
Abstract
Background:
Significant variability in organ acceptance thresholds have been demonstrated across the United States, but data regarding the rate and rationale for kidney donor organ decline in Canada are lacking.
Objective:
To examine decision making regarding deceased kidney donor acceptance and non-acceptance in a population of Canadian transplant professionals.
Design:
A survey study of theoretical deceased donor kidney cases of increasing complexity.
Setting:
Canadian transplant nephrologists, urologists, and surgeons making donor call decisions responding to an electronic survey between July 22 and October 4, 2022.
Participants:
Invitations to participate were distributed to 179 Canadian transplant nephrologists, surgeons, and urologists through e-mail. Participants were identified by contacting each transplant program and requesting a list of physicians who take donor call.
Measurements:
Survey respondents were asked whether they would accept or decline a given donor, assuming there was a suitable recipient. They were also asked to cite reasons for donor non-acceptance.
Methods:
Donor scenario-specific acceptance rates (total acceptance divided by total number of respondents for a given scenario and overall) and reasons for decline were determined and presented as a percentage of the total cases declined.
Results:
In all, 72 respondents from 7 provinces completed at least one question of the survey, with considerable variability between acceptance rates for centers; the most conservative center declined 60.9% of donor cases, whereas the most aggressive center declined only 28.1%, P-value < .001. There was an increased risk of non-acceptance with advancing age, donation after cardiac death, acute kidney injury, chronic kidney disease, and comorbidities.
Limitations:
As with any survey, there is the potential for participation bias. In addition, this study examines donor characteristics in isolation, however, asks respondent to assume there is a suitable candidate available. In reality, whenever donor quality is considered, it should be considered in the context of the intended recipient.
Conclusion:
In a survey of increasingly medically complex deceased kidney donor cases, there was significant variability in donor decline among Canadian transplant specialists. Given relatively high rates of donor decline and apparent heterogeneity in acceptance decisions, Canadian transplant specialists may benefit from additional education regarding the benefits achieved from even medically complex kidney donors for appropriate candidates relative to remaining on dialysis on the transplant waitlist.
Introduction
Kidney transplantation provides a quality of life and survival advantage for patients with end-stage kidney disease (ESKD) relative to remaining on dialysis. However, the number of patients on the transplant waitlist is steadily increasing relative to the number of available kidney donors. In Canada and the United States, the number of available deceased donors appears to have plateaued,1,2 which has exacerbated the disparity between kidney organ supply and demand. Despite this, while Canadian organ discard rates are not available, the proportion of discarded kidneys in the United States has paradoxically increased over time.2,3 From 2000 to 2015, approximately 17.3% of kidneys procured for transplantation were discarded, with significant overlap in donor characteristics between those accepted and not. 2 This suggests that there may be differences in perceived eligibility based on donor (and donor organ) quality. However, there are important negative consequences to organ decline. Over an 8-year period from 2008 to 2015, more patients either died or were withdrawn from the transplant waitlist (30.5%) than received a deceased donor kidney transplant (29.2%). 4 Approximately 10 candidates with at least one previous allograft offer declined by a transplant center on their behalf (that was later accepted by another center) died per day over the study period. 4 In the United States, factors associated with an increased risk of organ discard are a higher kidney donor profile index (KDPI), older donor age, female sex, Black race, obesity, diabetes, hypertension, and hepatitis C virus positivity, 2 with “donor quality concerns” cited as the primary cause of decline in 92.4% of declined offers. This varied little by decile of KDPI; poor organ quality was the cause for decline in 87.1% of kidneys with a KDPI of 0-10. 4 Significant variability in organ acceptance threshold across centers in the United States has been demonstrated in several studies,4,5 leading to a marked difference in access to transplant for patients at the most conservative versus liberal centers.
Importantly, transplantation with a “marginal” deceased donor kidney still appears to result in significant improvements in survival and quality of life over remaining on dialysis.6 -10 Recipients of kidneys from deceased donors where the other kidney was discarded had 1-year death censored graft survival rates >90%. 2 Given the unintended negative consequences of declining an organ offer, the discard of potentially transplantable organs must be avoided. While there is an abundance of literature regarding predictors of organ decline in the United States, to date, there are no data regarding the rate or rationale for deceased donor decline in Canada. Therefore, the purpose of this study was to better understand current clinical decision-making with respect to deceased kidney donor acceptance decisions in Canada.
Methods
Survey Development
A cross-sectional survey of increasingly complex potential deceased kidney donor cases was developed by one of the study investigators with input from the study steering committee. The survey was translated into French by a professional translator with the French version subsequently corrected by a French-speaking transplant nephrologist.
Survey questions are presented in Supplemental Table 1. There were 3 sections examining different kidney donor offer scenarios (Section 1: 8 questions; Section 2: 8 questions; Section 3: 16 questions) and respondents were asked whether they would accept or decline a hypothetical donor presented in the question stem, assuming there was a suitable recipient. Within each Section, donor cases were sequentially adapted to become increasingly complex (eg, in Section 1, a 40-year-old neurological determination of death (NDD) donor with normal renal function (Profile 1a), then a 40-year-old NDD donor with acute kidney injury (AKI) (Profile 2a), then a 40-year-old NDD donor with severe AKI but reassuring biopsy findings (3a), then a 40-year-old NDD donor with severe AKI and no biopsy (4a)). Within Section 1 this was then repeated, except with a donation after cardiac death (DCD) donor (Profiles 1b-4b). Respondents were presented the base cases for each donor scenario in each Section (Profiles 1a, b, c & d, Supplemental Table 1) but using skip logic and conditional branching they were only provided the next level of donor complexity within that Section if they accepted the donor in the prior scenario. Given the graduated increased complexity of each donor case, it was assumed that when a respondent declined a base donor in a particular scenario, they would also decline all downstream adaptations to that base stem. For example, if a respondent declined a 40-year-old NDD donor with normal kidney function (Section 1, Profile 1a), they would automatically be considered as declining the more complex and higher-risk donors from Section 1, Profile 2a (the same donor now with non-oliguric AKI) and 3a (the same donor now with oliguric and dialysis-dependent AKI). When a respondent first declined a potential deceased donor, they were asked to select all reasons for their decision, categorized as Donor age, NDD vs. DCD, kidney function, severity of AKI event, biopsy results, other.
In Sections 1 and 2, base donor cases were primarily stratified by mode of death (NDD or DCD) and donor age (40 or 60 years), with respondents being prompted to indicate if either of these factors influenced their decisions. Conversely, in Section 3, donor cases were stratified by mode of death and donor sex rather than age (fixed at 65 years). It should be noted that the creatinine values varied between profiles on the basis of sex which resulted in a higher estimated glomerular filtration rate (eGFR) for the female recipient (eGFR by CKD-Epi2021 101 mL/min/1.73 m2 for the 65-year-old female with admission creatinine 50 umol/L versus 77 mL/min/1.73 m2 for the 65-year-old male with admission creatinine 95 umol/L).
Survey Distribution
Surveys were distributed between July 22 and October 4, 2021. Invitations to participate were distributed to 179 Canadian transplant nephrologists, general surgeons, and urologists through e-mail (a sample of convenience with single stage sampling technique). Participants were identified by contacting each transplant program and requesting a list of physicians who take donor call and was felt to be representative of the Canadian landscape. During the study period, 2 reminder emails were sent out reminding invited individuals to please complete the survey if they had not yet done so.
Survey Respondent Characteristics
The specialty for each respondent was determined and presented as a count and percentage. Respondents included transplant experts working at adult only, pediatric only, and combination adult/pediatric transplant centers. Given the much more conservative criteria for pediatric versus adult deceased donor acceptance decisions and the very high decline rates among pediatric center only respondents, in our primary analyses we excluded those respondents working only in pediatric centers; however, response rates among pediatric transplant experts were examined in a sensitivity analysis.
Ethics Considerations
Requirement for a full ethics review was waived by the University of British Columbia Research Ethics Board (UBC REB) as respondents were consented to participate at the start of the survey. The survey was anonymous and results kept confidential, although potentially identifying information was collected including respondent transplant center and subspecialty. Respondents were, however, informed their responses would not be tied back to their transplant center.
Analysis
The proportion of respondents completing the survey was determined, as were overall and donor scenario-specific acceptance rates among those providing responses. The reasons for decline in each donor scenario were also determined and presented as a percentage of the total decline for a particular Section and within each Profile. Respondents who declined earlier profiles were assumed to have declined the later profiles as well, and were treated as such when determining acceptance rates for these more challenging cases with “decline” responses carried forward for that particular base donor case. Decline rates overall were established for the most and least conservative transplant centers, and univariable logistic regression was used to examine the odds of donor decline by subspecialty (reference group was Nephrology).
Results
Survey Respondents
Of the 179 individuals sent the survey, 81 (45.3%) respondents accessed the survey from 19 centers and 7 provinces across Canada (all provinces with at least one transplant center). In all, 72 respondents (40.2%) answered at least one question of whom, 65 (90%) made donor decisions for adult transplant centers, and 7 (10%) managed only pediatric recipients. Of the respondents representing adult transplant centers (primary analysis), 14 (21.5%) did not complete the survey. Details of where respondent drop-out occurred are shown in Supplemental Figure 3. Overall, 65 (90%) of respondents were nephrologists, 3 (4.2%) were general surgeons, and 4 (5.6%) were urologists.
Donor Decline Rates
Sections 1 and 2: Age, mode of death, acute kidney injury
Donor acceptance rates for Sections 1 and 2 are demonstrated in Figure 1. Overall acceptance rates were highest for the younger (40 years) donor scenarios and when the donor was NDD vs. DCD. Acceptance rates between a 40-year-old DCD donor and a 60-year-old NDD donor were very similar (7% versus 8% of respondents accepting even the most complex donor for each Section; versus 23% and 0% accepting the most complex scenarios for a 40-year-old NDD donor and a 60-year-old DCD donor, respectively). The most pronounced drop in acceptance rates for all donor scenarios was between Profile 2 (non-dialysis dependent and recovering AKI) and 3 (AKI with dialysis dependency and a biopsy demonstrating ATN but no coagulative necrosis). For example, a 40-year-old DCD kidney donor went from an acceptance rate of 92% in Profile 2 to 20% in Profile 3. Reasons for donor decline for Sections 1 and 2 for each profile and overall are shown in Figure 2. Severity of AKI was most likely to lead to non-acceptance of the 40-year-old donor, and donor age was the main factor for the 60-year-old donor scenarios. In all, 41% of respondents would accept a 40-year-old NDD with dialysis-dependent AKI and the biopsy results listed, whereas only 23% would accept this donor without a biopsy. Similarly, 9% of respondents would accept Profile 3 for a 60-year-old DCD, but no respondents would accept this same donor without a kidney biopsy.
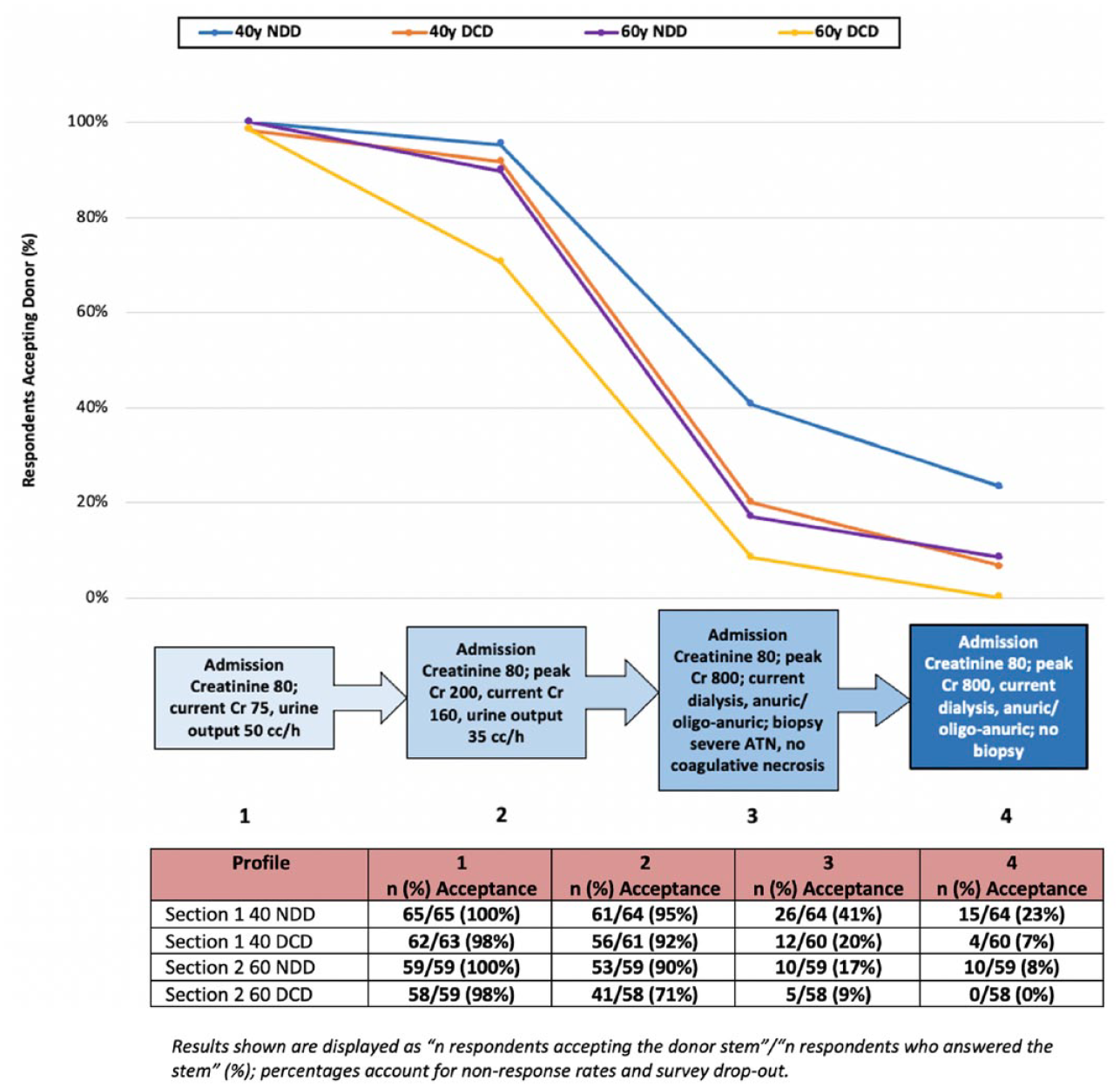
Deceased donor acceptance results for Sections 1 and 2 based on DCD versus NDD status and different profile attributes.

Rejection consideration for Sections 1 and 2.
Section 3: Older age, mode of death, comorbidities, chronic kidney disease
Donor acceptance rates for Section 3 are shown in Figure 3. Overall acceptance rates were highest for NDD versus DCD kidney donors. Acceptance rates were similar albeit slightly higher for female donors for each Profile. Like in Sections 1 and 2, the most pronounced drop in acceptance rates for all donor scenarios was between Profile 2 (comorbidities but no chronic kidney disease [CKD]) and 3 (CKD with a biopsy demonstrating 3 out of 12 glomeruli sclerosed, but no arterial hyalinosis). For example, a 65-year-old female NDD kidney donor went from an acceptance rate of 85% in Profile 2 to 25% in Profile 3. Reasons for donor decline in Section 3 for each profile and overall are shown in Figure 4. “Kidney function” was selected as the reason for decline most often for male NDD donors, whereas “donor age” was selected most commonly for female NDD donors, and DCD donors of both sexes.
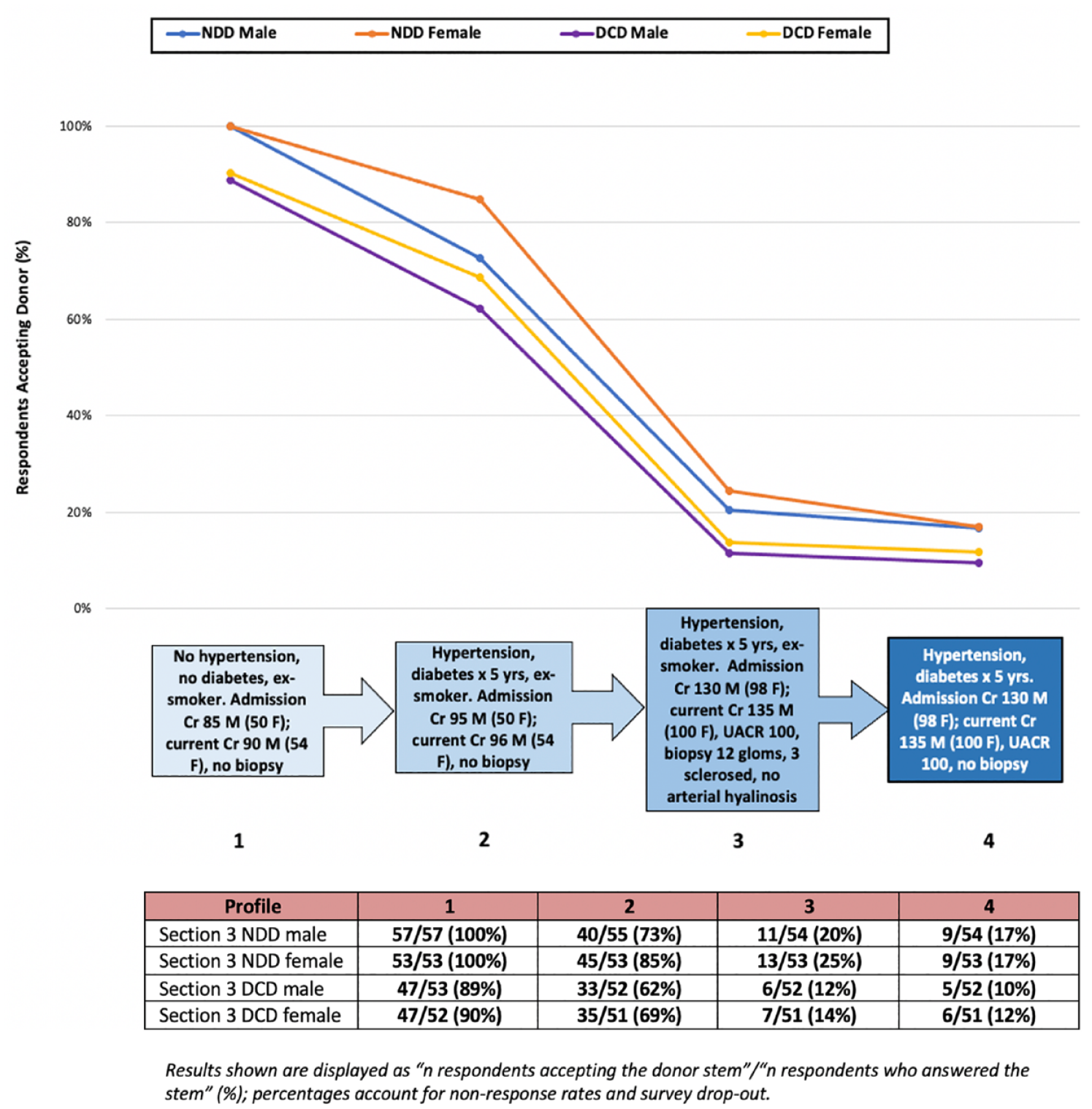
Deceased donor acceptance results for Section 3 based on DCD versus NDD status and different profile attributes.

Rejection consideration for Section 3.
Overall, there was significant variability in acceptance rates by transplant center. The most conservative center declined 60.9% of donor cases whereas the most aggressive center declined only 28.1%, p-value < 0.001, data not shown. In a univariable analysis examining the odds of accepting a particular deceased donor for adult kidney transplant, acknowledging the small number of general surgeon and urology respondents, there were no significant differences between general surgeons and nephrologists (odds ratio [OR] = 0.99, 95% confidence interval [CI] = 0.74-1.33 for surgeons); however, urologists were less likely to decline a particular donor (OR = 0.69, 95% CI = 0.53-0.91 for urologists relative to transplant nephrologists).
Pediatric center only respondents
Results from respondents caring only for pediatric transplant patients are shown in Supplemental Figure 4. While most respondents accepted a 40 year old NDD until Profile 2 (mild AKI) or Profile 3 (severe AKI), most other donor scenarios were declined immediately at the least complex scenario for a particular donor.
Discussion
In this study, we explore for the first time, predictors of deceased donor decline among a population of Canadian kidney transplant specialists. Our data demonstrate variability in donor acceptance thresholds with increased decline rate in potential donor offers with older donors, DCD, AKI, CKD and comorbidities (hypertension and diabetes).
While older donor age is associated with an increased susceptibility to ischemia reperfusion injury and reduced long term allograft survival relative to younger donors, in appropriate recipients, older donor kidneys still confer an improved overall patient survival relative to remaining on the dialysis waitlist.11,12 Acceptance of an older kidney donor may thus be an acceptable trade-off for an older recipient with a shortened anticipated survival, or a younger, sensitized recipient unlikely to find a compatible donor in a reasonable time period. Similarly, large registry studies have demonstrated favorable transplant outcomes with DCD kidney donors, including from expanded criteria donors. 13 While unadjusted transplant outcomes have been shown to be worse with DCD organs, DCD donors are often older and adjusted long-term survival between NDD and DCD donor organs is similar. 13 Despite this, in our study DCD status was cited as an indication for donor decline in >70% of declined cases for a 40-year-old DCD donor. Additionally, the presence of comorbidities (hypertension and diabetes) were also associated with an independent risk of donor decline in our survey. In the United States, diabetes is a common cause for organ discard among deceased kidney donors, with a discard rate of 39% overall, and as high as 57% among expanded criteria donors. 14 Although patient survival is lower after transplant with diabetic versus non-diabetic kidney donors, a kidney transplant from a diabetic donor provides a survival advantage over remaining on the waitlist for many candidates, especially among those with long wait times or high mortality risk on the waitlist. 7
AKI, particularly severe AKI requiring dialysis, was also associated with an increased likelihood of donor decline in our study. This is in keeping with earlier literature in the United States that shows a sevenfold increased likelihood of kidney discard with an elevated (>2 mg/dL) terminal donor creatinine. 15 Another study showed that nearly half of discarded kidneys had AKI; however, noted substantial variation in acceptance by center. 16 Importantly, kidneys with even severe AKI have been associated with a higher risk of delayed graft function, but overall favorable long-term outcomes.16 -19 However, AKI superimposed on an expanded criteria or marginal donor kidney has been associated with reduced long-term allograft survival. 20 Therefore, this may support the noted concerns regarding AKI in the older 60-year-old donor scenario (Section 2) where AKI was the second and third leading cause for decline in NDD and DCD donors, respectively. However, notably, in the 40-year-old donor scenario (Section 1), AKI severity was the leading reason for donor non-acceptance, despite evidence of long-term benefit when kidneys from similar donors are utilized.
Biopsy results were cited as a cause for donor decline in Sections 1-2 (severe AKI) 31% to 41% of the time and 15% to 23% of the time for Section 3 (CKD). Studies out of the United States have demonstrated that biopsy findings are cited as the most common reported reason for organ discard, despite a lack of consensus regarding the association of preimplantation biopsy findings with post-transplant outcomes. 2 In fact, implantation kidney biopsy results have not been shown to improve prediction of 5-year graft outcomes beyond clinical donor parameters alone. 21 Histopathologic and clinico-histopathologic scoring systems exist for decision making around use of deceased donor kidney organs, but without uniform consensus regarding thresholds for acceptance.22 -27 Additionally, there may be significant disagreement between on call and renal pathologists in terms of biopsy reporting, with 1 study demonstrating a kappa of only 0.25 (poor agreement) for arteriolar hyalinosis, 0.31 for interstitial fibrosis, and 0.14 for tubular atrophy. 28
Our biopsy specimen for the CKD case included 3/12 (25%) globally sclerosed glomeruli, but no other abnormalities; specifically, there were no vascular abnormalities. The association of glomerulosclerosis with graft outcomes is controversial. Some studies have suggested reduced allograft survival in donors with >20% glomerulosclerosis, 29 whereas others have demonstrated no reliable association with graft outcomes unless the biopsy specimen includes >25 glomeruli. 30 Other studies still have suggested that vascular change is the only significant histologic predictor of graft outcomes.31,32 The biopsy findings in our CKD cases correspond to a Remuzzi score 33 of 2 (low), which, even in a kidney donor with a KDPI of 98%, still correlates with a 3-year adjusted survival of 85.0%. 34 Additionally, the biopsy cases in our AKI scenario showed only ATN, with no evidence of coagulative necrosis. While there are no established histopathologic scoring systems for AKI in deceased kidney donors, in native kidneys with normal baseline kidney function, the rate of recovery from dialysis-dependent AKI in the recent Acute Renal Failure Trial Network study was 69% among those who didn’t die; however, none of these patients had a kidney biopsy and excluding those with coagulative necrosis or an etiology other than ATN would likely further increase the observed recovery rate. 35
Female donor sex was associated with a lower risk of organ decline (in the United States, female donor sex is a risk for organ decline). 2 Although it is possible that Canadian transplant experts may have an unconscious bias to accept female kidney donors, it is likely that the lower admission creatinine in the stem for the smaller female versus larger male donor cases (50 umol/L in a 50 kg female versus 95 umol/L in a 70 kg male) may have impacted some respondents, as the estimated eGFR for the female cases was higher than that in the male case by both CKD-Epi and MDRD.
To date, there is no robust set of guidelines to define eligibility for acceptance of deceased kidney donors, and most decisions are made based on expert opinion and clinician gestalt, which allows for variability in practice and acceptance thresholds (as shown in our current study). A study using US data from 2007 to 2012 showed that deceased donor kidneys were offered a median of 7 times before ultimately being accepted for transplantation. 5 Interestingly, the number of times a kidney has been declined before subsequent acceptance has not correlated with worse post-transplant survival outcomes. 36
Despite kidney transplant using “marginal” deceased donor kidneys still being associated with significant improvements in survival and quality of life over remaining on dialysis,6 -10 an important and often overlooked consideration is the patient’s perspective regarding willingness to accept a less than optimal donor organ. In the United States, patient willingness to accept a deceased donor kidney with a KDPI >85% decreased slightly from 2014 to 2015, after institution of the revised Kidney Allocation System, but has been relatively stable since. 37 A KDPI >85% deceased donor kidney transplant has been shown to result in better 5-year survival than a conservative approach (remaining on the waitlist for a lower KDPI offer), with even greater relative survival in patients >50 years and at centers with median wait times ≥33 months. 38 Despite this, less than two-thirds of patients ≥65 years of age and less than half of patients 50 to 64 years are willing to accept these higher risk organs. 37 Willingness of Canadian transplant candidates to accept higher risk kidney organs has not been previously examined.
Finally, dual kidney transplantation (DKT) has been shown to be a safe and effective way to increase the use of marginal donor kidneys (for example, >70 years with reduced eGFR <30 mL/min, or terminal creatinine >3.0 mg/dL) in the right recipients, with outcomes similar to single kidney transplantation from standard and expanded criteria donors. 39 Therefore, it is likely that even the most complex deceased donors from our survey may have provided benefit to an appropriate recipient if transplanted as DKT (despite 77%-100% decline rates in Profile 4 for each Section).
This study is the first to examine donor acceptance practices in a Canadian context. However, there are limitations, particularly in relation to the bias which is inherent to survey studies. As with any survey, there is the potential for participation bias (e.g. those respondents more passionate about donor acceptance are more likely to participate), compromising study generalizability. The order in which items are presented has also been shown to influence people’s response rates; an earlier item may change the way participants respond to later items (item-order effect bias) and because the order of questions was not randomized between respondents, it is possible this too may have contributed to bias.40,41 This survey was designed using skip logic and conditional branching whereby respondents were only provided sequentially more complex donor scenarios if they first accepted a straightforward base donor case. Therefore, those respondents who declined the earlier and more straightforward donor cases were assumed to also decline more complex adaptations of the base case. While this is a reasonable assumption, there may be factors that lead respondents to accept a more complex donor scenario (eg, the biopsy results provided may have dissuaded some respondents who would be more likely to accept without a biopsy available). If respondents who declined an earlier donor scenario would accept the same donor if they were more medically complex (an anticipated rare phenomena), this would impart bias on our results and amplify problems due to item nonresponse or response errors. 42 That said, recent microsimulations of survey results built using skip logic have shown that while bias is possible, the effect of this bias is usually inconsequential. 43 Skip logic is a commonly accepted survey practice 42 designed to minimize the risk of respondent burden and survey fatigue, which can also lead to biased results.42,43 Other potential sources of bias for consideration in this study include acquiescence bias (the tendency of respondents to agree rather than disagree with statements; ie, potentially accept donor offers), 44 and social desirability bias (the tendency to overreport desirable attributes; that is, potentially answer in a manner the respondent believes will make their transplant center be viewed in a positive lens) which can be conscious or not. 45 However, the survey was anonymous which minimizes the risk of social desirability bias, 46 and while information regarding transplant center was collected, respondents were informed responses would not be tied back to their center.
Although we attempt to identify predictors of donor non-acceptance, it is likely that donor acceptance decisions relate to the overall donor characteristics in a multiplicative rather than additive manner. Importantly, this study examines donor characteristics in isolation, however, asks respondent to assume there is a suitable candidate available. Whenever donor quality is considered, it should be considered in the context of the intended recipient. While a 65-year-old, diabetic, DCD kidney donor may not be suitable for a 25-year-old candidate, the expected donor organ survival time may well align with that for a 70-year-old diabetic candidate. While we had information on individual decision making, it is possible that decisions about donor eligibility may not be made in isolation. This may be more applicable to donors who are identified during the day, where formal or informal discussions among colleagues may influence decision making around deceased donor eligibility. The fact that refusal rates remained high for some cases despite “a suitable recipient being available” suggests that even more straightforward donors may have been declined in the absence of an appropriate recipient. The survey was not pretested other than within the steering committee who created it, and there were no formal strategies in place to prevent multiple participation, although respondents were all healthcare professionals instructed to complete the survey only once. Finally, there was no option for survey respondents to state whether they would consider a particular deceased donor stem for potential DKT.
Conclusions
In conclusion, we used a survey of increasingly medically complex deceased kidney donor cases to identify rates and reasons for donor decline amongst Canadian transplant specialists. We show that similar to the United States, advanced donor age, DCD donor status, AKI, CKD, and comorbidity burden were all associated with an increased risk of deceased donor non-acceptance. Given relatively high rates of donor decline and apparent heterogeneity in acceptance decisions, Canadian transplant specialists may benefit from additional education regarding the benefits achieved from even medically complex or “marginal” kidney donors for appropriate candidates relative to remaining on dialysis on the transplant waitlist. Additionally, given the variability in acceptance thresholds by center, it is likely that deceased donors declined by the more conservative Canadian centers may have been accepted by the more liberal centers, and bearing in mind the negative implications of prolonged cold ischemic insults, these kidneys may have been accepted for shipping and utilization at another Canadian center. Instead, in the current Canadian transplant environment, declining a potential donor at 1 center results in an unrealized transplant opportunity for 2 appropriate recipients at another center willing to utilize the organs (including patients on the highly sensitized national registry who may be less particular about donor quality). Finally, as illustrated by the variability in acceptance thresholds, national guidelines regarding the suitability of potential deceased kidney donors for acceptance in appropriate candidate populations are urgently needed.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581231156855 – Supplemental material for Disparities in Deceased Donor Kidney Offer Acceptance: A Survey of Canadian Transplant Nephrologists, General Surgeons and Urologists
Supplemental material, sj-docx-1-cjk-10.1177_20543581231156855 for Disparities in Deceased Donor Kidney Offer Acceptance: A Survey of Canadian Transplant Nephrologists, General Surgeons and Urologists by A. J. Vinson, H. Cardinal, C. Parsons, K. K. Tennankore, R. Mainra, K. Maru, D. Treleaven and J. Gill in Canadian Journal of Kidney Health and Disease
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.