
Abstract

Keywords
Introduction
A disaster is a “serious disruption of the functioning of a community or a society at any scale due to hazardous events interacting with conditions of exposure, vulnerability, and capacity, leading to one or more of the following: human, material, economic, and environmental losses and impacts.” 1 The hazardous events can be natural, such as earthquakes and hurricanes; technological, such as explosions and infrastructure failures; or societal or human-caused, such as conflicts, wars, and terrorist attacks.2,3,4,5 It is distinct from an emergency, whereby the disruption of the functioning of a community or society does not occur. 1 Although these terms are distinct as per the United Nations Office for Disaster Risk Reduction, we conceptualize them as a spectrum with the potential of an emergency to evolve into a disaster based on the resiliency of the community, and unfolding of the hazard, and in some cases, the aftershock. Given the potential fluidity between these terms and acknowledging the potential for conflation of the terms “disaster” and “emergency” in the medical literature, we will refer to both via the use of the word “disaster” from here on.
Canada has endured several disasters, which have directly or indirectly affected people living with kidney disease. 6 Significant wildfires occurred in 2023, starting in the early spring in Alberta and followed by large wildfires in Quebec, Nova Scotia, the Northwest Territories, and British Columbia. Many resulted in mass evacuations, such as two thirds of the Northwest Territories’ nearly 45,000 residents, 7 including the displacement of people receiving hemodialysis. Thirty-nine people on dialysis from the Northwest Territories were transferred to Alberta to receive dialysis (unpublished data). Forty remotely located Indigenous people who received hemodialysis in satellite dialysis facilities in Indigenous communities of Northern Quebec were evacuated to Montreal due to wildfires. 8 Prior to these events, in 2017, a wildfire in British Columbia led to a hemodialysis unit shutdown, disrupting the location of care for individuals on dialysis. 9 In 2021, torrential rain and winds in British Columbia also impacted the care of many people on dialysis; 50 were stranded without access to dialysis for up to 5 days in some cases. 10
Experiences and resilience of the Canadian kidney community during disasters to date have been anecdotal in the lay press or professional organizations’ news releases, remaining unprofiled in academic literature. While program-level and provincial-level initiatives to manage disasters exist in some regions, supported by a Bridge Grant from the Canadian Institute of Health Research and by the Sustainable Nephrology Action Planning Committee of the Canadian Society of Nephrology (SNAP-CSN), a pan-Canadian group of researchers, administrators and clinicians has initiated the process of strengthening disaster management in kidney care. In this opinion piece, we elaborate on why the Canadian kidney care community must champion a national approach to disaster and emergency risk reduction and management (DERRM).
Disaster and Inequities
Scope of Disasters (Not Emergencies) Globally
From 2000 to April 27, 2025, the International Disaster Database has recorded 16 209 natural and technological disasters that led to almost 1.8 million deaths, affected over 4.7 billion people, and caused over USD 4.5 quadrillion dollars in damages. 11 These numbers are likely an underestimate, given that only country-level human and economic losses for disasters that meet at least one of the following criteria are recorded: 10 fatalities, 100 affected people, a declaration of a state of emergency, or a call for international assistance. Thus, several emergencies and some disasters are likely not captured and reported. Nevertheless, the monetary damage incurred from disasters has risen, as depicted in Figure 1. Also, while reported deaths stabilized between 2011 and 2021, an increase in 2022 and 2023 likely represents the profound and multifaceted impacts of the COVID-19 pandemic on health systems globally.
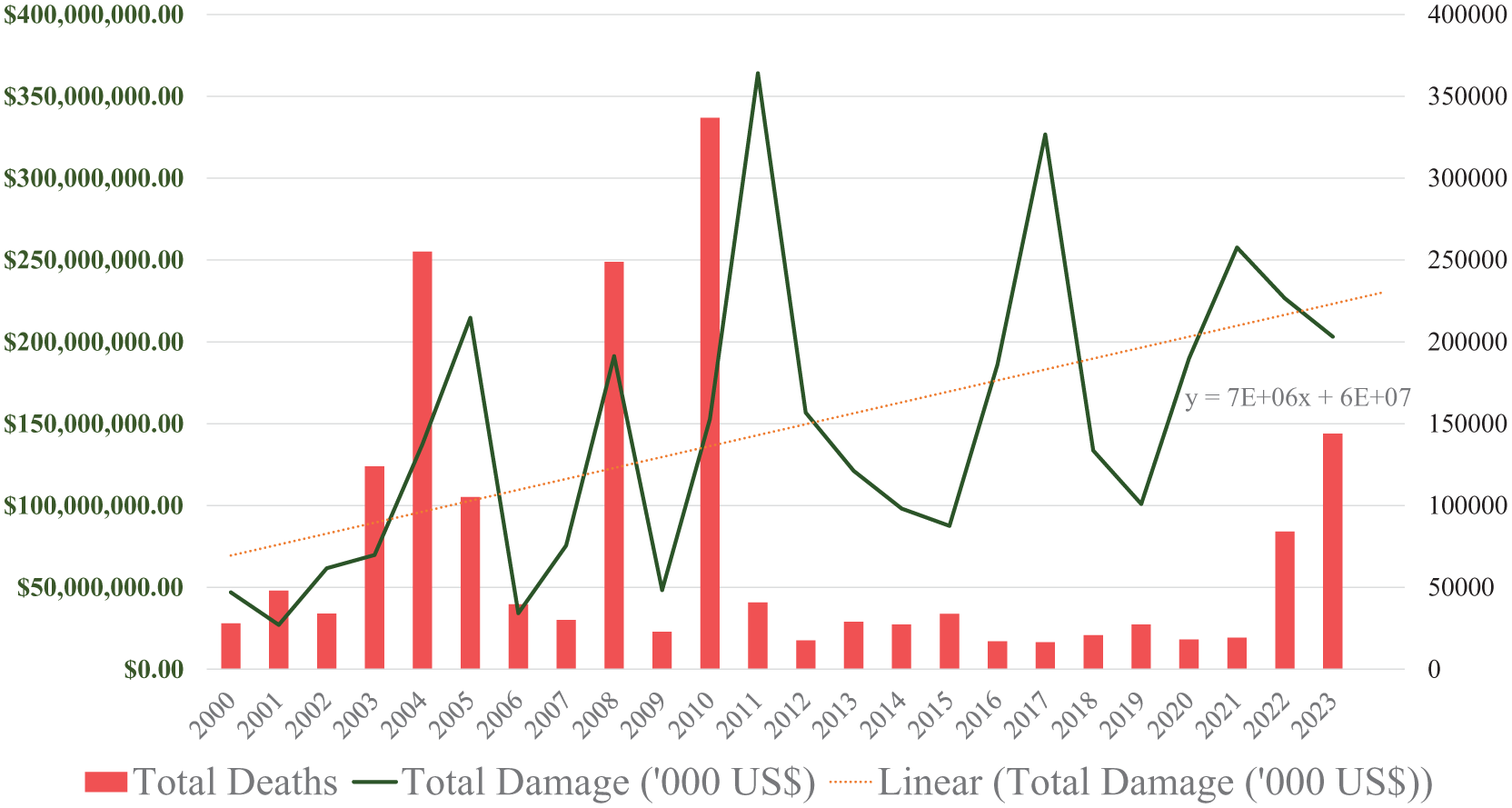
Total deaths and monetary damage based on the start year of a particular disaster.
Scope of Disasters in Canada
Canada is an at-risk country for severe weather and geological events due to its northern location, varied landforms, and weather types, 6 as well as its potential exposure to alterations in these factors brought on by climate change. In addition, reliance on technology has created vulnerabilities should power grids or electronic devices be compromised, increasing the risk of cascading effects on health systems, given the current tendency to consolidate technological resources into larger, more distributed networks.12,13 From 2000 to 2020, the Canadian Disaster Database has reported 424 climate-, conflict-, and technology-related disasters that have resulted in 1741 deaths, 12 792 injuries, displaced 603 549 people, and cost CAD >$19 billion. 6 This does not include data from the 2023 Canadian wildfires that severely impacted air quality. 14 The increasing incidence of these events threatens to overwhelm the ability of systems to protect Canadians and their communities. 15
Inequitable Impacts of Disasters
The impacts of climate and other disasters on communities are inequitable and vary by exposure and vulnerability.5,16-18 A range of individual factors and social determinants of health can increase person-level vulnerability to disasters and are pictorially depicted in Figure 2.5,16-18 For example, poverty and economic standing increase individuals’ vulnerability to disasters. In an analysis of flood disasters in 67 middle- and high-income countries between 1990 and 2018, the association between income inequality and flood mortality was demonstrated even after accounting for the per-capita real gross domestic product, the level of flood exposure, and other confounding variables. 17 Notably, the intersection of these factors can create or amplify risk. 5 Thus, people with intersectional characteristics, such as women with lower economic standing, become more vulnerable within the at-risk groups. 19
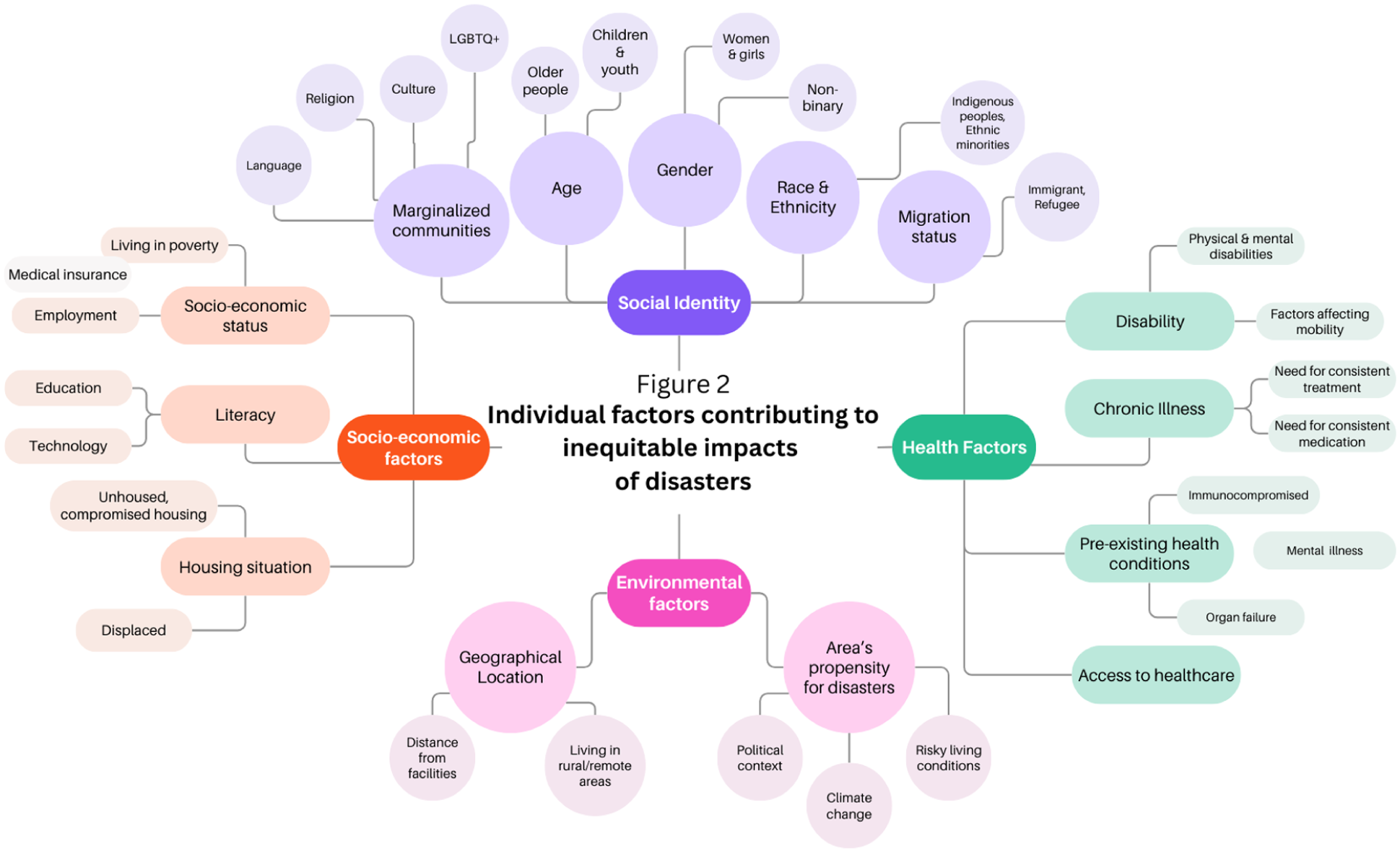
Person-level or individual factors that contribute to inequitable impacts of disasters (factors primarily derived from the World Health Organization 5 and the experiential knowledge of our team).
The Inequitable Impacts of Disasters on Canadians Living With Kidney Diseases
Excluding Quebec (data not available), in 2023, >49 000 Canadians were living with end-stage kidney disease (ESKD). 20 Of these, 29 906 were receiving different forms of kidney replacement therapies and 19 356 were kidney transplant recipients (KTRs). 20 Approximately 11% to 13% of the Canadian population is estimated to be affected by chronic kidney disease (CKD). 21 Moreover, the scope of both CKD and kidney failure is rising due to an aging population and an increasing burden of risk factors, such as diabetes, hypertension, and obesity.21-23 Indeed, there has been a 19% increase in incident patients receiving kidney replacement therapy (dialysis or pre-emptive kidney transplant) between 2014 and 2023. 20 Disasters’ impact on people living with kidney diseases is a function of hazard, vulnerability, and exposure. Given the frequent dependence of people with kidney disease on complex community and health system structures and the requirement for uninterrupted therapies, these individuals are uniquely exposed and hence vulnerable to the disruptive effects of disasters on system capabilities, as discussed below and depicted in Figure 3.
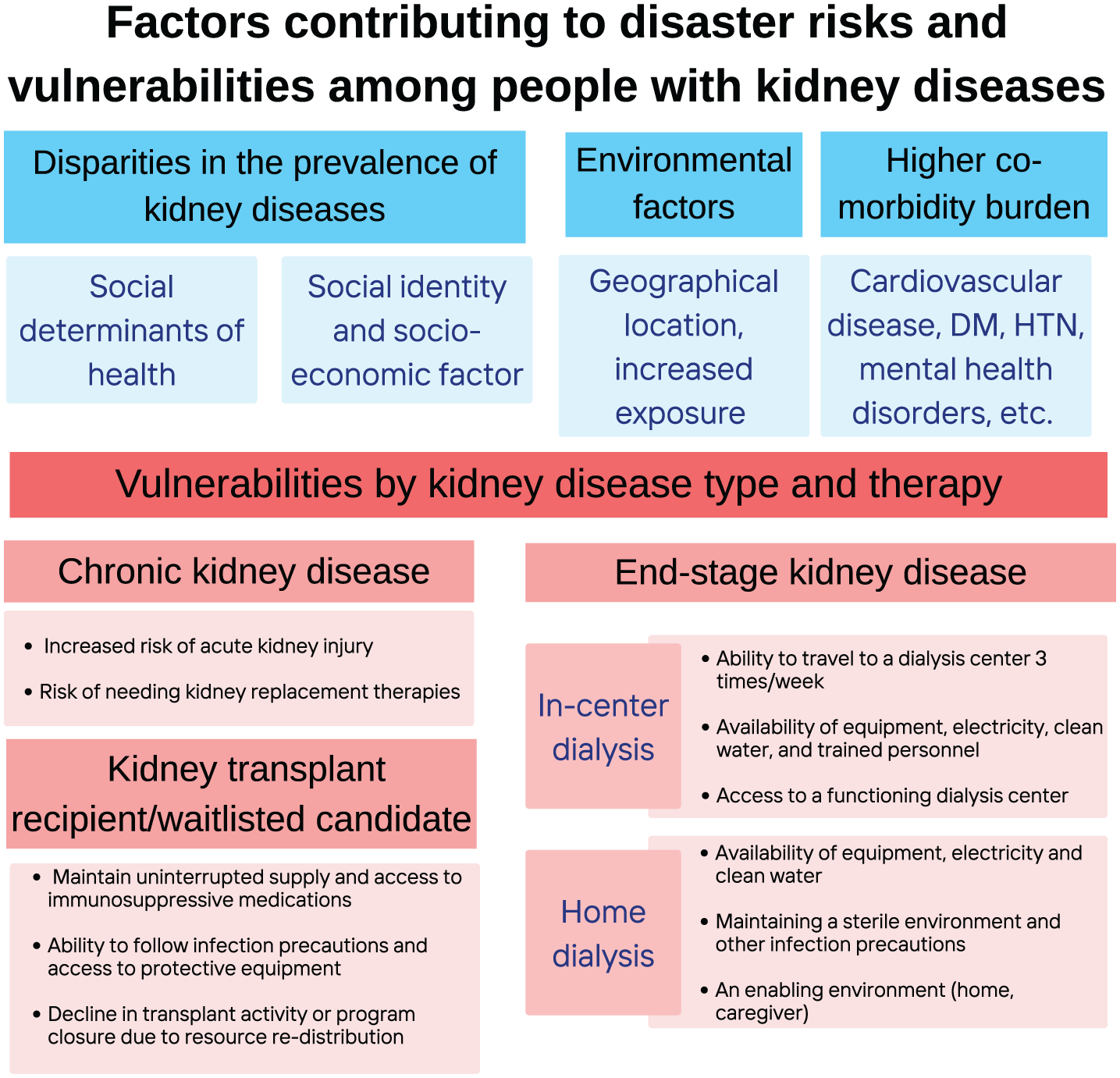
Factors contributing to the risks and vulnerabilities among people with kidney diseases to disasters and emergencies.
Disparities in the Prevalence of Kidney Diseases
Several factors outlined in Figure 2 contribute to a higher risk of CKD and ESKD. For example, the burden of kidney diseases and kidney failure is disproportionately higher in marginalized and Indigenous populations in Canada and in other countries.24-30 A synthesis of 35 studies reported that lower socioeconomic status was associated with 41% higher risk of low eGFR, 52% higher risk of high albuminuria, and 55% higher risk of kidney failure. 31 In another synthesis of 29 studies, limited health literacy, which tends to be more common in marginalized populations, was significantly and independently associated with hospitalizations, emergency department use, missed dialysis sessions, cardiovascular events, and mortality among patients with CKD and ESKD. 32
Vulnerabilities of Canadians Receiving Dialysis
Dialysis is a life-sustaining therapy offered on a large-scale outpatient basis and requires the uninterrupted availability of equipment, electricity, large quantities of clean water, and trained personnel, all of which might be disrupted in a disaster.33-35 The survival of those with ESKD depends on the safe provision of this therapy multiple times a week. Post-disaster analyses report an increased risk of hospitalizations and mortality among dialysis patients.36-38 In the United States between 1997 and 2017, hurricane exposure was associated with a 13% higher mortality risk when compared with other non-exposed dialysis patients. 37 An analysis of 52 995 patients on hemodialysis across the Eastern and Midwestern United States reported that the 2023 Canadian wildfires severely impacted air quality. The presence of wildfire smoke plumes was associated with an 18% increase in the risk of same-day all-cause mortality and a 3% increase in the risk of all-cause hospitalization. 14 People receiving home therapies generally perform dialysis 4 to 7 times a week and may also face logistical challenges in obtaining dialysis-related supplies and having an appropriate environment to perform their treatments. Disruptions can manifest from damaged health care infrastructure, limited water and energy availability, transportation difficulties, or the need to evacuate.33,34
Vulnerabilities of Kidney Transplant Recipients and Waitlisted Candidates
While the vulnerability of KTRs to disasters is generally accepted to be lower than that of people on dialysis, they are also vulnerable to the impacts of a disaster. First, KTRs take immunosuppressive medications, and unsanitary conditions that are likely to arise during disasters can increase infection risk. 39 Also, graft survival depends on the adequate and uninterrupted supply of immunosuppressive medications, and a lack thereof increases the risk of rejection and graft failure.34,40 In a study of 296 KTRs after the East Japan earthquake, 16% reported difficulty continuing medication due to medication loss, contamination, inability to access the location where medication was stored, and the inability to make an outpatient visit. 41 Disasters can also disrupt the functioning of organ procurement organizations and living and deceased donor programs, leading to a significant reduction in transplant activity.42,43
Vulnerabilities of People With Chronic Kidney Disease
People living with CKD are at a higher risk of acute kidney injury (AKI), 44 and pre-existing CKD in those experiencing AKI is a risk factor for mortality. 45 Many disasters are known to increase the risk of AKI via crush syndrome, dehydration, or infectious causes.46,47 In cases of war, AKI may develop as a result of polytrauma and toxin exposure.46,47 For example, following the 1988 earthquake in Armenia, nearly 600 cases of AKI were reported.48,49
Comorbidity Burden
Above and beyond the direct needs related to kidney replacement or kidney disease-specific therapies, people with kidney diseases have overall increased health care needs due to usually complex comorbidities.50-53 For example, in a retrospective population-based cohort study of 530 771 adults with CKD residing in Alberta, between 2003 and 2011, 25% of participants had ≥3 comorbidities and 7% had ≥5 comorbidities. 51 Comorbidities were associated with an increased risk of hospitalization. Limited access for management of these issues may also contribute substantially to the excess morbidity and mortality experienced by this population during disaster events.
Vulnerabilities of Children With Kidney Diseases
Disasters may disproportionately harm children by affecting their physical and mental health, interrupting their education and social development, and displacing them and/or their families.54,55 Displacement and related resettlement problems are particularly risky situations that may lead to exploitation and abuse. 55 Children with kidney diseases likely face all the risks mentioned above; however, there is limited data exploring these effects in pediatric populations. In the 0- to 19-year age group, excluding Quebec, the estimated rate of ESKD in Canada is 76.2 per million population. 20 Robust epidemiologic data on CKD prevalence in the Canadian pediatric population are currently lacking. 21
Championing Disaster and Emergency Risk Reduction and Management in Kidney Care
What Is Disaster and Emergency Risk Reduction and Management?
Disaster risk reduction entails developing strategies and policies aimed at preventing new disasters and reducing existing disaster risk while managing residual risk. 1 Disaster risk management is the application and implementation of these mitigating policies and strategies. 1 Together, they ultimately contribute to strengthening health system resilience and lessening disaster-related losses. Thus, our approach to DERRM entails setting out the goals, specific objectives, and related actions for reducing disaster-related risks.
Why Disaster and Emergency Risk Reduction and Management?
Simulation and analytical studies have shown that a robust disaster preparedness plan is a cost-effective method of reducing morbidity and mortality.56-61 A study of 4 earthquakes reported that a high preparedness index had a low case fatality rate (about 1 death per 100 injuries), while mixed and low levels of preparedness had 31 and 167 deaths per 100 injuries, respectively. 60 In a cost-benefit analysis, investment in disaster risk management was shown to have a benefit/cost ratio of 3.7. 57
Why Champion Disaster and Emergency Risk Reduction and Management in Nephrology?
The Alliance for Transformative Action on Climate and Health (ATACH) is a WHO-led initiative to build climate-resilient and sustainable health systems; Canada has committed to this initiative. 62 A DERRM protocol can facilitate the needs of people with kidney diseases and ensure that timely and appropriate care is delivered commensurate with the scope of the disaster/emergency and damage incurred. The urgent medication and dialysis requirements of people with kidney diseases may be unrecognized by national emergency organizations.63-66 Detailed planning is essential to ensure people receiving dialysis care have uninterrupted access to this life-sustaining therapy. 34 Also, an after-disaster return-to-service plan is essential to offload the workload of other dialysis centers that may have assisted in providing dialysis to displaced individuals. Consensus statements from leading organizations recommend preparing for disasters by developing effective action plans with regularly reviewing and updating them to help mitigate post-disaster disorganization, panic and chaos.34,63
Furthermore, a thorough assessment of risk-prone areas may help build resiliency by better promoting best practices in nephrology and advancing environmentally sustainable kidney care practices. 67 For example, a disaster-prone area may prefer to decrease patient exposure and vulnerability by promoting kidney transplantation or universal early CKD detection programs to intervene and decrease progression to ESKD. Simultaneously, education and communication activities may be strengthened using virtual technologies. 68
Why Pursue a National Approach?
Although impact assessments following disasters and emergencies that the kidney communities have faced have not been officially conducted, there is a perception that disasters in Canada affecting people with kidney diseases are often small-scale and isolated events; thus, DERRM may not be prioritized by individual health systems. In the United States, dialysis facilities are mandated by federal regulations to have an emergency preparedness plan in place. 63 Despite this, gaps in emergency preparedness for dialysis patients, facilities, and providers have been described.69-71 Thus, we believe a nationally led but locally delivered approach will allow the advantages of economies of scale, shared expertise, a network to amplify strategies, and collective bargaining power.
The Path to Resiliency
Many member states and partners of the WHO have committed to climate-resilient and low-carbon health systems: systems that are “capable of anticipating, responding to, coping with, recovering from, and adapting to climate-related shocks and stress, while minimizing greenhouse gas emissions and other negative environmental impacts to deliver quality care and protect the health and well-being of present and future generations.” 72 In addition to the ongoing initiatives of SNAP-CSN surrounding climate mitigation and environmentally sustainable kidney care,73-75 we outline some ongoing and future initiatives to strengthen resiliency, particularly related to DERRM.
Needs Assessment and Gap Analysis
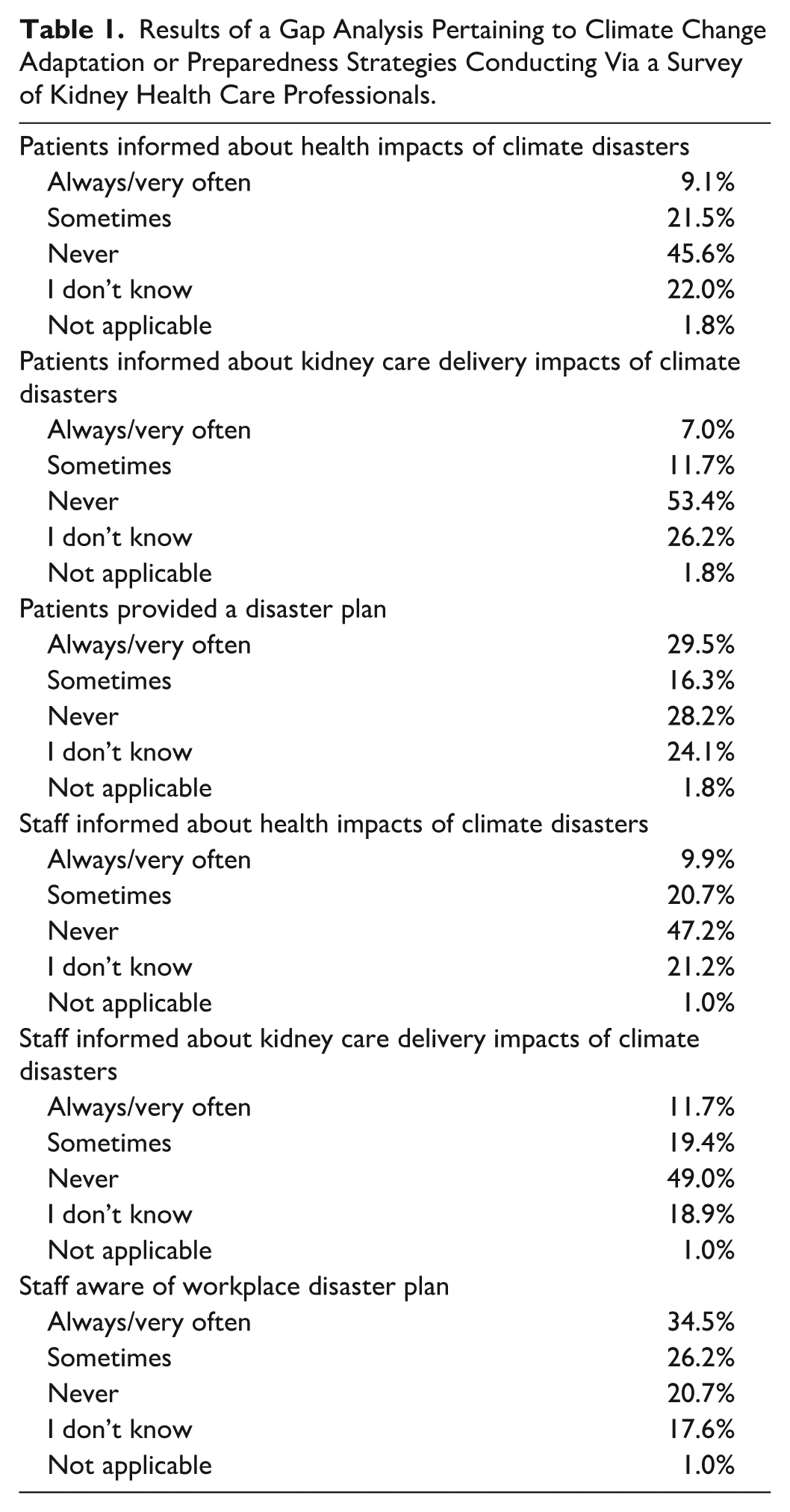
A gap analysis was conducted to help identify the knowledge and practice needs of kidney care professionals in Canada and internationally.76-78 The Canadian study included 421 kidney care providers from across Canada and also sought to identify climate change adaptation or preparedness strategies; pertinent results are presented in Table 1. Notably, over half the respondents in the Canadian survey either responded “never” or “I don’t know” to several questions related to disaster preparedness. An explanatory approach is now being adopted to explain these findings, explore provincial variations, and develop research and practice priorities.
Results of a Gap Analysis Pertaining to Climate Change Adaptation or Preparedness Strategies Conducting Via a Survey of Kidney Health Care Professionals.
A Framework in Disaster and Emergency Risk Reduction and Management
We conducted a scoping review and a content analysis of contemporary literature addressing disaster management in kidney care to create a framework across the domains of disaster preparedness, response, and recovery. 79 Of the 45 included articles, none emerged from Canada. Following a content analysis using the framework method, we have developed a roadmap in disaster preparedness, response, and recovery that will now inform a vulnerability and adaptation assessment of existing health care systems. We also aim to operationalize this roadmap to develop a context-specific DERRM approach.
Sharing Expertise
The BC Renal (a provincial renal program that plans and coordinates health care services for patients with kidney diseases) and the health authority renal programs in the province of British Columbia have jointly developed a Provincial Renal Emergency Management and Business Continuity Plan. 80 This Learning Health System is designed to address all types of hazards that might be experienced by the kidney community across the province and ensure hazard, risk, and vulnerability assessments are conducted at regular intervals to generate a continuous cycle of learning and improvement. 81 Members from this organization are integrally involved in our resiliency efforts to identify shareable practices and resources.
Patient-Inclusive and Patient-led Resiliency Efforts
Anecdotal reports from other countries state that during disasters, patients were reluctant to be separated from their families,82,83 or evacuate without their pets. 63 In a survey of 386 patients following Hurricane Katrina, while most participants were aware of the evacuation plan, only 73.2% stated they followed these plans; 72 reasons for this were not explored. Engaging patients and incorporating their perspectives in health research can inform education and policies, enhance health care delivery and governance, and increase the uptake of these policies by the end-users.84-87 Although patients with kidney diseases have expressed concern about the capacity of the regional system to accommodate their dialysis treatments, 88 literature examining patient and provider perspectives or experiences is scarce and at risk of bias, and there is a dearth of efforts on engaging both groups in resiliency efforts. 89 While individual resilience, preparedness, and knowledge are essential, established connections within the community and social capital can mobilize grassroots initiatives. People living with kidney diseases display incredible resilience, which serves as an inspiration in our approach to DERRM in Canadian kidney care. Meaningful partnership with Indigenous patients and communities will be a key goal, given their likelihood of being disproportionately affected by climate disasters due to often residing in geographically remote communities with a relative paucity of infrastructure. Yet, their extensive and generational ecological knowledge and environmental understanding, and spiritual, cultural, and communal aspects of life can provide holistic approaches not just to DERRM but also to climate mitigation in general.
Conclusion
Anecdotal experiences of our team and reports in the lay press suggest that the kidney care community has dealt effectively with several disasters and emergencies over the past decade. People living with kidney diseases are uniquely vulnerable to the impacts of a disaster due to a variety of factors. We propose learning from the remarkable resiliency of our patients, health care teams, and Indigenous communities, who can provide experiential knowledge to help build a robust approach in DERRM. We recommend a national and unified path to resiliency that allows the advantages of economies of scale, shared expertise, and collective bargaining power.
Footnotes
Acknowledgements
Drs S.S. and I.E. are supported by the Chercheur boursier clinicien—Junior 1 award from the Fonds de recherche du Québec—Santé. Dr C.S. is gratefully supported by the Marcia Bell Distinguished Scholar Award from the University of British Columbia.
ORCID iDs
Consent
Not applicable.
Author Contributions
S.S.: Contributed to idea and conception; writing first draft.
S.E.W.: Contributed to figures.
All other authors contributed to the critical feedback and review of the manuscript. All authors approve the final version to be published and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a CIHR—Priority Announcement—Pandemics and Health Emergencies Research—Multi-Year Funding (Funding ID: 202409PNM).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr S.S. Sandal has received an education grant from Amgen Canada to improve the care of patients with graft failure and has received a speaking honorarium from AstraZeneca. Dr R.S. has participated in advisory's boards and received speaker fees from Roche, Otsuka, Novartis, GSK, and Sobi. The other authors have no relevant disclosures.
Data Availability Statement
No new data generated.