
Abstract
Background:
Transplanting less-than-ideal (LTI) kidneys could help optimize organ utilization, but little is known about how patients and caregivers perceive the allocation process, waitlist, or LTI kidneys.
Objective:
To explore the perspectives of patients and caregivers on the Canadian kidney transplant allocation process, waitlist, and LTI kidneys.
Design:
Electronic survey.
Setting:
Canada.
Patients:
Transplant recipients, candidates, and caregivers.
Methods:
A bilingual electronic national survey was administered from January to March 2024. The questionnaire contained sections on demographics, perceptions of organ allocation and acceptance, LTI kidneys, and educational preferences. Descriptive analysis was performed.
Results:
Two hundred fifty-one responses were analyzed, including patients (63%, n = 159), and caregivers (37%, n = 92), from 11 provinces and territories. Three-quarters (74%, n = 186) understood how patients are placed on the waiting list, and 65% (n = 162) understood how donor kidneys are allocated, but 72% (n = 181) and 68% (n = 171) wanted more information about the waitlist and donor kidney allocation criteria, respectively. Approximately 20% felt that the waitlist and allocation processes were not transparent. Awareness about the option to refuse a deceased donor kidney offer was high (69%, n = 174), yet nearly half of respondents (46%, n = 115) expressed concern about being disadvantaged if an offer for a deceased donor kidney was refused. One-third of participants (33%, n = 83) were open to accepting an LTI kidney.
Limitations:
Compared to the general population, more study participants were white, and the majority were educated and financially at ease. This limits the generalizability of the results.
Conclusion:
Enhanced communication is required to improve transparency and information about the allocation system and waitlist in Canada.
Introduction
Transplantation has dramatically improved outcomes for people with kidney disease, yet patients continue to die on the waitlist and a concerning number of kidneys are discarded annually.1,2 In the United States as many as 1 in 5 kidneys from deceased donors are not transplanted. 3 One strategy for potentially augmenting the pool of available deceased donor kidneys involves transplanting organs from donors with characteristics indicative of potentially suboptimal long-term graft survival. 4 Various labels and definitions have been used for such kidneys (i.e., expanded donor criteria [ECD], extended criteria, marginal, high Kidney Donor Profile Index [KDPI], or less-than-ideal [LTI] kidneys). These kidneys may be of particular benefit for some patients; especially those who are older or have multiple comorbidities.5,6 When compared with remaining on dialysis, waitlisted patients have a survival advantage for accepting a LTI.7,8 For example, in a retrospective study using administrative data in the United Kingdom (n = 47 917) lower-all cause mortality was noted for those who received an ECD kidney (defined as deceased donor kidneys aged ≥60 years or aged 50 to 59 years with 2 from the following 3; hypertension; raised creatinine and/or death from stroke) compared with dialysis. 7 In Canada, deceased donor kidneys are primarily allocated within individual provinces, except for highly sensitized patients—those with a calculated panel reactive antibody (cPRA) score over 95%—who can access a national pool of organs. Organ donation organizations oversee the processes of identifying donors, procuring organs, and allocating them, considering factors such as dialysis duration, medical urgency, and pediatric priority. 9
The decision-making framework for transplant candidates regarding the acceptance or rejection of deceased donor kidneys—especially those that are LTI—necessitates a multifaceted approach encompassing ethical, medical, and personal considerations. This complex scenario requires an integrated strategy that emphasizes education, effective communication, and collaborative decision-making processes. Communication disparities can exist between healthcare providers and patients, supporting the call for improved dialogues to enhance patient comprehension of LTI kidneys.10,11 Our previous qualitative studies with patients and clinicians have highlighted the crucial role of transparency with respect to the decision-making process and underscored the need for targeted educational resources concerning the risks and benefits associated with LTI kidneys.10-12 Creating these resources, however, requires a thorough understanding of how patients and caregivers feel about decision making, LTI kidneys, and which patients would be interested in considering one. Moreover, we have a limited understanding on patient and caregiver perceptions of the current allocation and waitlisting process in Canada.
The purpose of this study was to survey transplant recipients, candidates, and caregivers regarding their perceptions of the allocation and waitlist process in Canada and their impressions of LTI kidneys.
Methods
A bilingual (English and French) electronic national study was conducted by way of a self-reported survey and guided by the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) framework. 13 An advisory committee consisting of 7 members (5 healthcare providers/researchers and 2 patient-family advisors) oversaw the project design and methods and advised on participant recruitment. Approval for the study was obtained from the University of Saskatchewan Behavioural Ethics Board (Beh 4210), Saskatchewan Health Authority, and the Centre hospitalier de l’Université de Montréal (CE23-149).
Recruitment
The population of interest included transplant recipients, candidates, and caregivers. Participants in this convenience sample were recruited through social media posts by transplant and kidney advocacy groups and organizations such as the Canadian Transplant Association, Kidney Foundation of Canada, and the Canadian Donation and Transplantation Research Program. Patients who were listed for a kidney transplant at the Centre hospitalier de l’Université de Montréal (CHUM) and the Saskatchewan Transplant Program were also invited to participate by way of an email and invitation letter, respectively.
Survey Development
The survey was developed by the advisory committee in English and then translated to French by a professional translator. It was input into the Research Electronic Data Capture (REDCap) platform and tested on 2 laypeople to confirm the functionality and ease of use. Filter questions were included to specifically identify kidney transplant recipients, candidates, and caregivers, and to exclude pediatric patients (i.e., those younger than 18 years). Respondents were anonymous to the research team and completion of the survey was taken as evidence of informed consent.
Data Collection
Data collection occurred between January and March 2024. A $10 gift card and invitation to participate in future studies were offered to respondents who filled out the survey; contact information was obtained through a separate survey to preserve the anonymity of the participants. Respondents were briefed on the concept of LTI kidneys; kidneys may come from donors who are older, have underlying medical conditions such as diabetes or high blood pressure, or have slightly decreased kidney function. The questionnaire contained a section on demographics and clinical situation; questions to assess understanding of organ allocation and acceptance (20 items); questions about LTI kidneys (8 items); and educational preferences (8 items), with each appearing as a separate page on the internet survey. To promote interprovincial sharing and optimize the use of LTI kidneys, Canadian Blood Services is considering the creation of a national registry for patients interested in receiving an LTI kidney. The last section of the questionnaire aimed to assess the respondent’s interest in joining a national LTI registry (Appendix A). A 5-point Likert scale was used to assess agreement with questions pertaining to organ allocation (i.e., how kidneys are offered and/or distributed when they become available) and decision making when a deceased donor kidney is offered. Adaptive questions were shown only to transplant candidates and recipients to assess the presence of dialysis, whether they preferred a support person to help with decision making, and for those who received a deceased donor kidney previously, whether they felt prepared and had enough time to decide (see Supplementary materials).
Data Analysis
Data were analyzed using IBM Statistical Package for the Social Sciences Statistics version 29 to report descriptive statistics and frequencies. Only completed surveys were analyzed. Likert scale questions for assessing perceptions on allocation and waitlist were recoded to the categories of “agree,” “neutral,” and “disagree” and reported according to patient and caregiver. To further assess perceptions of those who had an opinion other than neutral, the neutral category was removed and chi-square test of Independence was used to calculate relationships between those who “agree” or “disagree” and the demographic variables: age (≥50 or <50), location (Quebec versus the other locations combined), the highest level of education (up to high school completed or higher than high school), and annual income (≥100 K or less than 100 K). For questions about whether the participant would consider accepting an LTI kidney or participating in a national LTI kidney registry, location was categorized according to geography. (West = AB, BC, SK, MB; East = NB, NL, NS, PEI; North = territories. Ontario and QB were left as independent provinces since their sample size was large enough to stand alone.) A P-value less than .05 was considered statistically significant.
Results
Of 380 people who opened the questionnaire, 311 began answering the survey. The final dataset included 251 respondents from 11 provinces and territories in Canada. Quebec had the highest number of respondents (65%, n = 162), with just over half (54%) completing the survey in French. Approximately two-thirds of the respondents were patients (63%, n = 159), while the rest were caregivers (37 %, n = 92). Missing data primarily consisted of people who started or competed Section 1 (demographics) (42%, 25/60) or Section 2 (50%, 30/60).
Section 1: Demographics
Among the patient participants, the majority (68%, 108/159) had received a kidney transplant, with the remainder waiting (23%, 36/159) or considering a transplant (9%, 14/159). Approximately two-thirds of the patients with transplant (62%, 67/108) received their kidney from a deceased donor. Among the patients who were considering or waiting for a transplant, three-quarters of respondents were on dialysis (76%, 38/50), with hemodialysis being the most common modality (n = 24), followed by peritoneal dialysis (n = 13). Participant demographics are shown in Table 1.
Participant Demographics.

Answers may not add up to 100% because respondents could choose more than one answer
Section 2: Questions to Assess Understanding of Organ Allocation and Acceptance
Respondents indicated a substantial level of understanding about both organ allocation and acceptance, with 74% (n = 186) and 65% (n = 162) agreeing they understood how patients are placed on the waitlist and how deceased donor kidneys are allocated, respectively. Nevertheless, a significant portion of respondents expressed a desire for more information about both the waitlist placement (72%, n = 181) and the allocation of deceased donor kidneys (68%, n = 171). Furthermore, less than half of the participants (41%, n = 103) knew where to find more information about listing and allocation criteria. Figure 1 presents perceptions on allocation and waitlist according to patient and caregiver.
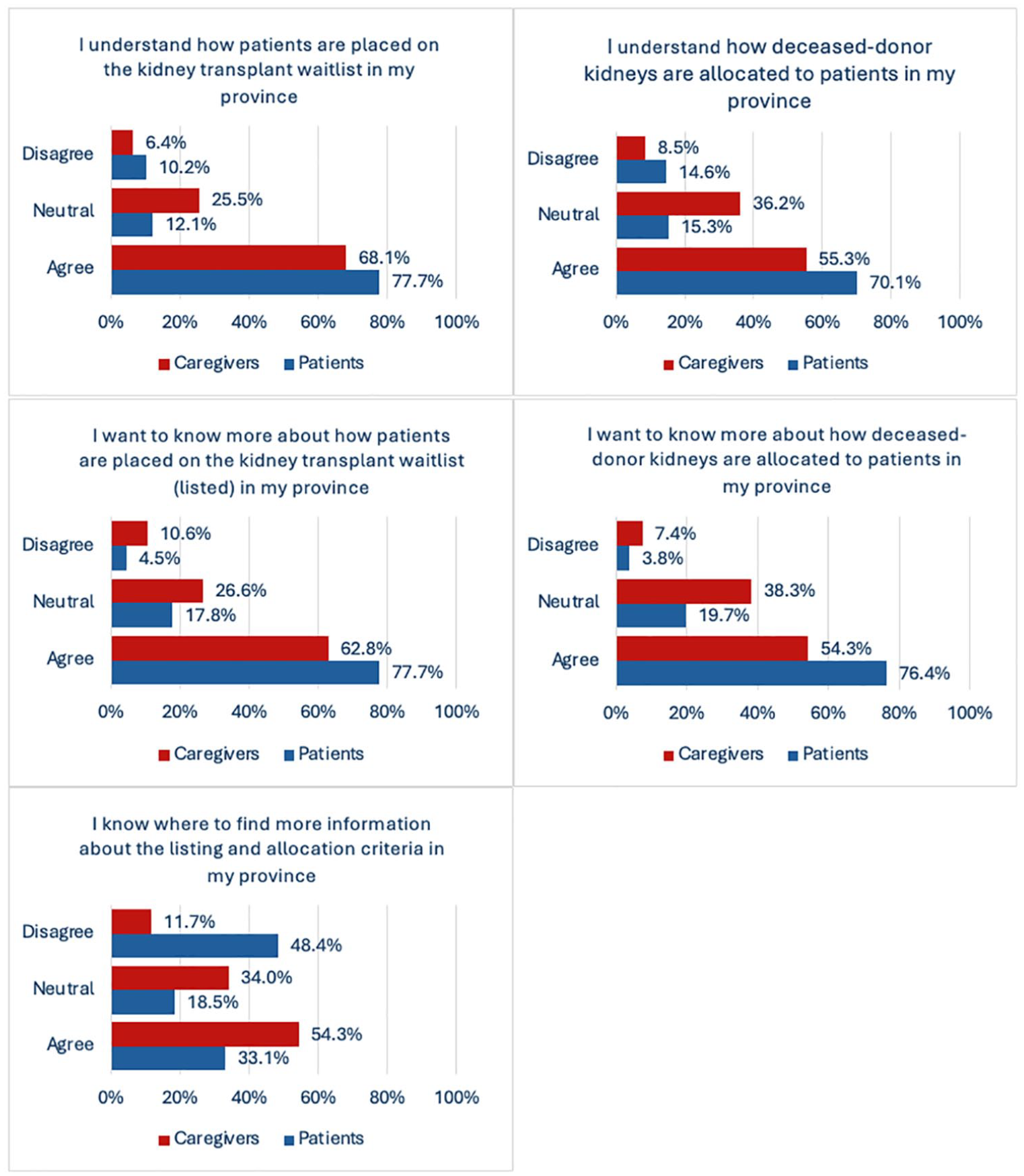
Perceptions on allocation and waitlist according to patient and caregiver.
Approximately 20% of the respondents felt that the waitlist (19%) and allocation processes (21%) in their province were not transparent. Free-form questions about whether the respondents had further questions about the waitlist and allocation processes indicated that they were seeking transparency, clarity, and efficiency. Some expressed frustration with the perceived slowness and lack of clear communication. Respondents had a broad variety of questions and comments about how the allocation criteria and the waitlist process work, which are presented in Table 2. Figure 2 presents perceptions of transparency according to patient and caregiver. Demographic variables including age, income, education level, and location were not associated with these questions.
Respondent Questions and Comments About the Waitlist and Allocation Criteria.


Perceptions on transparency according to patient and caregiver.
The trust in physicians was notably high, with (72%, n = 180) of respondents trusting their physician to make decisions about accepting a deceased donor kidney (Figure 3). In contrast, almost half of the patient respondents (49%, n = 78/159) disagreed that they required help from a support person or caregiver to make this decision (Figure 4). When asked who the preferred individual was to have discussions about accepting or declining a deceased donor kidney with, respondents preferred the transplant team (28%) followed by the transplant nephrologist (18%). Respondents who were at least 50 years old (χ2 (1, n = 195) = 7.5, P = .006) and respondents from Quebec (χ2 (1, n = 195) = 9.5, P = .002) were more likely to agree that they trusted the physician to make the decision about whether to accept a deceased donor kidney.

Perceptions on trust and involvement in decision-making according to patient and caregiver.
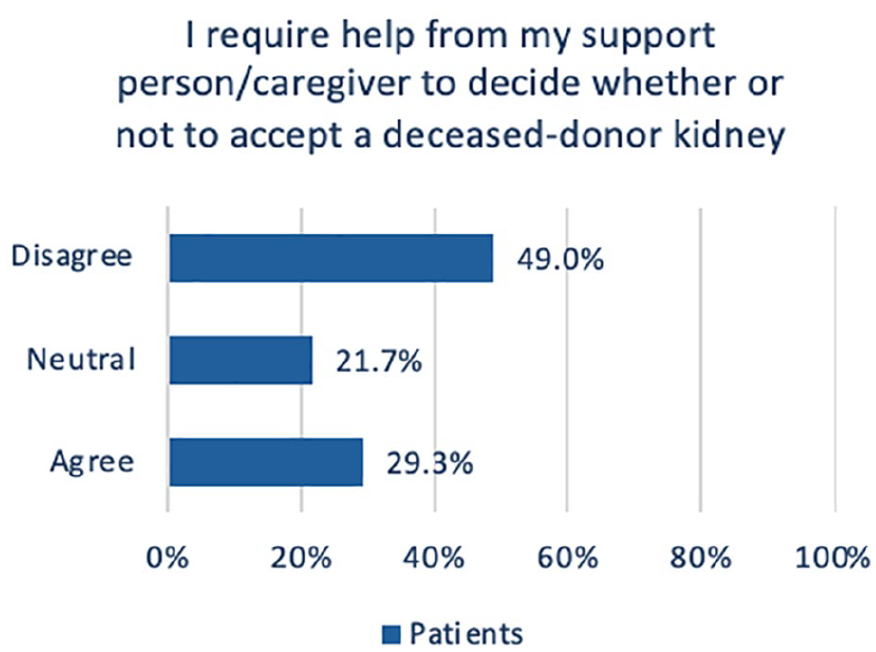
Patient perceptions on caregiver support with decision making.
Awareness about the option to refuse a deceased donor kidney offer was high (69%, n = 174), yet nearly half of respondents (46%, n = 115) expressed concern about being disadvantaged or removed from the waiting list if an offer for a deceased donor kidney was refused (Figure 5). This agreement of concern was higher in respondents from Quebec (χ2 (1, n = 183) = 6.7, P = .01). For those who received a deceased donor kidney offer, only a small percentage felt unprepared (3%, n = 7) or needed more time to decide (2%, n = 6).

Perceptions on refusing a deceased donor kidney offer according to patient and caregiver.
In terms of informed decision-making, respondents indicated a strong desire to be informed about the donor’s medical conditions (86%), risk of infection (83%), age group (78%), lifestyles (61%), and duration of kidney function (56%) when receiving a kidney offer. In the free-form text box, 3 participants also added compatibility and cause of death. When asked whether the respondents had questions about shared decision making, the most common questions were about the implications of being offered a deceased donor kidney and then refusing it. When considering what details might change their decision to accept a kidney, respondents most frequently cited the risk of infection (65%), medical conditions (55%), duration of kidney function (45%) and the donor’s age group (33%), as the critical factors in patients’ decision-making processes.
Section 3: Questions About LTI Kidneys
Participants were surveyed on their knowledge and acceptance of LTI kidneys. Nearly half (46%, n = 116) indicated that their transplant team had discussed the concept of LTI kidneys, while the rest either had not had such discussions (42%, n = 106) or couldn’t recall (12%, n = 29).
One-third of participants (33%, n = 83) were open to accepting an LTI kidney. A significant portion of respondents were either uncertain (30%, n = 76) or stated that their decision would depend on specific circumstances (20%, n = 50). Perceived risks of accepting an LTI kidney identified in free-form text included concerns about the functionality and potential complications (n = 88), fear of organ rejection and its implications (n = 24), concerns about a shortened lifespan of the kidney (n = 21), potential worsening of health and increased medical complications (n = 16), potentially having to return to dialysis if the kidney fails (n = 8), and inherent risks associated with undergoing transplant surgery (n = 8). When asked “Do you have any concerns about considering an LTI kidney transplant? If so, please describe,” worry about potential complications and the longevity of the kidney was most commonly described (n = 48). Others expressed concern regarding how healthy the LTI kidney is (n = 26) or that the kidney may not last long or may be rejected (n = 16). Concerns were mentioned regarding donor’s health leading up to their death (n = 8). Some respondents were looking for an assurance of a better quality of life (n = 20) or indicated they wanted to understand more before deciding (n = 6).
When asked about participating in a national registry for LTI kidneys, (45%, n = 113) of respondents indicated willingness. However (17%, n = 42) were against it, and a considerable number of participants (38%, n = 96) were unsure or indicated that their decision would depend on the circumstances. Statistically significant differences were noted in the respondents between above and below the cutoff of 50 and in location, but not education level or income. The results are shown in Tables 3 and 4.
Perceptions on Accepting a Less-Than-Ideal and Participating in a National Registry According to Age.

Perceptions on Accepting a Less-Than-Ideal and Participating in a National Registry According to Location.

AB = Alberta; BC = British Columbia; SK = Saskatchewan; MB = Manitoba; ON = Ontario; QB = Quebec; NB = New Brunswick; NL = Newfoundland; PEI = Prince Edward Island.
Participants were asked to rate how important various factors were about decision making whether to accept an LTI kidney on a Likert scale ranging from 1 to 10, where 1 indicates an aspect is “not at all important” and 10 signifies it is “very important.” Factors that were perceived to be the most important were current experience with dialysis or chronic kidney disease and donor factors. Responses are presented in Table 5.
Perceived Importance of Factors Related to Decision Making on Whether to Accept a Less-Than-Ideal Kidney Rated on a Likert Scale of 1 (Not at All Important) to 10 (Very Important).

Factors that would lead a respondent toward considering an LTI kidney were also derived from the free-form text. The most common responses were health status or how a person was managing on dialysis (n = 13), age (n = 8), quality or expected longevity of the LTI kidney (n = 7), and time spent waiting (n = 4). Perceived benefits of accepting an LTI kidney included the potential to stop dialysis (n = 53), improvements in quality of life (n = 20), the potential opportunity for a longer life without dialysis (n = 12), and a quicker match or only match for certain patients (n = 8). Some respondents expressed doubt and saw no benefits (n = 11).
Section 4: Questions About Educational Preferences on LTI Kidneys
Participants were asked about the information they would want if a new registry for LTI kidneys was created in free-formed text. Participants expressed a desire for information that allowed for comparison between LTI and standard kidneys (e.g., pros and cons of each option, advantages and risks (n = 25); the need to understand the possible problems post-transplant (n = 20); an interest in knowing the donor’s history), including health and lifestyle (n = 19) and wanted answers about the success rates of transplants with LTI kidneys (n = 16).
The majority of respondents expressed a preference to learn more about LTI kidneys and a registry at their transplant clinic (54%, n = 136), followed by the dialysis clinic (30%, n = 75). Some suggested information on a website would also be helpful. Most respondents wished to learn about LTI kidneys as soon as they decided to have a kidney transplant (n = 6%, n = 167) or during the pre-transplant assessment (54%, n = 135). Discussions with the transplant team were the most preferred method of learning (75%, n = 187), and the transplant doctor was the most preferred source (49%, n = 124), followed by the nephrologist or dialysis doctor (14%, n = 35) (Table 6).
Educational Preferences for Education About Less-Than-Ideal Kidneys and a National Registry.

Totals will not add up to 100% since respondents could choose more than one response.
Discussion
This survey of patients and caregivers provided insight into the perceptions regarding organ allocation and acceptance. While most respondents (74%) indicated they understood how patients are placed on the kidney transplant waitlist, and how deceased donor kidneys are allocated (65%), nearly the same amount expressed a desire for more information. Less than half knew where to find more detailed information about these processes, highlighting a crucial gap in accessible resources or communication from transplant organizations. 14
Transparency emerged as a critical concern, with approximately 20% of respondents perceiving the waitlist and allocation processes as lacking transparency. Such perceptions could arise from the complexities and variability inherent in the transplant system, which may not be fully communicated to patients and caregivers. 15 In a recent qualitative study in Quebec (n = 14), patients between 64 and 75 years with chronic kidney disease G4-5 generally perceived the allocation criteria to be fair. 16 However, in a cohort of waitlisted and kidney recipients in the United Kingdom (n = 36), some participants expressed concerns about how kidneys are allocated. 17 In the United States, concerns about the transparency of the transplant process were also identified by the general public. 18 Such concerns were not without consequence; participants who believed the allocation was “unfair” or were “unsure” about fairness were less willing to donate organs. 18
In the present study, high awareness about the option to refuse a deceased donor kidney offer was reported (69%), yet nearly half of the respondents (46%) expressed concerns about potential repercussions, such as being disadvantaged or removed from the waiting list if they refuse an offer. This highlights the need for clearer policies or reassurances from transplant authorities to ensure patients feel secure in their ability to make informed choices without fear of penalty.
Despite the mixed perceptions, trust in physicians remained notably high, indicating a strong relationship between patients and their transplant physicians. Similar results were noted in our previous qualitative study with kidney transplant recipients and transplant candidates, where trust in the medical team emerged as a common theme. 11 Consistent with other literature, older respondents were more likely to trust their physician with decision-making, 19 and patients and caregivers wanted to be involved in the decision-making process about organ acceptance.11,20,21 When it comes to making an informed decision about accepting a kidney offer, participants rated the donor’s medical conditions (86%), risk of infection (83%), and the age group of the donor (78%) as the most important factors. This shows a well-considered approach, prioritizing health, and long-term outcomes in their decision-making process.
The willingness to accept LTI kidneys was notably low, with a third (33%) open to this option and another third being uncertain (30%). Less-than-ideal kidneys may benefit specific groups of patients such as those who are older or with multiple comorbidities and generally would not be a consideration for young transplant candidates. Interestingly, in the present study, participants who were younger than 50 were more likely to express an interest in LTI kidneys. This finding highlights the need for better educational materials that clearly articulate the risks and benefits associated with LTI kidneys and the populations that are most likely to benefit from them. Under half of the respondents (46%) indicated that their transplant teams had discussed the concept of LTI kidneys, which raises concerns about the consistency and effectiveness of communication practices across transplant centers. Enhancing uniformity in discussing all potential transplant options, including LTI kidneys is crucial for informed decision-making and facilitating trust in the transplant process. Second to discussions with the transplant team (i.e., transplant physician), respondents indicated a preference for information booklets and video education to learn about LTI kidneys. Standardizing educational materials across the country could facilitate uniformity in messaging.
The limitations of this work deserve consideration. We achieved responses from patients and caregivers across the country, but there was a higher representation of respondents from Quebec. Notable differences were found within Section 2 of the survey (questions about organ understanding and allocation) which suggests there may be regional differences and that results may not be generalizable across the country. Selection bias could also have played a role as some programs have lower rates of living donors, and there is an increased reliance on deceased donor kidney transplants. Eighty-five percent of the sample was white, and the majority were educated and financially at ease. This contrasts with our Canadian population, where approximately 70% reported being white22. Given the well-documented disparities in access to transplantation with marginalized populations23,24 perceptions on kidney allocation, the waitlist, and LTI kidneys may vary. Furthermore, candidates who are ethnic minorities may not have access to social media and/or may not have been able to reply in French or English, which would have been missed in this study. We suggest a fulsome evaluation of this topic from the perspective of marginalized populations. For optimal contextualization of the responses, we opted to analyze only the complete surveys. However, this required the exclusion of 35 respondents who provided partial responses to sections 2 and 3 (12%). Finally, since the survey was anonymous and an incentive was offered through an unlinked survey, there is the possibility that surveys were completed more than once by the same respondent or by a respondent who was not a kidney transplant patient or care partner.
Conclusions
Patients and caregivers expressed a substantial level of understanding about organ allocation and acceptance, but many expressed concerns with the process, LTIs and an LTI registry. Enhanced communication is required to improve transparency about the allocation system and waitlist in Canada and facilitate decision making about deceased donor kidneys.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251324608 – Supplemental material for Patient and Caregiver Perceptions on the Allocation Process and Waitlist, and Accepting a Less-Than-Ideal Kidney: A Canadian Survey
Supplemental material, sj-docx-1-cjk-10.1177_20543581251324608 for Patient and Caregiver Perceptions on the Allocation Process and Waitlist, and Accepting a Less-Than-Ideal Kidney: A Canadian Survey by Marie-Chantal Fortin, Fabian Ballesteros Gallego, Héloise Cardinal, Manpreet Kaur, Rahul Mainra, Sylvain Patoine, Nicola Rosaasen and Holly Mansell in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to acknowledge the help and support of their friend and colleague, Mary Beaucage. Her dedication and unwavering commitment to creating a better world for those affected by kidney disease will never be forgotten. The authors would also like to thank Gabriela Loureiro and Ryan Chan for their help with data collection and writing, respectively.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the Canadian Society of Transplantation (CST) T3 Competition in Transplantation and Donation, with support from Paladin Labs Inc and Astellas Pharma Canada.
Ethics Approval and Consent to Participate
Approval for the study was obtained from the University of Saskatchewan Behavioural Ethics Board (Beh 4210), Saskatchewan Health Authority, and the Centre hospitalier de l’Université de Montréal (CE23-149). Completion of the survey was considered implied consent.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
No primary data is presented in this publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.