
Abstract
Background:
Kidney transplantation, a life-saving therapy for children with kidney disease, remains challenging to navigate for patients and families.
Objective:
To elucidate the experiences and educational needs of patients who have received a kidney transplant and their caregivers.
Design:
Qualitative descriptive study.
Setting:
One province in Canada (Saskatchewan)
Patients:
Patients who received a pediatric kidney transplant, transplant recipients and caregivers.
Methods:
Semi-structured interviews were conducted via video or by phone and recorded and transcribed verbatim in this qualitative descriptive study. Qualitative content analysis was used to analyze the data. Decontextualization involved an inductive approach, whereby the text was coded and organized into categories and subcategories. Dedoose® software was used to facilitate this process.
Results:
Twenty-three individuals participated, including 13 caregivers (aging in range from 20’s to 60’s) and 10 patients who had previously received a transplant (aging in range from adolescents to 40’s). Three categories emerged from their experiences: (1) the impact of the transplant on the individual (subcategories social, mental health, physical, lifestyle, returning to normal and new life perspective); (2) transplant expectations (transplant as a cure, unexpected experiences); and (3) the need for support throughout the transplant process (practical support, mental health support, healthcare support, support through shared-lived experiences, and challenges related to finding a community). Regarding education, participants identified the need for personalized, age-appropriate education delivered in digestible formats, with clear expectations, timely reinforcement, and emotional support tailored to both patients and caregivers.
Limitations:
Participants were recruited from a single small center in Canada. Patient participants had received their transplant at least 5 years prior to participation in the study and were reflecting on their past experiences.
Conclusion:
Feeling prepared for the transplant journey impacts the transplant experience and kidney transplant education can facilitate care and clarify expectations. The insights gathered from the study will help inform the development of educational resources for patients and caregivers.
Introduction
Kidney transplantation is considered the treatment of choice for children with kidney disease, 1 but it can be extremely challenging for patients and caregivers. Families must navigate new and complex medical information throughout the transplant journey. Knowledge of the transplant process and what to expect before, during, and after the transplant, increases the likelihood of a successful transplant experience. 2 Ideally, information is tailored to the patient’s and family’s level of medical literacy to optimize understanding. After transplant, patients must strictly adhere to a complex regimen of immunosuppressant medications, which expose the patient to new risks such as infections and malignancy. Understanding the timing, administration, and ongoing titration of transplant medications is critical for success.3,4 A lifelong commitment to lifestyle changes (e.g. hygiene practices and infection prevention) and new monitoring practices (e.g. routine bloodwork, medical appointments, and follow-up with the transplant team) is required. For pediatric patients, family caregivers provide much of this support and, in most circumstances, are required to attend appointments throughout the transplant journey until the child transitions into adulthood. Pediatric kidney transplantation is performed in specialized centers, adding complexity for families who must travel to obtain care. In our own institution (Saskatchewan, Canada), patients and caregivers are required to travel out of province for transplant surgery. Families relocate for 6 to 8 weeks until the recipient is stable enough to return to Saskatchewan and resume care at home. Previous work with caregivers of adult lung transplant recipients identified additional psychological, emotional, logistical, and financial burdens associated with traveling away from home for transplantation 5 and stimulated the development of new resources to improve pre-transplant education for this population. 6 Educational needs in the context of pediatric kidney transplantation are unknown and deserve to be explored.
Given the importance of transplant education, there is a surprising lack of research in this area. We conducted a scoping review to summarize existing literature and identified only 18 articles evaluating patient-focused educational interventions. 7 In a secondary objective to describe the educational experiences and needs of patients and caregivers, participants indicated that the transplant process was stressful or overwhelming (n = 6/9 studies). They indicated that social supports and education helped them cope with the stress of transplant,8-13 highlighting the importance of transplant education. Throughout these reports, participants consistently wanted more information than they received. 7 Notably, only 5 studies pertained to kidney transplant populations,8,9,12,14,15 and all except one report 9 were at least a decade old. Moreover, all kidney transplant qualitative studies, except two,12,14 excluded patients, instead focusing exclusively on caregiver experience.
The purpose of this study was to conduct an exploration of the educational needs during the pediatric process by interviewing patients who have received a kidney transplant as a child as well as with caregivers. Our objectives were to characterize the transplant experiences of the participants and to learn about their educational requirements before and after a pediatric kidney transplant.
Methods
Study Population and Recruitment
The study was approved by the Behavioural Ethics Review Board at the University of Saskatchewan (Beh#3511). The participants were patients who had received a kidney transplant as a child and caregivers in one province in Canada. Such patients were identified through the pediatric kidney transplant program (patients and caregivers) and adult kidney transplant program (patients who were transplanted as children but have since transitioned to the adult program for follow-up care). Prospective participants were approached by their regular healthcare provider to determine initial interest, and for potential patients under the age of 18, the caregiver was informed about the study prior to a conversation with the child. Potential participants were told that participation was completely optional, and their care would not be affected either way. Those expressing support were contacted by the research team. Pediatric patients and caregivers were offered the opportunity to participate jointly or individually. All participants then received a detailed study information package and were scheduled for a recorded telephone or video interview at least 48 hours after informed consent/assent was provided. To preserve patient confidentiality, the care team was not informed of their study participation status.
Data Collection
The questions and interview approach were designed by the research team in collaboration with a patient partner after an extensive review of the literature on pediatric transplant education. 7 The final version included questions designed to explore their lived experiences, determine which information was perceived to be important throughout the stages of the transplant process, 12 assess satisfaction with their educational experience, and tabulate suggested resources/supports for improvement (Supplementary Appendix A). Trained interviewers (i.e., a pharmacy student and a research associate with an MSc, both female) who were not known to the participants conducted the visits (BG and AB). Participants were told the rational for the study and the questions were asked one at a time until all open-ended questions were answered or until the participant chose to end the interview, whichever came first. Interviews were audio-recorded, and field notes were taken during the interview. To ensure transparency, participants were invited to review and edit their transcripts prior to analysis. All participants received $75 CAD or equivalent for their participation in this study.
Data Analysis
Data was categorized by members of the research team (BG, AB, and HM) through qualitative content analysis 16 to minimize abstraction and preserve participant input. The deidentified transcripts were divided among the group, and one reviewer led the first-pass analysis of each interview. Dedoose® (version 9.0.78) qualitative software was used to facilitate the process. Decontextualization involved an inductive approach, whereby one reviewer analyzed the transcripts line by line. Meaning units were labeled with codes, which were further organized according to categories and subcategories. Descriptive analysis occurred at the manifest level with low abstraction and low interpretation, 17 and the process was iterative. Group members reviewed the coding completed by each other and then met periodically to provide suggestions for category relabeling and refinement and come to consensus before proceeding with the next set of transcripts. After the coding was completed and the research team had achieved consensus on the categories, two researchers (HM and MR) drafted the results. The results were presented according to patient and caregiver subgroups. The decision was made to combine “adults who had been transplant as children” and “adolescents” into a single subgroup of patients since all patient participants had been transplanted at least 5 years ago (and in most cases more than 10) and to protect the anonymity of the three adolescents.
Several practices were used to establish trustworthiness of the data. 18 An iterative process involving multiple coders and internal debriefing sessions was used to maintain credibility and confirmability. Participants were also provided with the opportunity to review and discuss the final manuscript prior to publication, and a patient and family advisor provided guidance throughout the research process. Supplementary quote tables from multiple patients and caregivers are included for each category to support transferability. To ensure dependability, we maintained a documented audit trail and shared research folders (which included iterations of the interview guide, notes from the interviews, team meetings and analytical process) and reported our results according to the Consolidated Criteria for Reporting Qualitative Research (COREQ). 19
Results
Participants
Thirteen caregivers (including parents, a grandparent, and one spouse of a former pediatric patient who was not present during the pediatric transplant, aged 20’s to 60’s) and 10 patients who had previously received a kidney transplant participated in a one-time interview. Patients ranged from 13 to 42 years of age; however, all patients started their transplant process and received pre-transplant education before adulthood. All patient participants had received their transplant at least 5 years prior to participating in the study, while most caregivers (61%) had more recent transplant experience (less than 4 years post-transplant). Ninety percent (n = 21) of the participants identified as Caucasian. Demographic data are displayed in Table 1. The interviews ranged from 45 to 81 minutes; the average interview length was 61 minutes. A total of 16 interviews were conducted: 9 individual and 7 joint interviews. One interview was conducted by email as the participant requested accommodation. All interviews with adolescent participants (those aged 10-19) were conducted jointly with their caregivers.
Self-Reported Characteristics of Study Participants (n = 23).

Percentage will not add up to 100 since some participants stated more than one answer.
Not all patients were an eligible age to attend.
Objective 1. Exploring Transplant Experiences
Three overarching content categories were identified in the transcripts, including (1) transplant impacts (subcategories social, mental health, physical, lifestyle, returning to normal and new life perspective); (2) transplant expectations (transplant as a cure and unexpected experiences); and (3) the need for support throughout the transplant process (subcategories practical support, mental health support, healthcare support, support through shared-lived experience and challenges related to finding a community). (Figure 1). The categories are described in the following section, with additional supporting quotes available in Tables 2-4.

Overview of categories and subcategories pertaining to patient and caregiver transplant experiences.
Transplant Impacts: Additional Supporting Quotes.

Transplant Expectations: Additional Supporting Quotes.

Need for Support Additional Quotations.

Category 1: Transplant Impacts
Social
Transplantation profoundly impacted the entire family. Both patients and caregivers described a pervasive feeling of social isolation. In the words of one patient (transcript 18), “. . . you feel like kind of an exception. You feel like you’re a little bit different than other kids.” Caregivers strived to maintain a sense of normalcy but were often challenged by the logistics of caring for a sick child. For example, one said (transcript 2),
“My mom had to essentially just stop working so that she could be with me. And he [my Dad] would have to do weekend trips. . . we lived in the Ronald McDonald House in Edmonton and so I didn’t really have a sense of home for a while.”
The impact on siblings was also noted. According to one caregiver (transcript 15), “The other kids—children are so resilient. They need little crowns as well, her brother and sister, because they were so accepting. . .They never once resented her [the transplant recipient].”
Children undergoing the transplant process often struggled with fitting in with their peers and readjusting socially after the transplant. One patient (transcript 1) said: “I basically lost a year of school, year and a half maybe? I did not get to graduate with my friends. It’s a tough social reintegration almost. People sometimes don’t know how to treat you when you come back.” Lifestyle restrictions often caused a sense of “missing out” For example, a caregiver from transcript 21 explained,
“She’s kind of missed out on that team sport togetherness and having friends in that type of thing. Like she only has friends at school, and she’s never got to experience a team gathering, so maybe that was hard on her.”
Mental health
Mental health impacts were common as well. From a caregiver perspective, many aspects of the transplant process were described as stressful, including approaching a relative about organ donation, fearing that they personally wouldn’t be eligible to donate their kidney, guilt for having a sick child, and post-transplant concern for their child’s health, even when it was stable. One caregiver (transcript 15) said, “I’m always thinking the worst. What if she injures that kidney? She only has one and her daddy can’t give her his other one.”
Mental health struggles were described by both patients and caregivers. One caregiver said (transcript 10),
“[Patient] entered into a state of depression and self-loathing. . .And I didn’t picture that that would come, but he has had a lot in his life to challenge him. So, of course he got run down. He looks at his body after he’s had prednisone infusions and he’s puffed up and he gets zits, and it feels ugly and I just don’t like that he saw himself that way. . .So, I would say the psychology side of things is one that I wasn’t prepared for.”
A sense of resilience was also described. According to a caregiver from transcript 6, “Well, I think it kind of made us very strong. It made us feel that we can go through tough times. Sometimes you have to actually go through things to see what you’re capable of doing.”
Physical
Participants described the remarkable physical impacts from the kidney transplant, including a return of energy, appetite, and overall health. Caregiver from transcript 10:
“He got an appetite for the first time in his life. I think it was three days post-transplant and he sat himself up in bed and reached for a grilled cheese sandwich. That was astounding. His cheeks and his feet turned from yellow to pink.”
Adverse effects from the procedure and medications were also described, such as pain, cancer, diabetes, peripheral edema, acne, and weight gain.
Lifestyle
The need to remain adherent to a strict regimen of post-transplant medications, follow-up appointments, bloodwork, and limitations on physical activities (e.g., sports) were perceived to impact patient and caregiver lifestyles. Patient from transcript 18 said: “Being as I was a recent transplant recipient, contact sports were something they wanted me to avoid. I guess I still did sports but not really high contact sports.”
Return to normal
Many participants remarked on how receiving a transplant had allowed the patient and family to return to normal. Transcript 21:
“They always give you the worst possible outcome, and of course that’s what you focus on. . .We had a couple times where his body didn’t want to cooperate, so we had some setbacks, but for the most part we had all adjusted really well and once he was ready to come home after the transplant, he was just a normal five-year-old kid.”
New life perspective
Some patients and caregivers described how transplantation had changed their life. For example, one patient (transcript 1) mused:
“I was kind of your nerdy, average kid. . .It’s life changing, obviously, from a health side but from a spiritual and mental side. It reminds you of what’s important and focuses you. It kind of gives you a life goal. . .I technically should not be here. It’s just by happenstance that I had the appointment with the doctor, it’s just by happenstance that we discovered end stage renal disease; the chips all kind of fell in the right spot.”
Category 2: Transplant Expectations
Two subcategories emerged around the central category of “transplant expectations.”
Transplant as a cure
Some patients and caregivers embarked on their journey believing that receiving a new kidney would cure all ailments and life would go back to normal post-transplant. It was disappointing for them to learn that kidney transplant is another form of kidney replacement therapy, but not a cure for their kidney disease. For example, a caregiver from transcript 15 said,
“I just thought, once this transplant is over, it’s over. This rollercoaster will be over and we’re going to have our precious little baby and everything’s going to be so good. It really wasn’t that easy. . . It’s like, will it ever get better?”
Unexpected experiences in the transplant process
Many aspects of the transplant process were unexpected. Some caregivers were unprepared for wait times, numerous hospital visits required during pre-transplant evaluation and the reality of post-transplant care. Transcript 11:
“You need to come back once a month for appointments or once every couple of weeks, or now there’s blood work once a week, once a month, however many times they tell us to do it. I don’t remember them ever telling us about all that stuff.”
Some spoke of surprising aspects of the surgery, such as the length of the procedure, or what post-operative care consisted of. Transcript 21: “I don’t think they really told us about all the tubes that would be in and out of [patient], so it was a shock to see him in the ICU as he was waking up.” Participants also described feeling unprepared for post-transplant side effects, associated co-morbidities and complications, such as diabetes, hypertension, infections or the emotional impact of the transplant process. For example, a caregiver from transcript 10 said, “So, I would say the psychology side of things is one thing that I wasn’t prepared for.” A patient (transcript 2) recalled, “Three weeks before graduating, I had to get a biopsy. And that just created this shitstorm essentially of, ‘This is totally scary, and I don’t know what all these things mean.’”
Category 3: Need for Support
Given the significant social, mental, physical, and lifestyle impacts of transplant, the need for support was a common theme.
Practical support
For families traveling out of province for a transplant, the initial 6 weeks post-transplant meant a complete separation from their daily routines. Participants described how support networks allowed them to focus on the transplant, while alleviating the demands of daily tasks. One caregiver (transcript 6) said (in reference to the other caregiver), “He had somebody doing that job for him, and he didn’t have to worry about work at all—which I’m sure many people don’t have that privilege, but that’s very important.” The financial burden of living away from home for an extended period is considerable. Multiple participants expressed appreciation to their transplant team in making available financial aid resources part of the transplant planning, as well as appreciation for the direct financial support provided by non-profit agencies. Practical support was especially important for caregivers.
Mental health support
Many participants valued the mental health support they received through the transplant process. This support came from formal referral to mental health professionals and from informal personal connections. Participants described that their social networks provided essential daily encouragement through the challenges they faced. Transcript 15: “If you’re having a bad day, you could reach out to them and say, ‘I’m feeling discouraged today or I’m feeling tired.’ I think that would be so important. . .sometimes one just needs a little bit of moral support.”
Healthcare support
Many participants expressed their appreciation for the support of their healthcare team. Families perceived this support in the information and explanations they received. Transcript 9:
“It was all so well explained, especially when it came to the surgery. The surgeon himself that did it, he came back several times and if he would see that we were uncomfortable, he would just ask us or tell us more.”
Another demonstration of support was the availability of the healthcare team to answer questions. Transcript 15:
“I’m a firm believer, if you’re concerned, then you need to reach out. Even if it’s to have them give you reassurance. They were always there and they would tell [primary caregiver] what to do. Like, “Try this or try that.” And the phone was always open.”
Transcript 14: “We have so much support there, they’ve always had anything we need or want to discuss.”
Patients described that the contact with their healthcare team alleviated their concerns and allowed them the freedom to enjoy life post-transplant. Transcript 2: “This. . .doctor was like, ‘What’s something you’ve always wanted?’ That was actually how he put it and I was like, ‘I want to get my ears pierced.’ He’s like, ‘Ok, let’s get your ears pierced.’ And yeah, you think about when you’re told no so many times and then this person who’s now your doctor says yes.”
Participants expressed the value they found when their healthcare team was working with them toward shared goals. Transcript 10: “When you ask educated questions you can become part of the team and working as a team for the good of the patient is terrific. The best, it’s the most constructive thing you can do.”
Support from shared-lived experience
Participants who made a strong connection with someone who had been through the transplant process found this to be a valuable support. Transcript 6: “We actually had a friend that was. . .ahead of us all the time with her process so that was a big bonus for us. It was kind of an answer to the prayer, so we knew. . .what to expect.” These connections were made both organically during the time patients were at the hospital for care, and when patients specifically sought out this kind of support. Transcript 3:
“I almost feel like being on dialysis has helped me little because also you meet a lot of people on dialysis that have either had a transplant already or you would meet nurses that had seen people before and after, so there was a lot of different areas to gain information from and different perspectives.”
Finding a community
Communities may be large or small, and looked different for each participant. Both patients and caregivers described the support they felt from being part of a community that embraced them. For one caregiver, this community was the town in which they live. Transcript 15: “The whole community cheers for her, the whole community is so proud now that they see her out and about.” For one patient, the community was their classroom at school. Transcript 20: “I had some really supportive friends in elementary school. I would get large doses of prednisone before I went on dialysis, and I had a friend who would come with me.” Some communities formed during the transplant process. As one patient described (Transcript 21):
“I was staying at the [House] for a long time, so I met some friends. . .I have a lot of memories there, just playing around with kids that were kinda like me. It was very nice. I’d definitely say it was pretty helpful. I got out of my comfort zone and know that I’m not alone in this.”
Challenges with support
Despite the necessity of a support network, for some participants, even this was not without challenges. Many described the importance of confirming a support network prior to transplant, but some felt unable to reach out and ask for support. Transcript 15: “Maybe we should have. . .explained more to other family members. We could have had other family members want to be part of [patient]’s circle; part of her team. That would have helped.” Keeping a support network informed often came with the burden of information-sharing. Transplant 11: “We actually kept a journal and just posted in on Facebook. . .so everybody could see the updates and everything. We didn’t have to tell everybody twenty different times.” These challenges perpetuated the feeling of social isolation through transplant. Transcript 10: “Nurses felt like friends, and they were for a while. They were great. But I really did feel quite alone.”
Several participants described how they were able to rely on their support networks to meet care requirements. Transcript 14:
“There’s that planning involved in. . .how as a family you can make sure that your appointments are covered. If you and your husband are full-time workers, do you have another support system that can maybe help you get your child to appointments? We are lucky that we had that.”
However, this wider support network does not usually receive direct education on care tasks from the healthcare team, so training supports becomes an additional role for the primary caregiver(s). Transcript 6:
“Only me and [second caregiver]. . .touch those medications. If something would pop up and we couldn’t be available. . .it would be very important to actually teach family members a few of those things. Even my sister knows that [patient] needs a lot of fluid, but she doesn’t exactly know the amount of fluid she actually needs.”
Objective 2. Characterizing Educational Needs
Participants were encouraged to reflect on information, resources and supports they perceived to be helpful and what could have been done to improve their journey. Their responses revealed key insights.
Format and delivery of educational materials
Participants consistently emphasized the importance of accessible and engaging educational formats. Both caregivers and pediatric recipients valued child-friendly resources such as story books, illustrative “road maps” and media such as animated videos. These formats helped make complex medical information more digestible and less intimidating. For example, one patient (Transcript 1) said “In a perfect world, you make like a Magic School Bus episode. ‘This is your kidney, this is what it does, this is what it means when they fail and these are your options.’” Caregivers also appreciated structured formats like binders and pamphlets that could be referenced throughout the care journey. Transcript 14: “We got a booklet of basically everything; questions that you can have, things that can come up, changes that’ll happen within her body.”
Timing and repetition
Participants stressed the importance of receiving information gradually and repeatedly. Education delivered before and after surgery, and reinforced over time, was seen as more effective and less overwhelming.
Age-appropriate and emotionally sensitive content
Educational content needed to be tailored to the child’s age and emotional readiness. Younger children benefited from simplified explanations focused on outcomes, while older children required more detailed information as they became more involved in their care. According to one patient, “At that age, a very simple like, ‘We’re taking this because it makes you feel better.’ That would’ve been sufficient for me.” (Transcript 2). Caregivers often shielded children from distressing details to avoid unnecessary fear or non-compliance. Transcript 17: “You don’t tell the kids things like, ‘you’re at high risk for cancer.’” Transcript 9: “She asks me, why all of a sudden do I get hair on my hands? I don’t tell her. Because if I would tell her, she won’t be taking that medication anymore.”
Caregiver vs. patient information needs
Caregivers typically sought comprehensive, proactive information to manage care and anticipate complications. They valued open communication with the transplant team and often took the lead in learning and decision-making. For example, one caregiver said, “We’re constantly pushing for information as opposed to it flowing to us.” (Transcript 16). Patients, especially younger ones, preferred simplified and immediate information, often relying on caregivers to interpret and filter details.
Transcript 14: “I usually just ask my mom . . . I’ve never picked up a booklet.” Transcript 20: “I let my mom take the lead because it was easier.”
Structure and routine, and knowing what to expect
Establishing predictable routines and clear expectations was particularly important for younger patients. Knowing what to expect helped reduce anxiety and fostered a sense of control. Transcript 2: “Just having that sense of structure. . . what can we expect coming up.” Patients explained that even as a child, it’s important to be told what to expect. Those that were provided with sufficient information ahead of time to prepare expressed gratitude for it. According to one patient,
“In terms of surgery, at that age, I still remember, meeting with a vascular surgeon, they were going over all the different things they were going to do. That actually put my mind at ease a little bit, to be honest.” (Transcript 1).
Support systems and emotional needs
Participants highlighted the value of strong relationships with the transplant team and access to emotional support and that they appreciated the opportunity for open, unrushed conversation with the entire transplant team. For example, one caregiver said, “If you ask a question to the post-transplant team, they are really good about taking the time to explain it.” Families expressed a desire to be connected with other providers such as social workers who can help with finding financial support or accommodations, or dietitians and connection to mental health supports to help with the emotional and psychological impacts of transplant was perceived to be of particular importance. One caregiver (Transcript 10) said:
“So, I spoke with his doctor who gave recommendation to Psychology who joined our team at that point. We found a fantastic counselor. And she was able to bring in this this rather sullen, withdrawn, angry guy. . . she was able to make him feel safe and give him privacy and he was able to say whatever he wanted to say. . .Now it’s two years later, and it’s not like [patient] is not going to be susceptible to low feelings. The thing is now he’s got tools to overcome them.”
Support preferences varied widely. While some children preferred privacy and family-only support, others saw value in peer connections. “We offered talking to other people about it. He didn’t want that so we just sort of handled it while we were together as a family.” (Transcript 17)
“I think she would have really benefited from having somebody else to talk to.” (Transcript 20). Among those who sought out peer support, it was perceived to be of great benefit. One patient (Transcript 3) said:
“I learnt about this group of young adults that had had transplants. . .I definitely would recommend that for future transplant patients to get involved with a group of people that have had transplants, ‘cause there is experiences and questions that only they can answer.”
Some participants who did not have the opportunity to receive peer support expressed the value this would have brought to their experience with transplant. Transcript 8: “I think the ones that I would really love is lived experience. If there is a community of people that have done that, and they are able and willing to help others.”
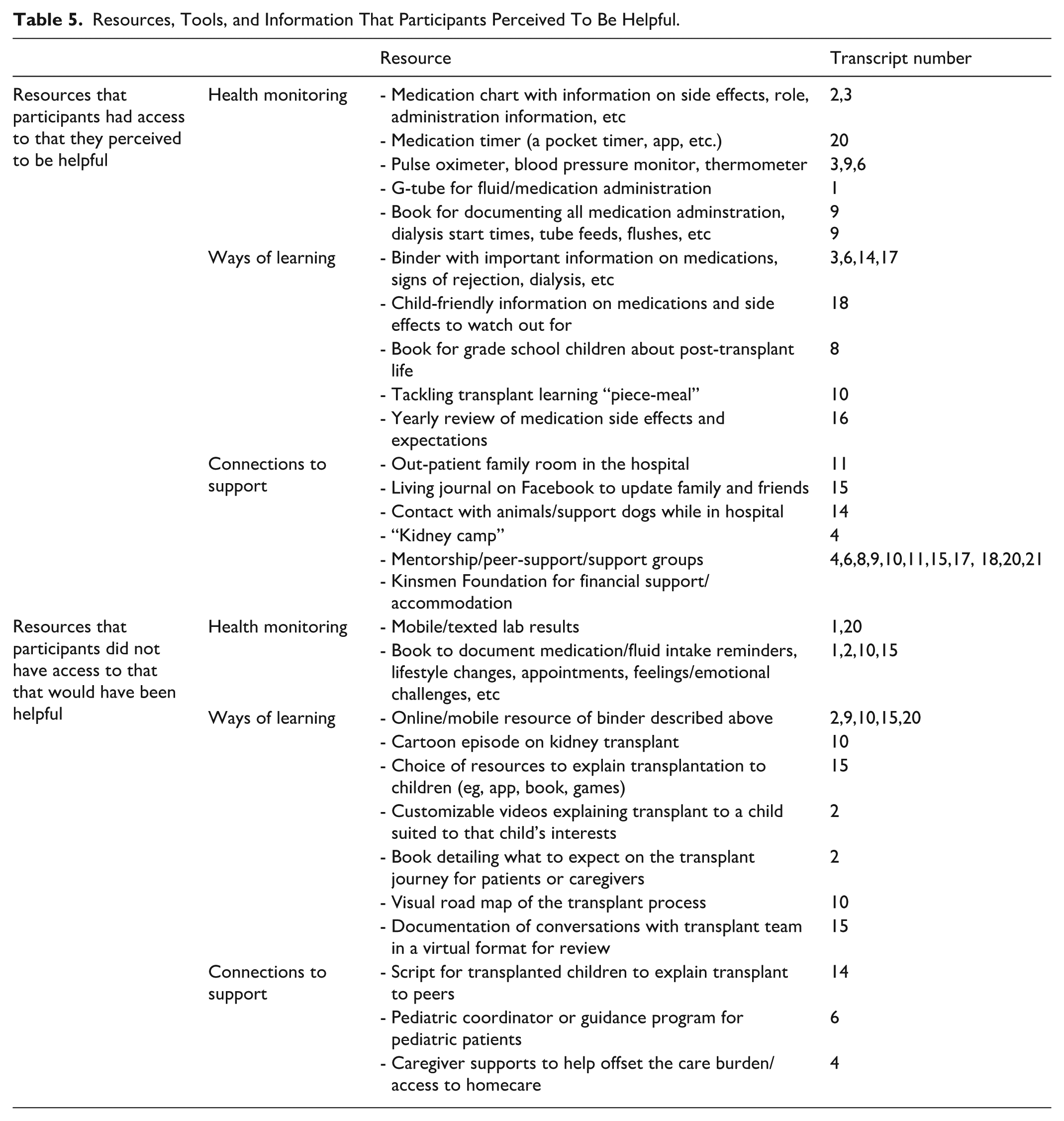
Table 5. presents resources, tools, and information that participants perceived to be helpful, while Table 6 presents the advice that participants would offer to help other patients and caregivers with their transplant journey. There is an emphasis on the importance of support as well as patience, positive attitude, communicating with the transplant team and asking questions. Patients and families would be well served by programs that work to provide social support, promote patient/family network development in addition to providing comprehensive, age-appropriate education.
Resources, Tools, and Information That Participants Perceived To Be Helpful.
Advice Participants Provided for Other Patients and Caregivers (in the Participants Own Words).

Discussion
Given the importance of education to improve success of pediatric transplantation and the lack of literature in this area, we conducted a study to characterize the experiences of patients and caregivers and to learn more about their educational needs. Previous reports have described the transplant process as stressful or overwhelming8-13 and have emphasized the life impacts on both the patient and caregiver.2,20,21 In the present study, patients and caregivers discussed how the journey to transplant is all-encompassing, with wide-ranging effects on the family’s social, mental health, and physical well-being.
While both patients and caregivers described the transplant journey as emotionally and logistically challenging, their experiences diverged in focus and perspective. Caregivers often emphasized the stress of managing care responsibilities, navigating healthcare systems, and coping with uncertainty—particularly around donor eligibility, post-operative complications, and long-term outcomes. They also expressed concern for the emotional well-being of their child and the impact on siblings and family dynamics. In contrast, patients reflected more on the personal and social consequences of transplant, such as feeling different from peers, missing out on milestones, and adjusting to lifestyle changes. Patients also described moments of empowerment and resilience, particularly when regaining physical strength or forming connections with others who had similar experiences. These differences underscore the need for holistic support strategies that address both the caregiving burden and the lived experience of the patient. 22 While patients and caregivers shared overlapping educational priorities, such as the desire for clear expectations and accessible formats, their needs diverged in important ways. Caregivers often sought comprehensive, proactive information to manage care and anticipate complications, preferring structured resources like binders and verbal explanations. In contrast, patients, particularly younger ones, benefited more from simplified, emotionally sensitive education tailored to their developmental stage, often delivered through visual or interactive formats. Caregivers frequently acted as information filters, shielding children from distressing details, while patients tended to rely on caregivers for interpretation or preferred to receive information only when immediately relevant. These differences highlight the importance of designing transplant education that is both age-appropriate and role-specific, ensuring that each member of the care team—patient and caregiver alike—is adequately supported.
Since most patient participants in the present study (70%) were adults reflecting on their childhood experiences, we compared educational insights across age groups within this cohort. Educational needs were shaped more by developmental stage and individual preference than by age alone. Children often relied on caregivers to interpret medical information and preferred simplified, emotionally sensitive explanations, focusing more on living life than understanding clinical details. In contrast, adults—particularly those reflecting on their younger selves—described feeling overwhelmed by complex information and emphasized the value of structure, routine, and visual aids to support comprehension. Both groups appreciated gradual, age-appropriate education, with younger patients benefiting from messages like “this makes you feel better,” and older individuals seeking more detailed, realistic discussions over time. Retrospective accounts highlighted that visual or interactive tools, such as videos or cartoons, could have eased understanding and reduced fear during childhood. These findings underscore the importance of flexible, patient-centered educational strategies that evolve with cognitive and emotional readiness. However, since only three participants in our study were under 19, further research is needed to better understand transplant education from the perspective of younger patients themselves.
As previously reported,2,7,21 the need for support was recognized as fundamental by both patients and caregivers, yet obtaining and maintaining a support network was not without obstacles. Education may help mitigate some of the challenges described by patients. Healthcare providers are optimally positioned to provide education that helps patients and caregivers form connections to the supports that they identify. Our study identified several challenges that we feel could be addressed by education. For example, to decrease the explanation burden on primary caregivers, healthcare providers could create a resource suitable for both alternate care providers and for knowledge transfer and sharing with friends and family.
A consistent message that arose within the dialogue was that both patients and caregivers benefit when they know what to expect. Participants recounted experiences where they were surprised by events that occurred before the transplant (such as the wait times and hospital visits), during the transplant (e.g., such as the length of the procedure, or what a child looked like post-operatively), and after the transplant (such as medication side effects, co-morbidities and complications). A previous study of family members’ experiences with patients’ treatment for end-stage kidney disease (including transplant) indicated that the degree of impact that transplant can have on daily lives and mental health can be unanticipated. 21 Notably, some unexpected experiences were attributed to a lack of forewarning from healthcare providers. 21 By providing effective education, healthcare providers can support families by helping them anticipate the transplant course more accurately. Participants in the present study described some novel educational ideas to facilitate preparedness, such as a visual road map of the transplant process or customizable video-based resources specific to a child’s interests. This has also been supported by other literature. 9
Despite the advantages of being ready as events unfold, the healthcare journey is unpredictable, no two experiences are alike, and support needs may vary for each individual throughout the journey. In the present study, frequent sources of support were found in community networks, but this looked different for every participant. Some patients and caregivers relied on extended family and friends, whereas others found support from religious communities. As healthcare providers, we tend to use a standardized approach for providing education and support, but we must recognize that this might not be enough. In the present study, some participants expressed the desire for a more personalized approach and suggested a choice of age-appropriate resources, such as books, video games, and cartoons. The desire for situation-specific information 8 and a preference for receiving information in a variety of formats 12 was also identified in our scoping review of pediatric transplant education. 7 However, creating personalized educational materials is both time and resource intensive and novel solutions can be explored. Our group is presently exploring the use of technology such as ChatGPT to create pediatric patient education. We also advocate for the use of relevant pediatric focused resources and internet-based web applications. For example, Transplant Families is a non-profit organization that offers a virtual space for resources and educational materials to help families throughout the transplant process. (https://www.transplantfamilies.org/).
The limitations of this study should be considered. Participants were recruited from a single center in Canada, and our participants were predominantly White, which limits generalizability. In the present study, we interviewed patients who previously received a transplant and their caregivers. Exploring perceptions of those who are in the pre-transplant stage (i.e., being assessed for transplant or on the waitlist) may garner additional unique insights. We included adults who had received a transplant as a child, and seven of the participants were over the age of 20. For the patient participants, all had received their transplant at least 5 prior to participation in the study and were reflecting on their past experiences in hindsight. Program changes may have occurred since their transplant experience. While these testimonials could be influenced by recall bias, thoughts and emotions recounted years later should still be considered relevant. All interviews with adolescent participants were conducted jointly with their caregivers. Although this was the choice of the participants, conducting paired interviews may influence feedback, as individuals might not speak as candidly about their experiences as they would have if interviewed alone. There is potential selection bias, given our sample may over represent patients and families with positive experiences. Finally, the ability to gain information from a wider age range of pediatric patients would have been ideal and we recognize this as a limitation.
Conclusion
Patients and caregivers described their experiences with the transplant process. Participants identified the need for personalized, age-appropriate education delivered in digestible formats, with clear expectations, timely reinforcement, and emotional support tailored to both patients and caregivers. Being prepared for the transplant can fundamentally impact the experience. As healthcare providers, we should strive to provide personalized and holistic education to facilitate expectations and prepare patients and caregivers for the journey that lies ahead. The participants’ call for enhanced social support throughout the transplant process should not be ignored. The insights gathered from the study will help inform the development of educational resources for pediatric patients and caregivers.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251399080 – Supplemental material for Characterizing the Experiences and Educational Needs of Patients and Caregivers During the Kidney Transplant Process
Supplemental material, sj-docx-1-cjk-10.1177_20543581251399080 for Characterizing the Experiences and Educational Needs of Patients and Caregivers During the Kidney Transplant Process by Michelle Ruhl, Ashley Burghall, Brianna Groot, Nicola Rosaasen, Kayla Flood, Keefe Davis, Natasha Minakakis, Jenny Wichart and Holly Mansell in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would also like to acknowledge the support of the Canadian Donation and Transplantation Research Program (CDTRP) and thank the patients and caregivers for sharing their stories.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by the Jim Pattison Children’s Hospital Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article cannot be shared publicly for the privacy of individuals that participated in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.