
Abstract
Cultural groups often participate in traditions and activities surrounding food and eating, which contribute to group differences in maladaptive eating-related patterns and outcomes. This study explored the relationships between cultural attitudes and eating behaviors of young adult African American men and women. Endorsing a strong orientation on various dimensions of African American culture were related to less dieting, bulimic, and anorexic behaviors and attitudes. This study extended our knowledge of the ways in which cultural attitudes were related to the physical and mental health of African Americans and recognized the significance of individual differences within this group.
Culture is a fundamental guide to all facets of a person’s life; it is symbolic, historic, and dynamic (Jones, 2003). Kroeber and Kluckhohn’s (1952) definition of culture includes learned behaviors and ideas that are based on tradition and their attached values which are socially transmitted from one generation to the next. Culture is entwined in a person’s daily actions and is consequently a key factor in the meaning of food and eating. This study will examine the relationship between cultural orientation and eating behaviors of African American men and women.
African American cultural attitudes
Jones (2003) posits that African American culture has a unique worldview that reflects the attitudes, cognitions, values, and behaviors of African American experiences in five dimensions: time, rhythm, improvisation, orality, and spirituality (TRIOS). TRIOS, as a theory, is a way to understand the psychological and cultural resources that helped Africans in America to survive and be resilient to racial oppression and dehumanization (Jones, 2003, 2004).
These coping mechanisms became cultural patterns, which in turn were passed onto the next generation of African Americans. Jones (2003) has developed a scale operationalizing the TRIOS dimensions, and African Americans score significantly higher than, or as high as, any other ethnic group on all five TRIOS dimensions in a test of validity. High levels of TRIOS are associated with greater psychological well-being in the African American population (Jones, 2003). This broad and comprehensive theory of cultural orientation for African Americans aids in our understanding of African American eating behaviors.
The current research
There are several limitations in the extant literature on the relationship between culture and eating among African Americans. One limitation is that the majority of studies on this topic have failed to examine how specific elements of African American culture may be associated with eating behaviors (Harris and Kuba, 1997; Lovejoy, 2001; Parker et al., 1995; Rich and Thomas, 2008). The second limitation is that research on African American culture and eating behaviors is still lacking a comprehensive measure of cultural orientation (Henrickson et al., 2010). While it is important to understand the relationship between eating behaviors and other proxy measures such as racial and ethnic identity, these measures may discount the richness of culture (Harris and Kuba, 1997). The final limitation is that previous research on this topic has been mainly comparative in nature. Comparative research fails to recognize and explain individual personality differences within African Americans.
This study addresses these limitations in the existing literature by investigating whether cultural orientation is related to eating behaviors for African American men and women. We are defining eating behaviors as dieting, bulimic behaviors, and oral control (exercising control of over eating or anorexia). This study will focus on the concepts of time, rhythm, improvisation, orality, and spirituality from the TRIOS measure.
Hypotheses
First, we expect time orientation to be related to dieting (hypothesis 1). According to TRIOS, time relates to one’s own personal perspective on the past and future. For past orientation, time has no independent value; time is not the driver, or the determiner. On the other hand, future orientation attributes great significance to the concept of time. Past orientation is more reflective of traditional African cultural systems which value connecting with ancestors and history (Jones, 2003). In contrast, future orientation is more prevalent in Western culture. In Western culture, a future orientation is coupled with individualistic and goal-oriented attitudes (Kelley and Worthley, 1981). Previous research has found that African Americans are more past-oriented and that European Americans are more future-oriented; these differences in temporal orientation have been related to health outcomes and health management (Brown and Segal, 1996).
In future orientation, behaviors, including eating, are more regimented. In past orientation, behaviors, including eating, are more organic and less tied to prescribed, external sources (Mbiti, 1990). Dieting is related to a focus on the future; if a person struggles in the moment they will be rewarded in the future with a thin body. Past orientation may be related to enjoying the eating experience with less concern for future consequences, such as weight gain. Present orientation may also view food as a means of connecting with African or African American culture and history, and those who endorse this view of time may derive more enjoyment and purpose from food. We predict that a strong past temporal orientation will predict less dieting behaviors as these behaviors are related to the future consequences of food and eating.
Second, we expect improvisation orientation to be related to bulimia (hypothesis 2). Improvisation is one’s ability to creatively solve problems and adapt to overcome barriers. Improvisation also reflects personal expression and style. African American culture fosters an improvisational orientation, which has been hypothesized to be related to attitudes about appearance and the body for women (Lovejoy, 2001). Improvisation is linked to a greater appreciation of creative style rather than a fixation on rigid standards of physical appearance (Lovejoy, 2001). Racial differences in standards of appearance and the body have been hypothesized to be related to African Americans having more fluid and flexible notions regarding standards of beauty and also less emphasis on external appearance (Lovejoy, 2001). Less restrictive standards of appearance are related to less eating behaviors (Hewitt et al., 1995). Therefore, we expect greater improvisation orientation to be related to less bulimia.
Third, we expect people who score high on improvisation to show less restrictive eating (oral control) (hypothesis 3). In addition to being able to meet the challenges of everyday life, improvisation includes optimism about the future (Jones, 2003). We hypothesize that people who feel capable of overcoming the obstacles that life throws at them will be less afraid of the possible negative consequences of eating and therefore less likely to show restrictive eating patterns.
Fourth, we do not expect a significant gender differences in eating disorder symptomatology nor cultural orientation. Recent studies examining the relationship between men and maladaptive eating behaviors suggests that while the gender imbalance still exists, the differences in eating disorder diagnoses between men and women may not be as great as previous literature has reported (Anderson and Bulik, 2004). Further research suggests that this gender difference is even smaller in the African American community (Croll et al., 2002). Gender differences in African American culture have not been empirically measured. We have no reason to hypothesize a specific difference for African American men and women.
Method
Participants
These data were collected as part of a study examining African American college students’ daily experiences. In Total, 439 self-identified African American second- and third-year undergraduate students were recruited from three universities in the United States (112 men and 327 women). Participants’ ages ranged from 19 to 22 years (M = 19.8 years, standard deviation (SD) = .95 years). The students were recruited from three universities: a large public university in the Midwest that is predominantly European American (n = 159); a large public university in the Southeast that is also predominantly European American (n = 151); and a medium-size private university on the East Coast that is historically African American (n = 129). The mean income of the participant’s parents ranged between US$55,000 and US$64,999, while individual incomes ranged from less than US$4999 to over US$105,000.
Procedure
Two procedures were employed to recruit participants for this study. The office of the registrar at the two predominantly European American universities provided contact information for all students who self-identified as African American on their admissions applications. We used this information to recruit students via email and telephone solicitations. At the historically African American university, researchers relied on campus-wide outreach methods including fliers, word of mouth advertising, and classroom announcements. At all three institutions, researchers asked potential participants screening questions to ensure that they self-identified as African American and were at least 18 years of age. If students answered affirmative to those questions, they were asked to participate in a study examining African American student’s daily experiences pertaining to race. The students then scheduled a time to come to a laboratory space to complete a web-based survey within 2 weeks of initial contact. Participants completed instruments assessing racial identity, psychological well-being, racial experiences, cultural orientation, and demographics. Participants were paid US$15.
Measures
Eating behaviors
Eating patterns were assessed using the Eating Attitudes Test–26 (EAT-26), a 26-item measure assess eating disorder symptomatology (Garner et al., 1982). This scale has been used in nonclinical samples as a continuous variable, due to the low base rate of clinical eating behaviors found in the general population (Mazzeo, 1999; Sabik and Tylka, 2006). Therefore, we used the EAT-26 as a continuous measure ranging from 1 (never) to 6 (always). This scale contains three subscales: dieting (13 items; α = .90), bulimic tendencies (6 items; α = .71), and oral control (7 items; α = .65) (Garner et al., 1982). The dieting subscale evaluated perceptions of body image, nutritional attitudes, and eating habits. A sample item is “I am preoccupied with the desire to be thinner.” The bulimia subscale assesses binging and purging behaviors. A sample item is “I have gone on eating binges where I felt that I may not be able to stop.” The oral control subscale evaluates a person’s attempts to exercise control over the circumstances of eating and is similar to anorexia nervosa symptomatology. A sample item is “I avoid eating when I am, hungry.” A higher score on any of the three subscales means a greater endorsement of those attitudes or behaviors. Participants’ scale scores were calculated by averaging across the items to which the participant responded, which allowed for the use of the response anchors to interpret the scale scores.
Cultural orientation
For this study, we used Jones’s TRIOS scale, a 28-item measure of dimensions of African American cultural identity. The five dimensions of African American culture give TRIOS its name: time, rhythm, improvisation, orality, and spirituality (Jones, 2003). Participants use a scale ranging from −3 (very untrue) to 3 (very true) to rate the extent to which they agreed with each item. The time subscale (six items; α = .70) measures the strength of personal present–past orientation (as opposed to future orientation), as this has been a historical tenet in African cultural systems (Jones, 2003). A sample item is “Preparing for what might happened in the future is often a waste of time.” The rhythm subscale (five items; α = .71) measures the strength of the internal responses to the rhythmic patterns found in the external world (Jones, 2003). A sample item is “I have a flow to my life that connects me with my environment.” The improvisation subscale (seven items; α = .79) examines the extent to which a person uses goal-directed creative problem solving as a means of control and structure in interactions with others (Jones, 2003). A sample item is “When a situation arises, I usually know 2 to 3 different ways to handle it.” The orality subscale (three items; α = .80) measures the preferences for oral face-to-face communication and personal expression and endorses the meaningful role of spoken words in human affairs. A sample item is “In my social group, laughter often holds us together.” The spirituality subscale (seven items; α = .92) accesses the degree to which a person believes in the value of a higher power and unknown forces that influence all living things and one’s life in particular (Jones, 2003). A sample item is “In most aspects of my life, I am strengthened by my spiritual beliefs.” For each subscale, higher scores corresponded with a greater strength in the endorsement of that cultural ideology. Participants’ scale scores were calculated by averaging across the items to which the participant responded, thus allowing for the use of the response anchors to interpret the scale scores.
Body mass index
Participants self-reported their height and weight which were converted into a body mass index (BMI: weight in kg/height in m2) score. A BMI of 25 is the threshold for the overweight category according for the Center for Disease Control, while 30 is the threshold for obesity (Flegal et al., 1998). However, it should be noted that there is some controversy about the classification of weight status using BMI for African Americans (Deurenberg and Deurenberg-Yap, 2001).
Results
The means and SDs for all measures are presented in Table 1. Overall, participants showed a past-time orientation (a negative TRIOS-TIME score), strong spiritual beliefs (a high TRIOS-SPIRIT score), a preference for humor and storytelling (a high TRIOS-ORAL score), an ability to adapt to challenging situations (a high TRIOS-IMPROV score), and an appreciation of the role of music and rhythm in shaping everyday living (a high TRIOS-RHYTHM score).
Correlations between variables used in the regression analyses.

Significant correlations at *p < .05 and **p < .01.
The eating disorder scores from the EAT-26 (Table 1) were significantly lower than those reported by majority European American women samples (Mazzeo, 1999; Sabik and Tylka, 2006; Tylka and Sabik, 2010). These eating disorder scores were also slightly lower than a sample of all African American women (Akan and Grilo, 1994). The BMI of participants ranged from 16.46 to 51.68. The mean BMI was 25.17 (SD = 5.31), indicating that the average participant was classified as overweight.
The correlations (presented in Table 1) indicate that cultural orientation (TRIOS) was negatively correlated with disordered eating behaviors and attitudes. The exception was time orientation, which was negatively related to dieting, but unrelated to bulimia and oral control. These results indicate that stronger African American cultural orientations are associated with less eating disordered behaviors and attitudes of dieting, bulimia, and oral control.
Cultural identity as a predictor of eating behaviors
Hypothesis 1 was supported with additional results. Multiple regression was used to determine the impact of TRIOS-RHYTHM, TRIOS-IMPROV, TRIOS-ORAL, TRIOS-SPIRIT, and TRIOS-TIME on EAT-DIETING. Screening of the data demonstrated linearity, the absence of multicollinearity, a lack of univariate and multivariate outliers, and homoscedasticity of residuals. Regression results indicate a model of two predictors (TRIOS-TIME and TRIOS-IMPROV) that significantly predicts EAT-DIETING, R2 = .115,
EAT-DIETING as a function of TRIOS.
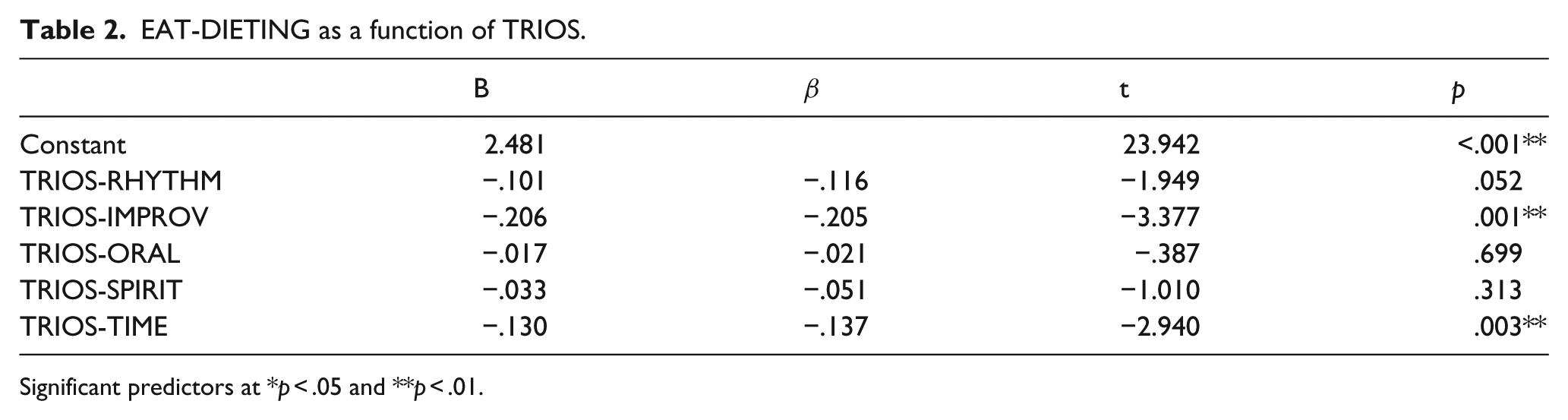
Significant predictors at *p < .05 and **p < .01.
Hypothesis 2 was supported with additional results. Multiple regression was used to determine the impact of TRIOS-RHYTHM, TRIOS-IMPROV, TRIOS-ORAL, TRIOS-SPIRIT, and TRIOS-TIME on EAT-BULIMIA. Screening of the data demonstrated linearity, the absence of multicollinearity, a lack of univariate and multivariate outliers, and homoscedasticity of residuals. Regression results indicate a model of two predictors (TRIOS-IMROV and TRIOS-SPIRIT) that significantly predict EAT-BULIMIA, R2 = .146,
EAT-BULIMIA as a function of TRIOS.
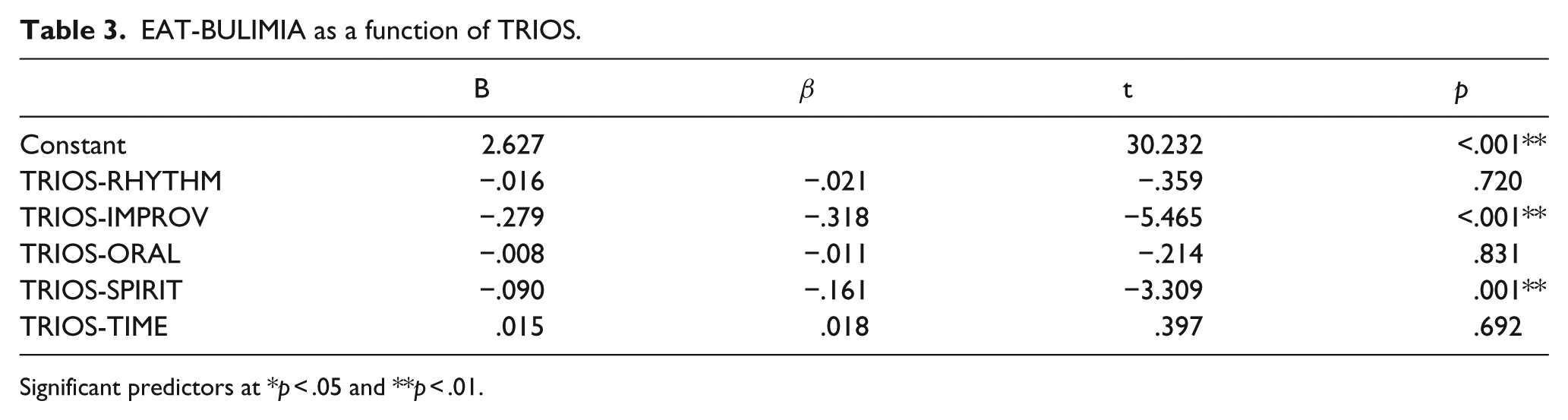
Significant predictors at *p < .05 and **p < .01.
Hypothesis 3 was supported. Multiple regression was used to determine the impact of TRIOS-RHYTHM, TRIOS-IMPROV, TRIOS-ORAL, TRIOS-SPIRIT, and TRIOS-TIME on EAT-ORAL CONTROL. Screening of the data demonstrated linearity, the absence of multicollinearity, a lack of univariate and multivariate outliers, and homoscedasticity of residuals. Regression results indicate a model of one predictor (TRIOS-IMPROV) that significantly predicts EAT-ORAL CONTROL, R2 = .050,
EAT-ORAL CONTROL as a function of TRIOS.

Significant predictors at *p < .05 and **p < .01.
Hypothesis 4 was partially supported. As predicted, mean gender differences in study variables were examined in the analysis presented in Table 5. There were no gender differences in any of the disordered eating variables. However, contrary to our hypothesis, there were gender differences with regard to time, spirituality, and improvisation. Men were more likely to be of a present orientation, women were more likely to be spiritually oriented, and men were more likely to display improvisation.
Gender differences across key measures.

Significant predictors at *p < .05.
Discussion
Time orientation was related to dieting for African American men and women. The greater endorsement of future orientation (as opposed to past orientation) was related to more dieting. In a future orientation, food may be viewed as a means to an end. For instance, if a person aims to maintain or achieve a culturally desired thin body size, eating may be viewed as a means to achieve that goal. This relationship supports the notion that if a person uses discipline and self-control through restriction of food, there will be benefits or a pay-off in the future when they obtain their desired body.
High levels of improvisation orientation were related to less bulimic behaviors. This may suggest that the use of creative problem solving in the face of stress may be a key factor in this relationship. A person with high improvisation orientation might face an emotionally taxing situation with better resources instead of turning the stress inwards, using eating as a means of coping. Binge eating demonstrates a loss of control where purging demonstrates a maladaptive coping method to regain control. Improvisation also endorses personal expressiveness or style. Perhaps African Americans endorse more fluid notions of beauty, which means standards are not rigid or fixed by restrictive standards of body size/shape rather style, attitude, and other characteristics can make someone attractive or beautiful as well (Parker et al., 1995).
As hypothesized, we found that improvisation is related to lower levels of maladaptive food control (oral control). Using food to regulate mood is a maladaptive coping mechanism that can contribute to the development of maladaptive eating behaviors (Sims et al., 2008). Perceived stress is commonly linked to binge eating episodes which can lead to increased obesity and long-term health risks (Ng and Jeffery, 2003). However, stress can also contribute to a desire to restrict eating. Ruggiero et al. (2008) have shown that high levels of stress are linked to an increased drive for thinness and more body dissatisfaction. High levels of improvisation are linked to more active coping mechanisms and less reliance on manipulating food intake when dealing with stressful situations. African Americans who show higher levels of improvisation are more optimistic and engage in more effective problem solving. These individuals feel a sense of control no matter what is going wrong with their lives and this may allow them to maintain healthier eating patterns.
A strong spiritual orientation was related to less bulimic behaviors, a relationship that was not originally hypothesized. Richards et al. (2007) have previously shown that attending to a patient’s spiritual growth may significantly reduce eating disorder symptoms when used as part of a comprehensive treatment plan. Jacobs-Pilipski et al. (2005) found that college women who rated spirituality as important were significantly more likely to use their spiritual beliefs and practices (i.e. praying, meditating, reading spiritual/religious texts) as a way to cope with distress related to eating. This study suggests that the use of spiritual beliefs and practices as coping mechanisms for distress related to eating could help prevent the development of maladaptive eating behaviors for both men and women. Greater belief in a higher power may also be related to respecting and accepting the body in its natural form and thus less likely to abuse one’s body by binging, purging, or pills.
Spirituality can be expressed in many ways including through organized religion. In Christianity, one’s body is conceptualized as the temple of the Holy Spirit (Parker et al., 1995). The body has greater significance than its outward appearance; instead, it is a vehicle to do God’s will. Therefore, harming one’s body through starvation, binging, and purging, or eating excessively could be perceived as contrary to God’s will. In the African American community, the church is a safe haven and a source of social support. It is also a place where a person can find comfort and display their own sense of style and these expressions will be appreciated by others (Parker et al., 1995).
Previous research on eating behaviors and spirituality has focused on how spirituality can be used in the treatment of disordered eating behaviors (Emmett, 2007). Spirituality has been shown to have a positive effect on African Americans’ physical health and psychological well-being (Blaine and Crocker, 1995; Bowen-Reid and Harrell, 2002; Bowen-Reid and Smalls, 2004). This study builds on this body of literature for African American populations.
This study found no gender difference in dieting, bulimia, and oral control. This is consistent with previous research which suggests gender differences of eating patterns are not as large in the African American community compared to the European American community (Croll et al., 2002). These results were contrary to a previous study (Taylor et al., 2007), which found that African American women suffer from disordered eating behaviors at a higher rate than men.
Contrary to our hypotheses, there were gender differences in three dimensions of cultural orientation. Men were more past-oriented in our study although previous research has been mixed about gender differences in time orientation (Harber et al., 2003; Padawer et al., 2007). Women were more spiritually oriented; this finding is expected since women are often viewed as the bearers of culture within a family. Spirituality is more central to African American culture (Jones, 2003) and spirituality may hold a special meaning for African American women as the church is often an institution to transmit culture (Lincoln and Mamiya, 1990). In addition, the African American church is often a place of female leadership and predominant female membership. Finally, men showed higher levels of improvisation. This may be due to the higher levels of collective coping shown in African American men (Lewis-Coles and Constantine, 2006).
Implications of findings
This study highlighted the importance of culture, not gender in eating behaviors. This is contrary to previous research which suggests the gender is a strong predictor of maladaptive eating patterns in the majority of European American samples (Lewinsohn et al., 2002). Our results also reveal the possible role of effective problem solving and coping skills in relation to eating behaviors (Lobera et al., 2009). Both improvisation and spirituality have components of these skills, which may be the driving force in their relationship to eating behaviors.
African American culture is related to less maladaptive eating behaviors, but not necessarily related to healthy eating. Results of this study suggest that African American culture may reject the thin ideal but may be linked to higher levels of obesity. Conventional weight-loss methods are often regimented in nature and may be related to cultural orientation. Promotion of intuitive eating, which is more aligned with African American cultural orientation may be more effective in achieving effective and long lasting weight loss.
Limitations
This study was limited to a college-aged population and thus might not be representative of the majority of African Americans. In addition, there may also be a cohort effect depending on cultural attitudes and orientation. Also, this study could potentially determine the basis for a causal relationship between cultural orientation and eating behaviors. However, future longitudinal research would be needed to establish the exact nature of this relationship. Finally, other factors related to eating behaviors, such as physical activity levels, were not included in this study.
Conclusion
This study highlights the significance of cultural attitudes in-group comparisons and clarifies previous research which suggests African Americans are uniformly protected against maladaptive eating behaviors. Instead, the study demonstrated that spirituality, improvisation, and time orientations are specific aspects of African American culture which are significantly related to less eating disordered behaviors. Identifying these aspects of culture in African Americans can be used to plan more efficacious treatments as well as aiding in the prevention of maladaptive eating behaviors.
Footnotes
Declaration of conflicting interest
The authors declare that they have no competing interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.