
Abstract
Background:
There is a gap between the number of patients waiting for a transplant and the number of kidneys available. Some deceased donor kidneys are currently nonutilized, as medical teams fear that they will experience suboptimal graft survival. However, these organs could provide an acceptable therapeutic option if they were allocated for preemptive kidney transplantation in elderly candidates.
Objective:
This project aims to gather patients’ perspectives on the allocation of kidneys with lower longevity for preemptive kidney transplantation in elderly patients.
Design:
Individual interviews.
Setting:
The Center hospitalier de l’Université de Montréal (CHUM) chronic kidney disease (CKD) clinic.
Participants:
Patients aged between 64 and 75 years with CKD G4-5 ND, followed at the CHUM and who have not initiated dialysis yet.
Methods:
Between March and July 2023, we conducted 14 individual interviews with patients aged between 64 and 75 years who had CKD G4-5 ND and were followed at the CHUM. The interviews were digitally recorded and transcribed. Thematic analysis was conducted.
Results:
Most participants were in favor of using kidneys with lower longevity to increase their access to transplantation, improve their quality of life, enable accelerated transplantation, and avoid dialysis. Patients also wanted to be engaged in the decision-making process, underlining the importance of informed consent. Although the use of kidneys with lower longevity offers the hope of returning to “normal” life, some patients were concerned about the risk of reduced graft survival and the need for a subsequent kidney transplant. In these cases, patients were interested in using mitigation strategies, such as prioritization for kidney transplantation from standard donors in case of early graft loss associated with receiving kidneys with lower longevity. They also recommended the development of a separate waiting list for patients consenting to preemptive transplantation with kidneys with lower longevity.
Limitations:
This study was conducted in only 1 nephrology clinic in the province of Quebec with French-speaking patients. Consequently, the results may not be generalizable to other populations, including ethnic minorities.
Conclusion:
The use of kidneys with lower longevity for preemptive kidney transplantation appears to be an interesting option for elderly kidney transplant candidates. However, patient information and participation in the decision-making process are essential. Moreover, organ donation organizations and transplant programs should develop a separate waitlist for transplant candidates who have preconsented to receive organ offers of deceased donor kidneys with lower longevity.
Trial registration:
Not registered.
Introduction
Kidney transplantation improves patient survival and quality of life, and decreases health care costs when compared with dialysis.1,2 The availability of organs is far from meeting the demand for transplants, with over 2000 Canadians waiting for a kidney transplant at the end of 2021. 3 During that same year, 1188 patients received a transplant and 99 died before receiving one. 3 Despite the overwhelming need for kidney transplantation, a substantial proportion of deceased donor kidneys are nonutilized. Although there are no Canadian data, it is estimated that in the United States around 20% of all deceased donor kidneys are nonutilized. 4 This is particularly true with kidneys that fit the criteria for expanded donor or have a kidney donor profile index (KDPI) above the 85th percentile, where the discard rate could be as high as 60%.5,6 A recent study conducted in the Netherlands also showed a nonutilization rate of 24.4%, with the reasons for nonutilization being expected impaired quality of the organs and acute kidney injury. 7
While using kidneys originating from expanded criteria donors or high KDPI kidneys could be associated with an adverse impact on graft survival, this impact is not as pronounced amongst older recipients. Accepting such kidneys for patients aged more than 60 years is associated with a better survival rate than remaining on dialysis. 6 ,8 -11 This could be particularly true if the marginal kidneys are used to perform preemptive transplantation. Currently and exceptionally in the province of Quebec, it is possible to receive a preemptive deceased kidney transplantation from a “standard criteria” donor. To be waitlisted, the transplant candidate needs to have an eGFR of less than 15 mL/min/1.73m2 allowing preemptive kidney transplantation. However, since time spent on dialysis is an important criterion in the current Quebec allocation algorithm, preemptive deceased donor kidney transplantation is a rare phenomenon. 12 A recent study has shown good outcomes for preemptive transplantation with high (>85%) KDPI kidneys. 13 A key barrier to using these kidneys is the risk of delayed or slow graft function, both of which are associated with higher complications after transplantation. However, the risk of delayed graft function or the need for hemodialysis could be mitigated by preemptive kidney transplantation where patients have enough residual kidney function to avoid dialysis until the kidney starts to work. Therefore, using marginal or high KDPI kidneys that would normally be discarded for preemptive kidney transplantation in elderly candidates could provide access to transplantation to those candidates who may have otherwise been denied access to transplantation due to expected long wait times. Moreover, using these kidneys—which are currently nonutilized—could increase the number of kidney transplantations performed, thereby improving patients’ survival and quality of life. 2 For the purpose of this manuscript, marginal, extended criteria or high KDPI kidneys that would normally be nonutilized will be referred to as “kidneys with lower longevity.”
In Quebec, there is no determined age limit for kidney transplantation. As recommended by the KDIGO, age is considered in the context of other comorbidities. 14 Preferentially allocating kidneys with lower longevity to candidates older than 65 years for preemptive kidney transplantation raises ethical issues in terms of fairness and justice. Indeed, this allocation could be viewed as ageism or discrimination based on age.15 -17 However, a kidney allocation system, such as the one used in the province of Quebec, that gives weight to time spent on dialysis also disadvantages elderly patients who cannot afford to wait a long time to have access to kidney transplantation. 18 The transplantation of kidneys with lower longevity should primarily be considered for patients who tolerate dialysis poorly and in whom a strategy of early transplantation with a lower longevity kidney is associated with a survival benefit compared to the alternative of continued waiting for a kidney with longer projected longevity. 19 However, there are few studies examining the perspectives of candidates on the topic of transplantation of kidneys with lower projected longevity. In this context, it is of paramount importance to gather stakeholders’ views on this new way of allocating kidneys in order to develop future allocation policies that are deemed ethical and fair for patients. The objective of this study was to gather the perspectives of patients aged between 64 and 75 years with chronic kidney disease and GFR category 4 and 5 not treated with maintenance dialysis (CKD G4-5 ND) on the use of kidneys with lower longevity for preemptive transplantation.
Material and Methods
This study was exploratory in nature and used semi-structured interviews with patients aged between 64 and 75 years who had CKD G4-5 ND and were followed at the Center hospitalier de l’Université de Montréal (CHUM) CKD clinic. To be included in the study, participants had to speak French or English and have no formal contraindications to kidney transplantation (cancer, dementia, or active infection). We used the consolidated criteria for reporting qualitative research checklist. 20 The CHUM research ethics board approved the study (CE 22.231) and all participants provided informed consent.
The recruitment and interviews were carried out between March and July 2023. A list of 263 patients followed at the CKD clinic was provided to the research team. Forty-one patients who met the inclusion criteria and were without a major contraindication to transplantation were contacted by email or by phone. Twenty showed an interest in participating. Of that group, 14 patients completed the sociodemographic questionnaire and were interviewed. Personal reasons, health issues, a lack of understanding of written French, or being unreachable were the reasons for not taking part in the interviews. Three attempts were made to reach candidates, and in the absence of a response, they were withdrawn from the study.
Fourteen participants took part in individual interviews. All were conducted in French. Three were conducted in-person, 8 by phone and 3 via videoconference. All interviews were conducted by the same member of the research team, who is not involved in the care of patients with CKD (CS). The interviews lasted on average 44 ± 19 minutes (ranged from 25 to 97 minutes) and were digitally recorded and transcribed. The demographic questionnaire was completed with participants during the interview. Participants received $30 as compensation. The raw interview transcripts were sent for review and approval to all the participants. No participants requested modification of the transcripts.
The issues covered during the interviews were outlined in an interview guide with open-ended questions that was developed by the research team based on a review of literature on the use of kidneys with lower longevity and the ethics of kidney allocation.21 -23 The questions addressed the following themes: (1) expectations related to kidney transplantation; (2) perspectives on the current deceased donor kidney allocation criteria in the province of Quebec; (3) use of kidneys with lower longevity and preemptive kidney transplantation; (4) ethical issues associated with the use of kidneys with lower longevity; and (5) sociodemographic data. Additional questions and reformulation techniques were employed to gain a more precise representation of participants’ perspectives. Consistent with qualitative methodology, the interview guide was modified during the study as new topics emerged from the interviews.24,25 (See Supplementary Material for interview guide and demographic questionnaire.)
We used a qualitative description approach.26,27 The goal of this pragmatic approach was to stay close to the data and provide a comprehensive summary of the topic studied, using thematic analysis. The latest version of NVivo (Lumivero) software was used to facilitate the analysis. Prior to coding the verbatim, the research team used a deductive approach and created the initial coding frame based on the interview grid and a review of the literature. During coding, we also used an inductive approach where new codes were added to the coding frame based on the interview content.28,29 The research team met frequently to discuss the coding frame and data analysis. A member of the research team with expertise in qualitative methodology (CS) coded the interviews and no new codes were created after the 10th interview. The number of participants allowed for data saturation. An independent researcher (AA) with experience in qualitative methods coded the raw data from 6 interviews, with the rate of coding agreement assessed at 94% and disagreements were discussed. Coded quotes were then organized by themes and subthemes.
Results
Participants’ Characteristics
Fourteen patients aged between 64 and 75 years, including 8 male and 6 female, with CKD G4-5 ND and followed at the CHUM CKD clinic, participated in the study. The median age of the patients interviewed was 69 years. Nine participants had a life partner, 64% of the participants were white and 9 had completed post-secondary education. Three were transplant candidates, 2 were on hold on the waiting list, 1 was deemed ineligible for a transplant, 1 was currently being assessed for a transplant, and 7 were not in the process of being assessed for a kidney transplant. Fifty-seven percent of participants described their quality of life as sufficient, while 43% responded that it was either excellent or good. More than half (57%) of participants agreed with the following statement: “I have health problems, but I am able to perform my daily activities normally.” Eight participants decided on dialysis, while 5 of them opted for peritoneal dialysis. Eight participants were willing to accept kidneys with lower longevity for transplantation, 3 were unsure, and 3 would decline such an offer. Table 1 summarizes participants’ characteristics.
Participants’ Characteristics.

The total number exceeds 14 because some participants indicated speaking more than 1 language at home.
Qualitative Interviews
During the interviews, participants discussed their perspectives on the current deceased donor kidney allocation process. Kidney transplantation was described as a way to improve their quality of life and maintain their autonomy. The advantages and arguments against using kidneys with lower longevity, the ethical issues and recommendations for a future program that would allocate kidneys with lower longevity to elderly patients preemptively were also discussed. In this section, we will present the major themes identified in our study.
1. The current deceased kidney allocation policy is fair but has some flaws
Most participants had limited knowledge about the current deceased donor allocation criteria in the province of Quebec. Despite their limited knowledge, they generally believed that the allocation process was fair for all patients. However, they perceived their older ages as a barrier to transplantation. They believed that younger candidates are currently prioritized in an organ shortage context. This belief was a source of frustration for many participants. However, they agreed with a system where the age of the donor is matched with the age of the recipient.
Since important weight is given to time spent on dialysis in the current allocation system used in the province of Quebec, some older patients received the information that their chances of receiving a deceased donor preemptive kidney transplantation were low and they were encouraged to find a living kidney donor. However, 1 participant expressed feeling a sense of helplessness because they did not have a potential living donor among their next of kin, and they felt that deceased kidney transplantation was not an option for them. Table 2 presents interview excerpts.
The Current Deceased Kidney Allocation Policy is Fair But Has Some Flaws.

2. Kidney transplantation is a way to improve quality of life, survival, and preserve patients’ autonomy
Participants expressed 3 main reasons to consider kidney transplantation: improving their quality of life, maintaining their autonomy since they viewed dialysis as burdensome and as an obstacle to their autonomy during daily activities, and improving their survival. Quality of life, as described by participants, encompasses various aspects such as being socially active, having the energy to sustain daily activities, feeling good, and experiencing fewer dietary restrictions. One participant emphasized the physical burdens associated with dialysis, such as frequent hospitalizations, interventions, and the need to take many medications. Table 3 presents interview excerpts.
Kidney Transplantation is a Way to Improve Quality of Life, Survival, and Preserve Patients’ Autonomy.

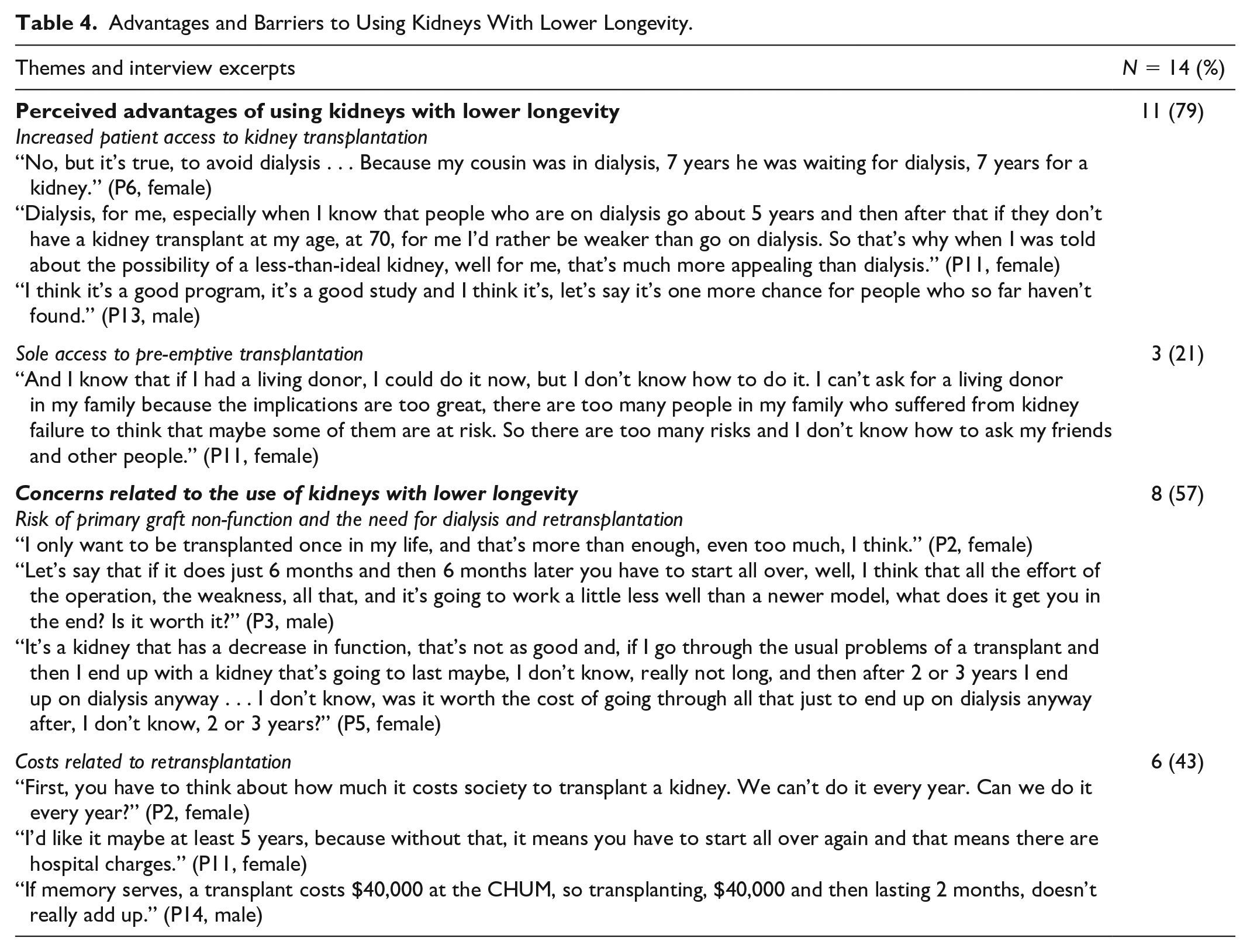
3. Advantages and barriers to using kidneys with lower longevity that would normally be nonutilized for kidney transplantation
Using kidneys with lower longevity that would normally be nonutilized was viewed as a way to increase the number of organs available and thus improve patients’ access to kidney transplantation. Moreover, this could be the only way for elderly patients who do not have any living donors to have access to a preemptive kidney transplantation, allowing them to avoid dialysis treatments and enjoy an improved quality of life.
One concern expressed by the participants about using kidneys with lower longevity for transplantation is the potential for primary graft nonfunction. They did not see any benefit to being transplanted preemptively if the chances of needing dialysis afterward are high due to the quality of the organ transplanted. Some participants described kidney transplantation as a demanding procedure and did not want to go through the process twice since the chances of primary graft nonfunction are high. A few participants were concerned about the costs related to a second transplantation. Table 4 summarizes the results with interview excerpts.
Advantages and Barriers to Using Kidneys With Lower Longevity.
4. Ethical issues related to preemptive allocation of kidneys with lower longevity to elderly patients
Most of the participants wanted to be involved in the decision-making process of whether or not to accept a kidney with lower longevity that would normally have been discarded. In order to participate in the decision-making process, they wished to receive information on the risks, the benefits and the potential impact of using such kidneys on their quality of life. The information needed to be tailored to their unique situation. However, some participants wanted to be more passive in the decision-making process and said that they would trust their health care professionals’ recommendations.
Some participants did not see any fairness issues with allocating kidneys with lower longevity preemptively to elderly patients since these patients are accepting a higher risk of primary graft nonfunction or lower graft survival. Other participants, however, questioned whether this allocation could be considered age discrimination since these kidneys with lower longevity are preferentially allocated to elderly patients. Some participants also questioned how patients should be selected to have access to a preemptive kidney transplantation with a kidney with lower longevity and if age should be the only criterion for this allocation. Table 5 summarizes the results with interview excerpts.
Ethical Issues Related to Preemptive Allocation of Kidneys With Lower Longevity to Elderly Patients.

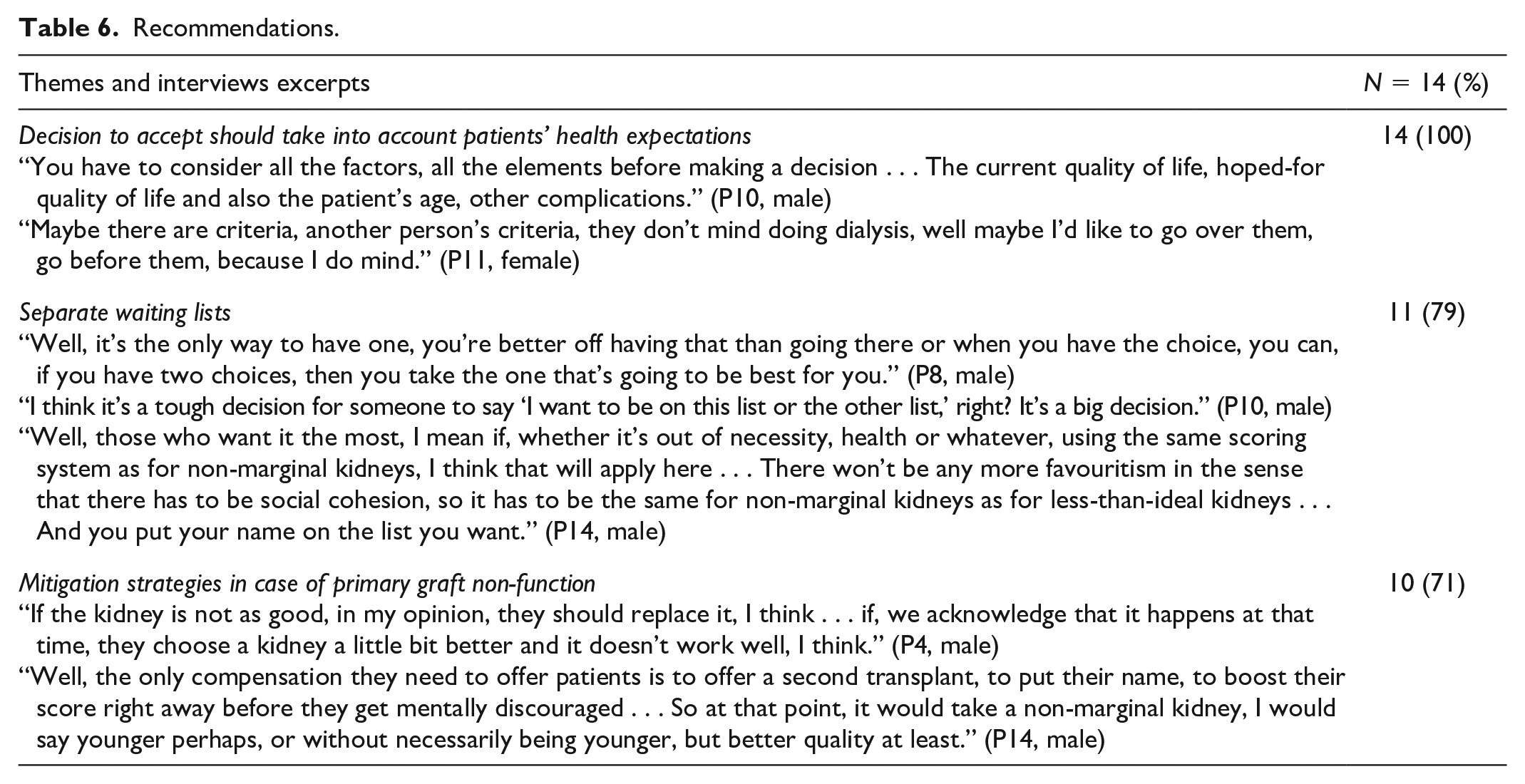
5. Recommendations
Participants made some recommendations in the event that a transplant program or an organ donation organization was planning to implement a program where kidneys with lower longevity that would normally not be utilized were offered to elderly patients not yet on dialysis. First, the participants believed that the decision of whether or not to accept this type of transplantation should take into consideration patients’ personal health expectations. They also suggested developing a separate waiting list for patients who agreed to be contacted for a kidney with lower longevity offer. The decision of whether or not to be on this separate waiting list should be regularly reassessed. The final recommendation was to develop a safety net in the event of primary graft nonfunction. Since the patients would be agreeing to take a higher risk, the system should offer some form of compensation. For some participants, the safety net should be to prioritize patients with primary graft nonfunction who are on the deceased waiting list for a retransplantation. Table 6 summarizes the results with interview excerpts.
Recommendations.
Discussion
This qualitative study reports the perspectives of patients aged between 64 and 75 years with CKD G4-5 ND but who have not initiated dialysis on the possibility of allocating them kidneys with lower longevity, which would not have been utilized otherwise, for a preemptive kidney transplantation. This is the first study to report the perspectives of patients who are not necessarily transplant candidates and who did not experience dialysis. Some participants believed that their ages could be a barrier to access to transplantation. It is possible that a better understanding of the kidney transplantation eligibility criteria and allocation policy would have changed their views on this topic. Also, since some participants believed that living kidney transplantation was their only option given their ages, it is also possible that better education and help to find living kidney donors would have modified participants’ views on the acceptability of using kidneys with lower longevity.
In recent years, different studies have explored patients’ preferences about less-than-ideal or high KDPI kidneys. Schantz et al conducted qualitative interviews with waitlisted patients and deceased donor transplant recipients on the decision-making process when a high KDPI kidney (>85) is offered. In that study, participants had limited knowledge about high KDPI kidneys. Patients’ willingness to accept these kidneys varied based on their health status. Experiences of dialysis, declining health and increased waiting times were factors associated with increased willingness to accept a high KDPI kidney. Although the majority of patients wanted to be transplanted to improve their quality of life, a significant proportion of patients underestimated the benefits of transplantation over dialysis in terms of survival. 30 This latter finding is aligned with our results where our participants considered accepting a kidney with lower longevity in order to avoid dialysis and improve their quality of life. Only a few participants mentioned the positive impact of kidney transplantation on their survival.
Another qualitative study was conducted with 10 individuals on the kidney transplant waiting list and 5 patients who had received a high KDPI in order to better understand their perspectives on kidneys with lower longevity. Participants’ reasons for accepting a kidney with lower longevity were to be free of dialysis, improve their quality of life, have the ability to travel and return to normalcy. For waitlisted patients, kidney transplantation with a kidney with lower longevity was worthwhile if it allowed them to gain 3-5 dialysis-free years. Participants also expressed a desire to receive transparent, clear, and standardized information about kidneys with lower longevity during the transplant assessment period in order to engage actively in the decision-making process. 31 Being free of dialysis, improving quality of life and wanting information were also themes that arose during our study with participants who did not have any experience of transplantation.
Two discrete choice experiments, one conducted in the United States 32 with kidney transplant recipients and candidates, and the other conducted in France 33 with transplant recipients, elicited patients’ preferences on receiving a kidney with lower longevity. In the American study, kidneys with lower longevity were acceptable for patients with longer expected waiting time. Participants older than 62 years, those of African American ethnicity, as well as those with a lower education level and with low performance status were more likely to favor a reduced waiting time. 32 In the French study, 86% of participants were willing to accept a kidney with lower longevity in an emergency situation, and 71% expressed willingness in situations that make it harder to find a compatible organ, such as being highly sensitized. As in previous studies, a majority of participants (67%) wanted to be informed about an organ with lower longevity in order to participate in the decision-making process. 33 As in our study, the issue of information and participation in the decision-making process were particularly important.
When questioned about ethical issues related to the use of kidneys with lower longevity, the participants in our study mentioned the need to receive sufficient and tailored information in order to give informed consent. Participants were divided on whether preferentially allocating kidneys with lower longevity for preemptive transplantation to elderly patients raised a fairness issue. Many allocation schemes take into account both recipient age and donor age. For instance, in the province of Quebec, pediatric patients are prioritized for organs from young donors. Age matching between the donor and the recipient is also taken into consideration. 12 Considering age in organ allocation aligns with the “fair innings principle” or the “justice over lifetime principle,” where a younger person is entitled to be prioritized in organ allocation over an older one. This is based on the notion that the older individual had the opportunity to live longer and achieve more in their life, including work, raising children, traveling, and building personal relationships. 21 Other participants questioned if this type of allocation could be viewed as age discrimination. Since older patients have paid taxes and participated in society their entire life, they should not be penalized in their access to transplantation. 18 Granting them preferential access to kidney transplantation with a kidney with lower longevity due to their age could be perceived as being discriminatory. However, we could remediate this problem by offering patients the possibility of accessing both preemptive transplantation with kidneys with lower longevity and waiting for a kidney transplantation from a “standard criteria” donor. This highlights the importance of implementing a registry of patients who have consented to receive kidneys with lower longevity and ensuring that they receive tailored information to make an informed decision and provide consent.
Surprisingly, in our study and other studies exploring patients’ perspectives on transplantation with kidneys with lower longevity, improving life expectancy is not a reason frequently mentioned for accepting a kidney with lower longevity. However, other studies have shown there are advantages to elderly patients in receiving a high KDPI, marginal or kidney with lower longevity over remaining on dialysis.10,11,13 Therefore, before implementing a program of preemptive transplantation with kidneys with lower longevity for elderly patients, it would be important to develop educational material that highlights the benefits in terms of patient survival compared to remaining on dialysis.
Our study has some limitations. First, we only studied patients’ perspectives and we did not gather those of other stakeholders, such as health care providers, caregivers and organ donation organization managers. Second, the participants were from 1 CKD clinic in the province of Quebec and had a good self-rated performance status. The majority of participants were white, had post-secondary education and a partner. They are therefore not representative of all elderly patients with CKD G4-5 ND who could be eligible for kidney transplantation, particularly patients from ethnic groups or those living in rural or remote areas. Moreover, our study did not address the needs of vulnerable populations who mistrust traditional medicine, such as Indigenous populations in Canada 34 or Afro-American populations in the United States. 35 Further studies are needed to better understand the needs of vulnerable populations in terms of the use of kidneys with lower longevity in order to not perpetuate mistrust of the health care system. Also, as clinical practice varies by country, our results may not be applicable to other parts of the world. However, organ allocation systems of other Canadian provinces and other countries share many important elements with the system used in the province of Quebec, and we believe that our results can reflect the perspectives of many elderly patients in Western countries with a well-developed deceased donor transplantation system on the use of kidneys with lower longevity for preemptive transplantation. Also, questions about how to reduce the kidney nonutilization rate and improve the use of kidneys with lower longevity are universal in a context of organ scarcity. Learning from patients’ perspectives and practices in Canada could trigger reflections that could improve the allocation and the use of kidneys with lower longevity in other countries.
Conclusion
The use of kidneys with lower longevity for preemptive transplantation in elderly patients is an interesting option for participants in our study since it could increase the number of organs available and allow elderly patients to have access to preemptive transplantation and avoid dialysis. Preemptive transplantation is viewed as a way to improve quality of life compared to being on dialysis. However, the fear of primary nonfunction is a concern for many patients. One of the recommendations was to develop a distinct waiting list for patients who consent to receive offers of kidneys with lower longevity. In order to provide consent, patients need to have access to educational material tailored to their reality. Further studies are needed to explore other key stakeholders’ perspectives on the allocation of kidneys with lower longevity for preemptive transplantation in elderly patients. Also, before implementing this type of allocation, clinical studies will be needed to document the medical outcomes of preemptive transplantation with kidneys with lower longevity.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581241267165 – Supplemental material for The Use of Kidneys With Lower Longevity From Deceased Donors to Improve Access to Preemptive Renal Transplantation for Elderly Patients: A Qualitative Study
Supplemental material, sj-docx-1-cjk-10.1177_20543581241267165 for The Use of Kidneys With Lower Longevity From Deceased Donors to Improve Access to Preemptive Renal Transplantation for Elderly Patients: A Qualitative Study by Carina Sancho, Aliya Affdal, Fabián-Andrés Ballesteros Gallego, Marie-Françoise Malo, Savannah-Lou Cochran-Mavrikakis, Héloise Cardinal, John S. Gill and Marie-Chantal Fortin in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-2-cjk-10.1177_20543581241267165 – Supplemental material for The Use of Kidneys With Lower Longevity From Deceased Donors to Improve Access to Preemptive Renal Transplantation for Elderly Patients: A Qualitative Study
Supplemental material, sj-docx-2-cjk-10.1177_20543581241267165 for The Use of Kidneys With Lower Longevity From Deceased Donors to Improve Access to Preemptive Renal Transplantation for Elderly Patients: A Qualitative Study by Carina Sancho, Aliya Affdal, Fabián-Andrés Ballesteros Gallego, Marie-Françoise Malo, Savannah-Lou Cochran-Mavrikakis, Héloise Cardinal, John S. Gill and Marie-Chantal Fortin in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-3-cjk-10.1177_20543581241267165 – Supplemental material for The Use of Kidneys With Lower Longevity From Deceased Donors to Improve Access to Preemptive Renal Transplantation for Elderly Patients: A Qualitative Study
Supplemental material, sj-docx-3-cjk-10.1177_20543581241267165 for The Use of Kidneys With Lower Longevity From Deceased Donors to Improve Access to Preemptive Renal Transplantation for Elderly Patients: A Qualitative Study by Carina Sancho, Aliya Affdal, Fabián-Andrés Ballesteros Gallego, Marie-Françoise Malo, Savannah-Lou Cochran-Mavrikakis, Héloise Cardinal, John S. Gill and Marie-Chantal Fortin in Canadian Journal of Kidney Health and Disease
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.