
Abstract
Health is regulated by homeostasis, a property of all living things. Homeostasis maintains equilibrium at set-points using feedback loops for optimum functioning of the organism. Imbalances in homeostasis causing overweight and obesity are evident in more than 1 billion people. In a new theory, homeostatic obesity imbalance is attributed to a hypothesized ‘Circle of Discontent’, a system of feedback loops linking weight gain, body dissatisfaction, negative affect and over-consumption. The Circle of Discontent theory is consistent with an extensive evidence base. A four-armed strategy to halt the obesity epidemic consists of (1) putting a stop to victim-blaming, stigma and discrimination; (2) devalorizing the thin-ideal; (3) reducing consumption of energy-dense, low-nutrient foods and drinks; and (4) improving access to plant-based diets. If fully implemented, interventions designed to restore homeostasis have the potential to halt the obesity epidemic.
Since the time of Hippocrates, the dictum of a good diet, exercise, and a proper night’s sleep has been a prescription for a healthy life. Prevention has been a popular idea ever since. The first president of the American Public Health Association stated in 1874, ‘… the customs of society must be so changed that the physician is employed to prevent rather than cure disease’ (Smith, 1874). Many recent editorials have addressed obesity, dieting, weight control and related issues (e.g. Drewnowski, 2014; Edmonds and Templeton, 2013; Fitzgerald, 2014; Gold and Graham, 2011; Ndisang et al., 2014; Pagadala and McCullough, 2012; Potenza, 2014; Sniehotta et al., 2014; Stuckler and Basu, 2013; The PLoS Medicine Editors, 2012; Yanovski, 2011). The obesity epidemic rolls on, unabated.
According to Dobbs et al. (2014), obesity is responsible for around 5 per cent of global deaths, and the global economic impact is US$2.0t, or 2.8 per cent of global gross domestic product (GDP), roughly equivalent to the impact from smoking or armed violence, war and terrorism. In the United States, in 2004, direct and indirect health costs associated with obesity were US$147 billion in 2008 U.S. dollars (Centers for Disease Control and Prevention (CDC), 2013). That figure could be doubled by now. Depending on the source, it is reported that the direct medical cost of overweight and obesity combined has been estimated to be 5–10 per cent of the US health-care spending (Tsai et al., 2010). Forty-two million children under the age of 5 years were overweight or obese in 2013. Prevalence of overweight or obesity in adults doubled from 6 per cent in 1980 to 12 per cent in 2008 (Stevens et al., 2012). By 2050, it is predicted that obesity will affect 60 per cent of adult men, 50 per cent of adult women and 25 per cent of children, making the United States, Britain and much of Europe a mainly obese society.
The main driver of the obesity epidemic and other non-communicable diseases is unregulated marketing of unhealthy foods and beverages. Stuckler et al. (2012) observed that the sales of unhealthy commodities across 80 low- and middle-income countries are strongly interrelated. Moodie et al. (2013) argued that the alcohol and ultra-processed food and drink industries are using similar strategies to the tobacco industry to undermine effective public health policies and programmes.
In this article, I describe a homeostatic theory of health and illness. Following this general theory of health and homeostasis, I describe a psychological theory of obesity, the evidence that supports it and examples of strategies for halting the epidemic. It is proposed that all conditions of health and illness, including overweight and obesity, are regulated by homeostasis.
Complexity of the issue
The world is full of contradictions, inconsistencies and inequities (Marks, 2015). On the one hand, the Food and Agriculture Organization (FAO) of the United Nations (2014) reported that 805 million people are chronically undernourished. Yet, the volume of food produced is more than 1½ times what is needed to provide everybody on the planet with a nutritious diet (Weis, 2007). It is not about lack, it is about inequity. While 805 million starve, 1460 million are overweight or obese, and that number is increasing.
The production and distribution of food and beverages has changed profoundly with globalization of unhealthy commodities – ‘McDonaldsisation’ and ‘Cola-nisation’. This trend is aided and abetted with commodification of animals in factory farms all over the world. Animals in factory farms live in cruel and harsh conditions that are regarded as efficient and profitable, and as long as consumers are given their fill of cheap beef, mutton, chicken, pork and salmon, there will be no halting of industrial farming of animals. Indeed, the industry is expanding (Foer, 2009).
In Western populations, the vast majority of people are meat eaters. It is estimated that around 95 per cent of the Western population eat meat. On average, in the United States, a meat eater consumes around 200 animals/part-animals a year or 16,000 over a lifetime (Mohr, 2012). To provide all of this livestock, the agri- and aquacultural systems degrade land and water, biodiversity and climate both directly through pasture and indirectly through its use of feed and forage, and the methane expelled by cattle (Foley, 2011). Ruminants use 86 per cent of the world’s agricultural land and consume 71 per cent of its total biomass, yet produce only 8 per cent of its food (Smith et al., 2013).
Strong evidence and warnings and advice by experts in nutrition and epidemiology go largely unheeded. The dead hand of governance gathers and reports statistics, but does little to abate the epidemic while giving every possible assistance to Big Food, Big Meat and Big Dairy (The PLoS Medicine Editors, 2012). This negligence is in spite of five interesting facts which can be summarized as follows:
‘Red meat consumption is associated with an increased risk of total, cardiovascular disease (CVD), and cancer mortality’ (Pan et al., 2012: 555).
High consumption of red meat is associated with higher circulating levels of gamma-glutamyl transferase (GGT; a biomarker of metabolic syndrome and obesity) and high-sensitivity C-reactive protein (hs-CRP; a biomarker of inflammation and CVD) (Montonen et al., 2013).
The intake of high-fat dairy products is associated with an increased risk of CVD mortality (Van Aerde et al., 2013).
‘Substitution of other healthy protein sources for red meat is associated with a lower mortality risk’ (Pan et al., 2012: 555).
High consumption of whole-grain bread is related to lower levels of GGT, hs-CRP and alanine aminotransferase (ALT; a biomarker of liver disease) (Montonen et al., 2013).
Big Food, Big Meat and Big Dairy pose major health threats with increased prevalence of obesity, diabetes, metabolic syndrome, CVDs and cancers everywhere (The PLoS Medicine Editors, 2012). An important clue as to causation of obesity is the fact that economically worse-off people are worst hit by unhealthy foods, while the well off can afford better food and are less prone to so-called disorders of ‘civilization’. Drewnowski and others have demonstrated a strong relationship between affordability of food and beverages and their energy density measured in terms of fat and sugar (Drewnowski and Specter, 2004). Energy-dense diets are associated with lower daily food consumption costs and provide an effective way to save money (Drewnowski and Darmon, 2005). On this basis, it is a reasonable assumption that ‘Good taste, high convenience, and the low cost of energy-dense foods, in conjunction with large portions and low satiating power, may be the principal reasons for overeating and weight gain’ (Drewnowski and Darmon, 2005: 900).
A systematic review of 27 studies across 10 countries showed that a healthful diet costs US$550 per year more than an unhealthy one (Rao et al., 2013). In England, another study suggested that the healthiest dietary pattern costs double the price of the least healthy, costing £6.63/day and £3.29/day, respectively (Morris et al., 2014). The inverse relationship between income and obesity prevalence is shown Figure 1.

Prevalence of obesity in adults (aged 16 years and over) by household income quintile, Health Survey for England, 2008–2012.
The obesity gradient shows that the rising incidence of overweight and obesity is not just a health issue, it is about social justice, because the least well off suffer significantly higher rates of obesity. In 2008, an estimated 1.46 billion adults worldwide had a body mass index (BMI) of 25 kg/m2 or greater and, of these, 205 million men and 297 million women were obese (Finucane et al., 2011). Taking into account the rate of increase in obesity, this half-billion figure is projected to increase by at least 30 per cent by 2050. The World Health Organization (WHO) estimates that around 3.4 million adults die each year as a result of overweight or obesity (WHO, 2014).
The WHO (2013) plans to halt the rise in diabetes and obesity with a vision to create ‘A world free of the avoidable burden of non-communicable diseases’. WHO interventions revolve around ‘mobilizing sustained resources … in coordination with the relevant organizations and ministries’, which consist of high-level meetings between governmental representatives and publishing position statements. Yet, leading authorities have concluded that
Obesity is the result of people responding normally to the obesogenic environments they find themselves in. Support for individuals to counteract obesogenic environments will continue to be important, but the priority should be for policies to reverse the obesogenic nature of these environments. (Swinburn et al., 2011: 804)
It has been observed that Big Food does not much care about consumer health (The PLoS Medicine Editors, 2012), and the lack of effective interventions suggests that, by and large, civil government has been impotent to stem the tide of health detriments created by the food and beverage industry.
The obesity epidemic is of comparable importance to the smoking epidemic. Arguably, it will prove to be even more significant in the history of human suffering than smoking. It took 50 years of consolidated pressure to reduce the prevalence of smoking-related diseases. There is enough scientific knowledge now to tackle the obesity epidemic. The fact that systems of governance are market-led with health policies compromised by the interests of multinational industries means that food policy and regulation are not based on scientific evidence but on economic imperatives. There can be little doubt that if the food chain could be rationally developed, the obesity epidemic could be solved within a decade from now.
In applying a biopsychosocial approach, it is recognized that a complex array of genetic, nutritional, developmental and environmental factors influences the development of overweight and obesity. None seems to ‘tell the whole story’. Obesity is a clear case of multiple causation. Classic twin study methods suggest that human body size is under substantial genetic control (Stunkard et al., 1986). It can be estimated that approximately 50 per cent of the variance in obesity risk is explained by environmental factors and 50 per cent by genetic factors (Bouchard, 1996). It remains necessary to explain how or why overweight or obesity can develop in a susceptible individual, and why some individuals develop it and not others.
The potential for complexity has never been more vividly displayed than in the Foresight Report (2007) that referred to a ‘complex web of societal and biological factors that have, in recent decades, exposed our inherent human vulnerability to weight gain’. The report presented an obesity map with energy balance at its centre and with over 100 variables directly or indirectly influencing energy balance. The Foresight committee recommended change at many levels – personal, family, environmental and national. The complexity of working with 100 or more variables is daunting, and to a degree, paralyzing, as there are so many different avenues and choice points that there is confusion about where exactly one should intervene for change.
To be useful in the real world, a scientific theory of obesity causation containing a relatively small number of explanatory variables is necessary. Sharpening the focus on such a theory will enable systematic interventions to change health outcomes on a mass scale. Two fundamental questions are as follows (1) Is the construction of such a theory feasible? (2) Which variables would be the operative ones? In this paper, I suggest the answer to question 1 is “Yes”. Review of the extensive health psychology literature from five decades of intensive investigation suggests three primary candidates in causation of overweight and obesity: (1) negative public perceptions of large body size and the resulting high levels of dissatisfaction among people with increasingly large body size; (2) the high levels of negative affect in the form of anxiety, depression and stress consequential upon increasing body size; and (3) the emotional consumption of fatty and/or sugary foods and beverages including alcohol. These three processes have been extensively investigated over several decades and the research evidence to be reviewed suggests strong links between them. The evidence suggests that these three processes form a feedback system which I term ‘The Circle of Discontent’ (COD), a circle that arguably goes some distance towards explaining the rising incidence of overweight and obesity. These three processes are well known within the field of obesity research and their interrelationships having been widely researched in thousands of studies. However, the intimate relationship that exists between them in the form of interconnecting, reciprocal feedback loops and their homeostatic significance have not been previously described in definitive form. The evidence to be presented suggests that the theory rests on a bedrock of well-established principles and is buttressed by solid evidence. The theory yields testable predictions and provides the foundations for strategies for preventing the further growth of the obesity epidemic.
The objectives of this theoretical review are therefore (1) to define and describe the concept of psychological homeostasis, (2) to propose a general Theory of Health based on the construct of psychological homeostasis, (3) to specify within the general theory the Circle of Discontent Theory (CODT) of overweight and obesity, (4) to summarize the body of evidence that is supportive of the general theory and the CODT, and (v) to describe interventions for preventing overweight and obesity based on the theory.
Health and homeostasis
Homeostatic regulation is a singular unifying principle in all health protection and illness prevention. Health is regulated by homeostasis, one of the distinguishing features of all living things; it preserves life when in balance; it removes life when imbalanced; when not present at all, a system cannot be living (Mamontov, 2006). Homeostasis operates at all levels of living systems: in cells, tissues, organs, organisms, societies and, some have argued, in biodiversity and the planet as a whole (the Gaia hypothesis; Lovelock, 2009). Tissue homeostasis regulates the birth (mitosis) and death of cells (apoptosis); many diseases are directly attributable to defective homeostasis leading to over production or under production of new cells relative to cell deletion (Fadeel and Orrenius, 2005). Biochemical and physiological feedback loops regulate billions of cells and thousands of compounds and reactions in the human body to maintain body temperature, metabolism, blood pH, fluid levels, blood glucose and insulin concentrations inside the body (Matthews et al., 1985). A body in good physical health is in biochemical and physiological homeostasis. Severe disruptions of homeostasis cause illnesses which can prove fatal.
Homeostasis is the in-built tendency of a living organism to maintain stable equilibrium among its internal components while interacting with the external environment. Homeorhesis is the tendency of living organisms to evolve along a trajectory while environmental conditions are continuously changing (Mamontov, 2007). Homeorhesis brings stability, order and normalcy in an evolving trajectory with internal and external disturbances. Homeorhesis is a necessary feature of any living system. If a system does not perform homeorhesis, it is nonliving (Mamontov, 2006). At any particular moment of time, homeorhesis reduces to homeostasis. In this article, I use the term ‘homeostasis’ as it is much better known. 1
Hippocrates viewed health as a harmonious balance of elements, and illness as a systematic disharmony of these elements. Galen (CE 129 – 200), the early Roman physician, followed the Hippocratic tradition with hygieia (health) or euexia (soundness) as a balance between four bodily humors, black bile, yellow bile, phlegm and blood. Galen believed that the body’s ‘constitution’, ‘temperament’ or ‘state’ could be put out of equilibrium by excessive heat, cold, dryness or wetness. Such imbalances could be caused by fatigue, insomnia, distress, anxiety or by food residues resulting from eating the wrong quantity or quality of food. These early ideas about balance and harmony were the foundation of biochemistry, physiology, psychology and medicine in the 19th and 20th centuries.
In the 1850s, Claude Bernard (1974) described the milieu intérieur (the environment within) as follows:
The fixity of the milieu supposes a perfection of the organism such that the external variations are at each instant compensated for and equilibrated … All of the vital mechanisms, however varied they may be, have always one goal, to maintain the uniformity of the conditions of life in the internal environment … The stability of the internal environment is the condition for the free and independent life.
Following Bernard, Walter Bradford Cannon (1929) described physiological homeostasis and, in so doing, acknowledged the views of Hippocrates and Bernard. He cited Pflüger (1877: cited in Cannon, 1932) who stated, ‘The cause of every need of a living being is also the cause of the satisfaction of the need’, and Fredericq (1885: cited in Cannon, 1932) who suggested,
The living being is an agency of such sort that each disturbing influence induces by itself the calling forth of compensatory activity to neutralize or repair the disturbance. The higher in the scale of living things, the more numerous, the more perfect and the more complicated do these regulatory agencies become. They tend to free the organism completely from the unfavourable influences and changes occurring in the environment.
Cannon (1932) defined the term ‘homeostasis’ as follows (see Figure 2):
The coordinated physiological processes which maintain most of the steady states in the organism are so complex and so peculiar to living beings – involving, as they may, the brain and nerves, the heart, lungs, kidneys and spleen, all working cooperatively – that I have suggested a special designation for these states, homeostasis. The word does not imply something set and immobile, a stagnation. It means a condition – a condition which may vary, but which is relatively constant.

Physiological homeostasis.
A person in good health is in a state of homeostasis of four principal kinds, biochemical, physiological, psychological and social. Outward and inward stability in a life form is only possible by constant adaptation. All living beings strive to maintain a state of equilibrium and stability with other beings and the surrounding environment through millions of micro-adjustments and adaptations to the continuously changing circumstances. Adjustments and adaptations can be both conscious and unconscious. The majority of fine adjustments are occurring at an unconscious level, hidden from both external observers and the individual actor.
Physiological homeostasis restores the balance in any physiological system that has evidenced an imbalance. There are literally thousands of homeostatic mechanisms operating at a physiological level. One of the most important examples is sleep, restoration from fatigue. In illness, the balance is disturbed and not properly restored. However, with treatment, there is rehabilitation and recovery.
Psychological homeostasis is a system of regulation and control of immense sophistication and complexity geared to maintain psychological equilibrium and stability as a person interacts with, and is affected by, the external world. In similar fashion to its physiological counterpart, it regulates through central control action, thought, motivation, emotion and action. Continuous activity of feedback loops strives to maintain psychological equilibrium from moment to moment. Psychological homeostasis occurs in response to the infinite variety of circumstances that can affect well-being, including both internal adjustments (e.g. emotional regulation) and external adjustments using behavioural regulation (e.g. communicating, working, eating and drinking). Psychological homeostasis operates throughout waking life, whether consciously or not. For most people, most of the time, homeostasis is maintained by thousands of largely invisible micro-adjustments and accommodations to the social and physical surroundings. These micro-adjustments are controlled centrally by cortical and neurological systems to regulate action, reaction and emotion and responses in light of motivational states such as hunger, thirst, fatigue, cravings and sexual impulses.
Social homeostasis serves an essential regulatory function in social action. The author of As You Like It referred to the world as a stage and men and women as merely players. Everyday idioms refer to not ‘upsetting the apple cart’, ‘rocking the boat’, ‘making waves’, ‘causing trouble’ and ‘disturbing the balance’ and so forth. These sayings make explicit reference to social homeostasis in which ‘self-control’ must be employed to maintain social stability.
In social psychology, self-observation and self-control, guided by situational cues to social appropriateness of expressive behaviour and self-presentation, have been referred to as ‘self-monitoring’ (Snyder, 1974, 1987). The social environment can only be kept in equilibrium by an infinitude of fine adjustments and accommodations to enable sociable interaction, conversation, sharing and intimate behaviour, in dyads, families, friendship, groups, teams and organizations towards common aims and purposes. Conflict and confrontation are successfully avoided by accommodations and compromises that are required for coexistence. Circumstances arise, however, when competing demands and pressures cause tensions and conflict. Conflict also may be created internally when a person has contrary emotions or desires or it may be external when two or more people seek different means or ends. In conflictual scenarios, the smooth operation of central control can breakdown momentarily, for example, in situations of high strain/stress, negative moods, loss of temper or inappropriate responses to sexual impulses. In the majority of cases, the individual returns to a set-point of equilibrium, a point of stability of function, perhaps with compensatory actions such as apologies, excuses, compromises, agreements, resolutions, contracts, rules, policies and regulations. If self-regulation fails, then institutional means of social control can be deployed (the police force and judiciary). The social milieu is, in effect, a platform upon which each individual actor plays out his or her roles.
In prevention and treatment of clinical conditions, the individual will be advised to monitor and maintain physiological variables using behavioural forms of homeostasis, for example, in cases of diabetes, metabolic syndrome, hypertension, thyroid problems, skin disorders, such as urticaria, or obesity. Examples of biochemical homeostasis are shown in Supplementary File, Figure 1. Biochemical, physiological and psychological homeostasis are of similar complexity. Behavioural forms of homeostasis occur in actions designed to support neural systems of regulation. Social homeostasis in supportive actions by other humans or animals, whether requested or simply volunteered, is another way in which the well-being is protected. Other forms of homeostatic control technologies include (1) electro-mechanical homeostasis, developed by engineers to enhance human control systems such as heating (thermostat), driving (cruise control), navigation (automatic pilot) and space exploration (computer navigation systems); (2) life support systems (e.g. artificial respirators, drip feeding, kidney dialysis, intensive care units); (3) medical interventions and surgery; (4) pharmaceutics; (5) alternative and complementary therapies; and (6) social, political and economic control. 2
Homeostasis of all kinds are mutually supportive and synergistic in nature. Only rarely and aberrantly would different kinds of homeostasis work in opposite directions. Examples of different levels of homeostasis in single scenario are shown in Table 1.
Different levels of homeostatis to a cooling temperature in a reference situation.
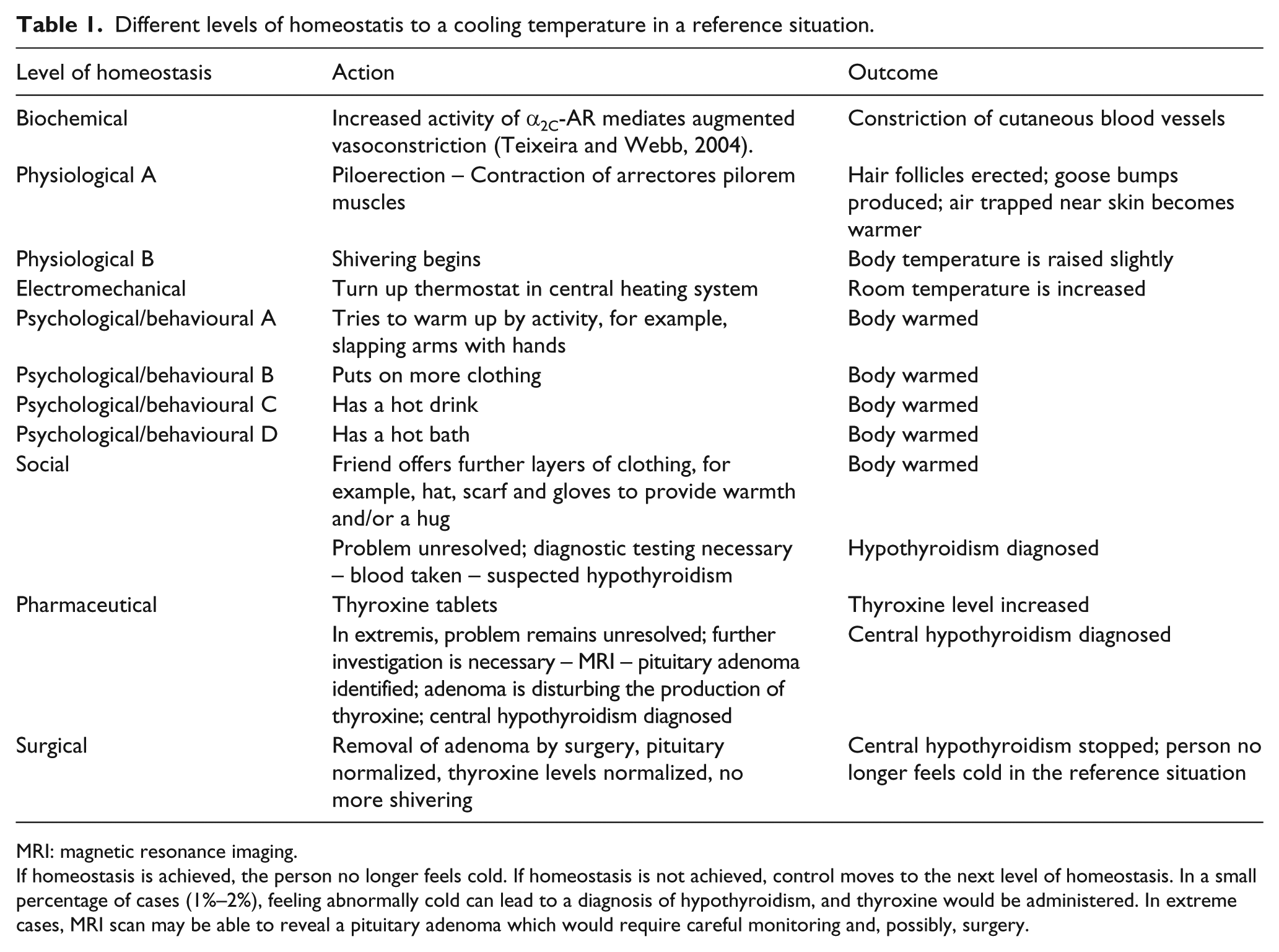
MRI: magnetic resonance imaging.
If homeostasis is achieved, the person no longer feels cold. If homeostasis is not achieved, control moves to the next level of homeostasis. In a small percentage of cases (1%–2%), feeling abnormally cold can lead to a diagnosis of hypothyroidism, and thyroxine would be administered. In extreme cases, MRI scan may be able to reveal a pituitary adenoma which would require careful monitoring and, possibly, surgery.
The different forms of homeostatic control complement and synergize one another. If one form of regulation fails, another form will be activated. Behavioural control is routinely used to rebalance physiological homeostasis. In diabetic control, an individual learns to monitor and maintain blood glucose levels as close to normal as possible, around 70–130 mg/dL before a meal and below 180 mg/dL 1–2 hours after a meal (American Diabetes Association, 2014). If a diabetic person is to avoid serious complications, then maintaining diabetic control is critical for long-term health. To maintain control, the individual must check his or her blood glucose levels several times daily and a physician should conduct the A1c test 2 to 4 times a year to assess average blood glucose control over the previous 2–3 months by measuring the level of glycated haemoglobin (HbA1c) in the blood stream. Individuals will be advised by their physicians to make modifications to routines of daily living, especially their diets, working habits and sleeping patterns to reduce depression, fatigue and stress. Other examples of self-monitoring include anticoagulant management with warfarin and blood-pressure self-management. Behavioural self-monitoring of food and drink consumption (Boutelle and Kirschenbaum, 1998), regular self-weighing to evaluate weight loss (Burke et al., 2011), the counting of cigarettes consumed in smoking control (McFall, 1970) and self-monitoring of physical activity with pedometers (Bravata et al., 2007) are all behavioural techniques for restoring homeostasis. Behavioural homeostasis works best when guided with a planned series of goals that can help to regulate action (Locke and Latham, 2002). Goal setting is an ideal strategy in stroke rehabilitation (Rosewilliam et al., 2011), cardiac rehabilitation (Moore and Kramer, 1996) and physical therapy (Baker et al., 2001). In rehabilitation, better outcomes and higher patient satisfaction are achieved when the patient can set his or her own goals.
In psychological homeostasis, the level of well-being at which the person feels comfortable is a well-balanced arrangement of living or working conditions, with no particular irksome feelings, and without the necessity to regulate consumption of food and drink. In this state, the individual eats and drinks freely without restraint. However, in illness, a person feels something is wrong, a dissatisfaction with his or her condition, and they feel ‘in a bad mood’, sad, lonely, anxious or stressed. One response to such disequilibrium is to eat and drink carefully and to take other restorative or conservative steps such as resting or ‘taking things quietly’ for a while’ in order to return to well-being. In many cases, such disequilibrium is episodic and short-lived (Figure 3).

Psychological homeostasis.
In this analysis of well-being, key significance is attached to the concept of ‘consumption’, a category that includes, in its broadest sense, not only food, beverages, medicines and substances but material goods, housing, vehicles, clothing, shoes, fashion accessories, cosmetics, hobbies, computers, mobile phones, tablets, devices, gadgets, sports, golf club membership, holidays, cruises, skiing, gambling, pornography, entertainment, leisure activities and other forms of ‘conspicuous consumption’, including generation of waste and an individual’s carbon footprint. An individual’s resources, especially his or her disposable income, the assets in their possession that can be disposed of in any way they choose and the ability to show restraint, to resist or restrict consumption by design, are the key driver and brake on consumption. Gaining energy through eating and drinking and using it through activity and mobility provide a feedback loop with the power to stabilize or destabilize well-being. In the majority of cases, overweight and obesity are the consequence of one of both of two processes: (1) a high set-point for adiposity based on genetic predisposition which resists intervention but can be altered by a lifestyle that has high levels of activity (Li et al., 2010b), or (2) gradual disruption of homeostasis caused by an imbalance in consumption of food and drink relative to energy output in physical activity.
Attachment
In conceptualizing health as an outcome of homeostasis, it is necessary to consider an individual across the lifespan (Figure 4). A lifespan perspective enhances understanding of life transitions such as the onset of overweight and obesity. Two processes that have been prominent within the health psychology literature and which play a significant formative role, attachment and life satisfaction will be briefly discussed in turn. The first of these, in particular, attachments in infancy, has been shown to play a profound role in emotional regulation (Bowlby, 1969, 1973, 1980) and consequential health-related behaviours. Bowlby’s well-known Attachment Theory described the infants’ need to maintain proximity to an anchor person who in the most ideal situation is a ‘secure base’ from where to explore the environment. ‘Attachment’ refers to an enduring affectional bond of substantial intensity (Bowlby, 1969, 1973, 1980). The availability and responsiveness of the anchor person in engaging with the infant’s needs creates a template for social interaction. The theory elucidates how experiences with significant others are internalized into mental models of the world and the self, and how these models are generalized to new relationships right through to the individual’s death (Ainsworth et al., 1978).

The Homeostatic Theory of Health.
Behaviours and strategies which develop and maintain affectional bonds persist throughout life and are activated in order to maintain some degree of proximity to highly discriminated persons. According to Bowlby’s theory, attachment behaviour is protective and facilitates learning. Three primary attachment types or styles have been distinguished – secure, avoidant and anxious-ambivalent – and attachment of whichever type can play a role in both childhood and adulthood emotionality (Hazan and Shaver, 1987). Bowlby and Ainsworth both emphasized that attachment experiences in early life involve strong affect across the whole gamut of emotions and feelings, including security, anxiety, fear, anger, love, grief and jealousy.
Thus, in Attachment Theory, a model for the whole of life is drawn from processes formed in association with the primary caregiver. The evidence to be reviewed indicates that early parental attachment style plays a critical role in the homeostatic regulation of emotion and in the formation and modification of health-related behaviours such as eating habits (Tabacchi et al., 2007), drinking habits (Van der Vorst et al., 2006), substance abuse (Schindler et al., 2005) and romantic love (Brennan and Shaver, 1995). Emotion regulation is a homeostatic process that plays a critical role in the production of ill health, both direct and indirect (Kuh et al., 2003). DeSteno et al. (2013) summarized evidence that chronic high childhood distress at age 7 or 8 is associated with a range of adult physical health outcomes such as obesity (Goodwin et al., 2009), number of physical illnesses (Kubzansky et al., 2009) and inflammation (Appleton et al., 2012).
Infant feeding is an intimate process that determines not only the content and amount of feeding but how a mother and infant interact during feeding (Shloim et al., 2015). Early feeding experiences predict eating later in life (Nicklaus and Remy, 2013). Parents who bottle-feed may not recognize the infant’s signals of hunger or fullness and thus overfeed their infant, potentially reducing the infant’s ability to self-regulate when older (Birch, 2006). Breastfeeding the infant can actively regulate the flow of milk from the breast, controlling the pace of the meal and the sense of fullness (Shloim et al., 2015). Long-term effects of early feeding styles have been observed at 6 years of age such that bottle-fed infants are more likely to be expected to empty their bottles and show lower satiety responsiveness compared to breast-fed infants (Li et al., 2014). Excessive parental control over feeding such as restriction or pressure to eat may be adversely associated with under- or over-feeding, respectively, potentially leading to feeding problems (Farrow and Blissett, 2006; Johnson and Birch, 1994). Other studies suggest that lower levels of controlling feeding behaviours promote healthier eating behaviours in childhood (Birch et al., 2007; Faith et al., 2004; Fisher and Birch, 1999).
Childhood dietary habits tend to persist into adulthood, with parental influences that are internalized and enacted in dietary choices throughout the lifespan. Future emotion regulation is set by parental/caregiver patterns of interaction with their children (Mikulincer and Shaver, 2007). Troisi et al. (2005) observed that women with eating disorders reported having more severe symptoms of separation anxiety during childhood, and scored higher on a scale assessing insecure styles of adult attachment. Goossens et al. (2012) reported that insecure attachment towards the mother among 8- to 11-year-olds predicted increases in dietary restraint, eating concerns, weight concerns and shape concerns, and adjusted BMI in children 1 year later. Insecure parental attachment, whether actual or recalled, has been associated with high calorific food consumption (Faber and Dubé, 2015). Similar findings exist for adult drinking problems and antecedent attachment style (Molnar et al., 2010).
Thus, there is a strong evidence base showing that attachment patterns in childhood are associated with a variety of homeostatic behaviours throughout life, particularly consumption of food, drink and drugs, and social relationships with romantic partners, family and friends. Complex social patterns, geared by early parental attachments, also affect subjective well-being and life satisfaction, to which I turn.
Life satisfaction
How satisfied a person is with his or her life, the level of subjective well-being, is a key concept for health as homeostatic equilibrium. According to Diener and Chan (2011), having high life satisfaction adds 4–10 years to the lifespan. The life-satisfaction construct is given an operational definition by the method used for its measurement. One prominent scale has been the Satisfaction With Life Scale (SWLS; Diener et al., 1985) that uses a 7-point Likert scale with five items:
In most ways, my life is close to my ideal.
The conditions of my life are excellent.
I am satisfied with my life.
So far I have gotten the important things I want in life.
If I could live my life over, I would change almost nothing.
The SWLS items provide a definition of well-being that is hedonic. However, life satisfaction is also about meaningfulness, purpose and self-realization, or the degree to which a person is ‘fully functioning’ (Ryan and Deci, 2001). Eudaimonic well-being occurs when a person lives in accordance with his or her ‘daimon’ or true self (Waterman, 1993). Eudaimonia occurs when life activities are informed by deeply held values and are authentic expressions of such values.
Empirical studies suggest strong and stable relationships between meaning in life and subjective well-being (Zika and Chamberlain, 1992). People who experience their lives as meaningful are more optimistic and self-actualized (Compton et al., 1996), experience more self-esteem (Steger et al., 2006), more positive affect (King et al., 2006), less depression and anxiety (Steger et al., 2006) and less suicidal ideation (Harlow et al., 1986). The salutogenic theory of Antonovsky (1979) emphasized the relationship between meaning and purpose in life, assessed using the Sense of Coherence scale, and positive health outcomes (Eriksson and Lindström, 2006). Eudaimonic well-being is similar to the concept of ‘self-actualization’ espoused by Maslow (1943). To date, the evidence for the protective effects of hedonic well-being on heart health is stronger than for eudaimonic well-being (Boehm and Kubzansky, 2012). When eudaimonic aspects to life satisfaction are combined with hedonic well-being, the association with longevity could be even more robust. Evidence for an association between life satisfaction and all-cause mortality is mounting in several domains, suggesting a causal link between life satisfaction, affect, consumption and health. These causal links are included within the Homeostatic Theory of Health (Figure 5).

The Homeostatic Theory of Obesity.
Considering any population as a whole, there is a large group of people who experience a statistically average level of life satisfaction who are neither satisfied nor dissatisfied with their lives. A range of one-half of 1 standard deviation on either side of the mean includes 38.2 per cent of the population who can be assumed to be at or close to homeostasis. They are neither content nor discontent. Set-points may move up and down according to circumstances (Diener, 2000), and adaptation processes occur to help people move towards a position of perceived (by them) well-being even if the objective circumstances are quite dire (Headey and Wearing, 1992). Although a small percentage (<5%) may swing from one extreme to the other, life satisfaction in adults is moderately stable over significant periods of the lifetime (Eid and Diener, 2004; Koivumaa-Honkanen et al., 2005). Homeostatic imbalance is evident when life satisfaction falls below an equilibrium set-point towards significant dissatisfaction and discontent (30.9% of the population). This state of relatively stable discontent is associated with negative affect and, frequently, over-consumption of unhealthy food and/or drink. The associations become stronger as the dissatisfaction level increases. Among an identifiable section of the population, life dissatisfaction can become persistent and more extreme, placing them at risk of adverse health outcomes (Koivumaa-Honkanen et al., 2005). A state of extreme dissatisfaction/discontent/disequilibrium over a long period typically is associated with a variety of adverse consequences including depression, anxiety, alcoholism, substance abuse, smoking, gambling, insomnia, accidental injury, inadequate coping and obesity. A few illustrative studies can be summarized here.
Newcomb et al. (1986) assessed 640 adolescents and 4 years later as young adults on associations between their alcohol use and dissatisfaction. Cross-lagged latent variable structural models were employed to evaluate the antecedents and consequences of alcohol use on the life-satisfaction measures. Alcohol Use and Self-Derogation were positively correlated at the first time point. However, adolescent alcohol helped them as young adults to feel better about themselves but increased dissatisfaction levels regarding peer relationships and the environment.
Self-reported life satisfaction and mortality were investigated in a prospective study (1976–1995) of 22,461 healthy Finnish adults (Koivumaa-Honkanen et al., 2000). Life satisfaction was scored as a three-category variable yielding the satisfied group (21%), intermediate group (65%) and dissatisfied group (14%). The age-adjusted hazard ratios of all-cause, disease or injury mortality among dissatisfied versus satisfied men were 2.11, 1.83 and 3.01, respectively. Dissatisfaction was associated with increased disease mortality, particularly in men with heavy alcohol use (hazard ratio = 3.76). In a related study, Koivumaa-Honkanen et al. (2004) investigated the relationship between life satisfaction and depressive symptoms in healthy adults both cross-sectionally and longitudinally with a nationwide sample of healthy adults (N = 9679), aged 18–45 years. Longitudinally, a strongly increased risk of moderate or severe depression in 1990 was observed among those who had been dissatisfied compared with those satisfied in 1975 (odds ratio (OR) = 6.7) and in 1981 (OR = 10.4).
Strine et al. (2008) examined associations between life satisfaction and health-related quality of life, chronic illness and adverse health behaviours among adults. They used the 2005 Behavioral Risk Factor Surveillance System database in which 5.6 per cent of US adults (about 12 million) reported that they were dissatisfied or very dissatisfied with their lives. A strong and consistent relationship existed between life dissatisfaction, negative affect and excessive consumption, including smoking and heavy drinking. As the level of life satisfaction decreased, the prevalence of fair or poor general health, disability and infrequent social support increased as did physical distress, mental distress, activity limitation, depressive symptoms, anxiety symptoms, sleep insufficiency and pain.
The association of alcohol use and alcohol-related problems in several domains of life satisfaction was studied in a sample of 353 students (Murphy et al., 2005). Alcohol-related problems were associated with decreased life satisfaction among both men and women. In a cross-cultural analysis of 17,246 students from 21 countries, Grant et al. (2009) studied the relationship between life satisfaction and seven health behaviours. Grant et al. found that life dissatisfaction was positively associated with smoking, lack of physical exercise, failure to use sun protection, not eating fruit and fat intake, but after adjusting for age, gender and data clustering, it was unrelated to alcohol consumption or fibre intake.
Zullig et al. (2001) explored the relationship between perceived global life satisfaction and selected substance use behaviours among 5032 public high school students in the 1997 South Carolina Youth Risk Behavior Survey. Cigarette smoking, chewing tobacco, marijuana, cocaine, regular alcohol use, binge drinking, injection drug and steroid use were significantly associated with reduced life satisfaction. In addition, age of first alcohol drink, first marijuana use, first cocaine use and first cigarette smoked were all significantly associated with reduced life satisfaction.
Kuntsche and Gmel (2004) found that binge drinkers had lower life satisfaction, more depression and were more often offenders of bullying and hitting. Solitary binge drinkers were found to be the most socially inhibited, prone to depressive symptoms and victims of bullying in comparison to social binge drinkers who were socially accepted but more likely to be actual offenders of violence (Kuntsche and Gmel, 2004).
Brassai et al. (2015) explored the role of meaning in physical activity and healthy eating among 456 East-European adolescents. The presence of meaning, search for meaning, subjective well-being and health values at Time 1 were used to predict levels of healthy eating and physical activity 13 months later. All four variables predicted engagement in healthy eating and physical activity; presence of, and search for, meaning were the most robust predictors of healthy eating among boys and physical activity among girls.
Conclusions on health and homeostatic regulation
Strikingly powerful associations have been evidenced between attachment style, life satisfaction and health-seeking behaviours, particularly those concerning consumption. Hazard ratios for discontented versus contented samples typically range from 3.0 to 10.0. It is apparent that dissatisfied, distressed and discontented people eat and drink to excess, assuaging not only their hunger and thirst but their considerable discontents. Those experiencing dissatisfaction over protracted periods of their lives are in prolonged disequilibrium. Although set-points may move up and down with adaptation to diverse scenarios and circumstances of living, either the balance point of equilibrium is set at a higher level or people are working harder to reach their balance point. When a thermostat is set at a higher temperature, more energy must be burned to reach homeostasis. When psychological homeostasis has a higher set-point, more energy must be consumed in striving for equilibrium.
Theory of obesity
In the present theory, obesity is at least in part a consequence of homeostatic imbalance in the psychological sphere (Figure 6). 3 I focus here on five feedback loops that form an insidious and vicious ‘COD’ (Figure 6). The theory assumes that for most people, much of the time, these five pathways are in equilibrium. When so, it is a Circle of Content. However, if, for whatever reason, high levels of dissatisfaction, negative affect, consumption or increased body weight should arise, then the interactivity through the feedback loops forms a vicious circle, a disturbance to the stability of the system that controls weight gain. Once activated, the system drifts away from equilibrium towards what in effect becomes a dysfunctional state of non-control. This follows from the fact that the activation of any one of the four processes within the circle will activate its neighbours. The feedback loops will run up activity levels throughout the system which will go into overdrive, similar to a badly performing motorcar with the accelerator pedal stuck all the way to the floor. 4 I discuss each of the six pathways in turn in light of representative studies. 5

The Circle of Discontent.
Pathway 1: Reciprocal causal relationships exist between overweight/obesity and body dissatisfaction
Many investigators have found an association between overweight or obesity and body dissatisfaction. Presnell et al. (2004) examined risk factors for body dissatisfaction using prospective data from 531 adolescent boys and girls. Elevations in body mass, negative affect and perceived pressure to be thin from peers, but not thin-ideal internalization, social support deficits or perceived pressure to be thin from family, dating partners or media, predicted increases in body dissatisfaction. Gender was found to moderate the effect of body mass on body dissatisfaction and also negative affect. McLaren et al. (2003) studied the relationship between past body size and current body dissatisfaction among 933 middle-aged women from a prospective birth cohort study. Women who were dissatisfied at mid-life were found to have been heavier at age 7 and showed a more rapid increase in BMI with age.
Neumark-Sztainer et al. (2006) investigated body dissatisfaction in a prospective study with 440 early adolescent girls and 366 boys and 946 mid-adolescent girls and 764 boys. Participants were followed up 5 years later (Time 2). Prospective risk factors included BMI, socioeconomic status, ethnicity, parent dieting environment, peer environment and psychological factors. Predictors of Time 2 body dissatisfaction were Time 1 body dissatisfaction, BMI, socioeconomic status, being African American, friend dieting and teasing, self-esteem and depression. However, the profile of predictors differed across the samples.
A construct that could be a valuable element in designing interventions is self-compassion with three components: (1) self-kindness – being kind and understanding towards oneself in instances of pain or failure rather than being harshly self-critical; (2) common humanity – perceiving one’s experiences as part of the larger human experience rather than seeing them as separating and isolating, and (3) mindfulness – holding painful thoughts and feelings in balanced awareness rather than over-identifying with them (Neff, 2003: 85). In a sample of undergraduates, Duarte (2015) found BMI to be highly positively associated with body image dissatisfaction (r = .58), in line with pathway 1. A novel finding was that self-compassion buffered the association between negative body image evaluations and young women’s quality of life.
An investigation by Cruz-Sáez et al. (2015) of emotional distress and body image concerns in 712 Basque Country, Spanish normal-weight and overweight adolescent girls reported evidence that is fully consistent with the CODT. Cruz-Sáez et al. (2015) found 12.3 per cent of normal-weight girls and 22.5 per cent of overweight girls with extreme weight-control behaviours (EWCBs), that is, self-induced vomiting, taking laxatives, diuretics, diet pills and fasting. In normal-weight adolescents, engagement in EWCBs was associated with high levels of somatic symptoms, a drive for thinness and control overeating. In overweight girls, high levels of emotional distress, body dissatisfaction and depression were associated with EWCBs. The Cruz-Sáez et al. (2015) findings are completely consistent with the CODT. Highly significant positive relations were found between BMI, emotional distress, body image concerns and EWCBs, as predicted.
EWCBs represent an adolescent’s striving to restore a more ideal state of homeostasis, to break the COD by restoring and normalizing equilibrium between their body weight, body satisfaction, affect and consumption. In Cruz-Sáez et al.’s study, EWCBs occurred with greater frequency in overweight than in normal-weight adolescents. The overweight adolescent females reported a greater drive for thinness, more body dissatisfaction and more negative self-beliefs. In normal-weight females, emotional distress, negative self-belief, control overeating and drive for thinness predicted engagement in EWCB. In overweight girls, General Health Questionnaire-28 (GHQ-28) total score, depression and body dissatisfaction predicted EWCB. These results led the authors to conclude
emotional distress, excessive importance placed on physical appearance to define oneself, low self-esteem and the negative cognitions associated with the body and eating, play an important role in the development of weight-control behaviours that put adolescent girls’ health at risk, even those considered normal-weight. (Cruz-Sáez et al., 2015)
Further analyses were presented by Cruz-Sáez et al. (2013).
Pathway 2: Reciprocal causal relationships exist between body dissatisfaction and negative affect
Several studies have provided evidence consistent with pathway 2 in the CODT. In a prospective study, Rierdan et al. (1989) evaluated the importance of body image in early adolescent girls’ depression. Depression scores of over 500 girls were assessed twice, in the fall (Time I) and spring (Time 2) of a school year. Discriminant analyses indicated that body image at Time 1 was important in the prediction of persistence of depression. Paxton et al. (2006) examined whether body dissatisfaction prospectively predicted depressive mood and low self-esteem in adolescent girls and boys 5 years later. Time 1 body dissatisfaction was a unique predictor of Time 2 depressive mood and low self-esteem in early-adolescent girls and mid-adolescent boys. They concluded body dissatisfaction is a risk factor for depressive mood and low self-esteem in both girls and boys but at different phases of adolescence.
Mond et al. (2011) found that impaired emotional well-being of overweight adolescents is due primarily to the effects of weight-related body dissatisfaction during both early and late adolescence. The authors concluded that body dissatisfaction is ‘central to the health and well-being of children and adolescents who are overweight’. A reciprocal causal association between depression and body dissatisfaction was also reported by Keel et al. (2001). Participants had completed a controlled treatment study of bulimia nervosa and participated in follow-up assessments 10 years later. Baseline levels of depression were found to prospectively predict body dissatisfaction at follow-up assessment, suggesting that depression is a contributing factor in the maintenance of body dissatisfaction over a 10-year period.
In a prospective study, Wardle et al. (2001) found that baseline depression was associated both with body satisfaction and binge eating and that depression contributed independently to binge eating and partly mediated the body-dissatisfaction effect. This pattern was confirmed in the longitudinal analysis with reduced depression being associated with less binge eating, and reduced depression partly mediated the effect of reduction in body dissatisfaction. Wardle et al. (2001) suggested that ‘reductions in depressed mood or improvements in well-being during obesity treatment might be expected to have enduring effects on eating control’ (p. 778).
Pregnancy tends to be a period of stress and anxiety, especially if there is an eating issue (Ward, 2008). Clark et al. (2009) examined depression and body dissatisfaction across pregnancy and the first 12 months postpartum. During pregnancy, women’s perceived attractiveness and strength/fitness remained stable, while feeling fat and salience of weight/shape decreased in late pregnancy. During the postpartum, feeling fat and salience of weight/shape increased. Depression and body dissatisfaction were correlated concurrently and across multiple time points. Prospective analyses carried out by Clark et al. suggested that greater depression late in pregnancy predicts body dissatisfaction at 6 weeks postpartum and feeling fat throughout the postpartum.
Pathway 3: Reciprocal causal relationships exist between negative affect and consumption of high-density foods and beverages
Reciprocal causal links in the pathway between negative affect and consumption of high-energy foods are well established in the literature. For example, the following quotations provide evidence from qualitative studies:
Food is like a sedative to me. It knocks me out, like a drug. When I feel any little bit of sadness or anger, I eat. It’s almost like being fed as a baby. I will eat and eat until I can’t move and then I go and lie down and I sleep. And it’s almost like, ‘Here baby, come to mother …
Or
Eating stops the process of my brain going. It offers relief from thoughts that might actually be quite uncomfortable. (Byrne et al., 2003)
These qualitative findings are borne out by many quantitative studies. People eat to calm themselves, reward themselves, assuage sadness or guilt or to reduce feelings of isolation. A variety of discontents have been shown to have associations with food consumption, including basic need satisfaction (Timmerman and Acton, 2001), anxiety (Nguyen-Rodriguez et al., 2009; Schneider et al., 2010), anger (Macht, 1999), stress (Adam and Epel, 2007) and boredom (Crockett et al., 2015). Emotional eating has been viewed as an ‘escape’ to avoid negative self-awareness resulting in behavioural disinhibition and overeating (Heatherton and Baumeister, 1991). Distress- or discomfort-induced eating, including binge eating, is an available response to negative emotions (Arnow et al., 1995; Stice, 2001; Stice et al., 2002; Van Strien and Ouwens, 2007) as is overeating in vulnerable individuals (Van Strien et al., 2005). Some studies suggest that women are more prone to emotional consumption than men (Grunberg and Straub, 1992; Tanofsky et al., 1997). Men may rely more frequently on other outlets such as drinking, drugs and gambling (see below).
Le Port et al. (2012) examined the association between dietary patterns and depressive symptoms over 10 years in a French cohort of 12,400 people aged 45–60 years. Low-fat, Western, snacking and fat-sweet diets in men, and low-fat and snacking diets in women, were associated with depressive symptoms at the start and at follow-up. Conversely, a traditional diet (characterized by fish and fruit consumption) was associated with a lower likelihood of depressive symptoms in women. The healthy pattern, characterized by vegetable consumption, was associated with a much reduced risk of depressive symptoms. The authors suggested that there was probably a reverse causality effect for the healthy pattern.
In a longitudinal, population-based study of 2359 men and 2791 women in Northern Finland, BMI at 31 years was highest among stress-driven eaters and drinkers, especially among women (Laitinen et al., 2002). Stress-driven eaters liked eating sausages, hamburgers and pizza and chocolate more frequently than other people and consumed more alcohol.
Rosenbaum and White (2015) investigated depression, anxiety and stress as independent correlates of binge eating in a mixed, community sample with diverse backgrounds. The findings indicated a relationship between anxiety and binge eating, and between stress and binge eating, independent of depression.
Holt et al. (2015) examined whether there is a relationship between trans fatty acid (TFA) intakes and emotion regulation, mediated by positive or negative affect. Archival data on 1699 men and 3293 women were analysed to measure TFA intake at baseline, positive and negative affect and emotion regulation at follow-up. Holt et al. (2015) reported that higher TFA intake was associated with subsequent difficulties with emotional awareness, clarity and regulation strategies, all of these relationships being mediated by affect. Lower TFA intake was associated with increased positive and decreased negative affect which, in turn, was associ-ated with improved emotion regulation. These findings suggest that TFA intakes may cause problems in the regulation of emotion.
Rocke (2015) revealed that proneness to boredom and difficulties in emotion regulation simultaneously predict inappropriate eating behaviour, including eating in response to boredom, other negative emotions and external cues. Economic pressures influenced depressive symptoms and spousal support which served as a buffer against poor health and weight management behaviours for husbands, while depressive symptoms exacerbated poor health and weight management behaviours for wives (O’Neal et al., 2015). Economic hardship can also trigger disrupted sleep. Lundahl and Nelson (2015) propose four ways in which sleep problems are likely to increase food intake, namely, homeostatic mechanisms which disrupt appetitive hormones, impaired executive/cognitive functions with corresponding increases in reward sensitivity, increased negative affect and stress and increased impulsivity. Guertin et al. (2015) tested a longitudinal motivation model for healthy eating in patients with CVD. Participants with self-determined motivation were found to be more likely to develop a sense of self-efficacy towards eating and a healthy diet, which had beneficial effects on their physical health and life satisfaction.
Brown et al. (2015) reported gender differences and correlates of extreme dieting behaviours (EDBs) among 15,425 US adolescents from the 2011 Youth Risk Behavior Survey. Being hit by a partner, being raped, bullied in school, e-bullied and feelings of hopelessness were all associated with a higher OR for EDBs in both females and males and concluded that ‘fasting, diet pill use, and purging may be quick and useful markers (‘red flags’) for other risk behaviours and mental health difficulties for both genders’. EDBs are an indicator of restraint, conscious striving towards homeostasis.
Restraint
When negative affect can so easily trigger emotional consumption, dietary restraint is used to strive towards a set-point for weight, a conscious form of homeostasis (Figures 5 and 6). The association between restraint, dieting and binge eating has been extensively researched for at least four decades (Herman and Mack, 1975; Polivy and Herman, 1985). Dietary restraint involves a conscious effort to eat according to cognitive cues rather than physiological cues such as hunger or satiety in order to lose or maintain weight (Herman and Mack, 1975). Herman and Mack (1975) presented sequence data indicating that dieting usually precedes binge eating chronologically. Evidence suggests that distress suppresses eating in non-dieters (unrestrained eaters), but increases it in chronic dieters (restrained eaters) (e.g. Baucom and Aiken, 1981).
Polivy and Herman (1999) investigated the ‘masking hypothesis’ that dieters use overeating to mask distress in other areas of their lives by eating when distressed so they can attribute their distress to their overeating rather than to more uncontrollable aspects of themselves or their lives. Other hypotheses include the idea that eating acts as a distraction from negative affect or that eating is a form of learned helplessness. Polivy and Herman (1999) led female college participants to believe that they had failed or not failed a cognitive test and then gave them either ad libitum or three small spoonfuls of ice cream to taste and rate. They indicated that the masking, distraction and helplessness hypotheses all received some support and that they may work in tandem with each other. Polivy and Herman’s results suggested that distress-induced overeating in restrained eaters may serve psychological functions for the individual, allowing distraction from the distress or masking of the source of dysphoria.
Restraint also can create a rebound effect as binge eating. Marcus et al. (1985) determined the prevalence and severity of binge eating among 432 women. In all, 46 per cent of the women reported serious binge eating, especially younger and heavier women, in whom binge eating severity was related to overall dietary restraint. Other studies have not confirmed this finding. In a prospective study, Johnson and Wardle (2005) found no evidence of a rebound of bulimic binge eating among restrainers, whereas body dissatisfaction was associated with all adverse outcomes, in line with many studies showing a strong association between body dissatisfaction and depression (e.g. Paxton et al., 2006).
Pathway 4: Reciprocal causal relationships exist between consumption of high-energy foods and overweight or obesity
Many strands of evidence suggest causal links between the consumption of high-caloric foods containing high levels of fat and/or sugar and the development of obesity. A review of clinical trials with humans that studied the effects of a reduction in the amount of energy from fat in the diet showed that a reduction of 10 per cent in the proportion of energy from fat was associated with a reduction in weight of 16 g per day (Bray and Popkin, 1998). A more recent review came to similar conclusions (Hooper et al. 2012), suggesting a causal link between ingested fat and weight change. Passive over-consumption of high-fat foods, in particular, has been linked with a higher frequency of obesity (Blundell and MacDiarmid, 1997). In a prospective study with 107,243 postmenopausal American women aged 50–79 years, greater chocolate-candy intake was associated with greater prospective weight gain (Greenberg et al., 2015).
Increased usage of sugar-sweetened beverages has been found to cause weight gain and incidence of type 2 diabetes in young and middle-aged women (Schulze et al., 2004). Systematic review of prospective cohort studies and randomized controlled trials (RCTs) by Malik et al. (2013) showed evidence that consumption of sugar-sweetened beverages promotes weight gain in children and adults.
Economic analyses suggested that the increased prevalence of obesity in the United States can be largely attributed to the increased frequency of snacking in the diet (Cutler et al., 2003; Jahns et al., 2001).
McDonald et al. (2009) investigated the prevalence of overweight and any associations with dietary patterns and physical activity in a prospective study in children in Bogotá, Colombia. Overweight was 3.6 times greater in children whose mothers were obese compared with children whose mothers had adequate BMI. Child overweight was also positively associated with adherence to a ‘snacking’ dietary pattern and to frequent intake of hamburgers and hot dogs with a prevalence ratio for at least once per week versus never of 1.93, independent of total energy intake and other potential confounders. In a second report, a snacking dietary pattern and soda intake were both found to be related to the development of adiposity (Shroff et al., 2014). Snacking and eating during the night is more apparent in people suffering from psychological distress (Colles et al., 2007) and depression, and is a risk factor for obesity (Gallant et al., 2012).
Pathway 5: Reciprocal causal relationships exist between obesity and negative affect
Setting aside the fact that weight gain is an unwanted side effect of some drug treatments for psychiatric disorders (Zimmerman et al., 2003), psychiatric studies indicate a reliable association between depression and obesity. This association has been observed in both cross-sectional and prospective studies. Onyike et al. (2003) studied rates of depression for both men and women as a function of BMI. The participants were 9997 respondents to the National Health and Nutrition Examination Survey (NHANES), an interview survey of the US population. Obesity was associated with increased rates of depression. A prospective study of depression and adolescent obesity with 9374 participants by Goodman and Whitaker (2002) showed that depressed mood at baseline independently predicted obesity at follow-up (OR: 2.05). Depressed mood at baseline also predicted obesity at follow-up among those not obese at baseline (OR: 2.05). Werrij et al. (2006) investigated whether depressive symptoms in people with overweight or obesity is related to increased eating problems and decreased self-esteem. Depressed participants were observed to suffer from more eating problems, more restraint and higher BMI than non-depressed participants.
Roberts et al. (2003) examined the temporal association between obesity and depression in a two-wave, 5-year observational study with 2123 participants, aged 50 years and older. Obesity at baseline was associated with increased risk of depression 5 years later, even after controlling for depression at baseline and an array of other covariates. Luppino et al.’s (2010) systematic review of longitudinal studies of depression and obesity indicated that obesity at baseline increased the risk of onset of depression at follow-up by 55 per cent, while overweight increased the risk of onset of depression by 27 per cent. Similar findings were published by Faith et al. (2011) from a Swedish longitudinal case control study of children from birth to 15 years in which children more than 15 per cent above average weight had suffered more psychosocial stress than controls (Mellbin and Vuille, 1989). In a prospective study of 7965 British civil servants aged 35–55 at entry into the Whitehall II study, Kivimäki et al. (2006) measured work stress and BMI at baseline and 5 years later. A bidirectional effect of work stress on BMI was evident among overweight and obese men, but weight loss was more likely among stressed lean men.
Pathway 6: Linking body dissatisfaction directly with consumption
Relatively few studies have investigated the direct association between body dissatisfaction and consumption of food and beverages. Stice and Shaw (2002) reviewed evidence that pressure to be thin, thin-ideal internalization and elevated body mass increased the risk for body dissatisfaction. They found consistent support for body dissatisfaction as a risk factor for eating pathology. However, they concluded that this relationship is mediated by increases in dieting and negative affect, in consistency with the CODT. Because findings have been inconsistent, the potential role of the pathway from body dissatisfaction to consumption remains uncertain (Figure 7, pathway 7).

Treatment and prevention of obesity as a restoration of homeostasis.
Variations in the COD
The pattern of findings across the studies reviewed is consistent with the CODT. Previous theories of overweight and obesity have focused on similar features:
The Psychosomatic Theory suggested that eating reduces anxiety, and individuals become overweight or obese because they learn to eat in response to emotional arousal or to reduce anxiety rather than in response to internal hunger cues (Bruch, 1961; Kaplan and Kaplan, 1957).
The Spiral Model proposed by Todd Heatherton and Janet Polivy (1992) hypothesized that negative self-evaluations by dieters when confronted with slim body images leads to a spiral of increased negative affect and body dissatisfaction, reduced self-esteem and increased susceptibility to dietary disinhibition and overeating.
The Stress/Reward Model of Tanya Adam and Elissa Epel (2007) has also proposed that the obesity epidemic is being exacerbated by the prevalence of chronic stress, unsuccessful attempts at food restriction and the effects on increasing the reward value of high-energy food.
The three theories, in common with the CODT, share the assumption that eating and drinking are, in part, responses to arousal of negative affect. As a specific case of the Homeostatic Theory of Health, the CODT can be confirmed or falsified using prospective investigations, qualitative studies and case reports. The unifying concept extends to the field of psychology, a principle that has been established in physiology for at least 150 years.
The ‘COD’ as a phenomenon of the human condition is evident in different populations, religious, cultural and ethnic groups, but the form of its expression varies according to national and group-specific preference patterns of consumption. A few illustrative examples follow.
In overweight adolescents and women, consumption of sugar-sweetened beverages is a trend that is associated with weight gain (e.g. Schulze et al., 2004). Large differences exist between different countries in the frequency of use of soft drinks and sweets (Kuusela et al., 1999). For a significant proportion of men, and a smaller proportion of women, alcohol, smoking, cannabis and/or psychotropic drugs may be used as a form of ‘self-medication’ instead of food when confronted by stress, anger, anxiety or depression (Breslau et al., 1993; Helzer, and Pryzbeck, 1988; Patton et al., 1996, 1998; Swendsen et al., 1998). For sexual minorities, of same-sex and both-sex attracted people, a greater reliance tends to be placed on binge drinking than in heterosexual people (Brewster and Tillman, 2011; Lindley et al., 2011; Midanik et al., 2007; Pega et al., 2012; Taliaferro et al., 2014).
Self-medication with tobacco, drugs and/or alcohol readily can become an ‘addictive behaviour’ with loss of control and unpleasant effects when ceased. Capitalist culture enshrines a belief in individualism and personal control, and addictive behaviours are viewed as ‘mental disorders’. Yet, the most harmfully addictive substances are promoted through televisual and multi-media mass propaganda to consumers who are ever consuming ever increasing amounts of sugary beverages in the form of cola and alcohol and fatty, salty, sugary foods, tobacco and gambling (Marks, 1998).
Vandewalle et al. (2014) explored the association between parental rejection and emotional eating in 110 obese young people aged between 10 and 16 years attending a Belgian treatment centre for obesity. Participants completed questionnaires assessing maternal and paternal rejection, emotion regulation strategies and emotional eating. Vandewalle and colleagues found that the use of maladaptive emotion regulation strategies mediated the relation between maternal rejection and emotional eating. Paternal rejection itself was not found to be associated with emotion regulation or with emotional eating in the young people. These findings are in line with the CODT.
Sutin et al. (2011) studied the association between personality and obesity across the adult lifespan. They investigated personality associations with adiposity and fluctuations in BMI in 1988 participants over more than 50 years. Sutin et al. modelled the BMI trajectory across adulthood and tested whether personality predicted its rate of change. Participants with higher scores on Neuroticism or Extraversion or lower scores on Conscientiousness had higher BMI, more body fat and larger waist and hip circumferences. The strongest association was found for impulsivity. Participants who scored in the top 10 per cent of impulsivity weighed, on average, 11 kg more than those in the bottom 10 per cent. Longitudinally, high neuroticism and low conscientiousness, and difficulty with impulse control, were associated with weight fluctuations, measured as the variability in weight over time, in line with pathways 3 and 5 of the CODT.
People with Type D personality experience increased negative emotions across time and situations and often choose not to share these emotions with others because they fear rejection or disapproval. Booth and Williams (2015) investigated the relationship between Type D and dietary intake in a cross-sectional study with 187 healthy participants measuring Type D personality, dietary intake and coping. Type D was associated with maladaptive coping and significantly less healthy food intake, including more consumption of fat and sugar, and significantly less consumption of fruits and vegetables (F/Vs). This relationship was partially mediated by coping. The negative affect experienced by Type D personality is a risk factor for unhealthy eating, in line with pathway 3 of the CODT.
Spoor et al. (2007) examined the association between negative affect, coping and emotional eating in 125 eating-disordered women and 132 women from a Dutch community population. Both emotion-oriented coping and avoidance distraction were found to be related to emotional eating, while controlling for levels of negative affect. The authors concluded that
It is possible that emotional eaters may have fewer emotion-regulation strategies that effectively downregulate negative emotions. They may then try to escape from these emotions by means of overeating as they believe or have learned that eating can possibly reduce aversive emotions. (Spoor et al., 2007: 373)
This suggestion is in line with pathway 3 in the CODT.
Chao (2015) examined the relationships between chronic stress, food cravings and BMI with a community-based sample of 619 adults. Chronic stress had a significant direct effect on food cravings, and food cravings had a significant direct effect on BMI. The total effect of chronic stress on BMI was significant. However, food cravings partially mediated the relationship between chronic stress and BMI. Thus, chronic stress potentiates emotional eating and food cravings which, in turn, contribute to stress-related weight gain, as predicted by the CODT.
Summary of evidence concerning the CODT and implications for obesity prevention
The evidence summarized above is supportive of five pathways defined by the CODT. The evidence from prospective studies is particularly strong. Pending systematic investigations to test the theory within prospective studies, there is strong empirical support for the theory that the human obesity epidemic involves a breakdown in psychological homeostasis. In this light, I turn to the issue of how the obesity epidemic can be halted.
Prevention of obesity
Several strategies for the prevention of obesity spring from the Homeostatic Theory of Obesity. Predictions about causes, consequences and effects flow directly and transparently from the theory that obesity results from imbalanced weight-control homeostasis. The main pathways for the control of obesity are illustrated in Figure 7.
There are many hotly debated controversies about food, diets and dieting. Different dietary interventions for obesity have been extensively explored, yet a review of the literature indicates that outcomes have been universally modest. To date, many interventions, from simple trials of a single method to complex multi-component treatments, have yielded unexciting results. An upbeat discussion paper providing an economic perspective on obesity prevention listed 74 interventions across 18 groups (Dobbs et al., 2014). Weight management programmes were listed fourth in terms of estimated impact beneath portion control, reformulation and high-energy food and beverage availability. Behavioural interventions in obesity prevention and treatment have yielded disappointing outcomes. The report contained valuable economic analyses but little discussion of psychological evidence on the causes or consequences of overweight and obesity, and reliance was placed on ‘subconscious mechanisms’ illustrated by this quotation: ‘subconscious mechanisms change the physical activity and food and drink environments, and are therefore more likely to change behavior’ (Dobbs et al., 2014: 46). For ‘subconscious’, I think we have to read ‘contextual’, but the two terms cannot be used interchangeably because environmental changes described as ‘subconscious’ in the Dobbs et al. report are invariably perceived, for example, improved labelling of foods. A psychological analysis of the causes and consequences of overweight and obesity which yields effective interventions is absent from the Dobbs et al. report. The current article fills that gap.
Behavioural interventions in obesity prevention and treatment have yielded disappointing outcomes. Raising false hopes among people with overweight or obesity by continuing to offer interventions that have such poor outcomes is a questionable practice that should be terminated. In spite of strong motivation and significant effort, many large-bodied individuals cannot lose significant weight as it has a significant hereditary component. However, people who have become obese from a slimmer baseline have the potential to shed their weight gain and return to that baseline.
Economic analysis has been applied to interventions to help determine which should be prioritized. Sacks et al. (2010) compared the cost-effectiveness within Australia of two commonly proposed policy-based interventions: front-of-pack ‘traffic-light’ nutrition labelling (traffic-light labelling) and a tax on unhealthy foods (‘junk-food’ tax). Estimates of changes in energy intake were based on an assumed 10 per cent shift in consumption towards healthier options in four food categories (breakfast cereals, pastries, sausages and preprepared meals) in 10 per cent of adults. Sacks et al. (2010) concluded that such policy-based population-wide interventions offer excellent ‘value for money’ as prevention measures.
Cecchini et al. (2010) outlined public health strategies for chronic diseases closely linked to obesity. Prevention policies could generate substantial health gains while entirely or largely paying for themselves through future savings in health-care expenditures (Cecchini et al., 2010). These strategies include health communication strategies to improve population awareness about the benefits of healthy eating and physical activity, fiscal measures that increase the price of unhealthy food content or reduce the cost of healthy foods rich in fibre and regulatory measures that improve nutritional information or restrict the marketing of unhealthy foods to children.
Economic growth is driving increased consumption of high-caloric, low-nutrient foods and beverages and energy-saving devices in an environment where passive over-consumption is pervasive. A recent review of the economics of obesity concluded,
The interventions most likely to be cost-effective were the upstream interventions that targeted the environmental drivers of the obesity epidemic such as regulation related to unhealthy food and beverage advertising, front of pack nutrition labelling and taxes on unhealthy food and beverages. (Ananthapavan et al., 2014)
In light of the above theoretical discussion, four practical strategies for obesity prevention are: (1) putting a stop to victim-blaming, stigma and discrimination using anti-discrimination legislation; (2) devalorizing the thin-ideal by enforcing truth in advertising; (3) reducing the consumption of energy-dense, low-nutrient foods and drinks; and (4) improving access to and attractiveness of plant-based diets. None of these strategies is new. The ideas have been discussed for many years. However, these strategies have yet to be implemented with the energy and commitment that is warranted in light of the scale of the obesity epidemic and the forces which are causing it. In addition, these four strategies previously have not been given an integrated theoretical framework for obesity prevention.
Anti-discrimination legislation
In reviewing research, Puhl and Brownell (2004) stated,
Research is clear in showing that obese individuals are highly stigmatized, and that bias and discrimination are often a consequence. Given that half the [American] population is overweight, the number of people potentially faced with discrimination and stigmatization is immense. The consequences of being denied jobs, disadvantaged in education, or marginalized by health care professionals because of one’s weight can have a profound impact on family life, social status, and quality of life. Obese individuals can suffer terribly from this, both from direct discrimination and from other behaviours (e.g. teasing and social exclusion) that arise from weight-related stigma. (p. 69)
An updated review in 2009 found no evidence that negative attitudes towards obese people were becoming less prevalent (Puhl and Heuer, 2009). The authors concluded that weight bias will remain a social injustice and public health issue, impairing the quality of life for both present and future generations of obese individuals.
What is concerning is the fact that weight bias exists not only in the lay population but in health-care professionals specializing in obesity. Schwartz et al. (2003) used the Implicit Associations Test (IAT) and a self-report questionnaire to assess attitudes, personal experiences with obesity and demographic characteristics with clinicians and researchers attending the opening session of an international obesity conference (N = 389). The IAT was used to assess implicit weight bias (associating ‘obese people’ and ‘thin people’ with ‘good’ vs ‘bad’) and three ranges of stereotypes: lazy–motivated, smart–stupid and valuable–worthless. The health professionals showed significant pro-thin, anti-fat implicit bias on the IAT. In addition, participants significantly endorsed the implicit stereotypes of lazy, stupid and worthless using the IAT. Lower levels of implicit anti-fat bias were associated with being male, older, having a positive emotional outlook on life, weighing more, having friends who are obese and indicating an understanding of the experience of obesity.
As Schwartz et al. (2013) point out, the fact that professionals whose careers emphasize research or the clinical management of obesity show very strong weight bias indicates ‘pervasive and powerful stigma’. There is little reason to think anti-fat stigma will have lessened over the last 12 years.
In the United States, discrimination is prohibited under public laws enacted by Congress. For example, federal funding of research is granted only if there is no discrimination on the basis of race, colour, national origin, religion, gender or physical or mental disabilities:
… no person in the United States shall, on the grounds of race, color, national origin, religion, gender, or physical or mental disabilities, be excluded from participation in, be denied the benefits of, or be subjected to discrimination under any program or activity (or, on the basis of sex, with respect to any education program or activity) receiving Federal financial assistance.
There is no mention of overweight or obesity. Currently, only one state (Michigan) and several localities across the United States (San Francisco and Santa Cruz in California; Washington, DC; Madison, Wisconsin; Urbana, Illinois; and Binghamton, New York) have laws prohibiting weight discrimination, as a protected category within existing civil and human rights statutes. Online surveys conducted in 2011, 2012 and 2013 indicate that there is strong, consistent support for policies prohibiting weight discrimination in the United States (Suh et al., 2014).
Similarly, in Europe, the EU Equal Treatment Directives implements the principle of equal treatment between men and women in EU Labour Law, and in the United Kingdom, the UK Equality Act of 2010 provides an anti-discrimination law protecting workers against discrimination in employment on grounds of religion or belief, sexual orientation and age. The Act requires equal treatment in access to employment as well as private and public services, regardless of the protected characteristics of age, disability, gender assignment, marriage and civil partnership, race, religion or belief, sex and sexual orientation. Once again, there is no mention of overweight and obesity.
Without legislation, there is little prospect that the human tendency to discriminate against and stigmatize overweight and obese people will change. There is an immediate need to develop specific anti-discrimination legislation to protect people with obesity and improve their quality of life.
Devalorizing the thin-ideal
There is an immediate need for legislation to control the prominent use of images representing the thin-ideal. As has been the case with tobacco advertising for many years, governments need to legislate to restrict presentations in the media, both print and electronic, of prominent display on magazine covers and in advertisements of abnormally thin models. In the United States, H.R. 4341, also known as the Truth in Advertising Act, is being considered by Congress. Similar legislation is needed throughout the world. Even under existing employment legislation, the employment of thin models to the exclusion of models with average of large body size should be considered illegal under equal opportunities legislation. If attempts to control the publication of images of thin models in print and electronic media do not succeed, which, to this author, seems highly probable, then legislation will be required to enforce plain covers on fashion magazines.
Reducing the consumption of energy-dense, low-nutrient foods and drinks
It was noted above that an inverse relationship exists between energy density of foods (kilojoules per gram) and their energy cost (dollars per megajoule). In addition, the inverse relationship between affordability and healthfulness helps to explain why the highest rates of obesity and diabetes are found among minorities and the working poor. With these facts in mind, the current situation behoves governments to enact legislation to make F/V intake more affordable and fast processed foods and beverages less desirable.
The imposition of a sugar, fat or salt tax on people who are already hard pressed making healthy food purchases would be unfair and only makes matters worse. What makes more sense is legislation to impose an Unhealthy Commodities Tax (UCT) on producers and suppliers. This tax could be rationally computed based on known contents of all foods and beverages available for sale. For example, for any product, the total weight in grams of saturated fat, trans fat, sugar and salt could be summated to give the total weight for the unhealthy content (UC) using the formula

A list of 10 products hypothetically subjected to UCT is presented in Table 2. For example, a McDonald’s Big Mac containing 10 g of fat, 9 g of sugar and 0.2 g of salt has a total UC of 19.2 g. Charging one penny per gram generates a UCT of 19 pence, 7 per cent of the price of a Big Mac in the United Kingdom. 6
Unhealthy content (UC) of products with associated tax levels using the formula UC = saturated fat + trans fat + sugar + salt (in grams) charged at one pence per gram capped at 10 per cent of current price.

UCT: Unhealthy Commodities Tax.
Trans fat values not included (except for Burger King Double Whopper).
To make the system as fair as possible, UCT should be divided equally between producers and suppliers. In the case of the Big Mac, McDonald’s would pay 3.5 per cent of the sale price, and the retail franchisee would pay 3.5 per cent also. This is a small price to pay for such an unhealthy but popular product. The imposition of UCT would incentivize suppliers to reformulate their products towards the lowest possible levels of fat, sugar and salt. Retailers would be equally incentivized to switch to less unhealthy products. Consumers would be given a healthier set of options to take home to their tables.
In the United Kingdom, with a food and drinks market worth around £100 billion, the revenue from UCT is estimated to be in the range of £5–10 billion. Tax revenues from UCT could be paid directly into two areas: (1) to fund the National Health Service to allay costs of treating patients with obesity and related conditions such as diabetes, metabolic syndrome and cancers; (2) to subsidize the production of organic F/V with payments to growers and sellers to enable lower retail prices of organic F/V.
The use of the tax for these purposes would be a fair use of resources because a share of the profits from sale of unhealthy commodities would contribute proportionately to (1) the resulting health service costs and (2) improving the diet of consumers towards higher F/V intake.
Legislation to introduce UCT would be a significant step towards reducing inequities and the eradication of the obesity gradient.
Improving access to plant-based diets
Boucher et al. (2012) on behalf of the Union of Concerned Scientists argued that a diet shift from beef towards chicken would greatly reduce the pressure on land and the resulting pressure for deforestation. It would also have health benefits, particularly in developed countries where beef consumption is already at levels leading to heart disease, cancer and other illnesses. Other authorities have been recommending a switch to a plant-based diets (e.g. Campbell and Campbell, 2006), a recommendation that is well supported by epidemiological studies. High F/V intake decreases risk of CVD and of certain cancers, mainly of the digestive system, and is inversely linked to body weight and fat mass. In comparison with high sugar and high-fat foods, F/V intake contributes to the prevention of weight gain among overweight individuals (Guillaumie et al., 2010). High F/V intake is associated with better health, especially among those who consume at least five servings per day (Heimendinger et al., 1996; Stables et al., 2002). Some countries such as Canada and Australia have considered increasing the recommended F/V intake to at least seven or eight servings a day. He et al. (2007) reported the finding from a meta-analysis that increased consumption of F/Vs is related to a reduced risk of coronary heart disease (CHD) Compared with individuals who had less than three servings/day of F/Vs, the pooled relative risk of CHD was 0.93 for those with three to five servings/day and 0.83 for those with more than five servings/day. Boeing et al. (2012) reviewed the protective effects of increased F/V intake on a wide range of conditions, which included obesity, type 2 diabetes mellitus, hypertension, CHD, stroke, cancer, chronic inflammatory bowel disease, rheumatoid arthritis, chronic obstructive pulmonary disease, asthma, osteoporosis, eye diseases and dementia. The authors concluded, ‘from a scientific point of view, national campaigns to increase F/V (intake) are justified. The promotion of F/V (intake) by nutrition and health policies is a preferable strategy to decrease the burden of several chronic diseases in Western societies’ (Boeing et al., 2012).
Meats are high in energy and fat, and it is not surprising that meat consumption (MC) is associated with overweight and obesity. Wang and Beydoun (2009) analysed data collected in the 1999–2004 NHANES to test the associations between MC and adiposity measures controlling for potential confounders. Those who consumed more meat had a significantly higher daily total energy intake, for example, those in the upper versus bottom quintiles consumed around 700 more kilocalories per day. Regression models showed consistent dose-related positive associations between MC and BMI, waist circumference, obesity and central obesity.
Reducing the amount of meat in one’s diet can be an effective dietary intervention for overweight or obesity. The most extreme forms of this diet are the vegetarian and vegan diets. Vegetarian diets include eggs and/or dairy but no other foods derived from animal sources. Vegan diets exclude all animal-based foods. In addition to improved health including weight loss, making the switch to a more plant-based diet can be driven by ethical beliefs against animal cruelty and by concerns for the environment. Recent scientific evidence has indicated that a vegetarian diet reduces the risk of most contemporary diseases and that vegetarianism is being increasingly accepted owing to health concerns and ethical, environmental and social issues including the need for a sustainable nutrition.
A meta-analysis with 120,000 participants reported a 29 per cent lowered risk of death from CVD in vegetarians and an 18 per cent lower incidence of cancer (Huang et al., 2014b). Vegetarians also have lower risk of hospitalization or death from ischaemic heart disease (Crowe et al., 2013), lower risk of hypertension (Pettersen et al., 2012; Yokoyama et al., 2013), lower risk of developing multiple sclerosis (MS) (Rizzo et al., 2011) and lower risk of some cancers than meat eaters.
In a systematic review of vegetarian diets and glycaemic control in diabetes, vegetarian diet was associated with a significant reduction in HbA1c (−0.39%) and a non-significant reduction in fasting blood glucose concentration compared with consumption of comparator diets (Yokoyama et al., 2014a). Yokoyama et al. concluded that consumption of a vegetarian diet is associated with improved glycaemic control in type 2 diabetes, suggesting that a plant-based diet can significantly improve blood sugar levels and potentially leave patients free of the disease. Although not compared directly in the analysis, the findings suggest relief from diabetes symptoms with a vegetarian diet is superior to those expected from drug therapy. Other studies showed that vegetarians and fish eaters have a lower risk of cancer compared to meat eaters (Key et al., 2009), lower risk of diverticular disease compared to meat eaters or fish eaters and vegans have an even lower risk (Crowe et al., 2011). Vegetarians, especially vegans, have a lower risk of developing type 2 diabetes (Tonstad et al., 2009, 2013). However, vegans require dietary supplements of vitamin B12, B6, D and iodine. In light of the evidence concerning plant-based diets as a diet of choice for people with overweight or obesity, the ability to change to a vegetarian or vegan diet, and to maintain the change, is a topic of some importance. On current evidence, vegetarian and vegan diets, with increased intake of F/V and reduced or zero, provide a sustainable and effective means for achieving healthful nutrition and a significantly beneficial method of reducing adiposity. For many people, however, the pricing of food requires rebalancing to make a diet of healthy plant-based foods as affordable as a diet that concentrates on meat and dairy.
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is the largest food supplement programme in the United States, serving around 9 million participants each year. Eligibility is based on nutritional need and income. Eligible participants receive five main benefits: (1) Supplemental food cheques or an electronic benefit card is issued to programme participants enabling them to purchase nutritious food at approved stores and the average monthly benefit in 2014 was US$43.26; (2) formula vouchers; (3) nutrition education; (4) access to health care and other social services; and (5) breastfeeding support.
In addition to the above five benefits, a system like the WIC provides an opportunity to improve F/V intake for millions of people. Trials have already shown positive results. Herman et al. (2008) tested the effectiveness of a subsidy for F/Vs to the WIC. Women who enrolled for postpartum services (n = 602) at three sites in Los Angeles were assigned to an intervention (farmers’ market or supermarket, both with redeemable food vouchers) or control condition (a minimal non-food incentive). Interventions were carried out for 6 months, and participants’ diets were followed for an additional 6 months. Participants increased their consumption of F/Vs and sustained the increase 6 months after the intervention. Farmers’ market participants showed an increase of 1.4 servings per 4186 kJ (1000 kcal) of consumed food from baseline to the end of intervention compared with controls, and supermarket participants showed an increase of 0.8 servings per 4186 kJ of consumed food.
In 2009, WIC added a F/V voucher to WIC food packages. Following the changes to the WIC food package, Whaley et al. (2012) found that consumption of whole-grain food increased by 17.3 per cent, a 51 per cent increase over baseline. In addition, caregivers and children who usually consumed whole milk decreased by 15.7 and 19.7 per cent, respectively, a 60–63 per cent reduction over baseline. Small but significant increases in consumption of F/V were also reported. The investigators concluded that the federal policy changes to WIC had the intended effect of increasing consumption of the prescribed food items. In support of this finding, Zenk et al. (2014) used a quasi-experimental design to determine whether F/V prices at WIC vendor stores decreased after the policy revision in seven Illinois counties. Results suggested that the WIC policy revision contributed to reductions in F/V prices. In light of these and other findings, there can be little doubt that adding fresh F/Vs to WIC food packages would result in increased access to F/V consumption. Following the WIC model, legislation should be considered in every state and country to improve F/V intake.
As suggested above, proceeds from the UCT could be used to subsidize the organic production of F/V with payments to growers and sellers to enable lower retail prices of organic F/V. These proposed interventions to increase access and affordability of F/V would help to slow the obesity epidemic.
Summary
Health is regulated by homeostasis, a property of all living things. Homeostasis maintains equilibrium at set-points using feedback loops for optimum functioning of the organism. Long-term imbalances in homeostasis arise through genetic, environmental and biopsychosocial mechanisms causing illness and loss of well-being.
Over-consumption of high-caloric, low-nutrient foods, combined with stressful living and working conditions, has caused loss of equilibrium, overweight and obesity in more than one billion people.
Research on different diets suggests that a plant-based diet containing low amounts of sugar, little or no red meat and the minimum of fats promotes weight loss and prevents obesity, diabetes, metabolic syndrome, CHD and cancer. A vegan diet with no meat, fish or dairy is especially anti-obesogenic.
The ‘thin ideal’ pervades popular culture with narratives and images of thinness. This influence has an entirely negative effect on youth the world over.
Discrimination against people who are overweight or obese causes stress and socioeconomic disadvantage. Approaches to the epidemic that invoke a narrative of ‘blame-and-shame’ exacerbate the problem. There are very few people who deliberately become obese through conscious effort or who would not like to avoid it if they possibly could.
Homeostatic imbalance in obesity includes a ‘COD’, a system of feedback loops linking weight gain, body dissatisfaction, negative affect and over-consumption. This homeostatic CODT is consistent with a large evidence base of cross-sectional and prospective studies.
Governmental actions independent of corporate interests are required at all levels of society to reduce the prevalence of obesity and related diet-based conditions. A four-armed strategy to halt the obesity epidemic consists of (1) putting a stop to victim-blaming, stigma and discrimination; (2) devalorizing the thin-ideal; (3) reducing the consumption of energy-dense, low-nutrient foods and drinks; and (4) improving access to plant-based diets. If fully implemented, the proposed measures would restore homeostasis and halt the obesity epidemic.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.