
Abstract
Background:
Quantifying the number and proportion of people with kidney failure (KF) who receive conservative kidney management is vital for health care system benchmarking and planning. It is not easy to ascertain this value precisely at the population level, but we can approximate it using information from different data sources to estimate the proportion of patients with advanced kidney disease who die without receiving dialysis or a transplant and should receive conservative kidney management.
Objective:
To approximate the proportion of people with KF in Ontario, Canada, who die without receiving kidney replacement therapy.
Design:
A review of unpublished provincial renal agency reports of 3 retrospective population-based cohorts combined with clinical interpretation.
Patients:
The 3 cohorts of people were: 1. those who died between January 1, 2013 and December 31, 2017, with an estimated glomerular filtration rate (eGFR) <10 mL/min/1.73 m2 and no evidence of receiving kidney replacement therapy; 2. those who initiated outpatient maintenance dialysis or received a preemptive transplant in the same period; and 3. those with a sustained low eGFR ≤ 10 mL/min/1.73 m2 between April 1, 2015 and March 31, 2018, and were followed for 1 year to determine if they started dialysis. In this last cohort, patients whose kidney function improved (evidence of an eGFR > 10 mL/min/1.73 m2) or who received a transplant during follow-up were excluded from the analysis.
Measurements and Methods:
The 3 cohorts were derived at ICES and used linked health care databases for the province of Ontario, Canada. In 2016, Ontario had a population of about 14 million people. Two nephrologists reviewed the data to provide the clinical approximation.
Results:
There were 1891 individuals with KF who died without kidney replacement (the no KRT cohort). The median (25th, 75th percentile) eGFR prior to death was 7 (5, 8) mL/min/1.73 m2. During the same period, 13 511 individuals started dialysis or received a preemptive kidney transplant (the KRT cohort). There were 7259 individuals in the low eGFR cohort; over the following year, 66% started dialysis, 20% died without dialysis, and 14% were alive without starting dialysis. The clinical approximation is that between 13 and 16% of people with KF die without receiving kidney replacement therapy.
Limitations:
The data reports lacked certain information to inform the clinical approximation. There was no information on the conversations health professionals had with people about kidney replacement therapy, any decisions made about receiving conservative care, or the circumstances that preceded death without kidney replacement therapy.
Conclusions:
After reviewing data from the 3 cohorts, we clinically approximate that 1 in 6 people with KF in Ontario, Canada, die without receiving dialysis and should receive conservative kidney management.
Introduction
Over the past decade, more attention has been given to conservative kidney management (CKM) which is defined as care for people with kidney failure (KF) that focuses predominantly on providing kidney supportive care to promote quality of life but does not include kidney replacement therapy (KRT).1 -5
Although KRT helps most people live longer than CKM, the survival advantage does not consistently extend to those who are older (>75-80 years old) or those with high comorbidity (Charlson comorbidity index >8). 4 ,6 -8 In some people, receipt of KRT, compared to CKM, is associated with higher hospitalization rates, higher care costs, and lower satisfaction with life.7,9
In 3 international surveys of nephrology stakeholders in 165 to 183 countries, 61% to 81% of respondents reported that CKM was available in some form, whether through shared decision making or choice restricted CKM.10 -12 However, the proportion of people with KF who receive CKM in countries that offer this care is challenging to determine. In studies addressing this issue, the definition of CKM varies, ranging from those who decide to pursue it early in the progression of kidney disease, to patients with an eGFR below a specific threshold who are not receiving dialysis.6,13,14 Better information on how frequently individuals with KF receive CKM relative to KRT is vital for health care system benchmarking and planning, and to ensure the resources required to provide this therapeutic option are available to people who would prefer it.
The primary objective of this publication is to approximate the proportion of people with KF in Ontario, Canada, who die without KRT, and therefore would benefit from receiving CKM. It is difficult to ascertain this value precisely at the population level, but it can be approximated by ascertaining the proportion of individuals with KF that die without receiving KRT. The secondary objective is to describe the characteristics and health care utilization of individuals with KF who died without receiving KRT in Ontario and contrast them to individuals with KF who initiated KRT during the same period.
Methods
Study Design and Setting
Two nephrologists reviewed data in 3 unpublished reports previously assembled for the provincial renal agency (the Ontario Renal Network) for internal purposes.
The reports used linked administrative health data and comprised 3 different population-based cohorts of individuals with KF in Ontario, Canada. Ontario is Canada’s most populous province with a population of ~14 million in 2016. 15 All Ontario residents have universal access to insured hospital and physician services. Ontario residents over 65 years of age or those receiving social assistance also receive universal prescription drug coverage, which allows for the assessment of outpatient medication dispensing. The use of data in the reports and this publication was authorized under section 45 of Ontario’s Personal Health Information Protection Act, and the Research Ethics Board did not require additional review. In this publication, we followed the Reporting of studies Conducted using Observational Routinely collected health Data guidelines (see Supplemental Appendix A). 16
Data Sources
In the reports, patient characteristics, receipt of maintenance dialysis and outcomes were obtained from 16 health databases at ICES (ices.on.ca). Detailed information on the datasets used in this study can be found in Supplemental Appendix B. These datasets were linked using unique encoded identifiers and analyzed at ICES.
KF Cohorts
Cohort 1: no KRT cohort
This was a cohort all those who died in Ontario between January 1, 2013, and December 31, 2017. After standard data cleaning, people with the following characteristics at the time of death were excluded: <18 years of age, evidence of dialysis in the prior 6 months, a vascular access created for hemodialysis in the preceding 6 months, a history of kidney transplantation, no serum creatinine measurement in the preceding year, or an eGFR persistently greater than 10 mL/min/1.73 m2. To ensure that the low eGFR was sustained, the cohort was restricted to those who had at least 2 eGFR measurements ≤10 mL/min/1.73 m2 separated by at least 2 weeks apart in the preceding year, where the last eGFR before death was less than 10 mL/min/1.73 m2. See Supplemental Appendix C for more details of the cohort build.
Cohort 2: KRT cohort
This was a cohort of individuals in Ontario who started maintenance dialysis or received a preemptive kidney transplant between January 1, 2013, and December 31, 2017 (the same period as above). After standard data cleaning, individuals with the following characteristics were excluded: those <18 years of age and those with evidence of prior KRT (either previous dialysis or kidney transplant). See Supplemental Appendix D for more details of the cohort build.
Cohort 3: low eGFR cohort
This was a cohort of individuals in Ontario, Canada, who had 2 eGFR values ≤10 mL/min/1.73 m2 separated by at least 2 weeks between April 1, 2015, and March 31, 2018. After standard data cleaning, individuals with the following characteristics were excluded: < 18 years of age, or a history of kidney transplantation or maintenance dialysis. Individuals were followed for 1 year, and those who had an eGFR >10 mL/min/1.73 m2or received a kidney transplant were also excluded. See Supplemental Appendix E for more details about the cohort build. After 1 year, individuals were categorized into 4 mutually exclusive groups: death without dialysis (consistent with our previous definition of no KRT), death after initiating dialysis, alive and receiving dialysis, or alive without having received dialysis.
Patient Characteristics
Baseline characteristics for the first 2 groups were assessed using the codes in Supplemental Appendix F. Two nephrologists reviewed this information to contrast the types of individuals with KF who died without KRT versus those who initiated KRT.
Health Care Use
Several measures of healthcare use in the 6 months before death were examined in the no KRT cohort. These measures included: location of death; hospitalization in the 30 days prior to death; intensive care unit (ICU) admission in the 30 days prior to death; emergency department visit in the 14 or 30 days prior to death, home visits in the 6 months prior to death, palliative care in the 6 months prior to death, and physician house calls in the 2 weeks prior to death. Several composite indicators were also examined: (1) aggressive care in the 30 days prior to death (defined as 2 emergency department visits, hospital admission or ICU admission) and (2) supportive care in the 6 months prior to death (defined as a physician house call in the last 2 weeks of life, or a palliative nursing or personal support worker home visit in the last 6 months prior to death). See Supplemental Appendix G for full definition details.
Statistical Analysis
Continuous variables are presented using mean (standard deviation; SD) or median (25th, 75th percentile) and categorical measures as frequency (proportion). Quality-of-care indicators for the no KRT cohort are expressed using proportions. The population at risk varied by indicator and is detailed in Supplemental Appendix G.
All analyses at ICES were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
Clinical Estimate
Using data from the 3 cohorts 2 nephrologists (AC and PB) calculated the proportion of individuals with KF who died without dialysis. Confidence intervals were calculated using the Exact Interval using R version 4.3.3.
Results
Cohorts 1 and 2: No KRT and KRT
There were 1891 individuals who died with KF without KRT (the no KRT cohort). On average, the last eGFR value was taken 24 days prior to death and the median (25th, 75th percentile) value was 7 (5, 8) mL/min/1.73 m.2 It should be noted that during the study period all outpatient laboratories, but not all hospitals contributed laboratory data to centralized databases. As a result, patients who had their bloodwork done exclusively at specific hospitals would not be included in this cohort.
During the same period, 13 511 individuals started dialysis or received a preemptive kidney transplant (the KRT cohort).
Select demographics and comorbidities of these 2 groups are shown in Table 1 (full baseline characteristics can be found in Supplemental Appendix H). No statistical comparisons were performed. As expected, individuals in the no KRT cohort were older than those in the KRT cohort (84 vs 65 years old). . They were more likely to be female (58% vs 38%) and had a greater degree of comorbidity. They more frequently lived in long-term care (26% vs 1%) and were more likely to have a record of dementia (42% vs 7%). On average, they were prescribed more types of medications (13 vs 10) but were less likely to receive antihypertensive medications, including RAAS blockers, beta blockers, and calcium channel blockers.
Selected Baseline Characteristics of the No KRT and KRT Cohorts.

Healthcare use
Eighty-four percent of those who died without KRT saw a nephrologist in the last year of life, with an average of 9 inpatient or outpatient nephrologist visits. Individuals who started dialysis or received a preemptive kidney transplant had 20 nephrology visits in the prior year.
Of the individuals who died without KRT (the no KRT cohort), 44% died while admitted to an acute care hospital or emergency department, 3% died in the ICU, and 20% died in long-term care. In the 30 days prior to their death, 63% received aggressive care (defined as a hospitalization, ICU admission or 2 emergency room visits). Sixty-five percent (65%) received palliative care services in the 6 months prior to death, which included both hospital and home-based palliative care.
In those who died without KRT, 65% were using opiates, and 31% were using benzodiazepines, suggesting a high symptom burden in this group. Conversely, almost half (48%) were taking statins, indicating the possibility of missed opportunities for deprescribing in the patients who were pursuing CKM.
Cohort 3: Low eGFR
There were 7259 individuals in the low eGFR cohort (individuals with 2 eGFR values <10 mL/min/1.73 m2 separated by at least 2 weeks, who were not receiving KRT, and did not have any subsequent improvement and did not receive a kidney transplant within the following year). Two hundred and eight patients were excluded from the cohort after receiving a kidney transplant. After 1 year, most of the cohort (59%) were alive and had started maintenance dialysis, while 20% died without receiving KRT (see Table 2). Fourteen percent of the cohort was alive without having received dialysis, while 7% received dialysis and subsequently died within a year of follow-up.
One-Year Outcomes of the Low eGFR Cohort.

Approximation of the Proportion of Individuals With KF Who Die Without Receiving KRT
Cohort 1 (no KRT cohort) had 1891 individuals, and cohort 2 (KRT cohort) had 13 511 individuals. Acknowledging several limitations, including that the cohorts were assembled in different ways (limitations detailed in Supplemental Appendix I), using these data, the proportion of individuals with KF who died without KRT is [1891 / (1891 + 13 511)] = 12.3%. As provincial laboratory values were incompletely captured during the study period (information needed to construct cohort 1), this proportion is considered an underestimate.
Cohort 3 (low eGFR cohort) only included individuals with available laboratory data. The proportion of individuals who died without receiving dialysis was 23%, a value that was consistent over 3 years (Table 3). However, this proportion is limited due to the lack of inclusion of those who start dialysis with an eGFR >10 mL/min/1.73 m2 in the denominator and is considered an overestimate. Taking this into account, the clinical approximation of the proportion of individuals with KF who die without KRT from this cohort is 16%. (see Supplemental Appendix J for further explanation on how this approximation was derived).
Estimated Proportion of Patients Receiving Conservative Care in All Three Cohorts and by Year.
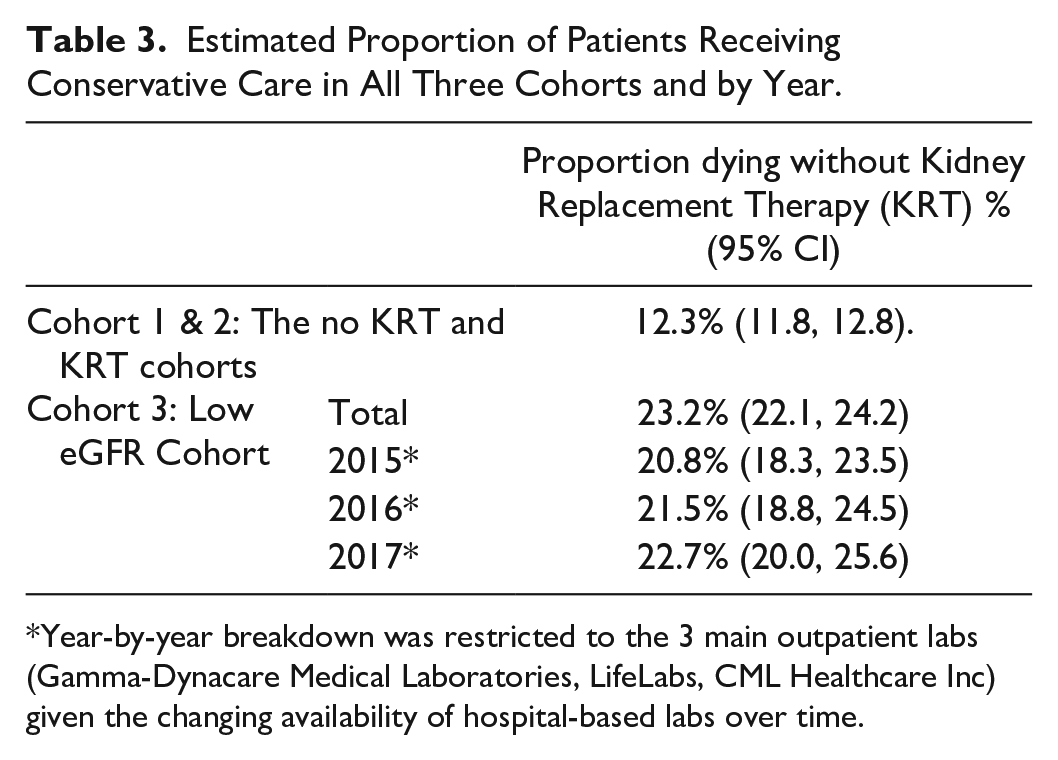
Year-by-year breakdown was restricted to the 3 main outpatient labs (Gamma-Dynacare Medical Laboratories, LifeLabs, CML Healthcare Inc) given the changing availability of hospital-based labs over time.
Discussion
Using 3 cohorts from Ontario in combination with clinical knowledge, we estimate the proportion of KF patients dying without KRT was 12.7% or 16%, with the true value likely in between these 2 estimates. The former estimate is likely an underestimation due to limitations with lab availability. Conversely, the second estimate required adjustment for those patients who received KRT with an eGFR >10 mL/min/1.73 m2 and is imprecise.
The proportion of individuals dying without KRT in our cohort is comparable to reports in the literature about rates of patients dying without dialysis or choosing CKM in high income countries. In a survey, European nephrologists estimated that around 15% of their patients received conservative care, while 2 single center studies from the United Kingdom found 15% to 18% of individuals approaching KF received palliative or conservative management.6,13,20 Two other studies however found higher rates of patients with advanced kidney disease not receiving dialysis. One Australian study examining death registry data found that 44% of all people with “kidney disease” or KF as the main or contributing cause of death did not receive dialysis. However, this likely included individuals with acute kidney injury. 21 A cohort from Alberta, Canada, found that approximately 50% of those whose eGFR decreased below 15 mL/min/1.73 m2 did not receive dialysis, however it is unknown whether this is the result of choosing CKM or an absence of indications to initiate KRT. 22
Our data show that approximately 1 in 6 Ontarians with KF die without receiving dialysis, meaning they should have been provided access to CKM. This includes kidney supportive care, focused on improving quality of life, as well as management of disease progression and its complications as far as it aligns with the patients priorities. 5 We found that 84% of the people who died without KRT saw a nephrologist at least once as an inpatient or outpatient in their last year of life (68% saw a nephrologist ≥3 times) suggesting an opportunity to implement kidney supportive care, and almost 2 thirds of participants received palliative care services in their last 6 months of life. Despite this, 62% of the no KRT cohort was hospitalized in their last month of life, similar to rates described in the literature.8,23 The proportion of individuals without KRT who died in hospital is also similar to previously described cohorts, with in-hospital death occurring in 27-68% of individuals. 24 Although this is lower than those who received KRT, and given that a hospital-based death is preferred in a minority of patients, this highlights a need to develop better systems for managing end of life outside of an acute care setting.24,25 In our study, we observed 1891 patients with KF who died without KRT over a 5-year period. Assuming the population remained steady at 13 448 494 (the population at the time of the 2016 census) 26 this corresponds to an approximate annual rate of dying without KRT of 28 per million population (pmp) compared to an KRT rate of 208 pmp in Ontario. 27 In comparison, the Australian study discussed above had a rate of dying without KRT of 94 pmp, and an KRT rate of 105 pmp, 21 suggesting that KRT rates, which are commonly reported, could be significantly influenced by rates of those who die without KRT in addition to being influenced by the prevalence of kidney disease.
As expected, individuals in the cohort who died without KRT were older and had more comorbidity than those who received KRT. These characteristics are consistent with previously described CKM cohorts, and align with the demographics of individuals who have been shown to have little or no survival advantage with dialysis. 5 ,24 -26 Although the index events differed by cohort (death vs dialysis start), these reflect important and definitive points in the care trajectory of individuals with KF. By choosing these as inclusions, we acknowledge that the KRT cohort was observed slightly earlier in their disease progression (which was confirmed by their 3 mL/min higher median eGFR) which may have contributed modestly to their appearance as younger with fewer comorbidities compared to those who died without KRT. However, it also eliminated any potential changes in treatment decisions that may happen prior to a definitive endpoint and ensured that only individuals who died without KRT or initiated KRT were included in the study. A recent meta-analysis of approximating the survival of patients who chose CKM found the median survival after reaching an eGFR <10 mL/min/1.73 m2 ranged from 6 to 16 months. 14 As a result, while we would expect some of the differences in baseline demographics observed between the no KRT and KRT groups (eg, older age and high burden of comorbidities) to be as a result of the differences in the cohort entry it would not fully explain these very large differences. It is likely that these differences were present at the time that patients were making the decisions about KRT and may have influenced those decisions.
Previously published cohorts comparing patients who chose CKM to those who elect to pursue dialysis have also shown similar striking differences in age, and comorbidity burden, even when the 2 groups are compared earlier in the disease process, such as at the time the decision to pursue CKM was made.6,13,14,20,28 One of the important demographic differences in our study was the prevalence of dementia in the no KRT group compared to the KRT group. Although some of this may have to do with the significant age difference in the 2 groups (as age is one of the biggest risk factors for dementia), this factor has previously been identified in the literature as being important both to nephrologists advising patients about CKM, and patients at the time of decision making around dialysis versus CKM.20,29
We also observed that those who die without KRT are more commonly women, in contrast to the higher proportion of men receiving KRT that we observed, which aligns with existing literature.17,18 It has previously been reported that women may be more likely to choose CKM.17,19 Alternatively, this may reflect the eGFR formula which gives women and older people a lower eGFR value for a given serum creatinine or may reflect the fact that women have a longer life expectancy than men so make up a larger proportion of a cohort of older adults.19,30 These issues have been discussed in detail in the recent literature but there is no clear consensus.17,19,30
Our study has several strengths.8,23,24 The unpublished reports we reviewed defined kidney function using laboratory data rather than administrative codes to increase sensitivity. We did require 2 eGFR measurements ≤10 at least 2 weeks apart to limit the inclusion of acute kidney injury (AKI), however we do acknowledge that this may have included some patients with AKI who were slow to recover. 31 They included a large number of individuals across a large geographic region to encompass practice variations across centers in the province of Ontario. They also required a definitive event such as death without dialysis or receiving KRT which avoided the inclusion of individuals who were undecided or might change their mind about their care path. However, because of this, the dates of cohort entry were different between the 2 groups, resulting in some confounding that needs to be carefully considered when describing the different cohort characteristics. For example, those who died without KRT were likely further along in their disease progression, older and more likely to have comorbidities that are associated with older ages. There are several limitations to the approximation of the proportion of individuals dying without receiving KRT. In the comparison of the first and second cohorts, only the first was defined by laboratory values. On December 31, 2017, laboratory data from hospitals covering 61% of the Ontario population were available in OLIS, while 100% of outpatient laboratories were available through OLIS for the entire study period. 32 Given that the no KRT cohort was defined by laboratory values, our proportion is likely an underestimation as individuals who exclusively had their bloodwork done at certain hospitals would not be included in the cohort. However, in individuals who have chosen CKM, it is possible that they might be more likely to use community-based labs which were readily available. There are also limitations to the proportionality between eGFR and the true degree of kidney failure and of symptomatic uremia. Although our cutoff for KF (eGFR ≤10 mL/min/1.73 m2) was lower than some reports in the literature to increase the specificity for those who died from kidney disease, it is possible that individuals who fell into this category may have died from other causes that would not have been reversed by dialysis initiation.
Further research is needed to determine the proportion of patients who die without KRT, having actively chosen CKM and to determine the factors that affect patients’ decision making.
Conclusion
After reviewing the data from 3 cohorts derived from Ontario’s administrative data, we estimate that 1 in 6 of individuals with KF die without KRT, which indicates that they should be receiving CKM.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251323961 – Supplemental material for Approximating the Proportion of Individuals With Kidney Failure Who Die Without Kidney Replacement Therapy in Ontario, Canada
Supplemental material, sj-docx-1-cjk-10.1177_20543581251323961 for Approximating the Proportion of Individuals With Kidney Failure Who Die Without Kidney Replacement Therapy in Ontario, Canada by Andrea C. Cowan, Nivethika Jeyakumar, Amit X Garg, Stephanie Dixon, Bin Luo and Peter G Blake in Canadian Journal of Kidney Health and Disease
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Ontario Renal Network as a part of Ontario Health through an annual statement of work organized with ICES Kidney Dialysis and Transplantation. This study was supported by the ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and Long-Term Care (MLTC). The research was done at the ICES Western facility with partners which include the Academic Medical Organization of Southwestern Ontario (AMOSO), the Schulich School of Medicine and Dentistry (SSMD), Western University, and the Lawson Health Research Institute (LHRI). Parts of this material are based on data and information compiled and provided by the Ministry of Health (MOH), Ontario Health (OH), and Canadian Institutes of Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are solely those of the authors, and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. We thank IQVIA Solutions Canada Inc. for use of their Drug Information File. This study used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. The data linkage was conducted by members of the ICES Kidney, Dialysis and Transplantation team, at the ICES Western facility, who are supported by a grant from the Canadian Institutes of Health Research (CIHR). Dr Andrea Cowan was supported by the University of Western Department of Medicine and the Division of Nephrology and the Academic Medical Organization of Southwestern Ontario’s Opportunities fund.
Ethics Approval and Consent to participate
The use of ICES data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act (PHIPA) which does not require informed consent or review by a Research Ethics Board.
Consent for Publication
All authors consented to publication
Data Access
The data linkage was conducted by members of the ICES Kidney Dialysis & Transplantation (KDT) team at the ICES Western facility (London, Ontario). The protocol can be obtained by emailing Dr Cowan at andrea1.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.