)
This process involves couples establishing a parameter between themselves and the outside world; privately and without fear of judgment, partners can express their concerns, especially in relation to aspects of the cancer that are shameful or embarrassing for one or both partners. For example, couples discussed if, when and how to disclose the cancer diagnosis or the resultant permanent colostomy to people outside of the relationship. Couples ranged in this regard with some couples deciding not to disclose widely, while others agreed to speak freely. After travelling to a neighbouring city to meet with their physician and receiving news of the RC diagnosis, Margaret described why she and her ill-husband, Daniel, took a 2-day detour on their way back home:
… we hadn’t told our kids, we hadn’t told our friends, like we just kept it all to ourselves … we didn’t want to trouble them until we knew what was going on … I think it was a good place for us to collect our own thoughts and have our cries and get emotional and then face the music.
Disclosure about the colostomy specifically was helpful to some, as one partner explained:
If somebody is just visiting or if we’re visiting somebody, he will explain. Like we went for the adoption classes, we had four days there, so the first day he explained to people who were sitting around the table that this is the problem, I may pass gas, and this is the reason.
‘We’-differentiating processes
My Body, My Personal Space (nc = 7)
This process occurs when the ill-partner erects a boundary clearly distinguishing the ‘I’ from the ‘We’ at the level of the body. Explicit indications of such a change in the dyad pertained to the patients’ requesting privacy during irrigation or while managing the colostomy. As well-partner, Julia, remarked on a subtle but real change in restroom etiquette between her and husband Gerry:
So there’s that boundary now that when he’s doing that – the irrigation – I would never barge in. Whereas if he was, before, having a bowel movement on the toilet, I wouldn’t barge in necessarily but I wouldn’t feel so – it wouldn’t cross my mind that he’s embarrassed that I’m there.
Less direct demonstrations of this shift were observed when the patient hid or covered the stoma in the presence of the partner. One patient, Matthew, remarked, ‘to me it’s like my body was perfect before, like it was. Now it’s this thing is […] I’ll let her see me with the bag hanging off it but that’s about it, I won’t let her see my stoma’. Well-partners’ reactions to this separation varied; Matthew’s partner admitted to feeling comfortable with never having seen his stoma, while Julia felt shut out and isolated in response to her ill-partner covering his stoma. Julia described,
I think what bothers me is that he’s self-conscious around me about it and I wish he wasn’t …. We’ve been together, married, for 16 years and I’ve had two children and he’s witnessed that … that’s about as intimate as you can be and I – it doesn’t bother me at all.
Representations of My Body, My Personal Space also included reminders to the partner that the cancer was contained within the body of the patient. Cathleen described feeling frustrated and unheard by those around her, including her partner Samuel, when discussing her illness and medical concerns and, in response, asserted her role as patient:
… then [I] say, ‘Who is the patient? You or me? Who is suffering?’ [And they say], ‘No because I know how you feel’. No you don’t. Which is the thing that everybody goes, ‘No I know how you feel’. No you don’t. Did you have my cancer?
Keeping this to myself (nc = 3)
This boundary occurs when well-partners experience thoughts or feelings which are considered inappropriate or unacceptable and therefore elect not to share these with the ill-partner. For example, one partner admitted,
There are sometimes when I think, ‘Why does he have to have more surgery?’ I’m tired of having the surgery, he’s healthy why do we have to […] and that’s such a negative way of thinking so it may last a few minutes when I’m mad or something.
Within the current sample, this choice to keep one’s thoughts to oneself also occurred in relation to experiencing disgust towards the colostomy. Genevieve described her initial thoughts towards her partner’s colostomy:
… before the operation I’m really worried. You know it was like, oh my God, he’s going to have that thing … I at first didn’t even know what it is … and oh my God I was like the [shallow] part to think that he’s going have that thing hanging on him and […] poo will come out from it.
‘We’-eroding processes
Misalignment around care decisions (nc = 2)
Partners’ disagreement surrounding the appropriate course of treatment is at the core of this ‘I–We’ process. While this shift was expressed only in a minority of couples in the current sample, its occurrence points to the struggle some patients have in relation to accepting and pursuing RC treatment that will result in a permanent colostomy. For instance, Matthew experienced the thought of a colostomy as an affront to his sense of self- and personal identity as a healthy, vital man. He wanted to explore alternative methods of treatment, stating,
I wanted to experiment with it; I felt I still had time. Like when they were talking about – the doctors – about the cancers and it was explained to me [that] different cancers have different personalities and that I’d actually had this for a long time and it took a long time to get where it was and I felt that I had time to try different things.
Meanwhile, his partner, Genevieve, felt disappointed given the potential risks of delaying recommended treatment. She explained,
I don’t agree with him looking for like natural [treatments] … I feel like no, he’s wasting his time and this cancer is not going to wait. It’s gonna just, you know, spread because it’s already on the – we were told it’s stage two.
Eventually, a discussion with his son helped him to overcome his ‘vanity’ and opt for treatment including the colostomy. In another case, the patient had decided that he wanted to enjoy the remainder of his natural life without having to cope with invasive cancer treatment and the colostomy. Not until he recognized the toll this decision took on his wife, did he decide to pursue treatment.
New ‘We’-Differentiating Code
Illness as a wedge between us (nc = 2)
In addition to observing many of the original ‘I–We’ classifications, new information from the RC sample provided grounds for creating this new code, not previously captured in the sample of breast and prostate cancer patients. This shift speaks to a physical boundary erected between the couple as a result of cancer treatment, precluding them from sharing in the same experience. Specifically, Julia and Gerry were unable to enjoy swimming together on their vacation because of the colostomy as Gerry recounted,
We went on a vacation when the kids were at camp, we went away and it was like 40 degrees like this and sitting by the pool wearing a t-shirt like I [did] when I’m outside now and you’re swimming and I’m watching you swim. I wasn’t allowed.
In another case, Sophia and Ali could not share the same bed for fear of Ali being injured by Sophia. She explained,
It was difficult [laughs]. My habit was, like I could not, I was not able to sleep, unless I really get close to him, otherwise I wasn’t able to sleep. So that was the difficult part for me, to stay away from him, not to hurt him or not to kick him or do anything. I had the habit of kicking him or banging into him.
Such a forced separation due to the physical limitations of the illness/colostomy leads to a sense of loss and frustration as partners’ usual ways of being close and sharing activities are disrupted. This dynamic is ‘We’-differentiating in the sense that it has the potential to be eroding of the ‘We’, should the loss consume or further separate partners or, alternatively, unifying of partners, should they accept the loss together, perhaps by recognizing the potential for more dire consequences (i.e. death of patient).
Discussion
This study investigated the application of the CSCAC to couples adjusting to RC and permanent colostomies and the ‘We’-affirming, ‘We’-eroding and ‘We’-differentiating processes experienced by couples facing the unique challenges associated with the illness. In addition to generating support for the ‘I–We’ classification system and its analytic generalizability (Firestone, 1993) beyond the breast and prostate cancer populations upon which it was first developed, this analysis broadened knowledge about dyadic coping dynamics in relation to RC and its intrusive and complex treatment sequela. On a theoretical level, the investigation serves to further our current understanding of couple resilience, which has tended to focus almost exclusively on the importance of ‘We’-ness and the couple’s ability to approach the disease in a unified way (Berg et al., 2008; Fergus, 2011; Kayser et al., 2007; Skerrett, 1998, 2015). However, partners’ attunement and respect for one another’s individual needs and separateness speak to their shared understanding and connectedness as well. When couples discussed moments in which they provided one another autonomy or space, they conveyed an awareness of the other’s needs and differences. A recognition that partners may desire independence and autonomy during their adjustment does not undermine the ‘We’ but instead serves to honour both ‘I’s and enhance their individual as well as collective functioning. It is also important to note that findings from the current investigation suggest that even couples who report successful adjustment to cancer and high relationship satisfaction experience times of ‘We’-differentiation and ‘We’-erosion during their cancer experience. In other words, it appears that it is natural or even inevitable that partners will go through periods of isolation and/or distance over the course of their adjustment to cancer and that such occurrences do not spell doom for the couples’ ultimate ability to prevail.
One ‘We’-affirming process that was particularly striking within the RC sample was the My Body, Our Battle code and couples’ use of plural pronouns when discussing the physical consequences of the cancer treatment and the colostomy. This observation is consistent with Fergus’ (2011) conceptualization of adjustment to cancer as a shared, embodied experience between members of a couple. By the same token, the newly created ‘We’-differentiating code of Illness as a Wedge Between Us highlighted how the physical demands of the cancer treatment or colostomy also sometimes precluded couples from engaging in formerly shared activities, such as swimming together or sleeping in the same bed.
Another significant ‘We’-affirming process in this sample was captured by the category Finding a Shared Language in which patients and partners developed ways of communicating, often in code, about the colostomy. Couples used humour to minimize the stress associated with RC and managing the colostomy, developed unique terms or language around activities such as irrigation and, remarkably, even named the stoma and/or pouch, a finding that extends Sun et al.’s (2013) study of individuals affected by CRC to the realm of couples. Within the context of couple adaptation, naming the stoma or pouch, and developing a shared language around it accomplishes several functions conducive to successful dyadic coping. First, it permits partners to communicate covertly about a potentially embarrassing topic in public. Moreover, the use of stoma-related humour enables the couple to ease tension around the stoma and ensure that not all conversations about the stoma are heavy or shameful. It also objectifies the stressor thereby separating the couple from the illness’ intrusive effects and reducing the likelihood of the couple becoming defined by the illness (Fergus, 2015). Finally, as a reflection of the couple’s unique identity, this idiosyncratic form of communication is indirectly affirming of the ‘We’ and the relationship the partners share (Fergus and Reid, 2001).
Despite couples’ efforts to engage their collective resources in tackling the illness, one ‘We’-eroding process, Clash in Coping Styles, was discussed by many participants. This failure to cope in tandem occurred when partners’ individual coping efforts conflicted with or undermined the others’. In these cases, couples’ coping could be conceptualized as incongruent or oppositional (Revenson, 2003). According to Revenson (2003), successfully coping with illness is believed to involve partners using similar coping strategies by which neither impede the other, or complementary coping strategies in which each partner’s coping efforts ‘fit’ with and strengthen the coping effort of the other. Reid and Ahmad (2015) describe couples’ coping as a ‘We’ as an emergent phenomenon of the partners’ individual coping systems. When couples undergo challenges together, they strengthen their mutual understanding, empathy and interpersonal processing, allowing them to cope better as a dyad, which, in turn, enhances their ‘We’-ness or identification with the relationship. Fergus and Skerrett (2015) compare this strengthening of couples’ ‘We’ to the strengthening of a muscle; both are able to grow and become more resilient because of adaptation and accommodation in response to adversity or rupture. Just as with a muscle, the more the couple is able to ‘exercise’ this practice, the greater their resources of ‘We’-ness grow and develop for use in response to future adversities. As evidenced by the current sample, couples may react to adversity through ‘We’-eroding, ‘We’-differentiating and ‘We’-affirming processes, and they may freely fluctuate between these processes over the course of their adjustment to cancer in response to the various challenges that arise. However, if their sense of ‘We’-ness is strengthened when couples draw upon it to overcome adversity, it would follow that the more often couples engage in ‘We’-affirming processes (and/or react to ‘We’-differentiating processes such that they evolve into ‘We’-affirming processes), the more likely it will be that the couples will once again engage in the ‘We’-affirming processes when faced with future challenges.
Limitations
While all of the ‘I–We’ process codes categorized as ‘We’-affirming and ‘We’-differentiating were identified in the current RC and colostomy sample, not all of the ‘We’-eroding processes were identified. Given the partners’ high ratings of relationship satisfaction, it is presumed that the current sample of couples was high functioning, which may have aided in their adjustment. In other words, it is possible that these couples had a strong sense of ‘We’-ness prior to their cancer experience which enabled them to resist engaging in ‘We’-eroding processes. Future investigations into the current ‘I–We’ classification system may benefit from interviewing couples with lower levels of relationship satisfaction in order to better explore and understand ‘We’-eroding processes.
Additionally, it is possible that the study design influenced the couples’ discussion towards disproportionately reporting experiences of ‘We’-affirming processes rather than ‘We’-eroding process. Specifically, the method focused on dyadic interviews and did not include separate individual interviews with either patient or partner. This approach was chosen in hopes of eliciting the dyadic processes within the context of the interview and encouraging discussion and perspective sharing by each partner on their common experiences. However, it is possible that conducting the interviews with both partners present deterred some participants from sharing certain relevant information, for example, rehashing experiences of conflict or sharing thoughts or feelings that could potentially upset or hurt their partner. This dynamic may have been particularly limiting in relation to the ‘We’-differentiating process, Keeping This to Myself, in that the very nature of the process would have prohibited its disclosure in the dyadic interview and may help to explain why few partners disclosed such an experience in this study.
The sample in the current investigation consisted primarily of male patients and their female partners because recruitment of female patient dyads proved difficult and generally unsuccessful. Investigations into gender differences in adjustment to CRC suggest that female patients with male partners tend to report lower relationship satisfaction, more distress and poorer adjustment than male patients (Baider et al., 1989; Goldzweig et al., 2009). Given these findings, it is possible that these couples declined to participate due to a tenuous adjustment to the illness and/or colostomy. It is also plausible that if more female patient–male caregiver dyads were included in the sample, more ‘We’-eroding processes would have been observed. Additionally, the inclusion of more female patients and their partners may have provided further gender-specific information pertaining to couple adjustment to CRC and a permanent colostomy. In addition to the gender bias, the current sample also heavily comprised individuals who identified as White/Caucasian. As a result, the investigation may lack the representation of important ethnic, cultural or religious challenges and/or ways of coping in relation to the RC and a colostomy.
Implications
The results provide couples and clinicians with a novel and experientially grounded means of conceptualizing complex dyadic coping processes. Moreover, a nuanced understanding of the fluctuations in couples’ cohesive identities that occur in response to cancer in general and RC in particular has the potential to inform psychoeducational interventions for couples by providing couples with a language with which to comprehend their adjustment process. In conceptualizing couple coping as an ebb and flow between couples’ sense of ‘I’ and ‘We’, clinicians can normalize patients’ and partners’ needs for separateness or experiences of disconnection and instill hope that these fluctuations are not only common but also hold the potential to ultimately affirm their mutual identity. These findings also provide insight into the specific concerns and challenges faced by couples adjusting to RC and colostomies, better equipping clinicians to anticipate and address these issues with their patients and spousal caregivers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Sunnybrook Health Sciences Centre Practice Based Research Award.