
Abstract
Background:
Chronic kidney disease of uncertain etiology (CKDu) is an emergent health concern, particularly in tropical farming communities in several global hotspots, including Sri Lanka. This particular nephropathy is characterized by a progressive decline in kidney function in the absence of conventional chronic kidney disease (CKD) risk factors such as diabetes mellitus, hypertension, and other identifiable kidney disorders. As it is almost asymptomatic at early stages, CKDu is mostly diagnosed at late stages with significant kidney damage. Hence, the identification of disease susceptibility and vulnerable communities at the earliest possible instances is highly important for the management of the disease.
Objective:
We aimed to compare kidney health across three different farming communities in Sri Lanka to identify CKDu susceptibilities.
Methods:
A cross-sectional study was performed with three selected farming communities: paddy farmers (PF; N = 581), sugarcane farmers (SF; N = 550), and vegetable farmers (VF; N = 244) in comparison with an age-matched control group of nonfarming (NF; N = 225) individuals. A medical examination was performed to investigate health status and medical history, whereas a urinalysis was performed to determine creatinine and albumin contents. Estimated glomerular filtration rate (eGFR) and urinary albumin-creatinine ratio (ACR) were used for assessment of kidney function. CKDu susceptibility was determined based on eGFR, and urinary ACR adhering to the clinical practice guidelines in Sri Lanka.
Results:
The median (interquartile range [IQR]) eGFR levels of PF (85 mL/min/1.73 m2 [72-97]) and SF (93 mL/min/1.73 m2 [73-112]) were significantly lower than that of the NF group (103 mL/min/1.73 m2 [87-125]) (P < .0001), whereas eGFR of VF (100 mL/min/1.73 m2 [80-111]) was not significantly different compared with NF. The median (IQR) urinary ACR levels of the study groups, PF, SF, VF, and NF, were 0.59 (0.26-1.45), 0.46 (0.28-0.88), 0.45 (0.34-0.90), and 0.44 (0.34-1.02) mg/mmol, respectively. However, urinary ACR did not differ significantly across the study groups (P > .05). The prevalence of CKDu within PF (13.60%), SF (12.54%), and VF (6.67%) communities was significantly higher (P < .05) compared with the NF (2.67%). Of the total CKD cases, CKDu susceptible cases represented 73%, 69%, 50%, and 25% in PF, SF, VF, and NF, respectively, indicating a high risk of CKDu susceptibility among farming communities. Moreover, a noteworthy association of CKDu was observed with agrochemical exposure (odds ratio [OR] = 3.11, 95% confidence interval [CI] = 1.36-7.09). Concerning the farming practices, sugarcane farming showed the highest association with CKDu prevalence (OR = 3.40, 95% CI = 1.49-7.78).
Conclusions:
Compared with the nonfarming group, a significant risk of CKDu was observed in the three farming communities, particularly among paddy and sugarcane farmers. Longitudinal epidemiological studies to identify vulnerable farming communities and associated risk factors are critically needed to develop effective management strategies against CKDu within farming communities.
Introduction
Chronic kidney disease (CKD) is a disease characterized by progressive deterioration of kidney function over time. According to recent estimates, the global prevalence of CKD is known to be 13.4% (95% confidence interval [CI] = 11.7%-15.1%) with 4.9 to 7 million patients with end-stage kidney disease requiring kidney transplants. 1 Estimated glomerular filtration rate (eGFR), serum creatinine (sCr), and urinary albumin-to-creatinine ratio (ACR) are the main parameters used for diagnosing and monitoring the progression of the disease. According to the current clinical guidelines, CKD is defined as eGFR < 60 mL/min/1.73 m2 and/or urinary ACR ≥ 3.39 mg/mmol present for at least 3 months. 2 Diabetes, hypertension, glomerulonephritis, and hereditary diseases such as polycystic kidney disease account for the majority of CKD globally. More recently, CKD of uncertain etiology (CKDu), which is not associated with the above causes, is emerging in epidemic proportions from multiple global hotspots. These include Central America, Sri Lanka, India, and Egypt. 3 This disease is characterized by chronic tubulointerstitial nephritis and is exceptionally prevalent among farming communities belonging to lower socioeconomic strata. Therefore, recently it was also termed as Chronic Interstitial Nephritis in Agricultural Communities (CINAC). 4 Naturally occurring and anthropogenic nephrotoxic substances, heat stress and dehydration, infections such as hantavirus and leptospirosis, and genetic susceptibility have been proposed with scientific justifications as potential etiologies while the association of agrochemicals with CKDu is a concern of wide discussion. 3
Chronic kidney disease of uncertain etiology in Sri Lanka was first reported in the early 1990s among middle-aged paddy farmers living in the North Central Province (NCP). 4 Subsequently it was reported in other parts of the country, including adjacent North Central and the Uva provinces. To date, CKDu is increasingly reported in the dry climatic zone in Sri Lanka, and the current epidemiology of chronic kidney diseases, particularly CKDu, 5 is elaborated in Figure 1. More recently, CKDu has been reported from the sugarcane and paddy farming communities living in other areas in the dry climatic zone. However, the exact prevalence of CKDu and the associated socioeconomic burden may be underreported in the communities due to the lack of adequate epidemiological studies. 6
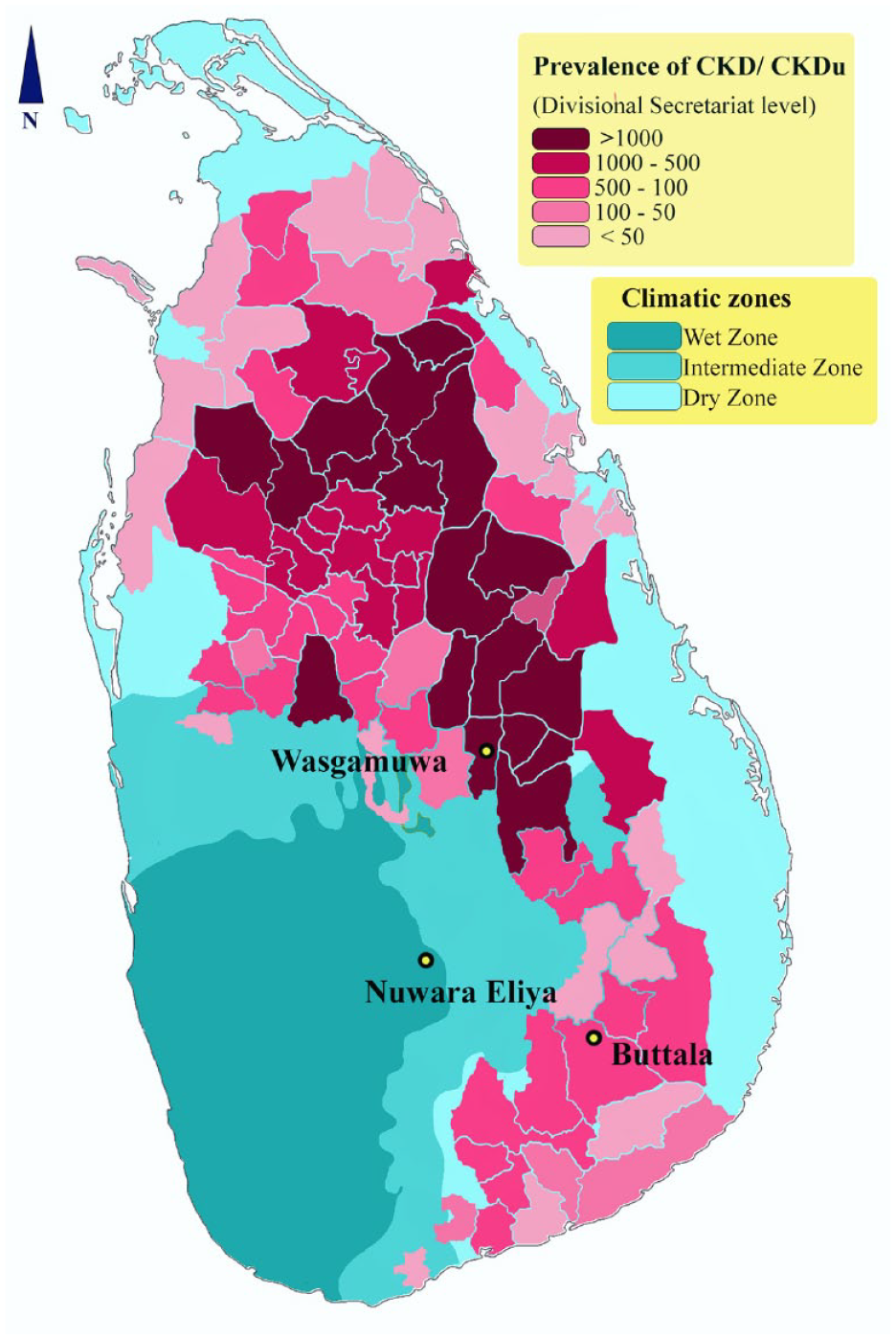
Epidemiology of chronic kidney diseases, including CKDu, in Sri Lanka.
Early diagnosis of CKDu is the key to timely interventions. As the disease is asymptomatic and relatively nonproteinuric in the initial stages, this is often difficult. The absence of usual risk factors of CKD and the lack of regular medical checkups have made it even more challenging. 7 The main focus of this study was to screen different farming communities within dry and wet climatic zones in Sri Lanka for impaired kidney function, and to study environmental risk factors associated with kidney health in these farming communities.
Methods
Study Settings and Participants
We conducted a cross-sectional study with participants representing 3 agricultural communities in Sri Lanka and compared their kidney health with individuals who are not involved in agricultural practices. Based on cultivation statistics, we selected 3 districts where paddy, sugarcane, and vegetable farming are predominant in Sri Lanka. Paddy farmers from Wasgamuwa (Polonnaruwa District, North Central Province), sugarcane farmers from Buttala (Moneragala District, Uva Province), and vegetable farmers from Nuwara Eliya (Nuwara Eliya District, Central Province) were recruited for the study using a multistage stratified cluster sampling approach. Within the selected districts, we identified Grama Niladhari divisions (GNDs; the smallest unit of public administration in Sri Lanka) where more than 50% of inhabitants are involved in the farming of selected crops. Three GNDs were randomly selected from them for the recruitment of participants. Lists of registered paddy, sugarcane, and vegetable farmers maintained at divisional agricultural offices were used for the selection of participants for farming groups, based on systematic random sampling. The initial selection included 640 paddy farmers, 625 sugarcane farmers, and 260 vegetable farmers. Individuals who did not involved in farming were selected from the same regions based on systematic random sampling, using the electoral registries of the respective GN divisions. The inclusion criteria were continuous residency in selected areas for 10 years, being a male or female below 60 years of age, active involvement in farming for a period of 10 consecutive years (for the farming groups), being an individual not involved in a farming-related occupation or unemployed residing within the selected GN divisions (for the control group), and expressed consent for medical examination, and provision of data and samples. The exclusion criteria were being a patient already diagnosed with kidney disease or receiving treatments. An overview of the sampling strategy is summarized in Figure 2.

An overview of the study design and sampling strategy.
Out of the final selection, 581 paddy farmers, 550 sugarcane farmers, 244 vegetable farmers, and 225 age-matched nonfarmers participated in the initial screening.
Data and Sample Collection
Demographic data along with details on medical history, lifestyle habits, occupational and environmental risk factors, and sources of drinking water were collected using an interviewer-administered pretested questionnaire. Participants’ current health status, comorbidities, medications, and medical reports were also examined for the collection of related data. Furthermore, the height and weight of each participant were measured using a portable stadiometer and digital scale, respectively. Resting blood pressure was measured using a standard mercury sphygmomanometer.
A nonfasting blood sample was collected into a sterile serum-separator tube (5 mL), and an early morning first void nonfasting urine sample was collected into a sterile container (50 mL) from each participant. Qualified physicians and nursing professionals involved in medical examination, measuring physiological parameters, and blood sampling.
Sample Preparation and Analysis
Following collection, blood samples were kept standing for 1 hour for coagulation. The coagulated blood samples were centrifuged at 3500 rpm for 20 minutes at 37°C and isolated serum was transferred into sterile plain vacutainer tubes. Urine samples and isolated serum were temporarily stored at 2°C to 4°C during the transit to the laboratory where the biochemical analysis was undertaken immediately. Urine samples were centrifuged at 1000×g for 10 minutes before the analysis.
Serum samples were analyzed for creatinine, and urine samples were analyzed for creatinine and microalbumin. The biochemical analysis of serum and urine samples was performed using an automated biochemistry analyzer (HumaStar 100; Human mbH, Wiesbaden, Germany) in the biochemistry laboratory of the Department of Zoology, Faculty of Science, University of Ruhuna Sri Lanka. Prior to analysis, the biochemistry analyzer was calibrated using standard calibrators, and quality control was done using specific calibrators and quality control regions given by the manufacturer. Urinary glucose concentration was assessed onsite using urine dipsticks test using in-vitro diagnostic (IVD) test strips (Combina 13; Human mbH) and a strip reader (Combilyzer 13; Human mbH). The strip reader was calibrated before the analysis, using the calibration strip given by the manufacturer.
Diagnostic Criteria
Urinary ACR, serum creatinine (SCr), and estimated glomerular filtration rate (eGFR) were used for the assessment of kidney function and damage. Albuminuria was defined as ACR ≥ 3.39 mg/mmol. The participants with a 1-time measurement of eGFR < 60 mL/min/1.73 m2 and/or urinary ACR ≥ 3.39 mg/mmol were considered as suspected CKD according to KDIGO guidelines 2 Estimated glomerular filtration rate (eGFR) was determined using CKD-EPI creatinine equation (2021). 8
Hypertension was defined as either systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg. 9 Obesity was defined in terms of body mass index (BMI ≥ 27 kg/m2). 10 Subjects with a fasting venous glucose concentration above 7 mmol/L were considered as having diabetes mellitus. 11 Individuals categorized as suspected CKD but not having diabetes mellitus, hypertension, or other identifiable cause of CKD were classified as suspected CKDu according to the case definition guidelines adopted by the Sri Lanka Society of Nephrology. 12
Data and Statistical Analyses
The clinical and demographic data were analyzed for normality with the Shapiro-Wilk test. Data showed significant deviations from normality; hence, a nonparametric approach was adopted for statistical analysis. Continuous variables were reported as median with interquartile range, whereas categorical variables were reported as proportions. Age-matched controls were recruited from each of the GN divisions where farmers were recruited from. As there were no significant differences in renal biomarkers (SCr, eGFR, and ACR) among the control groups from different GN divisions, they were considered as a single control group (NF) for comparison with farming groups.
Kruskal-Wallis one-way analysis followed by Dunn’s multiple comparison was used for intergroup comparison of clinical and demographic parameters. A χ2 test was adopted for the comparison of proportions. Spearman correlation analysis was performed to assess the associations of the studied risk factors with ACR and eGFR. A multivariate logistic regression analysis was carried out to assess the effects of selected risk factors on the likelihood of CKD and CKDu in the participants (separately for CKD and CKDu). Hypertension, diabetes mellitus, sex, lifestyle habits (alcohol consumption, smoking, and chewing betel), agrochemical exposure, use of untreated drinking water, and farming type (PF, SF, and VF) were used in logistic regression as binary (categorical) variables, whereas age, BMI and farming duration were continuous variables. We classified drinking water purity into 4 levels; low: untreated water from reservoirs and rivers; moderate: tube wells, surface wells, and disinfected water from water supply projects; high: bottled water and spring water with no trace of contamination; and very high: filtered water with reverse osmosis or domestic filters. We considered high and very high categories as treated water and low and moderate categories as untreated water to define the variable “untreated drinking water.” Accordingly, we adopted the variable “untreated drinking water” in logistic regression as a binary variable. Statistical and data analyses were performed using IBM SPSS Statistics 26.0 (IBM Inc) and GraphPad Prism 9.3 (GraphPad Software LLC).
Results
The key demographic and clinical data of the study participants (paddy, sugarcane, and vegetable farmers and nonfarmers; N = 1580) are presented in Table 1.
Demographic and Clinical Characteristics of the Study Participants.

Note. The prevalence of obesity, diabetes mellitus, and hypertension within communities, and demographic data are expressed as the number of individuals along with its percentage given in parentheses with respect to the total number of participants in each group. Intergroup comparisons of SCr and eGFR are given according to Kruskal-Wallis test, followed by Dunn’s multiple comparison. Comparison of prevalence is given according to the χ2 test. SCr = serum creatinine; eGFR = estimated glomerular filtration rate; ACR = urinary albumin-to-creatinine ratio; BMI = body mass index; IQR = interquartile range; PF = paddy farmers; SF = sugarcane farmers; VF = vegetable farmers; NF = nonfarmers.
Compared with NF.
Compared with VF.
Compared with SF.
Statistical significance: P < .05.
The highest median eGFR was observed in the nonfarming group that was significantly higher than that of the paddy and sugar cane farmers (P < .0001). Among the 3 farming groups, the lowest and the highest median eGFR values were observed in the paddy and vegetable farmers, respectively, with significant differences (P < .05). However, urinary ACR showed no significant differences among the 4 study groups (Figure 3).
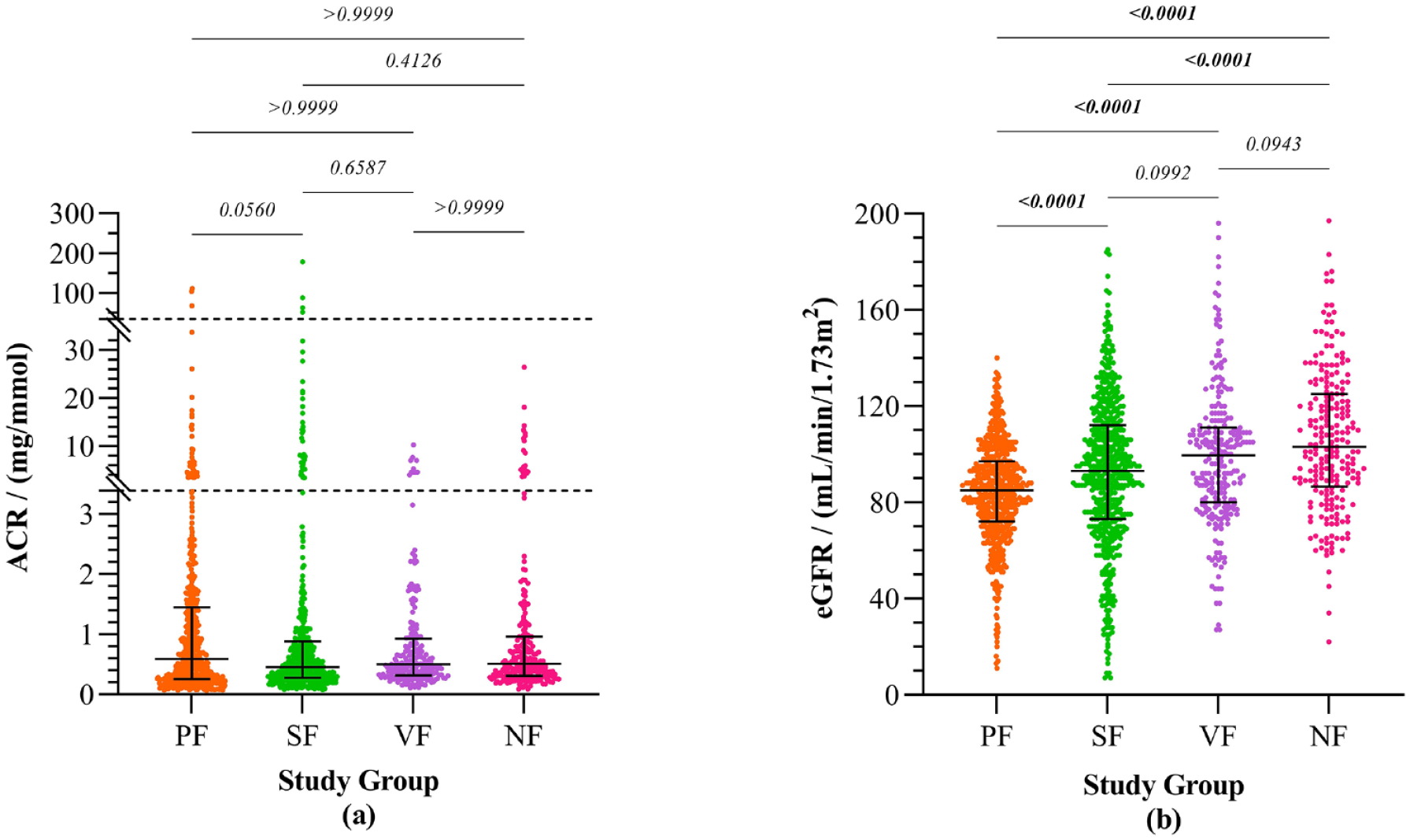
Biomarkers of kidney function of the study groups. (a) urinary ACR. (b) eGFR.
Moreover, the prevalence of the main risk factors of CKD (obesity, hypertension, and diabetes mellitus) was at the highest in the nonfarming group compared with the farming groups with significant differences (Table 1). Detailed interpretations on kidney health and CKD/CKDu susceptibility in the 3 farming groups and the nonfarming group are given in Table 2.
Implications on Kidney Health of the Study Participants, and Susceptibility of CKD and CKDu.

Note. The prevalence of suspected CKD and CKDu in each CKD category within communities are expressed as the number of cases along with its percentage given in parentheses with respect to the total number of participants in each group. Intergroup comparison of prevalence is denoted according to the χ2 test. CKD categories: G1: eGFR ≥ 90 with ACR ≥ 30, G2: eGFR 89-60 with ACR ≥ 30, G3a: eGFR 59-45, G3b: eGFR 44-30, G4: eGFR 29-15, and G5: eGFR < 151. PF = paddy farmers; SF = sugarcane farmers; VF = vegetable farmers; NF = nonfarmers; CKD = chronic kidney disease; CKDu = chronic kidney disease of uncertain etiology.
Statistical significance (P < .05).
Compared with NF.
Compared with VF.
Compared with SF.
The prevalence of suspected CKD was at the highest among paddy and sugarcane farmers compared with the nonfarming group (P < .05). Similarly, the prevalence of suspected CKDu in the 3 farming groups was also higher (P < .05) compared with the nonfarming group. The highest prevalence of suspected CKDu was found among paddy and sugarcane farmers. When expressed as a percentage of total CKD cases, CKDu occupied a high proportion (P < .05) in the farming groups compared with the nonfarming group. The prevalence of the main risk factors of kidney diseases in the study groups is given in Table 3.
Prevalence of Risk Factors for Kidney Diseases Among the Study Participants.

Note. Statistics on smoking, liquor consumption, and chewing betel are based on self-reports. The prevalence of risk factors is expressed as the number of individuals along with its percentage given in parentheses with respect to the total number of participants in respective groups. Intergroup comparison is denoted according to χ2 test (P < .05). Drinking water quality—low: untreated water from reservoirs and rivers; moderate: tube wells, surface wells, and disinfected water from water supply projects; high: bottled water and spring water with no trace of contamination; and very high: filtered water with reverse osmosis or domestic filters. PF = paddy farmers; SF = sugarcane farmers; VF = vegetable farmers; NF = nonfarmers.
Significant compared with VF.
Significant compared with SF.
Significant compared with NF.
The prevalence of habitual liquor consumption and smoking was significantly higher (P < .05) among farming communities compared with the nonfarming group. The highest prevalence of habitual liquor consumption and smoking was observed in vegetable farmers compared with the other 3 groups (P < .001). Age was significantly associated with ACR and eGFR in all the study groups. Particularly, age, diabetes mellitus, hypertension, BMI, and agrochemical exposure were significantly associated with ACR and eGFR in the 2 occupational groups: Paddy and sugarcane farming communities had the highest prevalence of suspected CKDu (Supplementary Table 1). The effect of the studied risk factors on the likelihood of having suspected CKD and CKDu is illustrated in terms of odds ratios in Figure 4.

Effect of selected risk factors on the likelihood of having suspected CKD and CKDu.
Hypertension (odds ratio [OR] = 8.47, 95% CI = 3.43-9.87) and diabetes mellitus (OR = 6.09, 95% CI = 2.78-8.95) showed the highest ORs associated with CKD. Considering the prevalence of CKDu, agrochemical exposure (OR = 3.11, 95% CI = 1.36-7.09) and chewing betel (OR = 1.79, 95% CI = 1.29-8.86) were noteworthy risk factors. There was no particularly distinct effect of sex (being male) on the prevalence of CKDu and CKD in the participants. Considering the farming practices, sugarcane farming showed the highest association with CKDu prevalence (OR = 3.40, 95% CI = 1.49-7.78), whereas vegetable farming showed the lowest risk.
Discussion
Chronic kidney disease of uncertain etiology is an emergent health concern among rural farming communities in several tropical regions, including Sri Lanka. The highest burden of CKDu is reported in the North Central Province in Sri Lanka, and this endemic zone has become the main focus of clinical and epidemiological studies. Sri Lanka is a country with diverse farming practices, with many localized farming communities residing on the outskirts of the North Central Province. However, along with findings from a limited number of studies, kidney health risks and vulnerabilities in these communities remain poorly understood.
In this study, we assessed the kidney function of paddy, sugarcane, and vegetable farmers in comparison with nonfarming individuals living in the same areas. Assessment of kidney function was based on eGFR and ACR according to KDIGO clinical practice guidelines. The median eGFR of the nonfarming group was significantly high compared with those of the two farming groups (paddy and sugarcane), whereas urinary ACR showed no substantial differences. In addition, a substantial increase in median SCr in paddy and sugarcane farmers was also observed compared with the nonfarming and vegetable farming groups. As inferred by these biomarkers (eGFR and SCr), there was a significant decline of kidney function in farmers compared with the nonfarmers. Depending on the farming practices, we observed impaired kidney function in individuals within the farming communities at varying degrees. The vegetable farmers living in the wet climatic zone demonstrated better kidney performance compared with the paddy and sugarcane farmers living in the dry zone. Moreover, a relatively high prevalence of suspected CKDu was observed among the farmers compared with the nonfarmers, and considering the 3 farming communities, CKDu was more likely among paddy and sugarcane farmers compared with the vegetable farmers. According to these findings, it is possible to assume a significant risk of CKDu within these farming communities, requiring prompt preventive interventions. Moreover, our findings appear to be consistent with those of a few studies that demonstrated a potential risk of CKDu in some other farming communities in the dry climatic zone in Sri Lanka.13 -15
A similar decline in kidney function has also been observed in sugarcane farmers and sugarcane field workers in Mesoamerica. Several long-term studies have shown a slow progressive decline in kidney function in sugarcane workers during long-term follow-up.16 -18 In addition, a decline in eGFR has been observed in sugarcane workers across the work shifts.19,20 Despite sugarcane farmers being a high-risk category to develop CKDu, 21 in Sri Lanka most of the studies have focused paddy farming communities for clinical and epidemiological investigations. However, none of the studies have performed a comprehensive assessment of the longitudinal variations of kidney function in agricultural workers, and this remains a significant limitation in many studies.
Several risk factors, including environmental toxins heavy metals, agrochemicals, 15 heat stress and dehydration, 22 genetic susceptibility, 23 fluoride in water and toxic effects with aluminum, 24 chewing tobacco, and history of snakebite, 25 have been proposed as potential risk factors of CKDu in Sri Lanka. Even in the present study, we identified significant agrochemical exposure in farming individuals due to improper use of personal protective equipment when handling and applying pesticides. In addition, chewing betel with tobacco was a common lifestyle practice in all farming groups compared with the nonfarmers. Moreover, several other occupational risk factors such as consumption of untreated water from surface wells, springs, and water sources located near agricultural fields were higher among the farming groups compared with the nonfarming group leading to an increased likelihood of toxic exposure via drinking water. 26 Importantly, paddy and sugarcane farmers from the dry climatic zone are more likely to experience heat stress compared with the vegetable farming group that was selected from the upcountry wet zone where mild climate prevails with relatively low temperatures. While precise heat exposure calculations remain to be completed, one or more of these risk factors alone or synergistically could have contributed to the higher prevalence of suspected-CKDu in farming communities. Although the prevalence of suspected CKDu was low, potential exposure to the above occupational risk factors (except high heat exposure) was also observed within the vegetable farming community. Thus, one or more distinct environmental factors in the dry climatic zone are likely to account for the higher prevalence of suspected CKDu in paddy and sugarcane farmers. But this requires in-depth investigations.
Habitual practices of smoking, alcohol consumption, and betel chewing were observed more commonly within the farming groups compared with the nonfarming groups. Particularly, chewing betel is a common practice among both men and women in rural areas, and it becomes a predominant practice during farming activities. Community studies conducted in CKDu endemic regions within the North Central Province (NCP) in Sri Lanka have reported both positive and null associations of betel chewing with the incidence and progression of CKDu. A study with 56 patients with CKDu and 54 controls from Medawachchiya in NCP revealed a significant association (OR = 6.11, 95% CI = 1.93-19.35) of betel chewing with CKDu incidence. However, this study did not identify occupational pesticide exposure and alcohol consumption as risk factors for CKDu. 27 On the contrary, a study with 140 patients with CKDu and 180 controls in Padavi Sripura in NCP showed null association of betel chewing with CKDu. Moreover, this study identified significant associations of drinking well water (OR = 2.52, 95% CI = 1.12-5.70), spraying glyphosate pesticides (OR = 5.12, 95% CI = 2.33-11.26), and being a male farmer (OR = 4.69, 95% CI = 1.06-20.69) with CKDu prevalence. 28 Furthermore, in the present study several risk factors, including, age, diabetes mellitus, hypertension, low BMI, and agrochemical exposure, showed substantial associations with ACR and eGFR, particularly in the paddy and sugarcane farming groups that accounted for the highest prevalence of declined kidney function.
Importantly, the present study explores the likelihood of CKDu among underrepresented farming communities residing on the outskirts of the recognized CKDu hotspots in Sri Lanka. However, the findings of our study should be interpreted within certain limitations. Despite having a high number of participants in each of the study groups, the number of individuals with suspected CKD and CKDu was low. Therefore, the regression model that we adopted here may not have accurately identified the significant risk factors associated with suspected CKD and CKDu. Moreover, in the present study, the interpretations of kidney health are based on a 1-time assessment of eGFR and urinary ACR, with no confirmation of CKD and CKDu through repeated measures. Therefore, it is possible that some of the individuals identified as having CKD/CKDu may simply be having acute kidney injury. Although eGFR and ACR are established markers for defining CKDs, these two conventional markers are known to be less sensitive in the identification of low-grade kidney injury, and nonproteinuric early stages of CKD and CKDu. 3 Hence, the use of more sensitive and specific biomarkers would be a more reliable approach for a comprehensive understanding of kidney health risks and early detection of kidney disease susceptibilities in the farming communities in Sri Lanka.
Conclusions
The present study provides important evidence of a potential risk of CKDu within paddy, sugarcane, and vegetable farming communities residing in highly agricultural areas of Sri Lanka. Particularly, this risk appeared relatively high among the paddy and sugarcane farmers in the dry climatic zone. Agrochemical exposure and consumption of contaminated drinking water appear to be significant risk factors for impaired kidney function in these communities. Beyond these investigations, in-depth studies with increased sample size and longitudinal observations are warranted for understanding potential health risks in farming communities. Moreover, the implementation of effective disease management strategies against CKDu is of utmost importance.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581231199013 – Supplemental material for Prevalence of Chronic Kidney Disease of Uncertain Etiology Within Selected Farming Communities in Rural Sri Lanka
Supplemental material, sj-docx-1-cjk-10.1177_20543581231199013 for Prevalence of Chronic Kidney Disease of Uncertain Etiology Within Selected Farming Communities in Rural Sri Lanka by E. M. D. V. Ekanayake, P. Mangala C. S. De Silva, T. D. K. S. C. Gunasekara, W. A. K. G. Thakshila, S. D. Gunarathna, R. A. I. Pinipa, Sudheera Jayasinghe, E. P. S. Chandana, E. S. Wijewickrama and Nishad Jayasundara in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to thank all the participants, medical staff, technical assistants, and administrative officers for their valuable support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Ruhuna research grants (Grant number: RU/PG-R/16/04) under the funds of the University Grants Commission, Sri Lanka, and Climate and Health Data Expeditions Grants by Duke University.
Ethical Considerations
The study was carried out under the approval of the ethics review committee of the Faculty of Medicine, University of Ruhuna, Matara, Sri Lanka (reference no: 09.03.2016:3.2), in accordance with the declaration of Helsinki. Informed written consent of the participants was obtained before participation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.