
Abstract
Background:
Patients with kidney failure represent a major public health burden, and living donor kidney transplantation (LDKT) is the best treatment option for these patients. Current work to optimize LDKT delivery to patients has focused on microlevel interventions and has not addressed interdependencies with meso and macro levels of practice.
Objective:
We aimed to learn from a health system with historically low LDKT performance to identify facilitators and barriers to LDKT. Our specific aims were to understand how LDKT delivery is organized through interacting macro, meso, and micro levels of practice and identify what attributes and processes of this health system facilitate the delivery of LDKT to patients with kidney failure and what creates barriers.
Design:
We conducted a qualitative case study, applying a complex adaptive systems approach to LDKT delivery, that recognizes health systems as being made up of dynamic, nested, and interconnected levels, with the patient at its core.
Setting:
The setting for this case study was the province of Quebec, Canada.
Participants:
Thirty-two key stakeholders from all levels of the health system. This included health care professionals, leaders in LDKT governance, living kidney donors, and kidney recipients.
Methods:
Semi-structured interviews with 32 key stakeholders and a document review were undertaken between February 2021 and December 2021. Inductive thematic analysis was used to generate themes.
Results:
Overall, we identified strong links between system attributes and processes and LDKT delivery, and more barriers than facilitators were discerned. Barriers that undermined access to LDKT included fragmented LDKT governance and expertise, disconnected care practices, limited resources, and regional inequities. Some were mitigated to an extent by the intervention of a program launched in 2018 to increase LDKT. Facilitators driven by the program included advocacy for LDKT from individual member(s) of the care team, dedicated resources, increased collaboration, and training opportunities that targeted LDKT delivery at multiple levels of practice.
Limitations:
Delineating the borders of a “case” is a challenge in case study research, and it is possible that some perspectives may have been missed. Participants may have produced socially desirable answers.
Conclusions:
Our study systematically investigated real-world practices as they operate throughout a health system. This novel approach has cross-disciplinary methodological relevance, and our findings have policy implications that can help inform multilevel interventions to improve LDKT.
Introduction
Kidney transplantation is the ideal therapeutic option for patients with kidney failure.1 -3 Although patients can get a kidney from a living or a deceased donor, a kidney transplant from a living donor has a longer median survival period than that from a deceased donor.4 -7 Those with living donor kidney transplantation (LDKT) experience lower rates of acute rejection, spend less time on dialysis, and have an improved quality of life.1,6,8 -13 Yet, limited progress has been achieved in increasing LDKT rates over the past decade.
Much of the current work on increasing LDKT rates has been concerned with microlevel interventions to improve LDKT delivery and increase rates, predominantly targeting living donors and patients14 -18 and, more recently, health care professionals (HCPs).19 -21 These interventions have had limited impact and may be contributing to transplant inequity. 18 , 22 , 23 This is because it is unrealistic to place the onus of finding a donor on an already overwhelmed and sick patient who has to deal with complex treatment regimens, an approach which can tend to favor those who have the social and financial means to learn to understand this process and seek donors.23 -25 Also, individual microlevel approaches fail to address the dynamic processes that are involved in delivering health services to patients. 26 Although some recent interventions to increase LDKT numbers have demonstrated interest in a more holistic approach to system functioning, 27 there remains little research to address how macrolevels of practice, such as organizations and the environment, influence the delivery of LDKT as a treatment option to patients. Currently, there is little evidence to guide these efforts.
Given these knowledge gaps, we have proposed a paradigm shift to better understand and address how health systems deliver LDKT. 23 We applied a complex adaptive systems (CAS) approach to LDKT delivery that recognizes health systems as being made up of dynamic, nested, and interconnected levels, with the patient at its core. These levels are environment, organizations, care teams, and patients, which reflect macro, meso, and micro levels of practice (Figure 1). We are implementing this theoretical approach to learn from existing health systems to understand the delivery of LDKT to patients, with the broader goal of improving it.
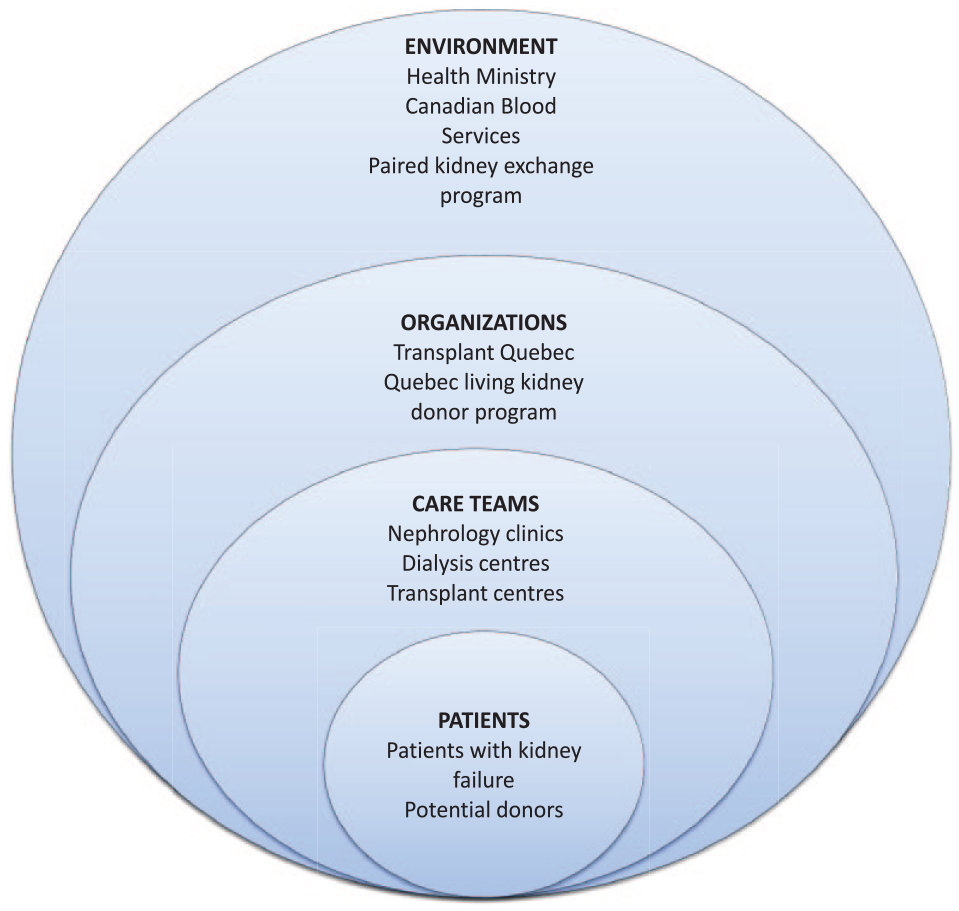
The case: The health system that delivers living donor kidney transplantation to patients in Quebec is envisioned as a complex adaptive system with entities within each level.
We sought to conduct a case study of a jurisdiction with a relatively low LDKT performance using a CAS approach to investigate LDKT delivery. This follows the understanding that studying areas of lower performance is formative and can clarify areas of concern and inform recommendations. 28 Our specific aims were to understand how LDKT delivery is organized through interacting macro, meso, and micro levels of practice; what attributes and processes of this health system facilitate the delivery of LDKT to patients with kidney failure; and what creates barriers.
Methods
Study Design
We adopted a qualitative approach to our case study, which combined interview and document data. Case study research is an in-depth and noninterventional examination of a single case over time to investigate a contemporary phenomenon in its natural context. 29 , 30 Our exploratory approach was designed to produce inductively derived themes and explanations 31 , 32 about how structural arrangements, activities, and patterns of behavior are linked to the provision of LDKT. We chose the health system in Quebec as the setting for this case study, the “case” being comprised of the organizations and people who are involved with facilitating LDKT in Quebec (Figure 1). This is because, while the living donor rates in Canada have averaged around 15 donors/million population annually, the rates in Quebec have been in the range of 5 to 7 living donors/million population, making Quebec the lowest-performing Canadian province for LKDT. 7 , 33 We considered this to be a low-risk study although there was 1 ethical consideration which was the potential for participants to recall negative experiences surrounding LDKT. This was reported in our consent forms, and participants were reminded of their right to pause or stop the interview at any time. Our study was approved by the McGill University Health Centre Research Ethics Committee (approval no. 2021-7126). All participants provided written or recorded informed consent prior to enrollment in the study.
Sample and Recruitment
Purposive sampling and a snowballing technique were used to identify prospective participants. 32 An initial list of eligible interview participants was formed by our research team and a patient partner. This list included representation from all 4 levels of the health system: environment, organizations, care teams, and patients. Purposive criterion sampling was used to ensure the representation of key LDKT leadership at Quebec’s Ministry of Health, Transplant Quebec (organ donation organization [ODO]), and all adult transplant centers. Participants holding leadership roles were included if they held decision-making authority with interorganizational impact. Members of our research team included HCPs who are familiar with the health care system in Quebec and were therefore able to direct us to the people and organizations that participate in facilitating LDKT. Our patient partner was a kidney donor and, therefore, provided valuable direction toward the people and organizations that are influential in a donor’s care pathway. Participants were contacted by email with an invitation to participate in an interview. Thereafter, a snowballing technique sampling was used to recruit providers at other levels of analysis (predialysis and dialysis centers), who were part of the web of professional contacts of the previous participants, as well as donors and patients. Of 48 individuals contacted for an interview, 32 agreed to participate. Interviews lasted between 33 and 74 minutes: The average length was 49 minutes. An equal number of interviews were conducted in French and English.
Data Collection
Data collection was conducted between February 2021 and May 2021. Semi-structured interviews aimed to understand the dynamic organization, governance, and care entailed in LDKT delivery and interdependencies between elements of the system in Quebec. We also sought to understand what aspects of the system variously promoted or hindered patient access to LDKT. Distinct interview guides with open-ended questions were developed for each category of participant: Guides were thematically similar, but questions were adjusted to suit the scope of involvement in LDKT facilitation of participants (see supplementary material for a sample guide). They were drafted based on the knowledge developed from literature reviews and previous research. 18 , 20 , 34 Thus, our interview questions were similar to those used in our study of the province with the highest rates of LDKT to allow for eventual comparison across data sets. Guides were then reviewed by our patient partner and research team and modified accordingly. Interviews were conducted by video call in English or French by a bilingual research associate (RA) (A.H.) who is experienced in qualitative research and semi-structured interviewing. That the RA’s primary background is in the social sciences and she was relatively new to the field of transplant nephrology suited our exploratory approach, as she held few preconceptions about health system processes regarding LDKT and interview participants were not familiar to her. Her academic background was also well matched to understanding health systems. Notes were taken during the interviews to inform an iterative approach to data collection. Document review served as a process for complementary data collection and as means of triangulation with interview data. 35 We used them to inform our understanding of programs, policies, and resources concerning LDKT in Quebec. Documents reviewed are listed in Table 1 and were identified by our research team, with the help of interview participants and using Web searches of governmental, ODO, and hospital platforms. Searches were conducted in both French and English.
Documents Pertaining to LDKT That Were Reviewed and Relevant Themes.
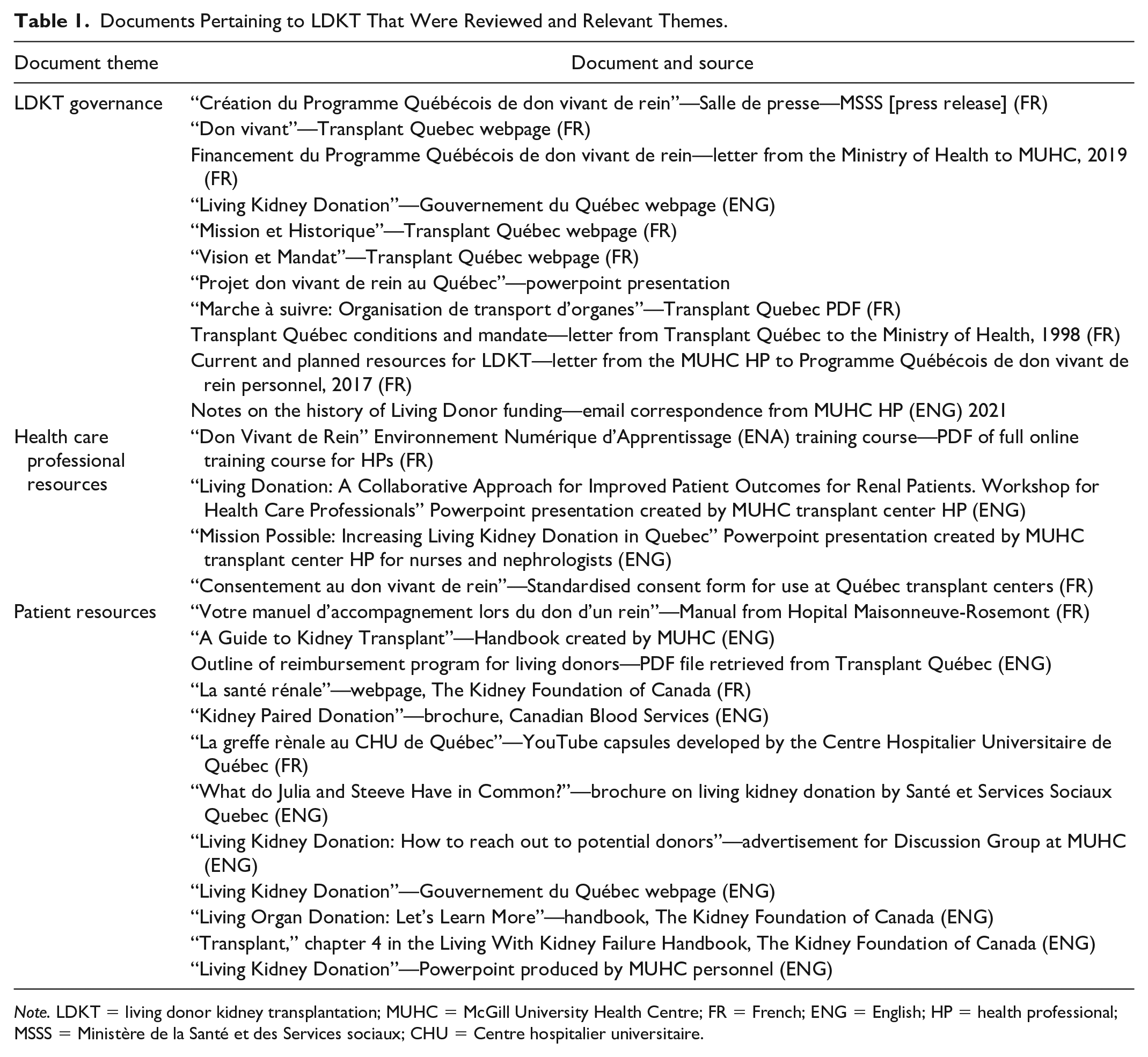
Note. LDKT = living donor kidney transplantation; MUHC = McGill University Health Centre; FR = French; ENG = English; HP = health professional; MSSS = Ministère de la Santé et des Services sociaux; CHU = Centre hospitalier universitaire.
Data Analysis
Interviews were transcribed verbatim directly into French or English. French-language transcripts were translated into English and verified by a certified translator, preceding analysis. Data from transcripts were analyzed using inductive thematic analysis. 32 All transcripts were analyzed independently by 2 RAs experienced in qualitative research (A.H. and K.L.). NVivo (version 12, 2018 QSR International) was used to support data management and analysis. The RAs began with immersing themselves in the data by reading transcripts and highlighting key sentences to openly derive preliminary codes. Qualitative codes were then organized into categories and subcodes to form an initial coding scheme. The coding scheme evolved as data analysis progressed. Coding, emerging themes, links between themes, and any disagreements between the 2 RAs were discussed at regular research team meetings. Themes were subsequently abstracted from categories and grouped into larger “barriers” and “facilitators” clusters. Data analysis occurred concurrently with data collection until saturation was obtained. Saturation was considered to have occurred when there were no new categories or themes emerging from the data: We considered this to be the case after conducting 32 interviews with stakeholders at all levels of the health system. 36 Our document review entailed appraising and synthesizing the data contained in documents, then clustering the documents thematically (Table 1). 35 Interview data were then compared to document data to substantiate our findings and enhance our understanding of the research topic.
Rigor/Trustworthiness
Credibility was optimized through (1) an iterative process of data collection and analysis; (2) maintenance of detailed notes from interviews; (3) team meetings to discuss emerging findings and interpretation; and (4) the consistent application of recognized research methods. 37 , 38 Team meetings involved reflexive discussion of how our roles and perspectives were implicated in the research process. 32 For example, as an interdisciplinary team spanning social science and biomedical expertise, we regularly discussed and compared how our respective professional backgrounds were implicated in interpreting our data and generating our analysis. We found these discussions helpful to consider different perspectives on our research topic and to reach consensus in a way that drew on the strengths of our various backgrounds. In addition, sufficient contextual information was provided in order for readers to determine the extent to which the findings may be transferred to other settings. We followed consolidated criteria for reporting qualitative research guidelines to ensure rigor in our study. 39
Results
Participants and Document Review
Participants included leaders in LDKT governance, HCPs, a recipient, and a donor (Table 2). Some categories have been aggregated to protect the anonymity of our participants; demographic information about our participants has been omitted for the same reason. Leaders in governance denote decision-makers in the Ministry of Health, Transplant Quebec, and the Quebec Living Kidney Donor Program (QLKDP). Transplant center HCPs included physicians, surgeons, nurses, and social workers. Predialysis/dialysis center HCPs included physicians and nurses. Our sample included participants from all adult transplant centers in Quebec. HCPs from predialysis and dialysis centers represented both urban and rural areas.
Participants Who Participated in Semi-structured Interviews.

Note. LDKT = living donor kidney transplantation.
Reviewed documents were clustered into 3 document themes: LDKT governance, HCP resources, and patient resources (Table 1). Categorizing documents into these themes allowed us to contextualize and corroborate interview data from different levels of the health system. This mostly pertained to examining guidelines, educational materials, organizational mandates, and budgets that were discussed by our research participants, which provided deeper understanding and context to their experiences and perspectives.
Organization of LDKT in Quebec
In Quebec, the ODO, Transplant Quebec, is a nonprofit organization that exists outside of the health system. Transplant Quebec has not historically had a mandate to facilitate LDKT but is involved in some aspects such as organ shipment, donor reimbursement, and public promotion. There are 5 adult transplant centers in the province, located in Montreal, Quebec City, and Sherbrooke, Quebec’s most populous urban centers. The transplant centers have historically received funding through the universal budgets of their respective hospitals. In 2018, the QLKDP, a new program, was launched, with the specific mandate to increase rates of LDKT in Quebec. This program is led by a transplant nephrologist at 1 of the transplant centers. It receives an annual budget directly from Quebec’s Ministry of Health, the majority of which is used to fund dedicated personnel in the 5 transplant centers. The 5 transplant centers receive patient referrals from dialysis centers and predialysis centers across the province. In addition to delivering transplants between compatible donor and recipient pairs, patients in Quebec can also participate in the Canadian Kidney Paired Donation program. This interprovincial organ-sharing program is delivered at a national level and matches incompatible donor and recipient pairs (Figure 2).

The typical trajectory of a patient with kidney disease and organization of health service delivery in Quebec.
Case Synthesis
Our key findings are summarized in Figure 3. The themes below are organized separately for coherence but were largely interdependent. Participants described more barriers to LDKT than facilitators. Therefore, while we have delineated 5 facilitators and 5 barriers, it must be noted that there was a lack of balance between positively and negatively described aspects and processes of Quebec’s system, with barriers strongly outweighing facilitators. Full tables of quotes illustrating these themes can be seen in Supplementary Tables 1 and 2.
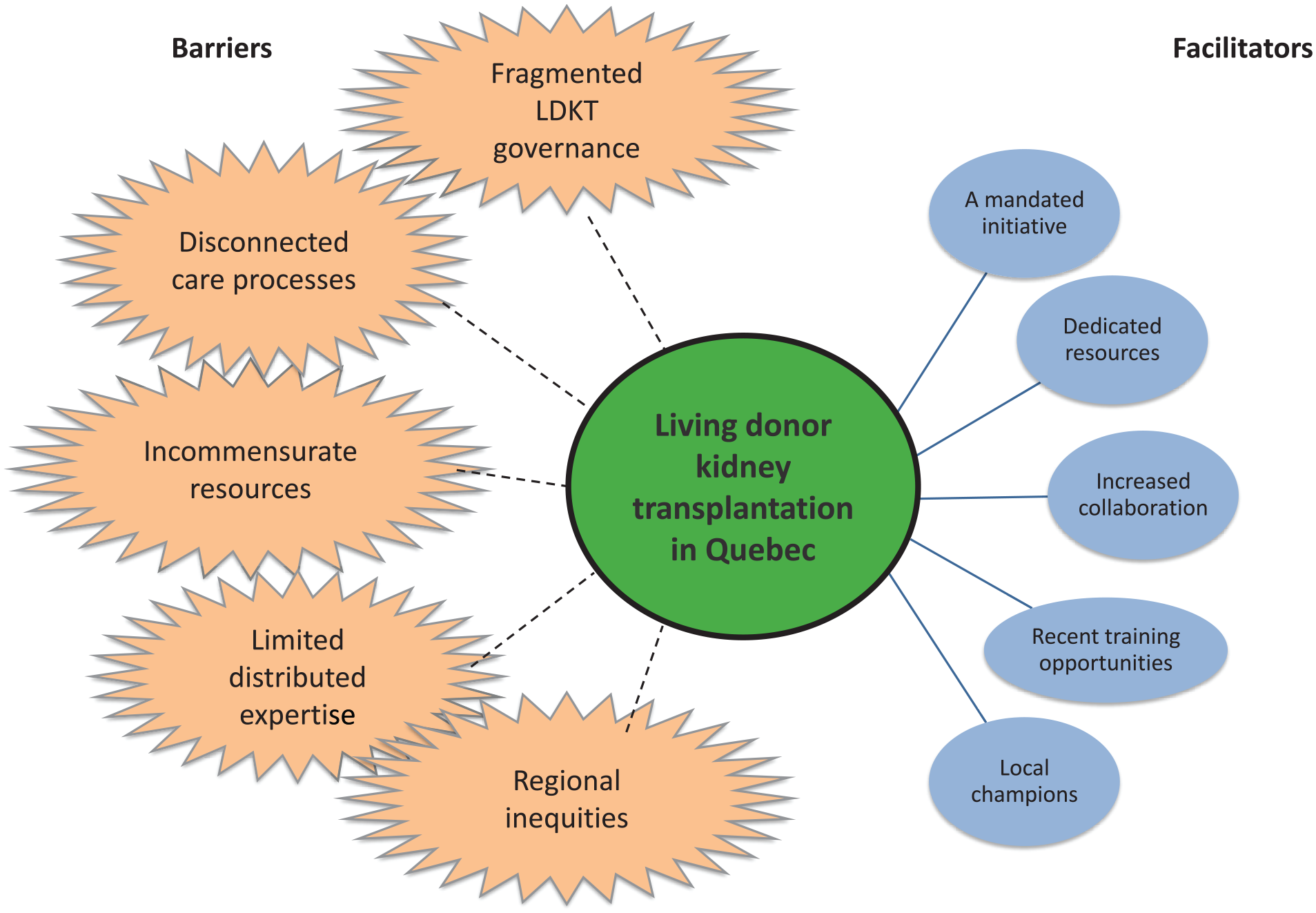
Barriers and facilitators: health system barriers (spiked circles) and facilitators (smooth circles) to living donor kidney transplantation in a low-performing health system in Canada.
Barriers to LDKT
Fragmented LDKT governance
From a CAS perspective, Quebec was reported as lacking a strong central agent to exert intentional influence across the system of LDKT. Participants conveyed that a lack of unified governance has made it harder to establish strong provincial advocacy for LDKT. Historically, there has been no single provincial organization whose job it is to promote LDKT: There are multiple organizations involved with varying levels of influence (Figure 2). Challenges in promoting, delivering, and monitoring LDKT were seen to arise from silos between these organizations, in terms of who is responsible for what, the relative resources of each organization, and a lack of communication between them. The ODO has no official mandate for LDKT, which was cited as limiting its ability to effectively promote LDKT delivery:
[Transplant Quebec is] not mandated to do that . . . So there has to be a change in [Transplant Quebec’s] mandate even to do these small things. And those requests have been made formally. But because the Live Donor Program is not part of [Transplant Quebec], the Live Donor Program [makes requests to] the ministry, so the ministry can tell their subsidiaries that they can give [Transplant Quebec] the money to pay for that, if the circumstance should rise. So the siloing of live donor in this way, creates all sorts of hassles that are not immediately apparent. (Leader in LDKT governance 3)
Participants also stated that there has historically been little communication between the 5 transplant centers, resulting in a lack of leadership, consistency, and standardization of care practices:
So, I think the challenge is I’m not sure there is the leadership. You know, it’s not clear to me that—I think all the centres traditionally would work independently. (Transplant Center HCP 7)
Although the recent work of QLKDP was positively described, some participants expressed concern that a hospital-run program may lack the impact of a national program:
That leadership should be macro, not just us at the transplant centres. There should be a real communication strategy, integrated with the Ministry of Health so that it gets to other dialysis or predialysis centres. (Transplant Center HCP 13)
Furthermore, many HCPs, mostly (but not exclusively) from outside the transplant centers, were unaware of this program. Many participants also considered that there has been stronger provincial investment in dialysis and deceased donation, which may have served to undermine LDKT as a treatment option. Evidently, the boundaries of the sub-systems in kidney transplantation were firmer than what optimal interaction, influence, and communication would require.
Disconnected care processes
Participants described a lack of continuity and poor coordination between regional clinics and transplant centers. Generally, communication was ad hoc, and there was limited support, guidance, and follow-up from the transplant centers regarding LDKT-related processes. Regional personnel were often not appraised of a patient’s progress in the transplant trajectory and hence could not respond to patient questions regarding delays. Transplant personnel did not know when the regional clinics had new patients to assess their transplant candidacy. Some participants also described poor role definition—a lack of clarity about procedures and who was responsible for what between transplant and regional centers:
My biggest frustration is that the patient is supposed to be taken care of by the pretransplant evaluation team, but in fact, everything rests on our shoulders. (Predialysis/dialysis HCP 10)
The confusion over responsibility for particular parts of the system suggested a lack of balance between the porous boundaries needed for optimal coordination and subsystem boundary strength for specialized roles that enable a complex system to function.
Archaic and inconsistent methods of sharing information also resulted in delays and loss of information. Disconnected care processes were exacerbated by internal organizational issues at both regional clinics and transplant centers, such as high staff turnover, workload, inadequate resources, and competing institutional priorities. Failures to pass on information about the status of patient evaluations, lack of clarity about procedures, and limited organizational capacity strongly contributed to inefficiencies and delays. These factors also contributed to problems with effectively synchronizing recipient and donor workups, with the effect that donors were processed much sooner than recipients. These challenges can result in the onus being put on patients to move the process forward and, ultimately, in low LDKT rates:
Poor referral and long workups of patients for listing for transplantation—all of that combined gives us a very low living donor rates in this province. (Transplant Center HCP 1).
Thus, while patterns of interdependent and dynamic relationships characterize LDKT delivery, disconnect between individual elements and agents produces systemic problems. The influence of an assertive common agency with a common vision and message was evidently lacking.
Incommensurate resources
A lack of directed resources for LDKT activity at both transplant and referring centers was cited as a barrier by stakeholders at all levels of the health system. Historically, funding for LDKT activity has come from the universal budget of the respective individual hospitals, with some external support. As such, there has been direct competition with other services for resources. Many HCPs from the transplant centers considered resources to be too limited:
The whole budget on transplantation for the various hospitals in terms of coordinators and the actual dedication by the hospital centres towards transplant is extremely low. And if I have to say one thing, my own university, they can say what they want, but they’re not supportive of us. (Transplant Center HCP 1)
Participants from transplant centers also highlighted competition for operating room time as causing significant delays to surgery. While recent resources from the QLKDP were positively described, some participants expressed concern that “the money is drowned in the multiple functions of the CIUSSS (integrated health and social services centers)” (Transplant Center HCP 13). These resources were seen as incommensurate with the organizational realities of the hospitals and were compromised by bottlenecks in other aspects of organizational operation:
So right now, one of the challenges is . . . the recipient side has a way bigger volume of patients, and they’re not getting that support financially. And you definitely need a lot of manpower there. So now you’re fully stocked with a living donor team, but your recipient team is struggling. (Transplant Center HCP 3)
Participants from regional clinics consistently described lacking targeted resources to effectively promote and facilitate LDKT. In particular, a lack of social work support for patients was described as a barrier and characterized by many as a “big opportunity [. . .] that we missed” (Predialysis/dialysis HCP 4). Additionally, many participants also considered financial support schemes for both donors and recipients to be inadequate and considered this to hinder access to LDKT. It seemed that the LDKT system suffered from a lack of strong agency from a central mechanism that could guide optimal interventions in the interests of the whole system and, thus, ultimately, for people who need transplantation.
Limited distributed expertise
The lack of a strong centralized agent in the system manifested in accidental rather than a guided distribution of priorities, which undermined the very coherence of the whole LDKT system. Limited professional expertise about LDKT outside of transplant centers, at referring clinics, was described as a strong barrier to LDKT:
it’s almost left to the transplant centre and the transplant nephrologist to introduce the concept [of living donation]. And it’s almost—the workups need to be done, and the discussion needs to start way before that. But I get the feeling that people are not easy about it and still defer that discussion to us. (Transplant Center HCP 1)
Expertise in LDKT was concentrated in the transplant centers, and there was great variation in the expertise and confidence of HCPs in predialysis and dialysis clinics. Many predialysis and dialysis nurses felt that they lacked the training needed to support LDKT and felt particularly ill-equipped to support patients in donor outreach. Crucially, a lack of professional expertise outside of transplant centers meant interventions to facilitate LDKT, such as patient education, support, and referrals for transplant, do not reach patients in a timely manner:
The care pathway is not well established and we don’t even know—and the patients are lost and they’re not even given the proper pathway or the option, even, of transplantation, sometimes. (Transplant Center HCP 1)
It was also considered that a lack of confidence to discuss LDKT meant that HCPs in regional clinics would favor other treatment options. Furthermore, some HCPs also expressed concern that outside of nephrology, family physicians may have evidence-uninformed assumptions about LDKT and may discourage their patients from pursuing it.
Regional inequities
Regional inequities were primarily discussed in relation to accessibility to care and testing and health care coordination. Patients and recipients who reside further from transplant centers experience an added logistical and financial burden of accessing transplant facilities for pretransplant testing. In addition to requiring more coordination and time off work, distance implies significantly higher out-of-pocket expenses for transportation and lodging:
But clients are often located in remote regions, are often not able to come to the [metropolitan hospital]—they will miss appointments, which will have a direct impact on their health. Those are big challenges: not being able to have access to care more easily, not have the necessary financial assistance. (Transplant Center HCP 8).
Following transplantation, donors require frequent follow-up and can experience obstacles in finding accommodation because not all cities with transplant centers provide accommodation to convalesce. Challenges in timeliness, coordination, and financial resources for donors are exacerbated when the donor is from another country. Participation in the paired exchange program can also come with added challenges associated with travel, financial resources, companion support, and linguistic barriers:
At the economic level, there is still some way to go, if I think of the exchange program, in particular, for living donation. Or even that currently expenses will be reimbursed, but not all donors necessarily have the means [to pay upfront costs]. (Transplant Center HCP 5)
In terms of organization-level service provision, interview participants highlighted differences in coordination between predialysis and dialysis units that are linked to transplant centers (eg, housed in the same hospital) and those that are not. Co-location (under 1 hospital roof) facilitates access to and coordinated exchange of information between the constituent parts of the system, contributing to shorter wait times and better continuity of care for patients and donors. Interview participants also argued that training and support for predialysis and dialysis centers in rural areas require more diffusion energy.
Facilitators to LDKT
A mandated initiative
Despite its relatively tenuous positioning in the provincial system, the QLKDP is the first initiative with the dedicated mandate to increase rates of LDKT in Quebec. It was strongly described as supporting LDKT delivery and has introduced measures that have helped to mitigate some of the barriers described above (and described as other facilitators below). Many participants noted positive changes that have been generated by the program:
I think that with the Quebec program, people are starting to be more and more aware and I have the impression that I see an increase in calls from potential donors. It’s positive. (Transplant Center HCP 12)
The program was seen to have instigated change in professional attitudes toward LDKT, with HCPs being more aware of and receptive to LDKT, and in it becoming increasingly “part of the regular discourse” (Predialysis/dialysis HCP 9). It was credited with having facilitated stronger communication between the 5 transplant centers, which has enabled cross-provincial learning, support, and standardization of care practices. The program was also commended by some participants for having introduced stronger performance monitoring for LDKT activity, which had been historically lacking:
The other thing that’s been good is that there’s been a push towards tracking the data. So entering, let’s say, times that it takes to work up a donor, how many donors, how to include it all in a spreadsheet . . . So I think that’s going to be helpful because by tracking the data, we know where we need to increase the efficiencies, or maybe we accept those are problems and we look for strategies to address it in other ways. (Transplant Center HCP 7)
Thus, a strong intentional agency has had an influence across the system. It should be noted that the program is a recent initiative, and at the time of data collection, it had suffered delays and setbacks due to the COVID-19 pandemic (eg, redeployment of dedicated HCPs). Participants believed that ongoing initiatives of the program, such as resources and educational material, would bear fruit in the future to improve LDKT rates and delivery.
Dedicated resources
Having dedicated roles for HCPs to facilitate LDKT was a well-described facilitator, both within and outside transplant centers. The QLKDP funds 3 full-time personnel at each of the 5 transplant centers: a living donor coordinator, a social worker, and an administrative assistant. Having these resources in place was broadly perceived to help improve care processes for donors:
We are fortunate to have had a budget from the Living Kidney Donation program to have a dedicated living donation nurse . . . Having a dedicated budget for dedicated staff is certainly helpful. As such, these are the organizational advantages of the program. (Transplant Center HCP 13)
Some participants also considered that these dedicated roles helped transplant centers to better support their referring clinics, in terms of providing guidance about LDKT for HCPs and facilitating the pretransplant workup for recipients. In regional centers, having dedicated professionals with a mandate for transplant—for example, a pretransplant nurse—was also described as a facilitator to LDKT, and to transplantation more generally. Professionals occupying such roles were seen to both expedite the pretransplant workup for recipients and provide more thorough education about LDKT than other HCPs felt capable to do, either because of lack of expertise or time limitations:
They created a position in xxx [clinic] for a proper kidney transplant nurse, so that has already improved things a lot. There’s someone dedicated to this that they didn’t have before. That has improved a lot. (Predialysis/dialysis HCP 12)
The creation of specialized and targeted positions represented an influential intervention in the system which was seen to deliver observable benefits. Tangible resources, such as accommodation for donors and recipients close to transplant centers and reimbursement schemes for donors, were also cited as facilitators, although many felt that these resources should be strengthened.
Increased collaboration
The QLKDP has fostered increased collaboration between transplant centers, through cross-organizational and interdisciplinary committee work. One of the initiatives was the establishment of a social work network focused on living donation, involving 5 social workers in transplant centers funded by the program:
“I had never had contact with other transplant centres or other social workers in transplant centres [before the QLKPD] . . . with regards to social services, [it has] made all the difference since we have had the living donation program, since 2018. Because now we talk to each other regularly, we have really put in place working committees to develop practice, to improve interventions to be made, precisely to promote living donation. This program has been really favorable for communication between the different centres. (Transplant Center HCP 8).
In addition, social workers have established peer support groups involving patient partners and prospective patients, to discuss LDKT. Personnel funded by the program also participate in regular meetings. These collaborative efforts are aimed toward streamlining the medical trajectories of donors and recipients, standardizing procedures across the 5 transplant centers, and lobbying the government for additional resources:
[. . .] the fact remains that we should have a little more of a facilitating trajectory at the level of the medical evaluation. We should also have a facilitating trajectory at the psychosocial level. But that is really the mandate of the provincial committee that was formed a few years ago. What I’m talking about right now is already in the works now. We are working to improve these things and to standardize as a province—so the five transplant centres. (Transplant Center HCP 12).
While connectivity and cross-provincial coordination between transplant centers and predialysis/dialysis centers were described by many HCPs as poor, some participants described recent improvements to system-wide professional connectivity that had occurred through the QLKDP.
Recent learning opportunities
To foster the self-organizing capacity of the system, the QLKDP was mandated to raise awareness of LDKT and to develop educational material on LDKT to align goals and priorities across the system:
The most important area of the project is promotion and awareness—activities promoting and creating awareness about live kidney donation. Because we realized that the issue essentially revolved around that, namely the lack of information and lack of awareness of health care professionals in dialysis and predialysis centres [. . .]. (Leader in LDKT Governance 1)
Part of the systemic influence of this initiative was to introduce online training regarding LDKT for HCPs. While the uptake of training at the time of data collection was still limited, interviewees reported that it represented a positive opportunity to enhance professional expertise on LDKT which would, in turn, increase their comfort discussing LDKT with patients. Social workers and living donor coordinators appointed as part of the program were also mandated to help educate and support HCPs in referring centers to better facilitate LDKT. Nephrologists at transplant centers had conducted some educational presentations on LDKT to their counterparts at referring centers. Training and support from transplant center staff were described by interviewees as beneficial: “It’s really recently when I attended training on living donors that I saw that we could refer people to a social worker” (Predialysis/dialysis HCP 13). Some educational interventions, for example, peer discussion groups facilitated by social workers, were designed specifically for donors and recipients. Such educational initiatives were seen to equip patients with the necessary information, making them more comfortable for approaching the topic with others.
Local champions
While fragmented governance was identified as a barrier to LDKT, some participants highlighted the benefits of having HCPs at their organization who championed LDKT. This was particularly the case in referring centers, where professional knowledge about LDKT was less concentrated. Advocacy for LDKT from an individual member of the team was cited as having a positive impact on the capacity of the team to facilitate LDKT, in terms of providing expertise and organization and advocating for resources from the hospital:
Dr. xxx has been extremely proactive since taking office. He had already worked for a year at xxx [transplant centre]. So, when he arrived in xxx [hospital], he quietly began to set up his program, and he succeeded in having transplants done much faster than what was done before. (Predialysis/dialysis HCP 12)
Encouragement of local champions thus optimized the agential power an individual can have in the LDKT system, even if the exact nature and extent of the influence were unknown. Additionally, having members of the transplant team who were approachable and receptive to questions made a strong difference to the expertise and comfort of HCPs at referring centers. The consistent support of a “pivotal” member of staff, particularly nursing staff, was also highlighted as a significant factor in the care and comfort of patients and donors during the process of LDKT:
Xxx [husband—LDKT recipient] used to love xxx [name of HCP]. Before the operation and after the operation, xxx was very important—the nurse. He would see her on a regular basis because his kidneys were failing. (LDKT donor)
It should be noted that cultivating HCP champions in referring centers is a stated goal of the QLKDP, but at the time of data collection, this was yet to be established.
Discussion
This qualitative case study aimed at understanding health system barriers and facilitators to LDKT delivery in the second-most populous province in Canada with the lowest LDKT performance. In alignment with a CAS approach, we discerned barriers and facilitators at macro, meso, and micro levels of the health system and analyzed the interdependencies and interactions among the various elements. 40 , 41 Overall, we identified strong links between system attributes and processes and LDKT delivery that can help guide comprehensive health system interventions to improve LDKT delivery and rates.
Although case study methods have been used to guide improvements in the delivery of specific health services to patients, 42 , 43 the contribution of this article has been to articulate organizational and environmental barriers to LDKT, on which there had been limited previous research. While there is some recognition of the influence of structural and systemic factors that may influence access to LDKT, 44 evidence about the role of macrolevel conditions in LDKT delivery has remained largely anecdotal. By linking higher levels of governance to LDKT delivery, our analysis suggests that strong advocacy at the macrolevels is required to successfully support current microlevel interventions. This is supported by our previous case study of the best-performing province in Canada, where macrolevel interventions were described as key to enabling LDKT delivery. 34
Our case study also highlights areas for intervention that recognize the interdependencies of individual levels of a health system. 23 , 26 , 45 , 46 Microlevel interventions, such as providing patient education and support on finding living donors, are important; however, to effectively implement them, greater investment is needed to address barriers at other levels of the health system as well. This includes the professional education of HCPs in predialysis and dialysis centers, stronger connections between referring clinics and transplant centers, investment in directed resources for LDKT delivery at transplant centers, and fostering local champions for LDKT. Thus, our findings complement existing work but provides a more integrated perspective.
Methodologically, our study advances the use of qualitative methods to health system learning. Our approach, rooted in the CAS theory, demonstrates that studying the interdependencies and interactions among various elements of a system can provide critical insights for understanding the organization and properties of a system. 46 , 47 This approach is novel in the fields of nephrology and transplantation and may also serve as a template for other disciplines to comprehensively investigate “real-world” practices as they operate throughout a health system. Recognizing the dynamic properties of a system and targeting relationship patterns and flows of behavior can provide opportunities to understand how a system can improve. 45 , 46 For example, targeted interventions by the QKLDP demonstrate possibilities for adaptability, improvement, and application, captured through delivery and embedded across health systems. 48 , 49
We acknowledge the following limitations. Interview participants may have provided socially desirable answers, 50 which is a common challenge in research involving self-reports. Although the semi-structured interview format permitted exploration of questions emerging during the interview, some aspects of participants’ roles and responsibilities may have remained unexplored. Also, while we consider that our document review served as an effective means of triangulation with interview data, we acknowledge that by not using Web search criteria, it cannot be considered exhaustive. Conducting this research in both English and French may have resulted in a certain lack of equivalence in translating specific terms, although we used a certified French translator. Finally, identifying the unit of analysis for case study research has long been identified as a challenge. 51 Although we made considerable efforts to include views from all levels of the health system, we acknowledge that some perspectives may have been missed. Our more recent work aims to expand this scope: For example, our research team is currently exploring the role of family physicians in LDKT.
In conclusion, informed by a CAS framework, we conducted a case study of a health system with historically poor LDKT delivery and identified strong links between system attributes and processes and LDKT delivery. We delineated 5 facilitators and 5 barriers and demonstrated the interdependencies and interactions among the various levels of a health system. Optimizing health services delivery requires a clear understanding of the overall system, as well as interactions among individual levels. Our work supports the need for a comprehensive system-level approach, and multilevel interventions are needed to optimize LDKT delivery to patients.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581221150675 – Supplemental material for Living Donor Kidney Transplantation in Quebec: A Qualitative Case Study of Health System Barriers and Facilitators
Supplemental material, sj-docx-1-cjk-10.1177_20543581221150675 for Living Donor Kidney Transplantation in Quebec: A Qualitative Case Study of Health System Barriers and Facilitators by Anna Horton, Katya Loban, Marie-Chantal Fortin, Sylvie Charbonneau, Peter Nugus, Michel R. Pâquet, Prosanto Chaudhury, Marcelo Cantarovich and Shaifali Sandal in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-2-cjk-10.1177_20543581221150675 – Supplemental material for Living Donor Kidney Transplantation in Quebec: A Qualitative Case Study of Health System Barriers and Facilitators
Supplemental material, sj-docx-2-cjk-10.1177_20543581221150675 for Living Donor Kidney Transplantation in Quebec: A Qualitative Case Study of Health System Barriers and Facilitators by Anna Horton, Katya Loban, Marie-Chantal Fortin, Sylvie Charbonneau, Peter Nugus, Michel R. Pâquet, Prosanto Chaudhury, Marcelo Cantarovich and Shaifali Sandal in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to sincerely thank the 32 individuals who participated in this study.
Ethics Approval and Consent to Participate
Ethics approval for this study was obtained from the McGill University Health Centre Research Ethics Board.
Consent for Publication
All authors provided their consent for publication.
Availability of Data and Materials
Not applicable.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.S. has received an education grant from Amgen Canada. M.R.P. is the director of the Quebec Living Kidney Donor Program and medical advisor for the Canadian Blood Services. P.C. is the medical director of Transplant Quebec. The rest of the authors have no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by a Gift of Life Institute Clinical Faculty Development Research Grant from the American Society of Transplantation and a Health Research Grant from the Kidney Foundation of Canada. The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, writing, review, or approval of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.