
Abstract
Purpose:
Iodinated contrast media is one of the most frequently administered pharmaceuticals. In Canada, over 5.4 million computed tomography (CT) examinations were performed in 2019, of which 50% were contrast enhanced. Acute kidney injury (AKI) occurring after iodinated contrast administration was historically considered a common iatrogenic complication which was managed by screening patients, prophylactic strategies, and follow-up evaluation of renal function. The Canadian Association of Radiologists (CAR) initially published guidelines on the prevention of contrast induced nephropathy in 2007, with an update in 2012. However, new developments in the field have led to the availability of safer contrast agents and changes in clinical practice, prompting a complete revision of the earlier recommendations.
Information sources:
Published literature, including clinical trials, retrospective cohort series, review articles, and case reports, along with expert opinions from radiologists and nephrologists across Canada.
Methods:
The leadership of the CAR formed a working group of radiologists and nephrologists with expertise in contrast administration and patient management related to contrast-associated AKI. We conducted a comprehensive review of the published literature to evaluate the evidence about contrast as a cause of AKI, and to inform evidence-based recommendations. Based on the available literature, the working group developed consensus recommendations.
Key Findings:
The working group developed 21 recommendations, on screening, choice of iodinated contrast media, prophylaxis, medication considerations, and post contrast administration management. The key changes from the 2012 guidelines were (1) Simplification of screening to a simple questionnaire, and not delaying emergent examinations due to a need for creatinine measurements (2) Prophylaxis considerations only for patients with estimated glomerular filtration rate (eGFR) less than 30 mL/min/1.73 m2 (3) Not recommending the routine discontinuation of any drugs to decrease risk of AKI, except metformin when eGFR is less than 30 mL/min/1.73 m2 and (4) Not requiring routine follow up serum creatinine measurements post iodinated contrast administration.
Limitations:
We did not conduct a formal systematic review or meta-analysis. We did not evaluate our specific suggestions in the clinical environment.
Implications:
Given the importance of iodinated contrast media use in diagnosis and management, and the low risk of AKI after contrast use, these guidelines aim to streamline the processes around iodinated contrast use in most clinical settings. As newer evidence arises that may change or add to the recommendations provided, the working group will revise these guidelines.
Introduction
Iodinated contrast medium (ICM) is one of the most frequently administered pharmaceuticals, with an estimated 80 million doses administered globally in 2006. In Canada, over 5.4 million computed tomography (CT) examinations were performed in 2019, of which 50% were contrast enhanced. 1 In addition to CT, ICM is used for angiography and other interventional radiology and cardiology procedures. Acute kidney injury (AKI) occurring after ICM administration has historically been considered a common iatrogenic complication which was managed by screening patients, prophylactic strategies, and follow-up evaluation of renal function. Although AKI associated with ICM administration is reversible (returning to baseline creatinine in 1-3 weeks), AKI in this setting is associated with a higher risk of both short-term and long-term mortality.2,3 To date, there have been no adequately powered clinical trials showing that its prevention results in survival benefit, and the deprivation of contrast-enhanced imaging may have important unintended clinical consequences, 4 most importantly a missed or delayed diagnosis.
Guidance on this topic requires interprofessional collaboration, given that contrast-enhanced diagnostic and therapeutic procedures are ordered by various specialties, performed by other specialists, and require management by nephrologists in the event that AKI develops. This document, which was developed by a multidisciplinary working group of radiologists and nephrologists, reviews the scientific evidence for contrast-associated acute kidney injury (CA-AKI) and provides consensus-based guidelines for its prevention and management.
A summary of terms used in these guidelines is presented in Table 1. Contrast-associated acute kidney injury, also known as post-contrast acute kidney injury (PC-AKI), is a general term used to describe a sudden deterioration in renal function that occurs within 48 hours after the intravascular administration of ICM. Contrast-associated acute kidney injury may occur regardless of whether the contrast medium was, or was not, the cause of the deterioration. Contrast-induced acute kidney injury (CI-AKI), formerly referred to as contrast-induced nephropathy, is a specific term used to describe AKI that is caused by the ICM administration; therefore, CI-AKI is a subgroup of CA-AKI. 5 Since the causal attribution of contrast leading to AKI is not clear, CA-AKI is the appropriate term used throughout this document, except in the sections describing the causal literature.
Definitions/Terminology.

Note. Italicized terms are historical and not recommended for use. KDIGO = Kidney Disease Improving Global Outcomes; OR = odds ratio; AKI = acute kidney injury; CKD = chronic kidney disease; CA-AKI = contrast-associated acute kidney injury; PC-AKI = post-contrast acute kidney injury; CIN = contrast-induced nephropathy; CI-AKI = contrast-induced acute kidney injury.
See supplementary appendix for actual criteria.
The Canadian Association of Radiologists (CAR) last provided guidance related to CA-AKI in 2012. 6 A summary of what has changed between this document and the 2012 recommendations is detailed in Table 2.
Changes to Recommendations Between 2012 and 2022 Guidelines.

Note. Changes in terminology: CIN (2012) to CA-AKI (2022); eGFR units mL/min (2012) to mL/min/1.73 m2 (2022); CM (2012) to ICM (2022). eGFR = estimated glomerular filtration rate; CM = contrast media; ICM = intravascular contrast media; CIN = contrast-induced nephropathy; CA-AKI = contrast-associated acute kidney injury; AKI = acute kidney injury; IA = intra-arterial; IV = intravenous; ACEi = angiotensin converting enzyme inhibitors; ARBs = angiotensin receptor blockers; CT = computed tomography; CAR = Canadian Association of Radiologists.
Is CI-AKI a “myth”?
Over the last 4 decades, the perception of CI-AKI has evolved from being viewed as a common and widespread complication to being questioned as a medical “myth.” In an influential study from 1983, it was reported that contrast media (CM) were the third most common cause of AKI in the hospital setting, after hypovolemia and major surgery. 7 Unfortunately, this study was a small case series that included only admitted inpatients, lacked a control group of patients who did not receive contrast, and evaluated high-osmolar CM, which are no longer used. A 2006 study reported that of 3081 articles published between 1996 and 2004 and containing keywords such as “contrast” and “kidney failure,” only 40 (1.3%) evaluated patients who received intravenous (IV) contrast, and only 2 had control groups of patients who did not receive CM. 8 Another study of over 32 000 hospitalized patients showed that fluctuations in creatinine levels are quite common: about 27% of inpatients have a 25% or greater rise in creatinine, even in the absence of any ICM administration. 9 A control group is important in such studies, since it allows for assessing the background incidence of AKI, which would be expected in patients who are unwell and undergoing CT examinations for various indications, such as sepsis or hypoperfusion. Some patients develop AKI from their underlying disease, or other concomitant causes, such as ischemic acute tubular necrosis due to renal hypoperfusion, drug-induced acute interstitial nephritis, and atheroembolic renal disease. 10
Subsequent studies using advanced statistical methods to control for confounding variables (propensity score–matched analyses) have failed to find evidence for true CI-AKI, with limitations described below. These studies demonstrate that the incidence of AKI associated with contrast-enhanced CT scans is no higher than the incidence of AKI associated with unenhanced CT scans (Table 3).11-14 It is important to note that negative propensity score studies cannot be interpreted as “CI-AKI is a myth”; however, the results do indicate that the incidence of true CI-AKI is far less than previously thought. However, propensity scoring only addresses known bias, and covariates are captured in an administrative database; unknown biases and confounders are not accounted for as they would be in a randomized clinical trial (RCT). Although these studies are large (n > 10 000), the number of patients with severely reduced kidney function (eg, estimated glomerular filtration rate [eGFR] ≤30 mL/min/1.73 m2) who are at highest risk for CI-AKI was low, with uncertainty persisting in this population. Paradoxically, some studies found a lower risk of AKI with contrast, compared with unenhanced scans, which reflects selection bias rather than any nephroprotective effect of contrast.11,12 In the study by Davenport et al, 14 there was a slightly higher risk of AKI when grouping by eGFR (especially when eGFR ≤30 mL/min/1.73 m2), but this finding has not been replicated in other studies. 2
Major Epidemiological Studies of Contrast and AKI.
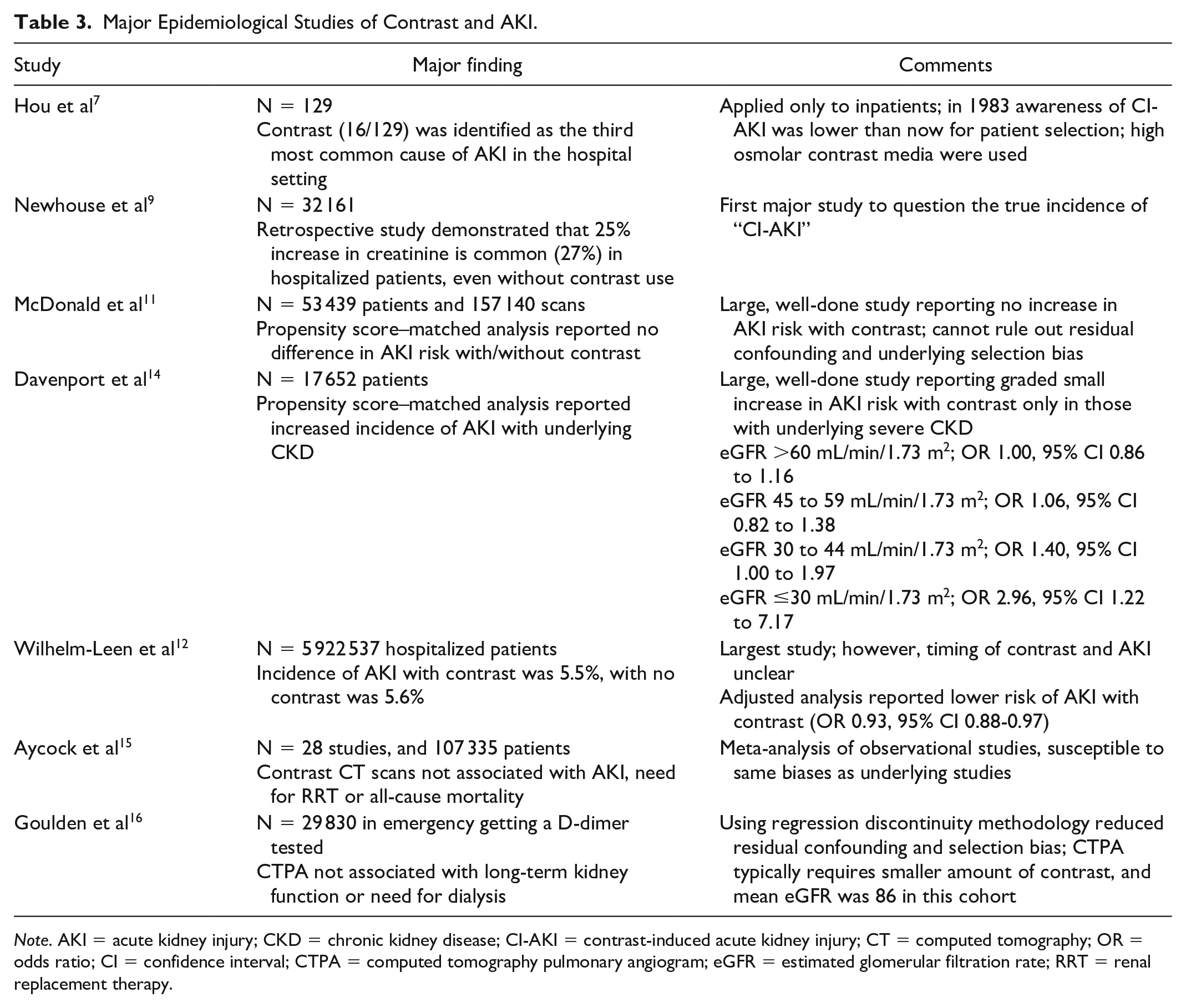
Note. AKI = acute kidney injury; CKD = chronic kidney disease; CI-AKI = contrast-induced acute kidney injury; CT = computed tomography; OR = odds ratio; CI = confidence interval; CTPA = computed tomography pulmonary angiogram; eGFR = estimated glomerular filtration rate; RRT = renal replacement therapy.
In summary, the role of contrast as the cause of AKI remains unproven and the risk of contrast as a cause of AKI is likely very low. However, there is currently insufficient evidence to claim that there is zero risk. The risk, if any, is only important in patients with severe underlying chronic kidney disease (CKD) with an eGFR ≤30 mL/min/1.73 m2, those with AKI, and/or those receiving a high volume of contrast especially through the arterial route. In addition, the above discussion on AKI after contrast relates to the occurrence of AKI as defined by a small rise in creatinine. The risk of severe AKI, including the need for renal replacement therapy (RRT), is several orders of magnitude lower.
Screening and Risk Stratification
Goals of Screening
The goals of screening are to identify patients at risk of preventable kidney function decline associated with the use of ICM. Since the publication of the 2012 CAR guidelines, 6 new research has significantly reduced our estimates of the risk associated with the use of ICM; at the same time research has increased our awareness of the negative clinical impacts of delayed imaging or suboptimal imaging done without ICM. 17 The guidance on screening has been summarized in Figure 1.

Iodinated contrast media guide.
Chronic Kidney Disease
The most important predictors of CA-AKI are the presence of CKD, and AKI from other causes. Risk can be stratified according to the Kidney Disease Improving Global Outcomes (KDIGO) staging (see Supplementary Table 1). Comorbidities, such as diabetes, exposure to nephrotoxic agents, hypovolemia, and congestive heart failure, are associated with CA-AKI. Similarly, having a single kidney, including a transplant kidney, can help to identify patients more likely to have CKD. However, none of these factors have been shown to be independent of eGFR.2,43
Patients with normal kidney function and those with stable mild or moderate CKD are considered at negligible risk regardless of other factors. Only those with severe CKD (eGFR ≤30 mL/min/1.73 m2), and those with preexisting AKI are at risk of CA-AKI.
The process of screening should allow the triage of most patients with small or negligible risk to receive a medically indicated contrast-enhanced CT scan without undue cost or delay. The screening should also flag those with an increased risk to a more intensive screening and prevention process with 3 targeted interventions:
Measure kidney function using eGFR
Decide whether ICM or an alternate imaging strategy can best address the clinical question
In at-risk patients that require ICM, consider prophylactic strategies
Specific Risk Groups
Outpatients with known eGFR
When the eGFR is known it should be used in the decision regarding the use of ICM. When the requisition indicates a history of kidney disease and no eGFR is available, the working group recommends that there be an automatic trigger for ordering an eGFR. For a stable outpatient, an eGFR within 3 to 6 months was considered acceptable by the workgroup. However, if the history indicates kidney injury, then a shorter interval would be more appropriate, and if the history indicates stability in renal function, then a longer interval may be appropriate.
Outpatients without a known eGFR
For patients without an eGFR and without a reported history of kidney disease, we recommend a simple screening questionnaire such as: “Do you have kidney problems or a kidney transplant? Have you seen or have you been referred to see a kidney specialist (nephrologist) or a urologist?” If the answer is yes, an eGFR is required before protocoling the study with ICM. If the answer is no, an indicated ICM examination can proceed without an eGFR value.
Emergency patients
In the emergency setting, a detailed history and eGFR may not be immediately available. Attempts should be made to determine the exam urgency and patient prognosis, and to obtain the current and baseline renal function. When a patient is facing a life-threatening illness, indicated examinations with ICM should not be withheld for fear of CA-AKI. Referring health care providers and radiologists must weigh the benefits of a contrast-enhanced CT versus the very small, theoretical risk of a transient AKI. In patients in whom that risk is considered to outweigh the benefits of ICM administration, other options to consider are the use of non-enhanced CT with a radiologist check or other imaging modalities. When other imaging strategies are inferior or impractical, ICM use may be the best option for the patient. Meta-analyses from the emergency medicine and stroke literature suggest that there is minimal AKI risk with ICM use in these settings.12,18,19
Inpatients
The working group recommends that the decision to proceed with ICM is made after reviewing the most current eGFR obtained not more than 7 days prior to the planned injection. When eGFR ≤30 mL/min/1.73 m2 or if AKI is suspected, then the inpatient care team or ordering physician should clearly indicate in the requisition that the study should proceed with ICM if needed for diagnosis. When this is unclear, the radiologist may proceed with ICM if the condition is urgent (eg, stroke code, pulmonary embolism, other high-risk unstable presentations) or if there is no practical substitute for ICM-enhanced scan. 20 If the scenario is uncertain, then the radiologist should contact the referring physician to discuss the urgency of the test and weigh the potential benefits and harms of administering versus withholding ICM.
Contrast use in AKI setting
In patients with AKI, risk stratification according to kidney function is not possible as eGFR measurement is unreliable. 21 While patients with AKI might be more susceptible to nephrotoxin-induced kidney damage than those without AKI, no controlled studies report on this risk. Given the current paucity of evidence, 5 a cautious approach might favor avoiding ICM. Nonetheless, in these patients, the potential risk of developing CA-AKI must again be weighed against the risk from delayed or missed diagnoses by avoiding ICM. Regarding the use of intra-arterial (IA) contrast in such patients, although the risk of CA-AKI may be higher overall, it is frequently indicated in the acute setting for potentially life-saving or limb-saving diagnostic and therapeutic procedures. Under these circumstances, the overall benefits are likely to outweigh the risks. Thus, as is the case in any clinical context, the use of contrast in patients with preexisting AKI requires clinical judgment with respect to the overall risks, benefits, and available alternatives.
Chronic dialysis patients
It is widespread practice to use ICM for indicated examinations in anuric dialysis patients as the risk of loss of renal function is nonexistent. There is no need to change the dialysis schedule; dialysis at the usual predetermined timing is the least disruptive and customary practice. Some dialysis patients have residual urine output (“residual renal function”) such as peritoneal dialysis patients or patients within the first few months of starting hemodialysis. Historically, it was believed that ICM could further reduce renal function in this setting. However, a systematic review of 9 studies reveals that there is little effect of ICM on residual renal function (weighted difference in means −0.16 mL/min, 95% confidence interval [CI] −0.66 to 0.34 mL/min; P = .53). 20 Thus, the presence or absence of residual urine output should not influence the decision to use ICM in dialysis patients. In summary, ICM can be given to patients on peritoneal or hemodialysis regardless of residual urine output and no change in dialysis schedule is required.
Safety of Repeat Contrast Administration
Two studies have demonstrated the occurrence of CA-AKI in patients that received a second dose of CM within 48 hours of their first dose.22,23 Neither of these studies specifically examined whether the risk of CA-AKI was increased relative to having had only a single contrast exposure or none at all. 5
Given the lack of evidence in this area, the working group considered it prudent to avoid repeated contrast exposures for 48 hours for elective procedures in patients considered at higher risk of CA-AKI (eGFR ≤30, AKI, high-volume IA ICM administration). 24 The working group did not recommend restricting repeat contrast doses in lower risk patients (eGFR ≥30, no AKI, IV route). The working group did not recommend withholding repeat doses for emergency or inpatients who have life-threatening or acute presentation of illness. Examples include a nondiagnostic CT pulmonary angiogram, short-term repeat evaluations of trauma, surgical complications, and vascular interventions. In the face of life-threatening illness, repeat dosing of ICM may be necessary and justified to establish a confident diagnosis and treatment plan.
Summary
Screening for at-risk patients is thought to be beneficial. . However, this must be balanced with the significant benefits of contrast-enhanced diagnostic and therapeutic procedures. These screening guidelines focus on balancing risks (risk of CA-AKI, patient delays, and health care costs) as well as significant benefits of timely diagnostic tests with ICM. The vast majority of patients having diagnostic tests and procedures with ICM will not experience a significant or permanent worsening of renal function, dialysis, or increased morbidity.
Arterial Contrast Administration
There is some evidence that the risk of CA-AKI is increased with the administration of IA ICM compared with the administration of IV ICM. 25 For elective diagnostic procedures requiring IA ICM, a similar approach to IV ICM is recommended with an acknowledgment that there might be an increased risk. In the setting of therapeutic procedures, the risk to the kidneys must be balanced against the benefits of the proposed treatment and the risks associated with an alternate procedure not requiring IA ICM, if available. With therapeutic procedures requiring ICM, alternates are rarely available or clinically appropriate, and ICM administration may be necessary, even in high-risk settings (eg, with eGFR <30 mL/min/1.73 m2). This decision should be made by the care team in discussion with the patient or family/alternate decision maker.
Prophylactic Measures
In this section, we discuss the evidence for various pharmaceutical agents and strategies to minimize the risk of CA-AKI.
N-acetylcysteine
N-acetylcysteine (NAC) is a mucolytic and can act as an antioxidant by regenerating glutathione. Since reactive oxygen species were initially thought to be involved in the pathogenesis of CI-AKI, there was some rationale for trying NAC in this setting. The initial small RCT was encouraging and reported a large benefit in lowering AKI, and given that this molecule is easy to administer, use became widespread. 26 However, subsequent trials showed mixed results. In the last decade, 2 large RCTs that together enrolled more than 7000 patients have settled this issue, with conclusive evidence that NAC use does not protect from the development of CA-AKI.27,28 Some intriguing recent evidence suggests that NAC may actually have an artifactual effect on creatinine measurement, rather than on the physiology of nephrotoxicity.29,30 Thus, there is strong evidence against prophylactic use of NAC for CA-AKI.
Hydration or Volume Expansion
The data on the need for volume expansion and the type of fluid used are summarized in Table 4. Briefly, there is high-quality evidence to support that in those with eGFR >30 mL/min/1.73 m2 undergoing elective ICM administration, there is little benefit with IV hydration compared with no hydration.31,32 There is insufficient evidence to support or refute the current widespread practice of hydration (IV or oral) at or below eGFR 30 mL/min/1.73 m2, compared with no hydration. In addition, there is low-quality evidence that oral hydration may be as effective as IV hydration. 33 There is a lack of evidence to either support or refute the use of hydration for prophylaxis of CA-AKI in high-risk patients (severe CKD, eGFR ≤30 mL/min/1.73 m2). As such, the working group makes no recommendation in this regard and institutions may choose practices best suited to their local environments.
Summary of the Literature With Volume Expansion and Hydration.

Note. CI = confidence interval; eGFR = estimated glomerular filtration rate.
The working group recognizes that organizing IV hydration may be logistically challenging in some patients. Thus, if volume expansion is being considered, either oral or IV hydration may be utilized in these patients for CA-AKI prophylaxis, acknowledging the low certainty of the benefit of this approach. For choice of IV hydration, bicarbonate-based fluid does not provide any added benefit to the use of normal saline for volume repletion around contrast administration. The 0.9% saline is easier to procure and administer, so would be the preferable option, though bicarbonate-based fluids may be used as being equivalent if local factors, protocols, or convenience support this. Some members of the working group endorsed a strategy of hydration and volume expansion more strongly for high-risk patients receiving IA ICM. However, there is insufficient evidence to support the benefits and the working group felt this was best left to judgment of the practitioner.
Contrast Dose
Higher doses and repeat dosing of contrast have been associated with a higher risk of CA-AKI.34,35 However, confounding by indication may contribute to the observed incidence. For example, technically complicated procedures in high-risk patients may receive higher contrast doses, particularly for some cardiac interventions. Extrapolating this to routine clinical doses in lower risk clinical scenarios is likely to result in suboptimal scans with little or no safety benefit. Reduced dosing of IV contrast administration for CT examinations is discouraged because it will lower parenchymal enhancement and deviate from established high-quality protocols. The working group recommends using the appropriate IV dose for high-quality CT imaging in all patients. For IA interventions, a pragmatic approach is recommended using the necessary dose to achieve the diagnostic and therapeutic results but judiciously reducing dose when adjunctive imaging and doses are low yield or can be delayed (such as ventriculography after cardiac catheterization). 36
The physicochemical characteristics of the CM also have a role to play in its nephrotoxicity. Until a few decades ago, ionic and high osmolar CM were used, with osmolality >1200 mOsm/L. Since then, nonionic and low-osmolar (osmolality typically ~600 mOsm/L) as well as iso-osmolar CM have been developed, and these are the only agents now used globally. There is convincing evidence from a meta-analysis with data from 31 RCTs that there is lower risk of CA-AKI (relative risk [RR] 0.61, 95% CI 0.48-0.77) with low-osmolar CM compared with high-osmolar CM. 37
With respect to low-osmolar CM versus iso-osmolar CM, the literature is mixed. A small initial RCT showed a large benefit in favor of iso-osmolar contrast, but subsequent RCTs and meta-analyses have conflicting and heterogenous results. 38 As an example, moderate statistical heterogeneity was reported in this meta-analysis of 25 RCTs with an overall RR of 0.75 (95% CI 0.44-1.26). 39 The authors resolved the heterogeneity by grouping low-osmolar contrast into iohexol (RR for iodixanol versus iohexol 0.45, 95% CI 0.26-0.76) and all other low-osmolar contrast (RR 0.97, 95% CI 0.72-1.32). Another 2017 systematic review included 10 RCTs, and demonstrates no added benefit with using iso-osmolar CM compared with low-osmolar CM (RR 0.72, 95% CI 0.50-1.04). 40 Any possible observed benefit was attenuated further when the analysis was restricted to large RCTs with sample size more than 250, as a surrogate for trial quality (RR 0.93, 95% CI 0.66-1.30). Thus, overall, there is little difference for AKI events between iso-osmolar and low-osmolar contrast in a high-risk setting, and hence a negligible difference in low-risk setting (venous contrast) for clinically meaningful outcomes. Hence the choice of CM between low-osmolar and iso-osmolar should be made based on other considerations (eg, cost, availability).
Dialysis
Renal replacement therapy in the form of hemodialysis or hemofiltration has been tried as a prophylactic strategy, which is paradoxical since the reason to prevent CA-AKI is to avoid dialysis and related morbidity. Physiologically, intravenously injected ICM reaches the kidney within a few cardiac cycles, and subsequent extracorporeal removal of circulating contrast would be unlikely to have any beneficial effect. Renal replacement therapy also lowers serum creatinine, hence leading to a spurious reported benefit in outcomes when measured as a change in serum creatinine in some trials. 43 A 2006 systematic review 44 and another larger subsequent trial 45 reported no benefit with RRT in AKI after contrast, as expected. The RRT procedure itself is associated with complications associated with catheter placement and hemodynamic instability, and increased health care resource utilization. There is no role for prophylactic RRT in the setting of contrast administration.
Statins
Statins have been trialed in preventing CA-AKI, mostly in the setting of coronary angiography and percutaneous coronary interventions. There is no clear mechanism by which statins should provide renoprotection, apart from their pleiotropic roles. 46 Most, if not all, RCTs with statins are in the setting of coronary angiography, and it may be argued that these patients with preexisting cardiovascular disease should be on a statin anyways for cardiovascular protection. Patients at elevated risk of AKI after contrast, specifically those with eGFR ≤30 mL/min/1.73 m2, are also at higher cardiovascular risk. 47 Thus, though the mechanism and evidence for AKI prevention in this setting for statins are not strong, there is no signal for harm as well, and the working group acknowledges that statins may be used for cardiovascular prevention in this population. However, the use of statins for the sole purpose of prophylaxis for CA-AKI is not recommended.
Other Agents
Several other pharmaceutical agents have been tried for prevention of PC-AKI, including theophylline, 48 prostaglandin E1, 49 nicorandil, 50 ascorbic acid, 51 allopurinol, 52 alpha-tocopherol, 53 fenoldopam, natriuretic peptides, 46 and trimetazidine. 54 Though some of these trials report a small benefit, these trials are small, and with unclear benefit in clinical outcomes, like the initial NAC trials. Unless large RCTs demonstrate any clinical benefit, there is no role to use these agents for CA-AKI prophylaxis in the contrast setting.
Drug Interactions With Contrast: Metformin, Renin-Angiotensin System (RAS) Inhibitors, Diuretics
Metformin is not a risk factor for developing CA-AKI and the injection of ICM is not contraindicated in patients receiving it. However, serious complications (metformin-associated lactic acidosis [MALA]) may rarely occur in patients taking metformin who subsequently develop CA-AKI. For this reason, metformin has often been held in patients undergoing studies with intravascular ICM. Whether this should be done at the time of, or 48 hours before, contrast injection and whether metformin must be held in all patients or only those with underlying kidney disease are controversial. The monogram for Glucophage (metformin; Merck Sante Corporation, Lyon) in the Compendium of Pharmaceuticals and Specialities 55 recommends that metformin be discontinued at the time of, or prior to, any planned contrast exposure and be withheld for 48 hours afterward, only being reinstituted after kidney function has been confirmed to be stable. In general, this guidance has gradually been superseded by less restrictive recommendations as evidence has accumulated that, independent of kidney function, the overall risk of MALA precipitated by metformin accumulation due to CA-AKI is exceptionally low in the absence of other concurrent acute medical conditions such as sepsis and/or AKI.
In this context, the American College of Radiology (ACR) Manual on Contrast Media 5 now recommends that, in patients with eGFR >30 and without evidence of AKI, metformin need not be stopped prior to ICM administration and there is no need for testing to evaluate kidney function afterward. Similarly, the European Society of Urogenital Radiology which had also previously endorsed a more conservative approach 56 now recommends continuing metformin at the time of contrast injection in patients with a baseline eGFR >30 mL/min/1.73 m2 (except patients with AKI or those receiving IA contrast with first-pass kidney exposure). 57 In our opinion, this less restrictive approach regarding metformin is warranted. Since the risk to patients is extremely low, 58 we consider it unnecessary to hold metformin or to recheck kidney function in patients with normal to moderately impaired baseline kidney function. For patients with AKI or an eGFR ≤30 mL/min/1.73 m2, it remains appropriate to stop metformin at the time of, or prior to, ICM injection. For these patients, ongoing use of metformin carries a higher risk of MALA irrespective of ICM administration. Therefore, radiologists/radiology departments should advise these patients to withhold metformin, and only restart the medication after discussion with the requesting physician (or a physician knowledgeable about their diabetes management plan).
Renin-angiotensin system inhibitors such as ACE inhibitors (ACEi) and angiotensin receptor blockers (ARBs) are commonly prescribed blood pressure medications that exert an effect on intraglomerular hemodynamics. In doing so, ACEi/ARBs might theoretically trigger or worsen AKI in the context of ICM exposure. A recent systematic review and meta-analysis analyzed the effect of holding ACEi/ARBs prior to coronary angiography. 59 This meta-analysis reported that discontinuation of ACEi/ARB did not decrease AKI risk (RR 1.48, 95% CI 0.84-2.60). 14 As such, the current evidence suggests that there is no meaningful benefit of discontinuing ACEi/ARB prior to contrast injection.
Although diuretic use has been previously shown to be a risk factor for CA-AKI, 14 the extent to which this is a causative relationship is unknown. Volume depletion in patients who are “over-diuresed” could theoretically contribute to a higher likelihood of, and more severe, CA-AKI. Yet there are also obvious risks to holding diuretics in patients who require them to maintain euvolemia. Diuretic discontinuation can precipitate fluid overload which, in addition to presenting a risk for pulmonary edema and other negative outcomes, may itself be detrimental to kidney function. 60 Currently, there is insufficient evidence to support routinely holding diuretics prior to contrast injection and the theoretical foundation for doing so is considered weak.
Post-contrast Administration Considerations
Follow-up
Contrast-associated acute kidney injury is diagnosed based on serum creatinine measurement after ICM administration. Typically, CA-AKI is defined by an elevation of creatinine of 26 µmol or higher. However, these are clinical research definitions of AKI, and do not necessarily meet any threshold for symptoms or necessitate management change. Routine measurement of creatinine in this setting is logistically difficult to arrange, and will provoke unnecessary anxiety for patients, and extra health care resource utilization with no clear benefit. Hence, routine measurement of creatinine should be reserved for those with extremely high risk of CA-AKI. A follow-up serum creatinine measurement is therefore recommended 48 to 72 hours only after IA ICM administration in patients with eGFR ≤30 mL/min/1.73 m2. For the remainder of patients, the risk of AKI is considered sufficiently low that routine testing is not warranted. However, other at-risk patients should be instructed to seek medical attention should they develop increased shortness of breath or peripheral edema and/or if they note a marked decline in urine output in the days following the procedure, which can trigger testing for kidney function.
Management of CA-AKI
As discussed above, there is no role for routine extracorporeal removal of ICM with dialysis. If CA-AKI occurs, we suggest that clinical evaluation and management of AKI due to CA-AKI be undertaken according to the KDIGO clinical practice guidelines for AKI 21 and taking account of the Canadian Society of Nephrology (CSN) commentary on those guidelines. 61

Supplemental Material
sj-docx-1-cjk-10.1177_20543581221097455 – Supplemental material for Canadian Association of Radiologists Guidance on Contrast-Associated Acute Kidney Injury
Supplemental material, sj-docx-1-cjk-10.1177_20543581221097455 for Canadian Association of Radiologists Guidance on Contrast-Associated Acute Kidney Injury by D. Blair Macdonald, Casey D. Hurrell, Andreu F. Costa, Matthew D. F. McInnes, Martin O’Malley, Brendan J. Barrett, Pierre Antoine Brown, Edward G. Clark, Anastasia Hadjivassiliou, Iain Donald Craik Kirkpatrick, Jeremy Rempel, Paul Jeon and Swapnil Hiremath in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
This article is being published concurrently in the Canadian Association of Radiologists Journal. The articles are identical except for minor stylistic and spelling changes in keeping with each journal’s style.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.