
Abstract
Background:
Hypnotherapy has been reported as being beneficial in the treatment of irritable bowel syndrome (IBS). We aimed to test the hypothesis that patients with IBS treated ‘holistically’ by hypnosis (i.e. by combined psychological and physiological symptom imagery) would have greater improvement in their IBS symptoms than patients treated by hypnosis using standard ‘gut-directed’ hypnotherapy, and both would be superior to simple relaxation therapy.
Methods:
Patients (n = 51) with Rome II criteria were randomised to ‘individualised’ (holistic) hypnotherapy, standard ‘gut-directed’ hypnotherapy or relaxation therapy for a period of 11 weeks with two follow-up assessments at 2 weeks and at 3 months after the completion of the trial. The primary outcome was bowel symptom severity scale (BSSS).
Results:
All the participants in this study improved their IBS symptoms (pain, bloating, constipation and diarrhoea) and physical functioning at the end of the treatment from baseline, but this was not significantly different across the treatment arms.
Conclusion:
Neither ‘individualised’ nor ‘gut-directed’ hypnotherapy is superior to relaxation therapy in IBS.
Introduction
Modern neuroscience has shown that emotions permeate both mind and body and can affect our susceptibility to stress, cognitive function, and vulnerability to particular psychiatric disorders and illnesses. Emotions can also affect the function of our respiratory, immune, cardiovascular, reproductive, endocrine and gastrointestinal (GI) systems (Davidson, 2013). Research in epigenetics further supports the idea that our beliefs and emotions translate into physiological changes in the body (Church, 2009; Lipton, 2008), and this mind–body connection is apparent in sufferers of irritable bowel syndrome (IBS).
IBS affects approximately 15 per cent of the general population at any one time and is one of the most common disorders encountered by both gastroenterologists and physicians in primary care (Camilleri and Choi, 1997; Farthing, 1995). The disorder typically affects those of working age and imposes an economic burden on the patient through increased health-care costs and loss of income because of illness (Dean et al., 2005). These patients also often experience a decrease in quality of life (Creed et al., 2000).
The aetiology of IBS is as yet unknown, but most researchers agree that a subset of IBS sufferers have visceral hypersensitivity of the gut (Bouchoucha et al., 1999; Camilleri et al., 2001). Other possible mechanisms in predisposed persons that have been proposed include previous infectious gastroenteritis, mast cell infiltration, an imbalance of neurotransmitters including serotonin dysregulation, small intestinal bacterial overgrowth and psychological precipitants including acute life stress and abuse (Gershon, 2004; Gui, 1998; Koloski et al., 2005; Levy et al., 1997; Neal et al., 1997; Pimentel et al., 2000). Hence, IBS is probably a multi-faceted brain–gut disorder resulting in alteration in the regulation of gastrointestinal (GI) motility and/or sensory function (Smith and Morton, 2001; Tortora and Grabowski, 2000). Studies have shown that emotions such as anger, fear, pain and anxiety affect colonic motility more in IBS patients than in healthy controls (Gorard et al., 1996; Welgan et al., 2000), and for IBS, the most frequent co-morbid psychiatric disorders are anxiety, depression and somatoform disorders (Creed, 1992, 1994).
This evidence suggests that the pathophysiology of IBS involves the brain–gut axis (Salt and Neimark, 2002), and ‘gut-directed’ hypnotherapy has been shown to be a successful intervention in breaking abnormal cycles occurring within this axis (Camilleri, 2001; Farhadi et al., 2001). Studies have especially shown the efficacy of hypnosis in the treatment of IBS (Palsson, 1998; Whorwell, 1987, 2006), but these studies only addressed physiological symptoms (‘gut-directed’ hypnotherapy) and did not take into account psychological symptoms such as anxiety and depression which are part of the IBS symptom picture.
The mechanisms responsible for the therapeutic success of hypnotherapy are largely unknown, but research has shown that it may act by modulating visceral sensitivity, motor function and psychological distress (Gruzelier et al., 2001; Houghton et al., 1999; Marchioro et al., 2000). Imagery is a major component of hypnosis, and research has provided numerous examples of the physiological effects imagery has on the body (Graham, 1995). Unlike many other treatment options which separate the mind–body by focusing on either the psychological or the physiological aspects of IBS, hypnotherapy potentially addresses both via the brain–gut axis. However, the application of ‘gut-directed’ hypnosis has not been compared with combined gut and mind–body hypnosis: the latter theoretically might increase the benefit of hypnotherapy as an intervention because psychological distress is so prevalent in patients with IBS (Labus et al., 2007; Park et al., 2008).
We aimed to evaluate the efficacy of hypnosis and imagery in the treatment of IBS. More specifically, we aimed to compare the use of standard ‘gut-related’ imagery used in previous trials which addressed the patients’ physiological problems only (Gonsalkorale et al., 2002; Whorwell, 1987, 2006), with mind–body imagery that reflects the patients’ complete symptom picture (i.e. imagery which addresses both the psychological and physiological aspects of IBS) in a randomised controlled trial.
Method
Study participants
A total of 51 symptomatic volunteers with IBS aged between 17 and 75 years were recruited from medical and naturopathic clinics and were invited to undergo a 1-hour screening session. They were then randomly assigned to one of three groups. Concealed allocation was assured by an assistant placing the names of participants into opaque envelopes and placing them in a locked filing cabinet. A fortnight after the screening session, all three groups began the treatment programme which consisted of five fortnightly treatment sessions (half an hour each) over a period of 9 weeks, with a subsequent follow-up of 2 weeks and 3 months. The flow of patients through the study is summarised in Figure 1.

Flow diagram of subjects’ progress through the phases of the trial.
The Ethics Committee of the University of Sydney approved the trial, and guidelines on patient consent were met.
Inclusion criteria
The participants were deemed suitable for the study after having been diagnosed with IBS by a primary care physician or gastroenterologist. All had to meet the Rome II criteria for IBS (Drossman, 1999; Drossman et al., 2000) (specifically, pain or abdominal discomfort relieved by defecation, and/or onset associated with a change in stool frequency, and/or onset associated with a change in stool form), had failed to respond adequately to conventional medicines, and who had experienced at least 4 days with at least moderate pain over a 2-week period after screening.
Exclusion criteria
Participants who were not free of organic disease (e.g. those who were diagnosed with coeliac disease, inflammatory bowel disease or diverticulitis as well as IBS) and who did not fit the inclusion criteria were excluded. Current medications were not discontinued.
Gastrointestinal screening of study population
During the initial screening session, participants completed the validated Talley Irritable Bowel Symptom Questionnaire (IBSQ) (Talley et al., 1995) to establish diagnosis and exclude other differential diagnoses. They also completed the validated Bowel Symptom Severity Scale (BSSS) (Boyce et al., 2000) to establish the severity of their IBS symptoms.
Interventions
The participants were randomly allocated to one of three groups – two experimental groups (either ‘individualised’ or standard ‘gut-directed’ hypnosis) and one control group (relaxation therapy) – by means of random number tables (Boyer, 1968) and were unaware of which treatment group they were assigned to and of other participants in the trial. Also, consultations for other patients were always interspersed between those for any IBS trial participants to minimise contact between subjects.
At the end of the trial, participants in the control group were offered two complementary sessions in hypnosis. The five treatment sessions were spaced approximately a fortnight apart over a period of 9 weeks. In the first of the five half-hour sessions, the patient’s full history was taken and the functioning of the GI tract was explained. The following procedure was then strictly adhered to for all five sessions of the trial.
‘Individualised’ hypnosis
Hypnosis was induced using a rapid eye catalepsy technique (Elman, 1964) after which the therapist read two prepared scripts – one containing ‘gut-directed’ imagery (physiological symptoms of IBS), plus a further script containing the patient’s individual psychological symptoms as evidenced by the Symptom Checklist 90-R (SCL-90-R) (Derogatis, 1994; Derogatis et al., 1975). At the end of the second session, a CD of the scripts used in this session was given to the patient to be taken home and practised daily.
Standard ‘gut-directed’ hypnosis
Hypnosis was induced (using a rapid eye catalepsy technique), after which the therapist read the same prepared script containing ‘gut-directed’ imagery (physiological symptoms of IBS) as for group one. No script containing the patient’s psychological symptoms was read. At the end of the second session, a CD of the ‘gut-directed’ imagery script was given to the patient to be taken home and practised daily.
Relaxation therapy
No hypnosis was induced. The therapist read a prepared script of a progressive relaxation exercise that contained neither the aforementioned ‘gut-directed’ imagery nor the patient’s individual psychological symptoms. At the end of the second session, a CD of the relaxation exercise was given to the patient to be taken home and practised daily.
Compliance for home practice was checked by the therapist at each treatment session and was also evidenced by the participants’ responses to Question 6 of the Bowel Symptom Scale 3 (BSS3) and Question 7 of the Bowel Symptom Scale 4 (BSS4).
Follow-up
The Bowel Symptom Severity Scale (BSSS) (Boyce et al., 2000) and the SF-36 Health Survey (Stewart et al., 1988) were completed by each participant, at 2 weeks and again at 3 months after completion of the 9-week treatment period, to assess whether IBS symptoms had significantly changed compared with baseline. No further treatment was given during the follow-up period, nor were participants invited to return for further treatment if symptoms returned.
Instruments
Irritable Bowel Symptom Questionnaire (IBSQ)
A modified validated version of the previously validated Talley BSQ (Talley et al., 1995) was utilised in order to verify the diagnosis of IBS and to acquire general data on patients participating in the trial. The BSQ addressed aspects such as pain/discomfort, bloating, frequency and type of bowel movement, urgency, and frequency of visits to a doctor or alternative therapist.
Bowel Symptom Scales (BSS1-5)
The BSS (Boyce et al., 2003) were used to assess change in IBS symptoms during the course of the five treatment sessions. The first item of all five BSSs consists of five visual analogue scales which refer to each of the principal symptoms of IBS (pain/discomfort, bloating, constipation and diarrhoea), plus an overall symptom severity rating. All five of the BSS also assess stool form and the degree to which IBS symptoms interfered with the patient’s life and activities (see Tables 2a to 2d and Figure 2).

Bowel Symptom Scales (BSS1-5) – overall symptom severity by treatment groups and control group.
Bowel Symptom Severity Scale (BSSS)
The BSSS (Boyce et al., 2000) consists of eight questions relating to possible symptoms the patient may have endured in the 2 weeks between treatment sessions. The symptoms specific in this questionnaire enquire about stool formation, abdominal pain, frequency of bowel motions, bloating, urgency, inability to have a bowel motion and a general feeling of discomfort in the abdomen. Each question also has two sub-questions which asked how distressed the patient had been during this period and how much the specific symptoms had interfered with his or her daily life. Each of the symptoms is given a severity rating between 0 and 4, a higher rating being indicative of greater severity.
Symptom Checklist 90-R (SCL-90-R)
The SCL-90-R (Derogatis, 1994; Derogatis et al., 1975) helps to evaluate a broad range of psychological problems and symptoms of psychopathology and is also useful in measuring the patients’ progress or treatment outcomes. It provides an overview of the patients’ symptoms and their intensity.
The questionnaire consists of 90 items which measure nine primary symptom dimensions: somatisation, obsessive-compulsive disorder, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation and psychoticism. For the purpose of this trial, four of the nine primary symptom dimensions (anxiety, depression, interpersonal sensitivity and obsessive-compulsive disorder) which reflected the psychological symptoms ofthe majority of the participants were measured a priori. Those participants in the ‘individualised’ hypnosis group who scored 10 or higher on any of the four scales were read specific scripts pertaining to their disorder during the treatment sessions.
Short Form General Health Survey (SF-36)
The SF-36 General Health Survey (McHorney et al., 1994) has been applied widely to clinical trials and is capable of discriminating between healthy participants and those with moderate levels of psychiatric illness (Russo et al., 1998). The SF-36 is a 36-item questionnaire consisting of eight health concepts or sub-scales broadly related to quality of life, mental health and social activities.
The sensitivity of the SF-36 to change in health status of IBS patients was tested by examining changes in SF-36 sub-scale scores throughout the treatment period and as follow-up 2 weeks and 3 months after the completion of the trial.
Duke-UNC Functional Social Support Questionnaire
The eight-item Duke-UNC Questionnaire (Broadhead et al., 1988) was completed by the participants at the screening session to assess the amount of support patients had and to what extent it influenced their health and well-being. The questionnaire contains questions in two content areas: confident social support, which reflects a confidant relationship where important matters in life such as social contact and personal/work/financial problems are discussed and shared; and affective support, which reflects a more emotional form of support and caring.
Survey of Recent Life Experiences (SRLE)
Emotional responses to life stress can influence GI function via the brain–gut axis and produce symptoms such as pain and altered bowel function (Lundberg, 2005; Mayer, 2000). The SRLE (Kohn and MacDonald, 1992) which consists of 51 items covering six concepts (social and cultural difficulties, work, time pressure, finances, social acceptability and social victimisation) was completed by the participants at the screening session to determine whether these stresses had had an influence on their IBS symptoms.
Credibility Scale
The Credibility Scale (Borkovec and Nau, 1972) was issued to participants on two occasions throughout the trial (session 2 and session 4) to assess the credibility of treatment as perceived by the participants and to test the success of blinding.
The four-item assessment contains questions on how confident the patients are in the treatment they are receiving, how confident they are in recommending the treatment to a friend suffering a similar complaint, how logical the treatment seems to them and how successful they think this form of treatment would be in alleviating other complaints.
Statistical analysis
For the primary endpoint (BSS), an intention to treat analysis of variance was used to determine the differences among groups at baseline, end of treatment, and follow-up and repeated measures for trend over time were also determined. All p values were two-tailed, unless otherwise indicated, and the alpha level of significance was set at 0.05. Missing scale and item scores were not replaced. Data for all other outcome measures (psychological stress (SRLE)), quality of life (SF-36) and social support (Duke-UNC) are presented as per protocol analysis.
It was hypothesised a priori that, with respect to the abdominal pain sub-scale of the SCL-90-R, the control group would not change on average, the standard therapy group would improve by one point and the individualised therapy group by two points. Under these conditions and with an assumed standard deviation (SD) = 2.0, n = 25 participants per study group would have yielded statistical power >0.85 at the 0.05 (two-tailed) level of statistical significance. Due to difficulty with recruitment, n = 17 participants were actually recruited per group, and this yields statistical power of approximately 0.72 under the same conditions. While this power is less than the desired 0.8, it is unlikely to have materially affected the statistical analysis.
Results
Baseline characteristics
At baseline, the 51 participants in this study were similar across treatment areas (Table 1). All participants presented with psychological problems. Of these, 30 participants presented with depression, 4 with anxiety, 2 with obsessive-compulsive disorder and 1 with interpersonal sensitivity. Of the remainder, 5 had both depression and anxiety, 5 had depression and obsessive-compulsive disorder, and 4 presented with depression and interpersonal sensitivity.
Demographic and baseline data for subjects randomised to the three treatment groups.
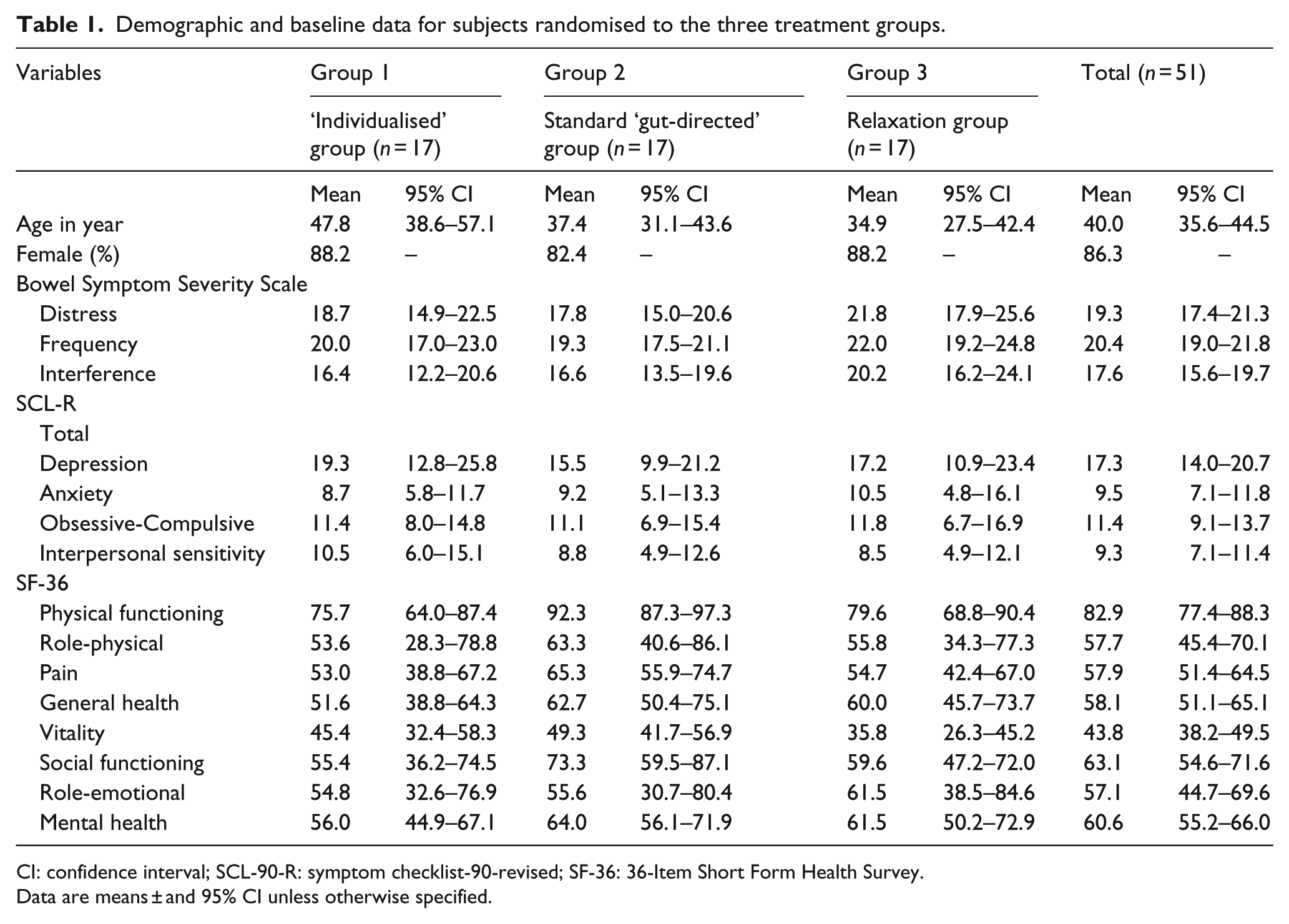
CI: confidence interval; SCL-90-R: symptom checklist-90-revised; SF-36: 36-Item Short Form Health Survey.
Data are means ± and 95% CI unless otherwise specified.
At the commencement of the trial period, the majority of participants (81.6%) suffered abdominal pain most of the time (of these, 59.2% had mild to moderate pain and 40.8% had severe to very severe pain) with 61.2% of participants experiencing pain several times a week or daily. In the 3 months prior to treatment, 98.0% of participants experienced bloating and 78.4% of participants had visible abdominal swelling. Of the 51 participants, 51% werediarrhoea predominant, 44.9% constipation predominant, and 4.1% had mixed diarrhoea and constipation. The majority of participants in this study were women (86.3%), and the majority of sufferers were aged between 20 and 40 years (82.3%).
Three participants withdrew from the trial (one each in sessions 1, 2 and 4), and six subjects were excluded from the analysis at the end of the trial due to incomplete or missing records.
Response to intervention
All participants demonstrated improvement in the overall severity of their individual symptoms and functioning at the end of the treatment period (Session 5), with the ‘individualised’ group (group one) having a numerically better outcome than the other two groups (Tables 2a to 2d). The overall symptom score was not significantly different at Session 5, and improvement in IBS symptoms (Figure 3) and general health outcomes (Figure 4) did not continue during the 3-month follow-up period.
Bowel Symptom Scales (BSS1-5) – abdominal pain: mean scores and SD at each session from randomisation.

SD: standard deviation; NS: not significant; F1: main effect; F2: linear trend; F3: treatment effect; SF-36: 36-Item Short Form Health Survey.
p < 0.01 and *p < 0.05.
Bowel Symptom Scales (BSS1-5) – bloating: mean scores and SD at each session from randomisation.

SD: standard deviation; NS: not significant; F1 = main effect; F2 = linear trend; F3 = treatment effect.
p < 0.01 and *p < 0.05.
Bowel Symptom Scales (BSS1-5) – constipation: mean scores and SD at each session from randomisation.

SD: standard deviation; NS: not significant; F1: main effect; F2: linear trend; F3: treatment effect.
p < 0.01 and *p < 0.05.
Bowel Symptom Scales (BSS1-5) – diarrhoea: mean scores and SD at each session from randomisation.

SD: standard deviation; F1: main effect; F2: linear trend; F3: treatment effect.
p < 0.01 and *p < 0.05.

Bowel Symptom Severity Outcome – treatment sessions and follow-up – by treatment groups and control groups.

Secondary Health Outcome SF-36 – treatment sessions and follow-up – by treatment groups and control group.
Psychological stress
The bowel symptom severity measures (BSSS) specific to frequency of bowel motions, distress and interference with daily life at the end of treatment sessions, and the SCL-90-R measures, depression, obsessive-compulsive and interpersonal sensitivity at baseline, were significantly correlated (p < .01), but anxiety was unrelated. At the end of treatment sessions, the overall severity of IBS (BSSS) was significantly correlated (p < .05) with all SCL-90-R scores except anxiety (Table 3).
Intercorrelations among four dimensions of the SCL-90-R at baseline and the SF-36 health concepts at the end of treatment.

Social support
At baseline, the confident social support score (Duke-UNC) was negatively correlated with bowel symptom severity scores and with all psychological scores (as per the SCL-90-R) except depression. The correlation between the confident support score and depression was significant (p < .05) (Table 3).
Quality of life
Participants in all three groups demonstrated an improvement in overall severity in their IBS symptoms and a subsequent improvement in their quality of life. There was a highly significant decrease in the level of pain, and also a highly significant improvement in the patients’ vitality, social functioning and mental health. There was also significant improvement in physical functioning, general health and the extent to which emotional problems interfered with their work or daily activities from baseline (Figure 4). However, there was no significant treatment effect (Table 4).
Medical Outcomes Index Mean Changes Over Time: Tests of Within-Subjects Effects, Linear Trend, and Treatment Effect.

p<0.01, *p<0.05.
Credibility Scale
The participants in all three groups showed that their expectancy for improvement increased from the commencement of their treatment to the end of treatment, although the results did not show statistically significant differences among the three treatment groups (Figure 5).

Credibility Scale: mean scores between Session 2 and Session 4 by treatment groups and control group.
Discussion
The study follows on previous research which has shown ‘gut-directed’ hypnotherapy to be of benefit to patients with IBS (Gonsalkorale et al., 2002; Whorwell, 1987, 2006). The study tested both physiological and specific psychological imagery in the hypnotherapy scripts and compared this technique to standard ‘gut-directed’ hypnotherapy. Psychological distress, which can trigger or exacerbate symptoms (Jarrett et al., 1998; Koloski et al., 2003), has been shown to be an important component of IBS symptoms and probably should be considered when treatment strategies are designed. To our knowledge, studies on hypnotherapy as a treatment for IBS have not taken this into account (Anbar, 2001; Forbes et al., 2000; Gonsalkorale et al., 2002; Harvey et al., 1989; Palsson, 1998; Whorwell, 1987). By using scripts that specifically target each individual patient’s emotional/psychological symptoms (in conjunction with scripts for the physiological aspects of the disease), the therapist in this trial attempted to address the whole patient profile.
Based on previous research and consistent with the aims of this study, the present research sought to empirically investigate three main hypotheses.
The first hypothesis was that participants who had been diagnosed with IBS would present with not only physiological symptoms but psychological ones as well and, that at the end of the study, participants who underwent ‘individualised’ hypnotherapy (using imagery which addressed both the psychological/emotional aspects and the physiological symptoms of the syndrome) would have a better outcome in the improvement in their IBS symptoms than participants who underwent standard ‘gut-directed’ hypnotherapy in which physiological symptoms alone were treated. In this study, participants presented with high baseline scores on psychological ratings. However, while all groups improved from baseline on multiple measures, there was no overall benefit detected for hypnotherapy over relaxation therapy.
The second hypothesis we tested was that participants’ IBS symptoms would improve during the trial period, and, as a result, their quality of life would subsequently improve. Quality of life did improve in all treatment arms but, again, we detected no differential effect of hypnotherapy.
The third hypothesis was that participants who had a support system in place would improve more quickly than those who had not. We found that there was no significant correlation between support and improvement in the overall severity of IBS symptoms. The only significant correlation found was between the confident support score and the depression score.
This study had several strengths. The study was randomised and concealed allocation was assured by an assistant placing the names of participants into opaque envelopes and placing them in a locked filing cabinet. IBS and the functioning of the GI tract were explained. Careful attention was given to blinding throughout the trial, and the therapist (the principle author) who administered the therapy was an experienced and qualified hypnotherapist. Other strengths of this study lie in the fact that participants were recruited prospectively; participants with other pre-existing functional GI diseases were carefully excluded; and both validated, standardised questionnaires to define the outcome measure of IBS and strict criteria for diagnosing IBS were utilised. Also, the drop-out rate during the trial was small.
There were also limitations in this study. It may not have been sufficiently powered. Due to time limits and the fact that the therapist was the only person recruiting, the sample size was modest. A much larger sample size would have been required to detect such a small effect size difference among the groups, but such a difference would possibly still not have been clinically significant.
Another potential limitation was an absence of contact with participants by the therapist during the follow-up period. In previous trials in hypnotherapy (Gonsalkorale et al., 2002; Whorwell, 1987, 2006), participants continued to receive hypnotherapy sessions on a monthly basis during the follow-up period and were asked to telephone if they experienced a relapse so that a further session of hypnotherapy could be arranged. In this study, there was no further contact with the therapist by the participants, adherence to protocols during the follow-up period was not checked and participants were not given further hypnotherapy sessions (either on a regular basis or in case of relapse) to maintain remission. This could be a possible explanation for the lack of improvement in IBS symptoms during the follow-up period. With continued checking of adherence to autohypnosis practice and ongoing hypnotherapy sessions with the therapist, improvement in scores may have increased but, in the authors’ view, to do so would not have addressed if any benefit persisted.
Research has indicated that EEG wave changes associated with hypnosis can also be triggered by other methods of deep concentration, such as the relaxation response (Jacobs and Friedman, 2004; Williams and Gruzelier, 2001). Previous trials on relaxation training as a treatment for IBS, however, have shown mixed results (Blanchard et al., 1993; Boyce et al., 2003; Spiller, 2005; Van der Veek et al., 2007).
Nevertheless, the control group in the trial underwent sessions in relaxation as a treatment for their IBS symptoms, whereas treatment for the other two experimental groups involved sessions in hypnotherapy. Considering that the relaxation response can trigger brain wave changes associated with hypnosis and that hypnotherapy sessions, themselves, involve deep relaxation, participants in the control group could have easily lapsed into hypnosis. This could account for the similarities in treatment outcome and the small effect difference between the groups.
Notwithstanding the limitations of this clinical trial and that the findings need further confirmation, this study appears to support a psycho-physiological hypothesis that successful treatment of the psychological aspect is accompanied by improvement in IBS symptoms. Future research needs to continue the investigation of the brain–gut axis in IBS and the role of hypnotherapy which addresses both the psychological and physiological aspects of this disorder, as an effective and viable treatment option.
In conclusion, in a randomised, controlled trial of hypnotherapy in IBS, symptoms (pain, bloating, constipation and diarrhoea) and physical functions improved from baseline in each arm. Hypnotherapy, however, was not shown to be superior to relaxation therapy for symptom reduction in this disorder. A possible explanation for this could be that the relaxation response is also associated with hypnosis and participants in the control group could have lapsed into a trance state. This also suggests that reducing anxiety through relaxation may be the key to reducing IBS symptoms in patients, whatever the mechanism may be.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not for profit sectors.