
Abstract
Background:
Patients with chronic kidney disease (CKD) at times must decide whether to take an invasive approach to management of coronary artery disease (CAD), which involves procedures such as angiography, angioplasty, and surgery, versus attempt management with medications alone.
Methods:
Human-centered design was used to develop the decision aid while concurrently identifying design features that could facilitate its incorporation within patient-physician clinical encounters. Interviews exploring use of the decision aid with patients and care providers were qualitatively analyzed according to the theoretical domains framework to identify barriers and facilitators to implementation. Simulated encounters between patient and physicians were used for pre-clinical testing and to identify additional training and resources that could support effective implementation.
Key Findings:
Implementation insights overlapped with decision-aid design input and influenced key design elements of
Limitations:
Clinical evaluation has not yet been completed.
Implications:
Background
Coronary artery disease (CAD) commonly accompanies chronic kidney disease (CKD), and can result in hospitalizations, reduced quality of life, shortened survival, and has implications for receiving a kidney transplant. 1 Patients with CKD and CAD often must decide whether to take an invasive approach to management, which involves procedures such as angiography, and revascularization procedures to diagnose and treat heart disease, versus attempting optimal medication management alone. This can be a challenging decision for patients and care providers to make, due to the complex trade-offs in the benefits of these procedures for treating heart disease versus their unique risks to the kidney health of people with CKD. 2
In earlier phases of work, our team engaged with patients with CKD and CAD, and their care providers to develop patient-oriented solutions to address this issue. As a project funded by the patient-oriented research network, Canadians Seeking Solutions for Chronic Kidney Disease (Can-SOLVE CKD), patient partners with lived experience guided all aspects of our research. We first conducted qualitative studies with patients and health care providers to characterize their experiences with CKD and CAD and identify potential strategies to overcome identified challenges in care.
2
We then developed and validated predictive models to provide patients and their care providers with personalized benefit-risk information under different treatment options for CAD. We also conducted a discrete choice experiment to better understand the values patients placed on the attributes of different treatment options, and how patient preferences varied.
3
Finally, we used human-centered design (HCD),4
-8 informed by International Patient Decision Aid Society9,10 and the Ottawa Decision Support Framework,
11
to synthesize current knowledge within a decision aid that we have named
This initiative has now progressed to implementation and evaluation of a SDM approach to invasive versus medical CAD management decisions, supported by the
Methods
This project’s activities revolve around Can-SOLVE CKD’s 4 pillars of: (1) implementation science/knowledge mobilization, (2) Indigenous cultural competency, (3) incorporation of equity, diversity, and inclusion (EDI) principles in knowledge mobilization and implementation efforts, and (4) patient engagement and capacity building. The ways each of these 4 pillars have been applied are described here.
Pillar 1: Implementation Science/Knowledge Mobilization
To ensure capacity within the project team to support implementation, 3 team members completed courses on “The How of Creating Sustainable Change” and “Implementation Scale and Spread” offered by the Centre for Implementation (https://thecenterforimplementation.com/). This allowed us to capture early insights into barriers and facilitators to implementing
To further augment our implementation strategy, we conducted simulated patient-physician encounters for pre-clinical testing of the decision aid. We created 4 unique patient personas and used them with 2 patients and 2 physicians to simulate and observe encounters using the decision aid in hypothetical outpatient clinic and hospital settings. The sessions were observed by the research team, and the patients and physicians who participated in the simulated clinical encounters were debriefed to understand their experience incorporating the decision aid into a patient-physician encounter, barriers to use during the encounter, and strategies to overcome challenges with its integration. Input from this activity was used to make final refinements to the decision aid and identify additional accompanying implementation training materials and guidance resources required to support clinical use.
We are now conducting an implementation pilot trial that will introduce and evaluate the
Pillar 2: Indigenous Cultural Competency
We have respectfully worked with Indigenous peoples and engaged representatives of Indigenous communities in the Treaty 7 territories of the Tsuut’ina First Nation, and the Stoney Nakoda First Nation to learn how we can promote SDM using the
Through in-person meetings, we introduced the objective of our project to support SDM for people with CKD and CAD. Together, we discussed personal and historical experiences of Indigenous peoples with health care, identifying racism, bias and injustices, and barriers to access to care as contributors to distrust of health care providers and the health system by Indigenous peoples. Using the
Pillar 3: Incorporating EDI Principles and Health Equity
Finding optimal treatment approaches to cardiovascular disease and heart health was previously identified as a top 10 research priority by patients with CKD and health care providers in Canada. 17 We have approached this topic using HCD4,5,18,19 and SDM13,14,20 frameworks that promote respect for each person’s unique experiences, values, and preferences for their care. These frameworks are well suited to support understanding personal and systemic contexts and to deliver equitable care and outcomes for all patients. Building upon these objectives, our project naturally progresses to embed EDI-promoting processes within implementation practices. Existing evidence demonstrates that decision aids can improve patient knowledge, reduce their decision uncertainty, improve patient experience, and value-congruent treatment decisions.21 -23 At the same time, we recognize that thoughtful implementation is also needed, so that decision aids do not exacerbate existing inequities and biases in care delivery.
We developed the
Pillar 4: Patient Engagement and Capacity Building
Patient partners with lived experience with CKD and CAD meaningfully contributed to the project from its outset by providing valuable input on the development of the decision aid, co-designing its implementation and evaluation plan, and in disseminating knowledge about the project to study participants and the public. Strategies used to engage patient partners included recurring full team meetings focusing on co-design and creation, participation in development of the education and implementation support resources, patient consent forms, and development of educational videos. A noteworthy contribution of patient partners has been their involvement in the development of the project evaluation framework. This involved meetings to prioritize the primary and secondary outcomes for the implementation pilot trial, and selection of the instruments used to measure patient experience, quality of SDM, and decision conflict from the patient perspective. One patient partner described the development and implementation planning meetings to the Can-SOLVE CKD Research Operations and Knowledge Translation (ROCKeT) Committee as follows: The learning process of the decision tool’s purpose was interesting: learning more about the interventions for heart disease and the relation to renal function. As a patient partner, I helped to review and reword materials and asked questions that caused the research team to “rework” a part. I don’t feel there were any challenges for me, the team was welcoming and ensured patient partners understood the importance of testing out the tool, and very open to any feedback. Team meetings were well attended, I thought, and it was nice to see everyone coming together for this project, whether you were a researcher, doctor, patient or nurse.
Key Findings
Thirty-two patients and 18 physicians provided implementation perspectives for the decision aid. Among patient participants, 47% were less than 65 years of age and 47% were women. Among the physician participants, 72% were less than 50 years of age and 22% were women. Supporting quotes and themes related to implementation planning across the domains of capability, motivation, and opportunity, organized within the TDF, 16 are shown in Table 1.
Insights From Patients and Clinicians According to the Theoretical Domains Framework (TDF) for Implementing the

Both clinicians and patients alike saw benefits in using
These findings led us to design the decision aid so that it would support varying use preferences and contexts, encompassing both digital and paper-based forms for use, depending on patient preferences and support available for use of digital technologies. Implementation considerations also influenced the order and arrangement of the content in My Heart and CKD to enhance its integration into the clinical environment of SDM encounters. The decision aid and implementation workflow were developed to be adaptable to variation in the amount of time and discussion that might be required between patients and their care givers or family before assessing patient knowledge and arriving at and documenting a decision.
Findings from our qualitative analyses and pre-clinical simulated patient-physician encounters indicated that additional training and implementation support materials would be needed by users to implement the decision aid. Guided by Can-SOLVE CKD’s 6-Step Pathway to Implementation Guide,
28
we thus created a collection of documents, resources, education, and training materials to help local teams implement
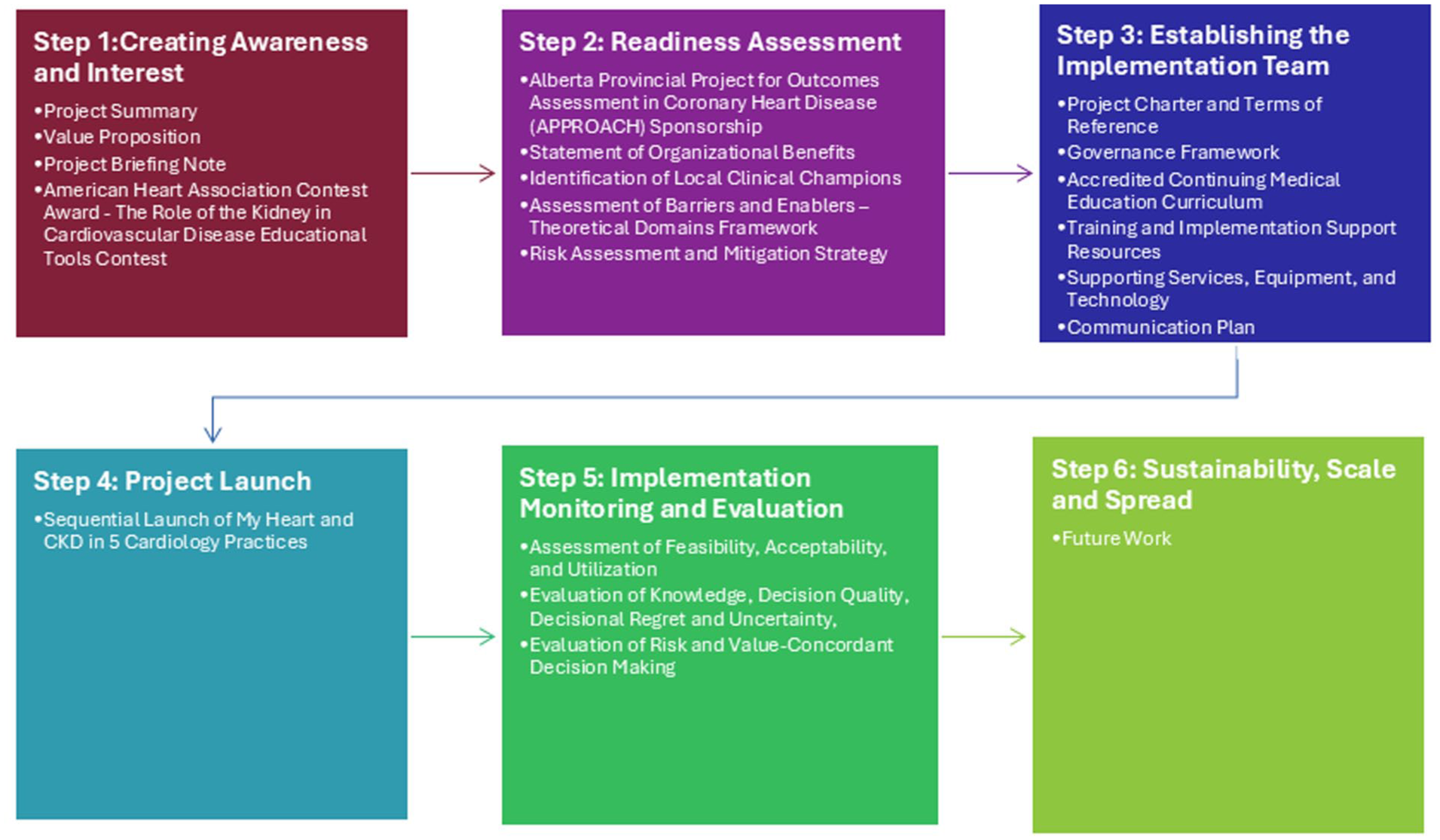
Application of the Can-SOLVE CKD network pathway to implementation for the

Outline of the training modules created for health care providers to support implementing the My Heart and CKD decision aid.
Discussion
We have worked across Can-SOLVE CKD’s 4 major pillars, following the six steps within the Pathway to Implementation to develop an implementation strategy for the
Implementation strategies for decision aids need to carefully balance physician expertise while making room for the patient voice in the shared treatment decision-making process. Throughout the project, patients have shaped the design of I would say use the tool, go slowly, go carefully, look at all aspects and ask questions. If you don’t understand or you are asking should I, could I, would I? There’s always somebody available to answer any question you have.—
Strengths of our project include the insights of patients with lived experience, clinicians with experiences caring for people with CKD and CAD, and application of evidence-informed frameworks, such as HCD, the Ottawa decision support framework, and the TDF in development and implementation of the decision aid. However, we have encountered several limitations. Much of the iterative development and interviews with patients was affected by the COVID-19 pandemic, which required us to use virtual sessions and may have altered people’s preferences and experiences with use of digital health technologies. This could have either enhanced or suppressed identification of certain barriers or facilitators to implementation of a web-based tool in clinical practice. However,
As we are still in early stages of implementation, we do not yet know for certain how our identified barriers and facilitators will translate into real world use. It is uncertain whether the intended flexibility of ways to use the decision aid will translate into implementation success in clinical practice. However, we have created a range of support materials for different audiences and in different modalities, and in-person implementation supports to help each clinical environment determine which form of use work best for their situation. While in-person support may not be possible beyond the pilot trial (ie, a potential limitation of scale and spread planning), we do intend to collect and apply the insights and experiences gleaned from the pilot trial to refine or development resources to support future broader implementation efforts.
Implications

Infographic conveying the value of implementing the My Heart and CKD decision aid.
By mobilizing knowledge through decision support, promoting SDM in a manner that addresses known health inequities, and amplifying patient involvement and recognition of their values and preferences in decision-making, this program of work aligns with Can-SOLVE CKD’s mission to transform kidney care and foster equitable health experiences and outcomes for Canadians living with CKD.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581251389602 – Supplemental material for My Heart and CKD: Pathway to Implementing a Decision Aid for Patients With CKD and Coronary Artery Disease
Supplemental material, sj-pdf-1-cjk-10.1177_20543581251389602 for My Heart and CKD: Pathway to Implementing a Decision Aid for Patients With CKD and Coronary Artery Disease by Julie N. Babione, Pantea Javaheri, Denise Kruger, Todd Wilson, Winnie Pearson, Maureena Loth, Violet March, Wayne Gerber, Bryan J. Har, Michelle M. Graham, Stephen B. Wilton, Krystina B. Lewis and Matthew T. James in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors thank all patients and care providers who participated in meetings and interviews to develop the
ORCID iDs
Ethics Approval and Consent to Participate
The Conjoint Health Research Ethics Board (CHREB) of the University of Calgary provided approval for this study (Ethics ID: REB19-1244).
Consent for Publication
All authors consent to the publication of this report.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by Canadians Seeking Solutions and Innovations to Overcome; Chronic Kidney Disease (Can-SOLVE CKD) (No. 202112KMI-477469-KMI-CAAA-104780) from the Canadian Institutes of Health Research (CIHR) Strategy for Patient Oriented Research (SPOR) SPOR Networks—Knowledge Mobilization and Implementation Grant. Matching support for this project was provided by the Libin Cardiovascular Institute, Nephrology Research Group, and Roy and Vi Baay Chair in Kidney Research, University of Calgary.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Research materials related to this study may be requested from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.