
Abstract
Background:
Self-management has shown to improve the quality of life in patients with chronic kidney disease (CKD). Readily accessible self-management tools are essential in promoting adherence to self-care behaviors. In recognizing that digital health facilitates efficient access to self-management programs, we developed a digital counseling program, ODYSSEE Kidney Health, to promote self-care behaviors while supporting health-related quality of life.
Objective:
To present the design and development of ODYSSEE Kidney Health for digital counseling for patients with CKD.
Design:
The study involved an iterative design process based on user-centered design principles to develop the digital counseling program, ODYSSEE Kidney Health.
Setting:
A sample of 10 to 15 participants were purposively sampled from nephrology clinics at the University Health Network, Toronto, Canada.
Methods:
Participants underwent 2 phases in the development process. In each phase, participants were presented with a component of the program, asked to perform goal-oriented tasks, and participate in the “think-aloud” process. Semi-structured interviews followed the first phase to identify feedback about the overall program. Thematic analysis of the interviews identified themes from the usability testing. Descriptive statistics were used to summarize patient demographic data.
Results:
We enrolled 11 participants (n = 7 males, n = 4 females, ages 30-82). The main themes generated anchored on (1) impact on nephrology care, (2) technical features, and (3) CKD content. Overall, participants reported positive satisfaction toward the navigation, layout, and content of the program. They cited the value of the program in their daily CKD care.
Limitations:
Study limitations included using a single center to recruit participants, most of the participants having prior technology use, and using one module as a representative of the entire digital platform.
Conclusion:
The acceptability of a digital counseling program for patients with CKD relies on taking the patients’ perspective using a user-centered design process. It is vital in ensuring adoption and adherence to self-management interventions aimed at sustaining behavioral change.
Background
Chronic kidney disease (CKD) is a significant health issue that impacts many patients with the global prevalence expected to rise further in the coming years. 1 Emerging data have shown that there is substantial heterogeneity in CKD progression which leads to increased morbidity and mortality. 2 Furthermore, kidney replacement therapy (KRT), particularly within the first 90 days, is associated with increased mortality. 3 Patients with CKD are best described as having a complex chronic disease, with multiple comorbidities needing the attention of multiple health care providers.4,5 Despite advances in medical therapy, patients with kidney disease continue to experience low adherence and decision-making capacity, leading to poor clinical outcomes.6,7 Studies have shown consistent CKD knowledge gaps in these patient populations. 8 Care delivery models that encourage patient participation and promote self-management are needed to fill this gap. Evidence and international guidelines have shown that patient education plays a major component in effective self-management to improve patient outcomes in kidney disease. 9 In addition, comprehensive predialysis education has been shown to improve the selection of home dialysis as the chosen KRT in patients with CKD. 10 Furthermore, studies using guidelines from cognitive behavioral therapy (CBT) have shown improvements in self-care behavior change and the quality of life in CKD. 11 Unfortunately, CBT and self-management programs have relied on face-to-face encounters, and current programs can be resource-intensive and taxing on an already-strained health care system. 12 Novel delivery methods to support psychosocial interventions to promote behavior change and self-care are needed.
Digital media has the potential to address gaps in promoting self-management programs without imposing additional burdens on the health care system. Effective digital health tools often benefit from tailored patient-directed information, a user-centered design process, and an inter-disciplinary approach. The present digital counseling program aims to facilitate long-term adherence to self-care behaviors and improve the quality of life of patients with CKD. It is an automated digital counseling program that uses key components of motivational interviewing (MI) and CBT. This study presents the design and development of the patient-centered digital counseling program using an iterative process in patients with advanced kidney disease.
Overview of the ODYSSEE Kidney Health Digital Counseling Program for CKD
ODYSSEE Kidney Health is an automated digital counseling program for patients with CKD that is accessed via the internet. In keeping with the principles of MI13,14 and CBT,15-17 our digital counseling protocol uses evidence-based guidelines to facilitate the following: (1) personal goal setting that guides the participant in identifying their priority for “living well,” and that connects this priority with therapeutic change in CKD self-care behavior; (2) tailoring of planned change in the participant’s selected CKD self-care behavior according to their stage of readiness for change; (3) interactive self-assessment tools to resolve ambivalence about behavior change; (4) self-monitoring of behaviors with digital tools to build efficacy with performance-based feedback; (5) self-guided training in cognitive behavioral skills to initiate and maintain changes in CKD self-care behavior and to promote positive mental health.15-17
Participants in ODYSSEE-Kidney Health initially select their priority for self-care behavior change, adherence to either medications or dialysis, or to dietary self-care behavior or active living. In keeping with MI, digital sessions in the early phase of the intervention are designed to resolve ambivalence about behavior change. Motivational components help to promote change by (1) validating each subject’s initial stage of readiness, (2) guiding them to select a change goal that is matched to their current level of readiness, (3) reinforcing their active and collaborative role in the intervention, and (4) helping them to resolve ambivalence about change by linking their behavior change goal to a salient personal priority, and by self-assessment tools that evoke adaptive “change talk.”13,14 Subsequent digital sessions follow a cognitive behavioral guideline that helps patients to (1) initiate or sustain behavior change with digital self-monitoring tools and educational feedback, (2) develop a flexible repertoire of skills to maintain behavior change with video-based educational segments, and (3) reinforce self-efficacy as feedback about behavior change is provided with e-based trackers and assessment tools. In addition, the program facilitates user engagement with CKD self-care resources by proactively sending weekly emails with an URL link over the 16-week interval of this intervention. Each email links the program user with a novel topic in an online counseling session.
The content of ODYSSEE Kidney Health is organized into 16 e-sessions, delivered over a 4-month period. The program sends an email reminder once every week to inform users of available new content. Each session consists of 4 core features: (1) self-help video which connects users with CKD medical experts or other CKD patients who reflect and validate the experiences of living with CKD, (2) educational content that provides self-help information in CKD knowledge and self-care and in cognitive behavioral guidelines for psychological distress, (3) interactive e-tools to develop and strengthen self-care behaviors, and (4) e-trackers to enable self-monitoring of behavior change. Users are guided to complete each e-session as they are presented with graphs that indicate which session tasks are completed. They are free to revisit any sessions accessed previously. The collaborative tone of the e-messages is designed to promote active participation as subjects develop and self-direct their change plan. Finally, the counseling and educational procedures use short films to ensure a dynamic method of presentation (Figure 1).

ODYSSEE Kidney Health sample screenshots.
A user-centered design process is integral to maximize the adoption, satisfaction, and sustainment of patients.18,19 In this study, the development of ODYSSEE Kidney Health was guided by patients with CKD, grounded on a user-centered design process. The present study builds on a previous usability study by our team where the web page design and interactive digital tools and trackers were adapted. Design features were positively evaluated using an iterative design with successive rounds of feedback from patients with chronic heart failure. 20
In keeping with the user-centered design principles of MI,13,14 our digital intervention explicitly validates and reinforces the participant’s effort to identify their priorities for living well, and to connect these priorities with their goals for improving CKD self-care behavior. Furthermore, we use multimedia (video and infographics) to engage participants more holistically—in terms of the content and use of a dynamic medium for the method of patient engagement. Role modeling is also provided insofar as each user is provided with a video where CKD self-care and interpersonal support are presented. Accordingly, this study examines the design and development of the ODYSSEE Kidney Health program in patients with CKD.
Methods
Study Design
We conducted an iterative design process to develop the digital counseling program, ODYSSEE Kidney Health.
Study Setting
The study was conducted in the renal clinics at the University Health Network (UHN), Toronto, Canada. The clinics serve patients with category 4 to 5 CKD and patients who are receiving KRT (eg, home peritoneal dialysis and home hemodialysis).
Study Procedures
We used purposive sampling to gain representation and feedback from participants of varying backgrounds and experiences, including the years of CKD, primary cause of CKD, gender, ethnicity, and stage of CKD. For the purposes of this study, the intended aim of the platform is for patients with advanced CKD (category 3b to 5 and 5D but on a home-based modality). The involvement of key users in the process was intended to increase wider acceptance by patients and improve its overall adoption and effectiveness on a larger scale. A sample of 10 to 15 participants was anticipated through the purposive sampling method based on ensuring data quality and representation. 21
Eligible patients included adults (greater than 18 years of age) without cognitive impairment, proficient in English, and could provide informed consent to participate in the study. Research assistants identified eligible patients with the assistance of the clinical team by referring patients to the program. The study received ethics approval from the University Health Network Research Ethics Board (REB # 18-5969).
This study involved an iterative design and the development process guided by user-centered design principles with patients interviews and high-level usability testing.22,23 Two rounds of sessions informed successive adjustments and refinements of the program. Each round consisted of 2 parts. In the first part, participants reviewed the first sample e-session with the (1) self-help video, (2) educational infographics, (3) eTool, and (4) self-monitoring tracker. Participants took part in a “think-aloud” goal-oriented task where participants verbally expressed their thoughts as they completed each task by vocalizing thoughts about the program, expressing efficiencies and challenges with tasks (logging into the website and navigating through the site using links between pages). This task tested the users’ ability to navigate and complete the session and use the tools and media without assistance. Research assistants did not offer help during the tasks to minimize disruptions to the user’s thought process and used audio recording with field notes for data collection (Supplemental Appendix S1: Interview Guide).
After the completion of all goal-oriented tasks, the second part involved semi-structured interviews. During the interview, participants were asked to provide feedback on how the application could be incorporated into their day-to-day life and on any perceived benefits and challenges of using the application, which reflected their satisfaction and reflection on the digital program. Average time for the entire 2-part session was 60 minutes. The entire 2-part session was audiotaped for analysis, along with transcripts and field notes.
Data Analysis
Quantitative analysis: Descriptive statistics using means, SD(s), and percentages were calculated and used to characterize the study participants’ demographics and technology experience.
Qualitative thematic analysis: Transcribed data from the goal-oriented think-aloud session, interview responses, and field notes were analyzed using a thematic analysis approach based on user-centered design principles. 18 Initial categorical themes were derived based on digital solutions’ development cycle 22 (Supplemental Appendix S2: Data Analysis Guide). The responses were coded and categorized to address the overarching themes of the digital counseling program’s acceptability of the digital platform, feasibility of use, and impact on nephrology care. The themes identified related to the overall satisfaction of the participant’s usage of the program (eg, layout, navigation, content). Interviews took place until data saturation was reached, where no new information was obtained from additional interviews to further expand on categories or themes. Saturation was reached at 11 participants, prior to the targeted sample of 15 participants. Coding discrepancies were discussed and resolved between the 2 coders until consensus was reached.
Results
A total of 11 patients participated in the study. The baseline participant characteristics are summarized in Table 1 along with their familiarity and use of digital technology. Most of the participants were white (n = 6) and male (n = 7) and the mean age was 58 (±17) years, used or had access to a computer at home. Two participants did not have access to a computer nor broadband. Level of comfort with technology with all participants was reported to be high in the range of 7 out of 10, on a scale of 0 (not at all comfortable) to 10 (extremely comfortable). The Flesch-Kincaid grade level for written material used in this study was 8.5.
Baseline Study Participant Characteristics.

Thematic Findings
Main themes derived from the user-design process of the digital counseling program are summarized with supporting sample quotes in Table 2. The core theme that emerged while testing the counseling program is illustrated in the overlap in the diagram, highlighted in orange. It relates to the impact in kidney care of the digital counseling program in a patient’s day-to-day life. This impact stems from all behavioral components that make up self-management of CKD, which include behaviors that patients engage in daily (eg, diet, medications, exercise). These behavioral components are supported or hindered by the presence or absence of the second and third domains illustrated by the joint circles (red and yellow): technological features and the content and information of the digital counseling program.
Quotations From Study Participants With Thematic Categories.
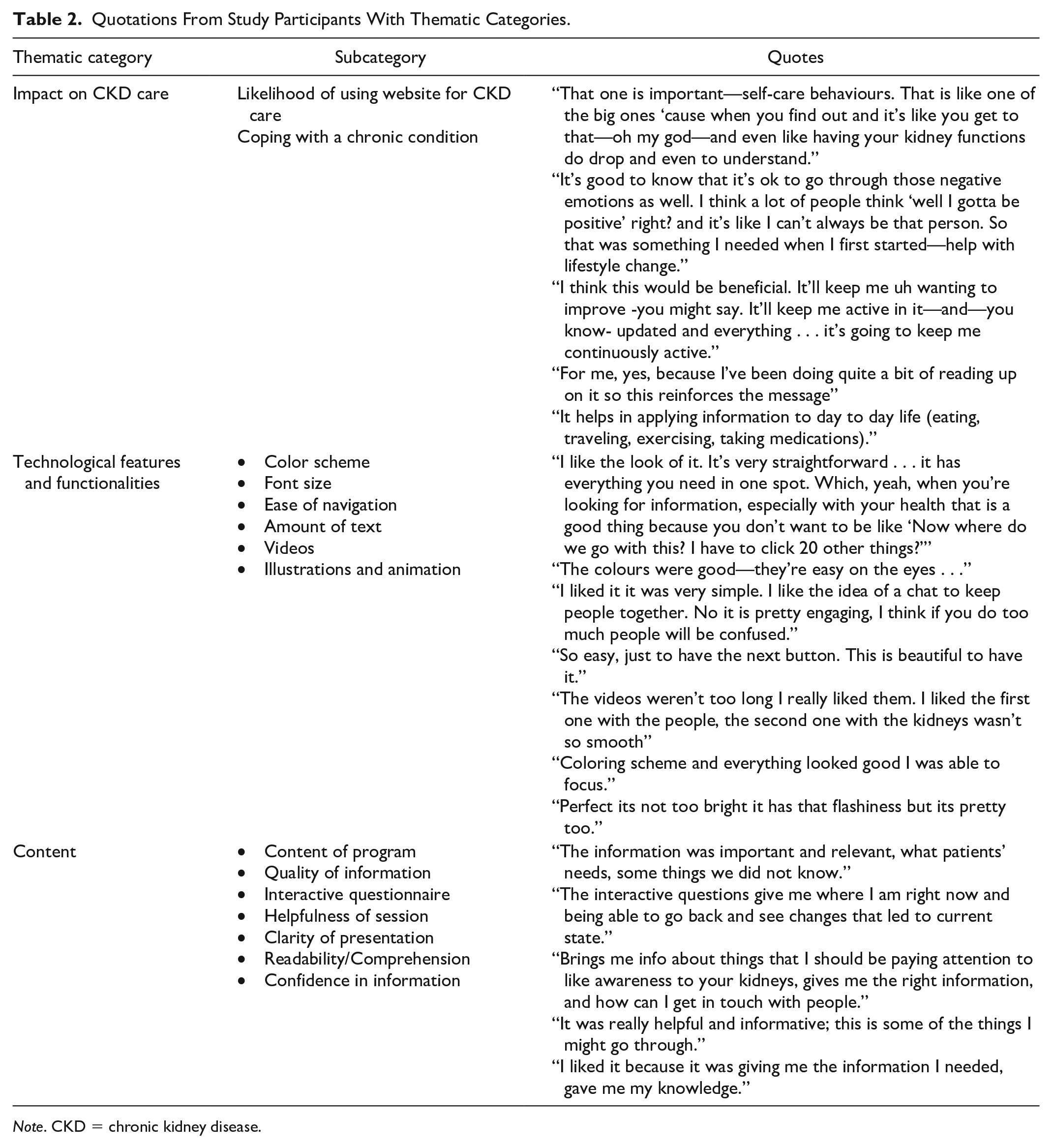
Note. CKD = chronic kidney disease.
Impact in nephrology care
The interplay between technological features, functionalities, along with clinical content, ultimately determines the role and impact the program will play in nephrology care. Participants repeatedly discussed the value of the program in a patient’s life and journey with CKD. Not only did the materials reinforce behaviors patients need to partake in, but participants also reported that the materials can also help them make informed decisions, particularly about the foods they eat and how to cope with stress. Participants learned how to stay engaged with their health and adhere to self-care behaviors while understanding why these are important in CKD care. Participants highlighted the impact of stress and negative thoughts on chronic disease and emphasized how the sample session taught them how to cope and manage their emotional well-being. Participants appreciated hearing about stress management and normalizing it with chronic disease, realizing that they have tools to help them manage it.
To further the program’s impact on CKD care, participants recommended several features that they foresee value in. These include the availability of online chat rooms to reach out to other kidney patients and have open discussions. Participants also noted that they need stage-specific information about CKD (nondialysis versus dialysis) so that patients can apply specific information to their current state. Participants also wanted to see “what-if” scenarios to know what they can do when their condition changes. Finally, participants expressed an interest in having “frequently asked questions” or “recent news,” to allow for constant and ongoing updates.
Technical features (navigation; design)
Participants described the overall navigation of the program as being “user-friendly” and “easy to navigate.” They were successful in logging into the website and accessing the e-session along with various types of media and pages associated with it. Participants did not report specific challenges related to the navigation nor the interpretation of program icons. Font size and color were well-received by patients and described as easy to view and readable. Some patients commented on the speed of the speaker’s speech delivery in the video as something that may hinder their learning. They recommended that if the speaker’s speech was delivered at a more moderate pace, comprehension and engagement would improve with patients. Participants did not provide any suggestions for further improvements regarding the navigation and design of the program.
Content
Participants expressed positive comments about the content of the program. Specifically, participants reported that having personalized CKD content was valuable. They stated that the variety of learning materials will also be of benefit to other patients, especially those who were recently diagnosed. Participants valued receiving information from medical experts who are known in the nephrology field. They expressed a sense of validation when receiving information from medical experts. Having different experts speak about common patient experiences and aspects of CKD management reinforced the importance of self-management in CKD. They commented that a variety of learning materials, such as infographics and videos, reinforced the messages.
Patients reported that information about CKD found from the Internet is often generic and not personalized for patients with CKD. Therefore, participants noted that information provided by the ODYSSEE Kidney Health program was from a “trusted source” and it applied meaningfully to their day-to-day life. Specifics on daily living with CKD along with managing stress and anxiety reinforced behaviors and coping mechanisms they need to adapt well with CKD. Learning to cope with the daily challenges of CKD management, such as managing a CKD-friendly diet, was also widely reported as important and needed. Participants felt that they wanted to see more information about local social supports or community services tailored for patients with CKD. They recommended that the incorporation of these resources would assist other patients who may be coping with other aspects in life affected by CKD such as finances, school, and employment.
Discussion
The adoption and sustained use of digital health tools rely heavily on meaningful user-centered design processes. In this study, we presented the design and development of a novel digital counseling program to promote adherence to self-care behaviors in CKD. Participants with advanced CKD underwent a thorough analysis of the use and performance of the digital program which revealed positive acceptance and feedback in these initial stages. There is a paucity of prior published studies examining the automated digital counseling program targeting patients with CKD. Widespread implementation and acceptability will hinge upon results from implementation studies, anchored on user-designed processes.
Although self-management has been heavily promoted in the care of chronic conditions like CKD, mechanisms to support and reinforce self-care behaviors including mental health management of patients are lacking. ODYSSEE Kidney Health aims to support patients with CKD in managing their condition along with providing personalized information and psychosocial support. A recent scoping review revealed that most CKD-directed self-management interventions do not follow a patient or user-centered approach, and most are not grounded on a theoretical framework. 24 Incorporation of end-user perspectives at the initial stages of development ensures that the program addresses end-user needs, eventually determining their adoption and adherence to self-management behaviors. Like other self-management interventions, 25 ODYSSEE Kidney Health targets key elements of CKD management including food, monitoring blood work, and adherence to medications. On top of reinforcing self-management behaviors, ODYSSEE Kidney health expands on core behaviors to include support for mental health issues such as stress, anxiety, and depression. Previous studies using CBT-based interventions in CKD were found to be acceptable and demonstrated improvements in treatment adherence and health-related quality of life.26-28 The combined strategy of self-management and psychosocial intervention increases the likelihood that patients will acquire skills to cope and adhere to behaviors needed to manage their condition. The structured and organized format of ODYSSEE Kidney Health focuses on building skills and knowledge in a patient, and it includes a holistic team-based approach and cognitive behavorial support. This elevates self-management into a new dimension to ensure behaviors are treated using a motivational and cognitive behavioral framework.
The CKD population generally consists of patients aged 65 years or older with lower health and digital literacy.29,30 Despite increased use and interest among patients with CKD in digital health tools, sustained adoption is low. 30 Educational resources often do not consider the health literacy level or patients with CKD nor support their decision-making processes. 31 Engaging users from the development and design stage is significant to ensure the needs and requirements of end-users are addressed, including health and digital literacy gaps. The layout, design, navigation, and CKD personalized content were well-received and did not pose challenges to participants. In summary, comments from participants suggested that a wide range of CKD users is likely to adopt and engage with the ODYSSEE Kidney Health program and that it will be accessible to individuals with various levels of literacy and technological familiarity.
To the best of our knowledge, this presents an innovative first automated digital program that focuses on self-care behaviors for CKD in an organized and structured format that is enhanced with evidence-based models of behavioral counseling, CBT, and MI. The study included patients with CKD in various stages of disease progression and sociodemographic backgrounds. Despite these strengths, the study does present certain limitations. First, many study participants had previous exposure with technology which may have impacted their experience during goal-oriented tasks during the study. The participants did represent a variety of backgrounds and ranged from 30 to 82 years. Second, we only used one of the 16 sessions in the “think-aloud” session. Although participants did not have the opportunity to comment on other sessions, the test session included all the core content elements, multimedia, and interactive tools and trackers that are representative of the entire program. Finally, study participants were derived from a single center and may not represent the general CKD population. The purposive sample aimed to ensure representation from various CKD types and address this limitation.
This study is significant in several ways. First, it demonstrates the role of active patient involvement in the co-design and development of a digital health tool and digital counseling program that is based upon core features from established cognitive behavioral and motivational models of counseling. Iterative rounds of the development process provided early evidence of the intervention’s acceptability and feasibility in various areas of nephrology care. Second, this study addresses current gaps in self-management interventions for patients with CKD. Gaps in present interventions include lack of patient engagement during development and absence of a behavior change theory framework in their design. 24 Overall, a sample of participants who are representative of the CKD patient population at our hospital positively accepted the program, and the feedback generated was used to iteratively refine ODYSSEE Kidney Health. Patient participants consistently cited the significance of such an intervention in day-to-day CKD care. Finally, findings from the present study highlight the need to ensure patient engagement is incorporated in interventions intended to promote CKD self-care. Chronic kidney disease is a complex condition requiring attendance to multiple care domains. The complexity of care requires patients to be supported and interventions tailored to their needs and specific stage of kidney disease. Future research will implement the digital counseling program with a wider group of patients with CKD to address long-term acceptability, as well as its efficacy in improving clinical outcomes and quality of life.
Conclusion
The success and effectiveness of integrating a digital counseling tool such as ODYSSEE Kidney Health rely on incorporating the patient’s voice and realizing the impact in their daily lives. The iterative design of ODYSSEE Kidney Health supported this which will then be implemented in a feasibility trial in patients with advanced CKD.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581221103683 – Supplemental material for Design and Development of a Digital Counseling Program for Chronic Kidney Disease
Supplemental material, sj-docx-1-cjk-10.1177_20543581221103683 for Design and Development of a Digital Counseling Program for Chronic Kidney Disease by Stephanie W. Ong, Julia V. Wong, Bourne L. Auguste, Alexander G. Logan, Robert P. Nolan and Christopher T. Chan in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We thank all the patients who agreed to participate in the study as well as the administrative and clinic staff in the renal clinics at the University Health Network for their support in patient recruitment.
Author Contributions
All authors participated in the planning, execution, and analysis of the study. All have read and approved the final submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project sponsor was the Toronto General & Western Hospital Foundation—Slamen/Miller Fund in Nephrology.
Statement of Ethics
The study was reviewed and approved by the University Health Network Institutional Research Ethics Board (REB # 18-5969).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.