
Abstract
Background:
Nontargeted renal biopsy is essential to diagnosis, classification, and prognostication of medical renal disease. Inadequate biopsies delay diagnosis, expose the patient to repeated biopsy, and increase costs.
Objective:
The purpose of this project is to characterize nontargeted renal biopsy specimen adequacy and identify areas for improvement.
Design:
This project was designed as a clinical audit of specimen adequacy rates of nontargeted renal biopsies from 13 hospitals, as well as a questionnaire of radiology and pathology department staff regarding current practices surrounding renal biopsies.
Setting:
Retrospective analysis of 2188 adult native renal biopsies was performed from January 1, 2018, to September 9, 2021, across 13 hospitals.
Patients:
Adult patients with medical renal disease undergoing a nontargeted renal biopsy were included.
Methods:
Retrospective analysis of 2188 adult native renal biopsies was performed from January 1, 2018, to September 9, 2021, across 13 hospitals. Adequacy was divided into 4 categories based on number of glomeruli received: ideally adequate (≥25 glomeruli), minimally adequate (15-24), suboptimal (<15 and diagnosis rendered), and inadequate (<15 and no diagnosis rendered). Two targets were chosen; target 1, to achieve a combined suboptimal and inadequate rate ≤ 10%, and target 2, to attain an ideally adequate rate ≥80%. Radiology department heads in the province were surveyed on biopsy equipment, technique, technologist support, and feasibility of possible interventions to enhance biopsy adequacy. Pathology department staff were surveyed on their education and experience.
Results:
Adequacy was as follows: ideally adequate 64.7%, minimally adequate 26.0%, suboptimal 7.9%, and inadequate 1.4%. The province (and 8/13 hospitals) met target 1 for native biopsies (9.3%). Two hospitals achieved target 2 for native biopsies. A key finding was that the 2 hospitals with the lowest target 1 scores did not have a technologist present at biopsy.
Limitations:
Survey data was used to assess biopsy technique at each hospital, and specific technique for each biopsy was not recorded. As such, a multivariate statistical analysis of specimen adequacy rates was not feasible. Data on complications was not collected.
Conclusions:
Preintervention the province was at target for limiting inadequate and suboptimal native biopsies. There was a substantial shortfall in the ideally adequate rate from the proposed target. Using insight from survey data, interventions with the greatest expected impact were identified and those that are feasible given limited resources will be implemented to improve sample adequacy.
Trial Registration:
Not registered.
Introduction
Renal biopsies enable diagnosis and classification of medical kidney disease, which guides treatment and prognostication. Inadequate biopsy delays diagnosis and treatment, exposes patients to the risks of repeated biopsy, and increases health care costs.
For nontargeted renal biopsy when there is no mass lesion, the aim is to collect sufficient cortex, the site of glomeruli, and medical renal disease. 1 For native kidneys, an adequate sample is typically defined by having sufficient tissue for diagnosis. However, this definition does not address the amount of tissue required to exclude the possibility of focal disease in the context of negative findings, nor does it include the ability to provide prognostic information for long term kidney function. As a result, no standard criteria for native renal biopsies are widely accepted. Bearing this in mind, the reported rates of native kidney biopsy specimen adequacy range from 90% to 99%.2-5 Audit and quality improvement interventions have been shown to result in significant improvement in rates of suboptimal biopsy adequacy. 5
In the province, adult nontargeted renal biopsies are performed at 13 independent hospitals, placed in fixatives, and then transported to a central specialized renal pathology laboratory for further processing and pathologist review. Kidney biopsy adequacy was not previously quantitated in a way that was meaningful for pathology and radiology to understand and improve overall quality. This concern was raised to a government medical imaging advisory committee. In response to this concern, pathology and radiology collaborated to propose standards for specimen adequacy and collected data on biopsy technique and sample adequacy. Results were presented to the medical imaging advisory committee for review and to identify opportunities for improvement. This project was designed utilizing previously published audit templates.6-8
Methods
Ethical Approval
As this study was a quality improvement project, this project was deemed exempt from clinical research ethics board approval by our institution. Instead, a privacy review was completed with our institutional privacy office, which received approval.
Setting
Adult nontargeted percutaneous native renal biopsies are performed at 13 hospitals across the province. Biopsies targeting a mass lesion for kidney tumor diagnosis were not included. Renal pathology is a provincial service centralized at a single site that processes and diagnoses all medical renal biopsies, both adult and pediatric native and transplant. The pediatric biopsies and transplant biopsies were not included in this study.
Specimen Adequacy Methods
Percutaneous native nontargeted biopsies from January 1, 2018, to April 30, 2021, were retrospectively analyzed for adequacy. No power calculation was performed. Biopsy attempts with no tissue sent to the central lab were not included. Three hospitals that rarely performed biopsies (fewer than 4 per year) were excluded.
Analysis of biopsy adequacy was conducted using aggregate de-identified patient data. Data was stratified by hospital, with each of the 13 sites randomly assigned a letter (A-M) for the purpose of anonymity.
Renal biopsy evaluation includes tissue collection by radiology and tissue allocation into the various fixatives by pathology. The focus of this quality review was on tissue collection, and thus, specimen adequacy was defined based on the total number of glomeruli collected by radiology in the total tissue sample. The number of glomeruli were determined microscopically by adding the total number of glomeruli for light, immunofluorescence, and electron microscopy at the time of pathologist review. The total number of glomeruli included both patent and sclerosed glomeruli because all glomerular pathologies contribute to diagnoses and prognostic information. Extent of chronic findings, including total number of globally sclerosed glomeruli, are important for prognosis of long-term kidney function and were determined by the expert renal pathologists to be essential to the total glomerular count. The number of cores and core volume were not recorded. The collecting sites do not all record total number of cores collected, and tissue cores can fragment in transit so number of cores received in the centralized lab is not an accurate indicator of number of cores collected. The number of cores does not correlate with biopsy adequacy as core totals do not account for amount of medulla sampled, which is considered inadequate tissue that does not contribute to diagnosis or prognosis because medulla does not contain glomeruli, proximal tubules, or larger vessels. Core volume was not an option because it does not account for variance in needle gauge and core diameter.
Definition of specimen adequacy
Category 1, Ideally adequate: ≥25 glomeruli total, diagnosis and prognostics can be rendered.
Category 2, Minimally adequate: 15-24 glomeruli total, diagnosis and at least some prognostics can be rendered.
Category 3, Suboptimal: <15 glomeruli total, diagnosis can be rendered but no prognostics.
Category 4, Inadequate: <15 glomeruli total, no diagnosis or prognostics can be rendered.
Specimen adequacy was based on provincial renal pathologists’ expert opinion and best practice as per recent literature. The rationale for these definitions is as follows. For categories 1 to 3, there is a diagnosis. For category 1, classification and prognostic determinations can be made. For categories 2 to 4, classification and/or prognostic determinations are incomplete or not possible to determine. The number of glomeruli needed in light microscopy for diagnosis is variable, but generally 15 to 20 glomeruli is regarded as sufficient for confidence in diagnosis as well as providing an appropriate sampling of glomeruli for accurate appropriate classification systems for various diseases, such as the International Society of Nephrology/Renal Pathology Society classification of lupus nephritis or the Oxford classification for IgA nephropathy. These classification systems provide important prognostic information and guide patient treatment and management. However, medical renal disease can be focal (ie, involving only a few glomeruli), and 25 glomeruli may be needed for light microscopy to have greater than 95% chance of detecting those processes.9,10 At least 1 glomerulus each is required for immunofluorescence and electron microscopy, and 2 to 3 glomeruli are preferred for each. The need for sufficient glomeruli for analysis must be balanced with the higher risk of complications when multiple biopsies are performed. 11
The number total of glomeruli collected was defined as the sum of glomeruli (patent and sclerosed) in all core biopsy samples provided per patient to the pathology lab. Sclerosed glomeruli as well as patent glomeruli were considered adequate because chronicity is an important prognostic factor for patient dialysis and transplant, and a high percentage of globally sclerosed glomeruli in the context of severe interstitial fibrosis and tubular atrophy is diagnostic for end stage kidney disease. How local pathology laboratories allocated the biopsy tissue for each type of microscopy did not affect the adequacy category as this is a separate quality project and this project focuses on collection. The number of arteries was not recorded.
The provincial renal pathologists determined the appropriate adequacy category based on their prospective evaluation of the number of glomeruli for light, immunofluorescence and electron microscopy, which is included in every pathology report.
Targets
The audit aimed to calculate 2 metrics:
Inadequate and suboptimal categories: target of ≤10% of biopsies.
Ideally adequate category: target of ≥80% of biopsies.
Target 1 was chosen as a proxy to specimen adequacy in the Bethesda system for thyroid fine needle aspiration, where a combined rate of nondiagnostic and unsatisfactory <10% is the target.11,12 Target 2 was chosen retrospectively upon initial analysis of the data, and arbitrarily as a realistic value given 2 hospitals achieved this level.
Analysis of specimen adequacy
The percentage of ideally adequate, minimally adequate, suboptimal, and inadequate was calculated for the preintervention period. Associations between biopsy technique and specimen adequacy were evaluated using a 1-way analysis of variance test. A p-value < 0.05 was considered statistically significant. No multivariate analysis was performed. Calculations were performed using GraphPad Prism v9.2.0 (San Diego, CA, USA).
Survey Methods
Radiology Survey
Objective and target population
The survey’s research objective was 2-fold: (1) to identify the specific biopsy technique and resources available at a hospital and (2) to assess subjective feasibility and preference for possible interventions to improve specimen adequacy rate. The target population was operators performing renal biopsies in adults. A closed survey, nonrandom sampling frame of radiology department heads was chosen, to answer on behalf of their colleagues performing biopsies. The survey was chosen to be not anonymous as hospital identification was necessary to help characterize any associations between biopsy techniques and specimen adequacy.
Development
Questionnaire development was guided with input from a renal pathologist, pathology technician, abdominal radiologist with experience in renal biopsy quality improvement, literature review of biopsy techniques and the medical imaging advisory committee. The survey is provided in Supplemental Appendix 1. Questions were grouped into 5 domains (respondent information, equipment factors, operator factors, complications, and quality improvement), with 28 questions, in accordance with published survey design recommendations. 13
There have been many publications focused on the impact of technical factors on biopsy yield, so a number of these questions were in the survey. End-cut needles have been shown to have better glomerular yield per core sample than side-notch needles. 14 Similarly, coaxial technique was shown to have better glomerular yield than noncoaxial technique in a randomized clinical trial. 15 Needle gauge is a somewhat controversial topic, with some published results indicating improved yield with a larger bore without increased complications, while others showing a larger bore is associated with a higher rate of complications.16,17
Administration
The survey was distributed via email on December 17, 2020. Response collection was closed on February 17, 2021, when all responses had been received. Qualtrics survey software (Qualtrics, Utah, USA) was utilized.
Response rate
Response rate was defined as the number of radiology department heads who responded (numerator) divided by the number of radiology department heads who were sent the survey (denominator). Completion was not mandatory and no incentives were offered.
Analysis
No questionnaires were excluded from the analysis. The unit of analysis was the hospital. Descriptive and inferential analysis methods were applied. Survey responses were manually entered into a database.
Pathology Survey
Additionally, the pathology department participated in an informal 21 question online survey. The purpose of the survey was to gather information on biopsy technique from the technologists’ perspective, including set up, assessment and allocation practices, and interest in proposed QI interventions. This was distributed electronically by laboratory management to general staff (both pathologists and technologists) in June 2021, and the end of survey collection was July 2021. Questions were written in a multiple-choice format, and questions are provided in Supplemental Appendix 2.
Results
Specimen Adequacy
A total of 2188 native renal biopsies were performed during the 28-month period. Province-wide adequacy and average number of glomeruli over the preintervention period is summarized in Table 1, and adequacy over time is displayed in Figure 2. Of the biopsies, 64.7% were ideally adequate, 26.0% were minimally adequate, 7.9% were suboptimal, and 1.4% were inadequate. By hospital site, rates of ideally adequate ranged from 45.0% to 87.7%, minimally adequate 10.0% to 42.5%, suboptimal 0.0% to 19.5%, and inadequate 0.0% to 5.0%. Target 1 (inadequate and suboptimal ≤ 10%) was achieved by the province, with a rate of 9.3%. Eight of 13 individual hospitals reached target 1. Target 2 (ideally adequate ≥ 80% of biopsies) was not achieved by the province, but was achieved by 2 hospitals.
Summary of Specimen Adequacy of Native Renal Biopsies.


Province-wide specimen adequacy variance during the preintervention period. Adequacy category data plotted by average percentage each month.
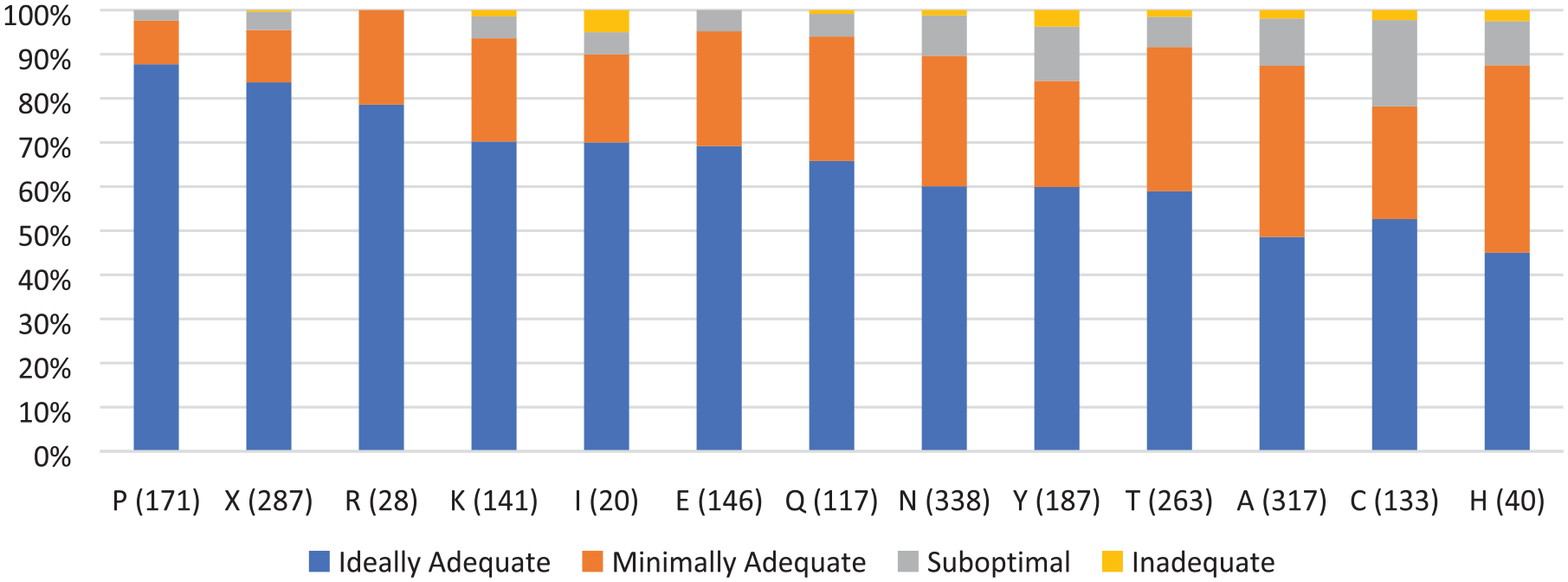
Individual hospital site specimen adequacy. Hospital sites are de-identified and displayed by a randomly selected letter. The number in brackets next to the hospital site letter is how many biopsies were performed by that hospital site during between January 1, 2019, and April 30, 2021.
Survey Data
Radiology survey
A response rate of 100% (13/13 radiology department heads) was achieved. All questionnaires were completed in full, except for the last question which was an optional written response to provide ideas not already mentioned for quality interventions, which was completed by 31% (4/13) of respondents. On average, respondents represented 10.8 radiologists per hospital whom performed renal biopsies.
Results on preintervention biopsy technique, operator, support from pathology and complications are summarized in Table 2. To highlight findings of note:
Most departments used ultrasound guidance (92%), 18-gauge needles (92%) and semi-automatic biopsy guns (92%).
A minority of departments used 16-gauge (8%), full cores (31%), and co-axial systems (38%).
Most departments determined the number of core biopsies to acquire based on microscopy findings communicated by the technologist during the procedure (69%). A few departments took a standard number of cores (31%).
About half of the departments received feedback on specimen adequacy via formal written reports (46%). Department heads were most interested in being provided with a one-sentence summary of any issues with adequacy (92%).
Four hospitals are not able to handle significant complications (eg, hemorrhage requiring embolization), and are located 9, 66, 108, and 529 km by road away from the nearest hospital able to perform such a procedure respectively.
Radiology Department Head Survey Data on Preintervention Biopsy Technique, Personnel, Support From Pathology and Complications.

Results on feasibility of possible interventions are summarized in Table 3. Microscope phone adaptor was not applicable to 11 of the 13 hospitals because a pathology technologist was already available locally for specimen assessment. To highlight findings of note:
All departments not already using 16-gauge needles thought it was feasible to implement; 12 of 12, 100%; 9 (75%) possibly feasible, 3 (25%) easily feasible/preferred.
All departments not already using end-cut (hollow) core biopsy devices thought it was feasible to implement; 8 of 9, 89%; 7 (78%) possibly feasible, 1 (11%) easily feasible, and 1 (11%) unsure.
About half already restricted biopsies to a subset of operators (46%). Among departments that did not restrict biopsies to certain operators, most said it was not feasible (5 of 7, 71%).
Among nonacademic hospitals, only one (1 of 11, 9%) preferred centralization of collection of renal biopsies. Some thought that centralization was not feasible (36%) and listed reasons including the distance required for patients to travel would be too significant.
All departments not already receiving a statement on specimen adequacy thought it was feasible to implement; 8 of 8, 100%; 1 (12%) possibly feasible, 7 (88%) easily feasible/preferred.
Radiology Department Head Survey Data on Estimated Feasibility of Various Quality Improvement Interventions.

Data listed as number of hospital sites.
Pathology survey
The survey received 26 responses from 10 different hospitals performing renal biopsy (response rate unknown). Most respondents were technologists (20; 83.3%), and a minority were pathologists (4; 6.7%). Twenty (77%) participants had specialized training, including anatomical pathology (11; 42%), hematology (5; 19%), medical lab technologist (2; 8%), cytology (1; 4%), and pathologist assistant (1; 4%).
The majority stated that the number of cores taken was guided by adequacy evaluation at the time of biopsy (18; 69%) while a minority used a standard of either 3 or 4 cores (6; 23%); 2 respondents did not answer the question. Likewise, the location of tissue assessment was at bedside for most (18; 69%). However, 6 (23%) respondents mentioned samples had to be taken to the lab for analysis, with an associated time delay ranging from approximately 10 to 30 minutes.
When asked which factors play a role in determining adequacy and multiple response could be chosen, 73% (19) selected total glomeruli, 69% (18) selected presence of cortex, 65% (17) selected core length, and 62% (16) selected total cores. In rating their confidence in determining adequacy, 69% (18 of 26) were somewhat confident or very confident in determining cortex versus medulla, 85% (22 of 26) were somewhat/very confident determining presence of glomeruli, and 50% (13 of 26) were somewhat/very confident in determining number of glomeruli.
Method of tissue allocation varied, with 50% (13) using certain lengths of tissue per container, 5 (19%) certain number of glomeruli per container, 1 (4%) case-by-case basis, 1 “few glomeruli each,” 4 (15%) 1 core per container, and 2 (8%) nonrespondents.
Discussion
In this preintervention period, target 1 (inadequate and suboptimal ≤ 10%) was achieved by the province with an overall rate of 9.3%, and individually achieved by 8 hospitals. Target 2 (ideally adequate rate ≥ 80%) was more challenging, and overall, the province only achieved a rate of 64.7%. However, 2 hospitals reached target 2, suggesting that it is attainable.
The radiology survey was completed by all hospitals (100% response rate). It provided a useful snapshot of biopsy equipment, technique, personnel involved in the procedure and feasibility of potential interventions. In particular, the survey highlighted that the 2 hospitals with the highest combined rate of inadequate and suboptimal biopsies (ie, worst target 1 performance) were the 2 hospitals without a pathology technologist present during biopsy. One of these sites averaged 60 biopsies per year, and the other 30 biopsies per year. This underscored the value of technologists and supports, their education and knowledge of local specimen adequacy standards, concordant with a published prospective review of renal biopsies. 18 Furthermore, a similar quality improvement project doubled their specimen adequacy rates after introduction of contemporaneous pathology technologist review. 5 Data from the pathology survey was complimentary to the radiology survey data; it indicated there was variable collection and assessment procedures and techniques among different hospitals. Ideally radiology survey data would have been gathered prospectively at the time of each individual biopsy, on an observational basis, but this was deemed not be practical in practice. By surveying a small group (13 radiology department heads) we were able to quickly achieve a 100% response rate and ensure a reasonably high quality of survey responses, both of which were anticipated to be lower had we surveyed all biopsy operators (approximately 140 radiologists) instead.
Native kidney adequacy rates are not easily directly compared to the literature because there are no consensus criteria for specimen adequacy. This reflects the challenge in assigning definitions for all biopsies, which does not take into account that the number of glomeruli needed varies based on the underlying pathology and clinical question. For instance, higher numbers of glomeruli are useful to improve diagnostic confidence in excluding a disease. Some papers define adequacy vaguely as having sufficient tissue to render a diagnosis. Recently published renal biopsy guidelines helped determine the specimen adequacy definitions.9,10
For instance, Korbet et al 4 reported a specimen adequacy rate of 99%, which is maintained at 98% when requiring ≥10 glomeruli but falls to 76% when requiring ≥20 glomeruli. In our study, we chose to have 2 levels of adequacy (ideally adequate defined by ≥25 glomeruli and minimally adequate defined by 15-24 glomeruli) because our aim was to provide not only diagnosis but also have enough glomeruli for kidney disease classification and prognosis. Although our suboptimal category (<15 glomeruli) yielded a diagnosis, we do not consider it adequate because of its lack of prognostic information. For example, a diagnosis of IgA nephropathy could easily be made with 6 total glomeruli but an Oxford classification cannot be provided (Oxford paper) and important prognostic and treatment information is absent. One study from a Canadian university in a different province had a somewhat similar definition of adequacy, defined as > 12 glomeruli. 5 They achieved a preintervention native kidney adequacy of 31%, which improved to 90% after 2 phases of interventions. Preintervention, our province had 90.7% of native biopsies with ≥15 glomeruli (minimally and ideally adequate categories combined). Since our study is designed to improve biopsy adequacy in collection, we chose to avoid classifying the number of glomeruli required for light microscopy, electron microscopy and immunofluorescence separately. The approach of dividing adequacy for each of these diagnostic modalities has been variably applied in the literature and is somewhat controversial given that redistribution of tissues into various fixatives is possible but comes with limitations including specimen artifacts. We chose to exclude allocation of tissue and simplify our definition instead to specifically what the operator needs to acquire for an adequate specimen collection.
An unanticipated benefit from this project was that the pathology department re-developed their biopsy data database to allow real-time entry of specimen adequacy details, which theoretically will allow efficient monitoring of specimen adequacy and facilitate regular audits, an important quality assurance activity. Adequacy rates are not intended to factor into accreditation or individual operator status, rather as a feedback model.
There are several limitations to the survey and preintervention data. Survey responses from department heads rather than true observational data were used to assess hospital techniques, which may decrease accuracy. The survey did not quantify differences in patient populations undergoing biopsy at each site, which may factor into varying adequacy rates. A multivariate statistical analysis of the data was not performed, and as such the results described are descriptive. Procedural complications were not recorded. Biopsies were only included in specimen adequacy rates if the lab received tissue, such that biopsies terminated prior to tissue collection (for example due to a complication) would be underestimated. Without generally accepted criteria for native kidney specimen adequacy in the literature, comparison between our data and other publications cannot be easily made.
The next step for this quality improvement project is to carry out the proposed interventions and record specimen adequacy in period 2. Several potential interventions were discussed in the survey. Hiring new pathology technologists at sites without a staff currently filling this position may not be feasible due to resource limitations, but further education of existing staff is a possibility. One intervention that the authors hope to implement is a standardized biopsy kit for all sites. Survey data indicated there was variable collection and assessment procedures and techniques, and local pathology technical leads indicated high interest in such a kit. These kits will provide both physical specimen containers and written instructions on biopsy assessment, allocation, and whom to contact for assistance.
There are several logical future directions for research and audits in this field. Consensus definition on native renal biopsy specimen adequacy would aid significantly in standardizing research and identify realistic targets. Furthermore, a similar analysis of renal allograft biopsies in the province is on the horizon. In addition, further research into effect of individual interventions on adequacy is worthwhile, and variabilities can be easily compared head-to-head (eg, full core vs hollow core biopsies). This audit focuses on adequacy, and an audit of biopsy complications could be considered.
Conclusion
Renal biopsy is a key component in the diagnosis of medical renal disease. In an attempt to improve disease classification and prognostic information, new rigorous medical renal biopsy adequacy definitions were implemented. The province achieved target 1 (suboptimal and inadequate ≤ 10%) for native biopsies. Only 2 hospitals reached target 2 (ideally adequate ≥ 80%) for native biopsies, with the province lower overall (64.7%). A survey of radiology department heads and pathology department staff provided insight into current practices and variation in adequacy between sites. The next step is to monitor quality improvement interventions and assess post-intervention specimen adequacy.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581231205161 – Supplemental material for Nontargeted Native Renal Biopsy Adequacy: Preintervention Data From a Province-Wide, Multicentre, and Interdepartmental Audit
Supplemental material, sj-docx-1-cjk-10.1177_20543581231205161 for Nontargeted Native Renal Biopsy Adequacy: Preintervention Data From a Province-Wide, Multicentre, and Interdepartmental Audit by James P. Nugent, Mei Lin Z. Bissonnette, Brian Gibney, Myriam Farah and Alison C. Harris in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-2-cjk-10.1177_20543581231205161 – Supplemental material for Nontargeted Native Renal Biopsy Adequacy: Preintervention Data From a Province-Wide, Multicentre, and Interdepartmental Audit
Supplemental material, sj-docx-2-cjk-10.1177_20543581231205161 for Nontargeted Native Renal Biopsy Adequacy: Preintervention Data From a Province-Wide, Multicentre, and Interdepartmental Audit by James P. Nugent, Mei Lin Z. Bissonnette, Brian Gibney, Myriam Farah and Alison C. Harris in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We would like to thank members of the BC Provincial Renal Pathology Laboratory and the Physician Quality Improvement initiative for their tireless contributions to data collection and analysis. In particular, we would like to thank Bobby Grewal, the Team Lead for Anatomic Pathology at St. Paul’s Hospital for his dedication and leadership.
Ethical Approval/Patient Consent
As this study was a quality improvement initiative, the institutional clinical ethical board exempted the study from REB approval, and recommended privacy approval. As such, privacy approval was obtained through our institution’s privacy review office.
Author Contributions
Conceived and designed the analysis: JPN, MLZB, BG, MH, ACH
Collected the data: JPN, MLZB
Contributed data or analysis tools: JPN, MLZB, ACH
Performed the analysis: JPN, MLZB
Wrote the paper: JPN, MLZB, BG, MH, ACH
Other: N/A
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.