
Abstract
Background:
Symptom burden among long-term hemodialysis (HD) patients is high, and addressing symptoms has been identified as a key research priority by patients. Acupressure has shown some effectiveness in management of symptoms in patients with HD.
Objective:
The purpose of this study was to explore the feasibility and the effect of implementing a self-administered acupressure intervention on symptom burden and quality of life for in-center HD patients.
Design:
A pilot randomized controlled study.
Setting:
Two outpatient community HD clinics between in Calgary, Alberta, Canada.
Patients or Sample or Participants:
Patients on HD for at least 3 months and with at least one symptom score rated greater than moderate were eligible for the study.
Methods:
Participants were randomized into either the (1) self-acupressure + usual care or (2) usual care alone group. Participants in the acupressure group were given a wooden acupressure tool and taught how to self-administer protocol on 6 acupressure sites for the 4-weeek study duration. Feasibility outcomes were assessed through satisfaction surveys and attrition. Other outcomes included quality of life and symptom scores by validated questionnaires (EQ-5D-5L and Integrated Palliative Outcome Score—Renal [IPOS-Renal]).
Results:
Thirty-two participants were successfully enrolled in the study; acceptability was high with study completion at 98% in the intervention group and 82% adherence rate to the 4-week protocol. Participants in the intervention group reported an improved change score in quality of life (EQ-5D-5L Index Score change = +0.053; EQ-5D-5L visual analog scale score change = +6.7). Participants in the intervention group also reported improved symptom scores (IPOS-Renal overall change = −2.8).
Limitations:
Small sample size and intervention duration are limitations of this pilot study.
Conclusions:
The results from this study suggest that self-acupressure was acceptable and feasible in this sample of HD patients. Self-acupressure may have a role for supporting the management of symptoms in HD patients. These pilot results can be used to inform larger more definitive investigations.
Introduction
Symptom burden among long-term hemodialysis (HD) patients is high, despite provision of adequate dialysis. Commonly reported physical and mental symptoms include fatigue, sleep disorders, pain, anxiety, depression, nausea, pruritus, restless legs, and muscle cramp.1,2 Most patients endure not just one, but multiple symptoms, impacting an individual’s ability to work, socialize, or live independently; while increasing the risk of mortality and an increased reliance upon medical resources. 3
Through priority setting, engagement surveys, and interviews, HD patients have identified symptom management as a top priority for researchers and nephrology teams.1,2,4 While pharmaceuticals have historically been the first-line intervention for symptom management, recent guidance placed an emphasis on offering nonpharmacological options and promoting the adoption self-management strategies. 5
One nonpharmacological and noninvasive intervention with potential for ameliorating several unpleasant symptoms experienced by those on HD is acupressure. This alternative healing technique has been used in Chinese medicine for over 2500 years and is based on the meridian theory. 6 This theory suggests that applying firm manual pressure to specific locations along meridians in the body will reduce blockages and restore imbalances. This can stimulate the flow of Qi (bio-energy) through a network of pathways, providing symptom relief. 6
Evidence for the use of acupressure to manage the symptoms in HD patients is growing in both diversity and popularity. Benefit has been reported for symptoms such as fatigue,7,8 pain, 9 sleep,10-14 depression,15-17 pruritus,18-20 cramps, 21 dizziness, 22 restless legs, 23 thirst, 24 blood pressure, 25 nausea, 26 and constipation. 27 In most of these studies, an acupressurist or trained researcher delivered the intervention to the participants either before or during their HD treatments.
To our knowledge, there have not been self-acupressure studies completed in HD patients. Self-acupressure has been shown to be beneficial in non-HD populations for itchiness, 28 sleep, 29 knee pain,30,31 and long-term low back pain. 32 A systematic review reported positive effects of self-acupressure in a variety of conditions and symptoms. 33 Given the reported benefits in other long-term disease populations, examining the use of self-acupressure for HD patients is warranted. The purpose of this pilot study was to explore the feasibility and the effects of implementing a self-administered acupressure intervention on the symptom burden and quality of life for in-center HD patients.
Methods
Study Design
We completed a 2-arm pilot randomized controlled trial to assess feasibility and effectiveness of the self-acupressure protocol on symptom change over 4 weeks via symptom self-reporting and quality-of-life questionnaires. Ethics approval was granted by the University of Alberta (ethics ID: REQ00007147).
Participants
Participants were recruited from 2 outpatient community HD clinics between January 2020 and October 2020 in Calgary, Alberta, Canada. Integrated Palliative Outcome Score—Renal (IPOS-Renal) surveys 34 were currently being done as part of standard care every 2 months with patients in the clinics; therefore, those who completed these surveys were identified for inclusion in the study. Patients with at least one symptom score rated between 2 and 4 (or “moderate, severe, or overwhelmingly”) based on the IPOS-Renal survey were eligible for the study. Additional criteria for participation required being on three 4-hour treatments per week, being on HD for >3 months, and no cognitive impairment, vision impairment, or language barriers affecting understanding of the study instructions or land-marking of the acupressure sites on the body. Informed consent was obtained from all patients by a staff researcher who did not directly work with the patients at the clinic. All guidelines within the Declaration of Helsinki were adhered to.
Intervention
Research assistants were trained on the self-acupressure protocol by an acupressure professor from the local school of Chinese medicine, which involved approximately 1 hour of teaching and practice. During this training, the research staff learned how to explain the protocol, how to accurately landmark the 6 sites (Supplemental Material), the symptoms managed by each site, the proper use of the wooden acupressure tool (or finger pressure), and the appropriate amount of weight or pressure to apply (approximately 4-5 lbs of pressure). Participants were randomized into either the (1) self-acupressure + usual care or (2) usual care alone group by a computer-generated randomization program. Investigators and research staff were not aware of the treatment allocation prior to randomization. If patients were assigned to the intervention group, a member of the research team provided the participant with an acupressure tool (Kaittiyashop, Thailand; found at www.amazon.ca) and were taught how to perform the Acupressure Protocol (Supplemental Material). Each of the 6 acupressure points (Outer Thigh—Gallbladder 31 [GB 31]; Front Thigh—88.01,02,03; Wrist Bone- Small Intestine 4 (SI 4); Thumb—Large Intestine 4 (LI 4); Mid Wrist—Pericardium 6 (PC 6); and Pinky Side Wrist—Heart 7 (HT 7)) were to be stimulated for 2 minutes using either their finger, thumb, or the wooden acupressure tool twice per day (once in the AM, once in the PM) for 4 weeks. The researchers ensured the entire first session was conducted during HD so they could observe the patient and ensure correct land marking of the sites and technique was being done. Participants were asked to record the completion of each session using an Acupressure Completion Chart. Space was available for the patient to note any observations, comments, adverse effects, or to cite reasons for missed sessions. Research team members followed-up with participants in the intervention group on a weekly basis for 5 to 10 minutes to assess their technique and to ensure they were completing their completion charts.
The usual care group received standard care for 4 weeks. In accordance with current practice at the HD clinics, patients were asked by nursing staff if they wished for support with managing their symptoms and if so, which symptoms they specifically wanted to address. If the patient was in favor of this, then the nursing staff used the standardized clinical symptom management guidelines to develop a nonpharmaceutical (primary option) or a pharmaceutical plan (secondary option if the nonpharmaceutical option was unsuccessful). This could include education in the form of patient handouts or a referral to appropriate members of the multidisciplinary care team (nephrologist, social worker, spiritual care practitioner, kinesiologist, dietitian, access nurse, or pharmacist).
Outcome Measures
Assessing the acceptability and feasibility of the intervention was the primary outcome. This was done in the intervention group through a qualitative participant survey, adherence tracking (percentage of sessions completed and dropout rate), and documentation of any adverse effects. The participant survey gathered information on satisfaction, perceived feasibility, likelihood to continue, and patient’s perceptions and feedback and were themed. Participants were asked to fill in completion charts for each session performed and turn them in at the end of 4 weeks.
Quality of life and symptom burden were secondary outcomes and were assessed using surveys performed at baseline and follow up (4 weeks) in both groups. Quality of life was measured using the validated EQ-5D-5L Index. 35 This tool has 5 questions with a Likert scale ranging from 0 (nothing) to 5 (most serious) and has been validated in HD populations. 36 The EQ-5D-5L (visual analog scale) VAS scale depicts the patient’s perception on how they are doing on a particular day with a score of 100 describing “The best health you can imagine” and a score of 0 illustrating “The worst health you can imagine.” The symptom score was collected via the IPOS-Renal. 34 The IPOS-Renal has been validated in the kidney disease population and includes 11 questions with additional physical and psychological sub-items. This study examined individual symptom scores, which are rated on a 0 to 4 Likert scale with 0 illustrating “no symptom” and 4 being an “overwhelming” symptom.
Statistical Analyses
Participant characteristics for each group are reported as proportions (n, %) or medians (interquartile range) as appropriate. Pre and post scores for the 15 symptoms on the IPOS-Renal inventory and the 5 dimensions of EQ-5D-5L were expressed as mean ± SD. Differences in mean pre-post change between the 2 groups in IPOS-Renal Total Score and overall EQ-5D-5L Index and EQ-5D-5L VAS scores were determined. We determined the proportion of patients achieving a minimal clinically important difference (MCID) in each group (i.e. a change of more than 10 points in EQ-5D-5L VAS Score or a change of more than 0.04 points in the EQ-5D-5L Index Score. 37 All statistical analyses were performed using SPSS, version 25 (IBM Corp, Armonk, NY).
Results
Patient characteristics are outlined in Table 1. The control group had a longer HD vintage and fewer individuals with a diabetes diagnosis than the intervention group. It is important to note that one HD clinic had completed the study just prior to the COVID pandemic shut down in March 2020, while the other location started recruitment during the pandemic in October 2020; however, participants were randomized in each clinic. Figure 1 outlines flow of participants through the study.
Patient Demographics.


Participant flow.
Retention within the study was high with 98% of the acupressure group completing the 4-week protocol. Only one participant dropped out of this group after deciding to transition to palliative care. The usual care group had 2 noncompleters due to a transplant (n = 1) and a cardiac event (n = 1). Adherence was calculated at 82% in patients who returned their acupressure completion charts (2 patients lost their sheets). Common reasons for not completing the acupressure session included feeling too tired, feeling sick, forgetting, pain, or a scheduling conflict. The satisfaction survey conducted at the end of the study illustrated positive perceptions and receptiveness of the patients (Figure 2). Interestingly, 80% of patients in the acupressure group believed they were adherent to the protocol and 73% felt they had benefited from the study. Most of those in the treatment group reported they would continue self-acupressure for their symptom management (87%), felt it was easy to do (87%), and would recommend this to other HD patients (87%).
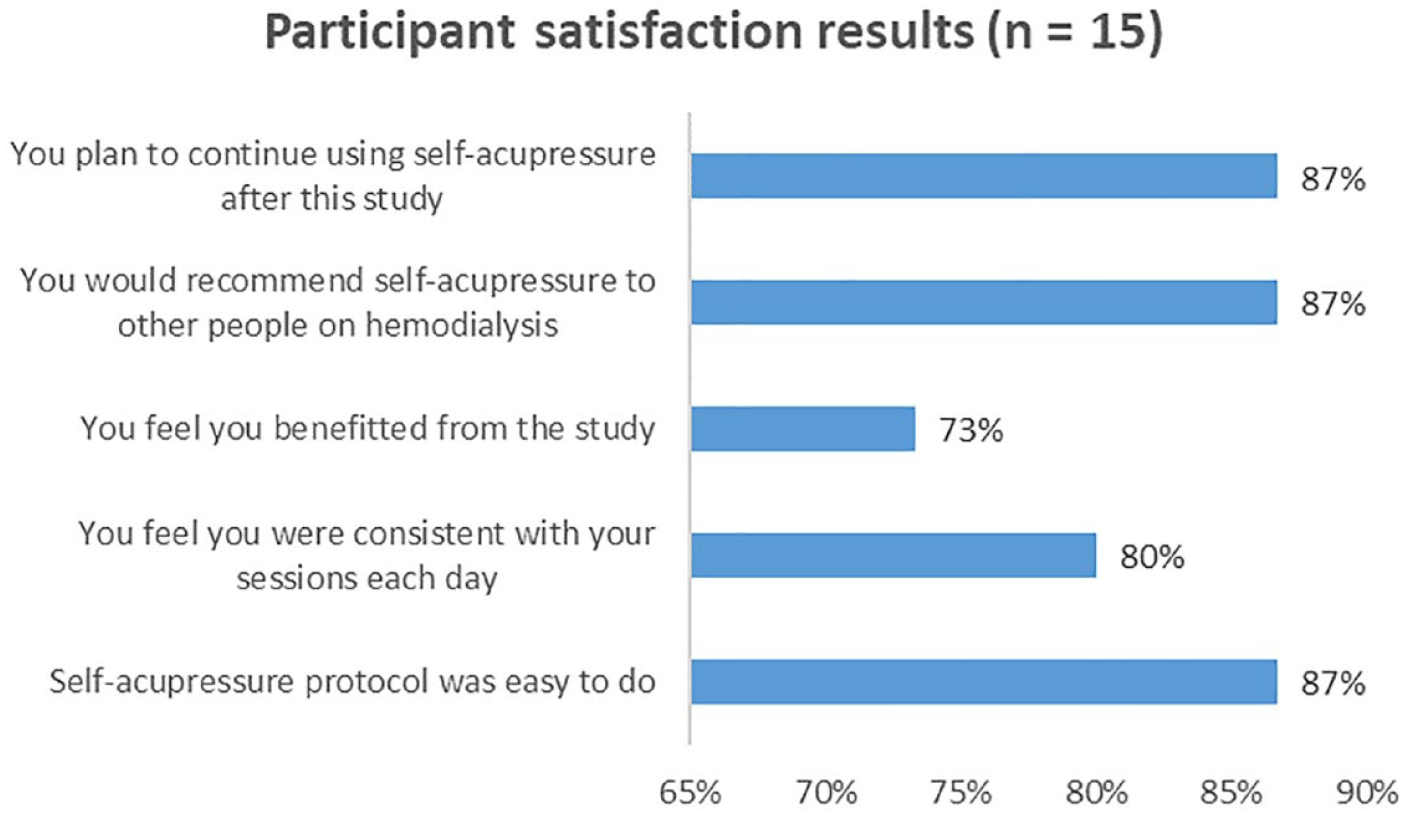
Participant satisfaction survey findings.
When comparing the intervention and control groups, improvements were noted for both the EQ-5D-5L Index score and the EQ-5D-5L VAS (Table 2). Those in the acupressure intervention group reported an increase in their EQ-5D-5L VAS scores by an average of 6.7 points, while mean scores in the usual care group decreased by 11 points, indicating lower perceived health state. Table 3 outlines the change within the specific domains of the EQ-5D-5L. The intervention group reported improvement in all 5 of the domains with the largest improvement in “problem doing usual activities.” Of note, the usual care group reported improvements in “mobility” and “pain and discomfort” domains and reported a worsening of their perceived rating of anxiety/depression.
Comparisons of Differences in Change in Overall EQ5D Index and EQ5D VAS Scores Between Intervention and Control Groups.

Note. A decrease in score indicates a lower perceived health state.
Pre vs. Post Comparisons for Intervention and Groups for Specific Dimensions of EQ5D.

Note. A decrease in score indicates an improvement in symptom scoring while an increase indicates a worsening in symptom scoring.
The IPOS-Renal symptom scores trended for improvements in the symptoms (pain, shortness of breath, weakness, nausea, drowsiness, poor mobility, itching, sleep, restless legs, and changes in skin) for participants in the acupressure group, while the usual care group overall scores showed a slightly worsening symptom burden (Table 4). The overall change score was −2.8 in the intervention group and +1.0 in the usual care group, where a reduction in score is a reported improvement in symptoms.
Pre vs Post Comparisons for Intervention and Control Groups for Specific Symptoms and Total Scores From IPOS-Renal Survey.

Note. A decrease in score indicates an improvement in perceived health rating.
Qualitative Findings
The participant survey provided a qualitative aspect to this study. Fifteen of the 16 intervention participants completed the survey. Thoughts from the patients centered on similar themes, such as the ease of use and feeling a sense of control over their health and symptoms:

One patient shared their thoughts about their lack of change with the self acupressure:

Other general comments were conveyed below by patients regarding their self-acupressure:
No serious adverse effects were reported; however, some mild issues were mentioned, such as bruising (n = 1) and discomfort (cited as pain/numbness/tenderness) to the acupressure sites (n = 4). One patient had 2 separate hospital visits for reasons unrelated to the acupressure protocol. Another patient complained that he injured a rib (stating this was related to an old injury). One patient had a fall early in the study causing bruising to her wrist and arm, thus affecting the ability to administer her self-acupressure. The research team assisted with modifications and suggestions on holding the acupressure tool, and encouraged the patient to work the pressure points on the noninjury hand/wrist instead.
Discussion
To the best of our knowledge, this is one of the first studies to examine the effect of self-administered acupressure on symptoms in HD patients. The retention rate was high (with only one drop out in the acupressure group) and 82% of all potential home sessions were adhered to. The results from this pilot study suggest that self-acupressure was feasible, easy to administer, and acceptable to participants; and may have some role for supporting the management of symptoms in this complex population of HD patients. While small sample size limits the conclusions, there did seem to be a perceived improvement in quality of life and symptoms scores within the acupressure group.
The IPOS-Renal scores suggested improvements in the acupressure group for several symptoms; previous studies have concluded that acupressure has a positive effect on HD-related symptoms.9,13,17,19,21,38 However, all these previous examinations had a practitioner or trained researcher performing the acupressure on the patients, making it difficult to compare our findings. A review by Song et al, 33 has outlined self-acupressure studies in long-term disease populations; however, the authors stated they were unable to perform a meta-analysis due to the heterogeneity of populations, protocols, durations, and a lack of standardized outcome measures. There have been reported benefits when using self-acupressure to treat symptoms in non–HD populations.29,32,39-42
There was potentially a difference in the EQ-5D-5L VAS score change when comparing the 2 groups. This was congruent with the work by Lyu et al, 39 in which type 2 diabetic patients improved their quality-of-life scores (QOL) after doing 12 weeks of a 10 site acupressure protocol on themselves. Improvements in QOL with provider-administered acupressure have also been reported in those with ischemic heart disease 42 and in HD patients in a recent Malaysian study in which patients got 8 weeks of either acupressure or zolpidem. 20
The usual care group reported an increase in their perception of anxiety and depression after the 4 weeks; however, this was not an unexpected finding and this may have been impacted by the COVID pandemic lockdown. Some in the acupressure group also had a slight worsening in their anxiety and depression scores in this survey—again this may have been related to the pandemic. Previous reports have shown otherwise and have been successful in improving levels of depression in HD patients7,14,15 or in other long-term disease populations. 43
Our retention rate was high and this is comparable to other self-acupressure reports who tracked both retention and adherence and involved protocols of 4 to 6 weeks in duration.29,32,44 It is not clear if retention would be similar in a longer or with more time-intensive acupressure protocols.
Five patients (30%) commented on mild adverse effects such as bruising and discomfort directly related to the self-acupressure sites. These experiences were consistent with other studies.31,32,44,45 It has been suggested that finger pressure is safer versus use of a wooden tool in those who experienced bruising or soreness at the sites. 31 One patient in our study commented specifically that they would use their fingers instead of the wooden acupressure tool in the future for the same reason, but still found benefit overall.
This pilot study has limitations worth noting. The sample size was small which limits the conclusions that can be drawn and the statistical power. Subjective outcomes will always be subject to bias, but QOL and symptoms are key outcomes in the HD population. The duration of the acupressure protocol was relatively short (i.e., 4 weeks); however, this is in line with other published studies. While dedicated research staff did continue to follow-up each week with ensuring the accurate land marking and adequate pressure for all 6 acupressure points, it is possible patients may not have had as great as impact versus a trained professional. Li et al 31 required patients to pass a fidelity check at their second visit to ensure correct technique, and this may be a valuable aspect to include in methodology for future studies. Finally, although some patients may have only had a few symptoms and thus met inclusion criteria, they were still required to do all 6 acupressure locations in the protocol. This “blanket approach” to dealing with a large number of HD related symptoms may have been a reason for the lack of significant changes in the IPOS-Renal scores. It is not clear if targeting specific acupressure sites for specific symptoms would yield stronger results. Minimal or no changes would likely be noted in those who did not have the symptoms at baseline, potentially diluting the effects.
Future research in this area is warranted, and the results from this pilot study can be used to inform the design of a larger more definitive trial. While there were trends of potential effects on outcomes such as quality of life and symptoms, a larger sample size would allow for inferential statistics and stronger conclusions to be drawn. Considerations for future study design include obtaining details on medication use, considering an attention control where control participants receive similar levels of attention from staff, and the application of a sham intervention where participants in the control group receive sham acupressure therapy on nonspecific acupoints. A design that allows for blinding of health care practitioners would also increase the rigor as well as clearly standardizing usual care as it pertains to HD symptom management.
Conclusion
The results from this study suggest that self-acupressure may have a role for managing symptoms in HD patients. Self-acupressure is an example of a nonpharmacological self-management tool that is convenient, has potential for reducing the symptom burden, and may improve quality of life. These techniques are free of cost and easy for HD patients to administer, with little adverse side effects. Future examinations can build on the results of this study and should engage larger HD patient populations.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581241267164 – Supplemental material for The Feasibility and Effects of Self-Acupressure on Symptom Burden and Quality of Life in Hemodialysis Patients: A Pilot RCT
Supplemental material, sj-pdf-1-cjk-10.1177_20543581241267164 for The Feasibility and Effects of Self-Acupressure on Symptom Burden and Quality of Life in Hemodialysis Patients: A Pilot RCT by Kristen Parker, Shauna Raugust, Becky Vink, Kuljit Parmar, Allan Fradsham and Marni Armstrong in Canadian Journal of Kidney Health and Disease
Footnotes
Ethics Approval and Consent to Participate
Ethics approval was granted by the Research Ethics Board at the University of Alberta (ID: REQ00007147). Informed consent was obtained from all participants.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded and supported through the Alberta Health Services Research Challenge Program. This work was also supported through the Kidney Health Section of the Medicine Strategic Clinical Network with Alberta Health Services.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.