
Abstract
Background:
Delayed graft function (DGF) is associated with an increased risk of graft loss. The use of cold hypothermic machine perfusion (HMP) has been shown to reduce the incidence of DGF in kidney transplant recipients (KTRs), especially when extended-criteria donors (ECDs) are used. HMP can also improve graft survival. However, there is a paucity of data on the determinants of HMP use in clinical practice.
Objective:
We aimed to determine the factors associated with the use of HMP in a cohort of donors and KTRs.
Design:
Multicenter retrospective cohort study.
Setting:
5 transplant centers in Quebec.
Patients:
159 neurologically deceased donors (NDD) and 281 KTR.
Measurements:
Use of HMP.
Methods:
We collected data on consecutive NDD admitted to a dedicated donor unit in a single university-affiliated center and their KTRs between June 2013 and December 2018 in 5 adult transplant centers across the province of Quebec, Canada. All organs were recovered in a single hospital center where a HMP device was available for every organ recovered and the decision to use HMP was left at the discretion of the procurement surgeon. Generalized estimating equations were used to predict the use of HMP.
Results:
The cohort included 159 NDDs and their 281 KTRs. Thirty-three percent of donors were ECDs, and 59% of KTRs received organs placed on HMP. The median cold ischemia time (CIT) was 12.5 (IQR 7.9-16.3) hours. In univariate analysis, none of the donors’ characteristics were associated with the use of HMP. ECD represented 33% of KTR on HMP vs 35% of those not placed on HMP (P = .77). In univariate analysis, the use of HMP was associated with KTR race (non-Caucasian), longer CIT, use of basiliximab/alemtuzumab, year of transplant, and transplant center. The use of HMP varied largely across transplant centers, ranging from 15% to 82%. In multivariate analysis, use of HMP was associated with longer CIT (odds ratio [OR] 1.15, 95% confidence interval [CI] = 1.07-1.25), transplant center as well as transplantations performed after 2013.
Limitations:
One dedicated donor unit including NDD only, absence of specific data on surgeons’ experience and personal or logistic reasons for using or not HMP.
Conclusions:
We found that use of HMP remains low and varies largely across transplant centers. The use of HMP was strongly associated with the transplant center where the surgeons practiced, suggesting that surgeon preference/training plays an important role in determining the use of HMP. Availability of HMP at the time of organ procurement might also be limited by logistic issues such as difficulty in returning the device. Further studies aimed at determining the reasons underlying the barriers precluding the use of HMP could help increasing its use and improve transplant outcomes.
Introduction
Kidney transplantation (KT) is the treatment of choice for patients treated with kidney replacement therapy, offering longer survival and improved quality of life compared to dialysis.1,2 Following KT, delayed graft function (DGF) occurs in up to 30% of patients3-6 and is associated with suboptimal graft function, 7 graft loss,3,8-11 and mortality.3,12,13
The use of hypothermic machine perfusion (HMP) reduces the risk of DGF in kidneys from donation after circulatory determination of death (DCD) and neurologically deceased donors (NDD) with high certainty evidence. 14 The effect is more important when extended-criteria donors (ECD) are used.14-21 In addition, HMP improves graft survival in the first years after transplantation compared with isolated cold storage.18,20,22,23 We also recently confirmed that HMP reduces DGF in Quebec, as shown in other regions. 24 Despite these benefits, HMP is used in 14% to 56% of transplanted kidneys.24-29
There is a paucity of data on the determinants of HMP use in the clinical setting. One study performed more than 10 years ago aimed at demonstrating the cost benefit of HMP. 28 This study showed that use of HMP was associated with donor race, body mass index (BMI), ECD, recipient race, higher human leukocyte antigen (HLA) mismatches, and longer dialysis vintage.
There is a need for a better understanding of the factors that are associated with HMP use so that facilitators and barriers to implementation can be identified. Hence, our aims were to assess the frequency of HMP use and to determine which donor, recipient, or transplant center-level factors are associated with HMP use.
Materials and Methods
Study Design and Population
We performed a retrospective cohort study of consecutive NDD admitted to a dedicated donor unit in a single university-affiliated center where all organs were recovered and their corresponding kidney transplant recipients (KTR) from all 5 transplant centers in the province of Quebec, Canada, between June 2013 and December 2018. This study was initially designed to assess the impact of meeting NDD management goals on DGF. 24 This study used the same database, including all adult NDDs for whom at least one kidney was transplanted. Exclusion criteria were DCD, pediatric KTR, patients transferred outside the province with no follow-up data, and combined organ transplantation with dysfunction of the other organ, for example, a kidney-liver transplantation with acute liver dysfunction.
The province of Quebec has a population of approximately 8.4 million residents who have universal access to health care services. KTR centers are located between 13 and 270 km from the dedicated donor unit. There is no guideline on the use of HMP in Quebec and Transplant Quebec does not oversee its use. In the dedicated donor unit where this study was held, a perfusion machine was made available to the surgical team recovering the organs. The decision to use HMP was left at the discretion of the procurement surgeon. As for kidney transplant centers, each center was responsible to cover the costs associated with the use of HMP at their own location if HMP was not already provided by the dedicated donor unit.
We followed the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines for observational studies. 30 The ethics committees of each institution approved the study (MP-32-2015-1132). Written consent was waived given the retrospective observational nature of the study. The study was performed in accordance with the 1964 Declaration of Helsinki and its later amendments.
Data Collection
The primary outcome was the percentage of organs placed on HMP. Organs were machine-perfused in a cold solution using a Kidney Transporter System® (Organ Recovery Systems, Chicago, IL, USA).
We collected data on kidney donors and recipients, including demographic characteristics, and past medical history. ECD was defined as donor age ≥ 60 years or 50-59 years with 2 of the following: stroke as cause of death, serum creatinine > 1.5 mg/dL (133 µmol/L) or history of hypertension. For donors, occurrence of cardiac arrest, cause of neurological death, laboratory results, and use of HMP were also collected. We calculated the kidney donor risk index (KDRI), which includes donor characteristics to predict allograft survival 31 and converted KDRI, as per convention, to obtain the Kidney Donor Profile Index (KDPI). For KTR, we collected data on transplant center, year of transplant, use of HMP, panel reactive antibody (PRA), cold ischemic time (CIT), and immunosuppressive regimen. We also collected data on DGF status at 1 week, as well as kidney graft function and survival at 6 months.
Statistical Analyses
We used descriptive statistics to summarize characteristics of patients. Continuous variables were described using mean and standard deviation (SD) when the data followed a normal distribution or median and interquartile range (IQR) if skewed. Frequencies and percentages were used for categorical data. We analyzed continuous variables using t-tests or Mann-Whitney tests. We compared categorical variables using χ2-test or Fisher exact test. To account for the cluster effect of paired kidneys from the same donor, we performed multiple logistic regression using generalized estimating equations (GEE). 32 Variables with a P < .05 by univariate analysis were included in the multivariate model which was adjusted for recipient age and sex. Statistical tests were two sided and P < .05 were considered statistically significant. Statistical analyses were performed using SPSS, version 26.0 (IBM, Armonk, NY) and SAS 9.4 software (SAS Institute, Cary, NC, USA).
Results
The study cohort included 159 NDDs and their 281 KTRs (Figure 1). Donor characteristics are presented stratified by HMP use (Table 1). The median age for donors was 53 (37-62) years and almost two-thirds were Caucasian males. ECD represented a third of the cohort. Significant discrepancies in organ quality were observed, as shown by the wide dispersion of KDPI. In univariate analysis, none of the donors’ characteristics were associated with the use of HMP (Table 1). ECD represented 33% of KTR on HMP and 35% of those not placed on HMP (P = .77).

Study population of deceased kidney donors and recipients.
Kidney Transplant Donor and Recipient Characteristics, Stratified by Hypothermic Machine Perfusion Status.

Note. IQR = interquartile range; BMI = body mass index; DND = donor neurological death; KDRI = kidney donor risk index; KDPI = kidney donor profile index; KTR = kidney transplantation recipient.
Between hypothermic machine perfusion and no hypothermic machine perfusion.
KTR characteristics and perioperative management are shown in Table 1, stratified by HMP status. The median CIT was 12.5 (IQR 7.9-16.3) hours. On average, 59% of KTRs received organs placed on HMP and there was fluctuation in the use of HMP over time. The use of HMP varied largely across KTR centers, ranging from 15% to 82% of all transplanted kidneys. A wide variation in the number of KTR performed from kidneys received from our dedicated donor unit was observed across centers, with numbers ranging from 13 to 116 KTR. In univariate analysis, KTR race, CIT, use of basiliximab/alemtuzumab, year of transplant, and transplant center were associated with the use of HMP (Table 1).
In multivariate analysis (Table 2), the use of HMP was associated with longer CIT (odds ratio [OR] 1.15, 95% confidence interval [CI] 1.07-1.25), transplant center, as well as KTR after 2013.
Predictors of Use of Hypothermic Machine Perfusion Using Generalized Estimating Equations (n = 281).
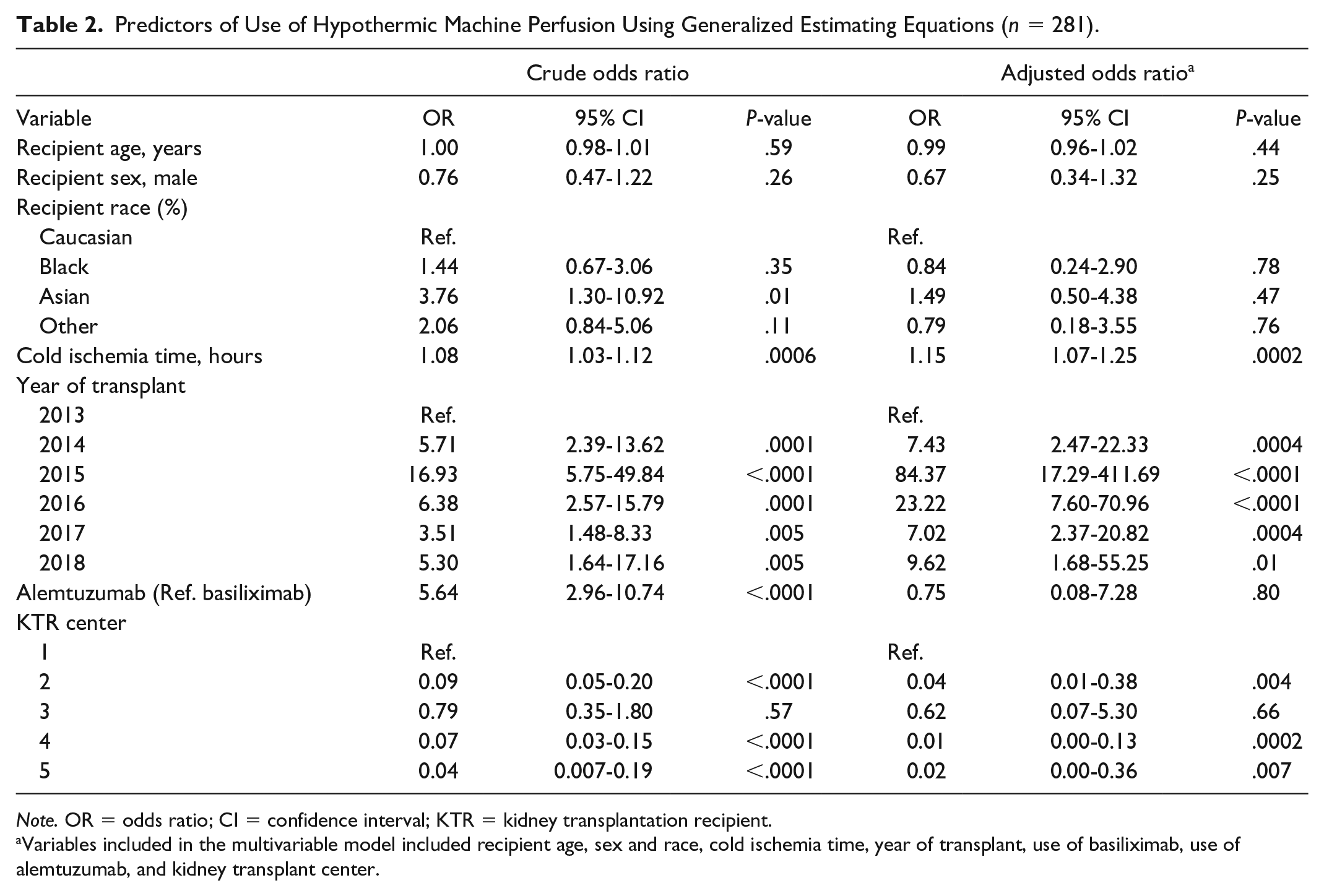
Note. OR = odds ratio; CI = confidence interval; KTR = kidney transplantation recipient.
Variables included in the multivariable model included recipient age, sex and race, cold ischemia time, year of transplant, use of basiliximab, use of alemtuzumab, and kidney transplant center.
In this cohort, as previously demonstrated in a smaller subgroup of KTR of the same cohort, 24 the use of HMP remained associated with a significant decreased risk of DGF (OR 0.53, 95% CI 0.30-0.92). However, the use of HMP was not associated with a higher graft survival rate at 6 months (94% with HMP vs 93% without HMP, P = .86) nor with a better kidney function at the same timepoint (median glomerular filtration rate of 56 mL/min/1.73 m2 with HMP vs 52 mL/min/1.73 m2 without HMP; P = .45).
Discussion
We found that approximately 60% of organs recovered in a dedicated donor unit where a perfusion machine was always made available to surgeons were placed on HMP prior to transplantation. This result is similar to previous findings from the United States and Europe.25-29 In our study, donor characteristics, including ECD status, were not associated with HMP use. The main determinants of HMP use were the transplant centers where surgeons practiced, transplant era and cold ischemia time.
The main finding of our study is that the use of HMP was strongly associated with the center where the surgeons practiced, suggesting that their training or preference plays an important role in determining its use. We explored the reasons for HMP use through personal communications with 1 transplant nephrologist from each of the 5 transplant centers in the province. In 1 center, surgeons considered that HMP use might delay transplantation and preferred avoiding its use. In other centers, some surgeons almost never use HMP, while others use HMP if CIT is expected to be prolonged. In another center, HMP is used for almost all kidney transplantations due to concerns regarding access to the operating room. In addition, the availability of HMP at the time of organ procurement might also be limited by logistical issues such as the difficulty of returning the device to the dedicated donor unit with increasing distance to the transplant center. However, we observed variations in the use of HMP within transplant centers in Montreal, where the dedicated donor unit is located, suggesting that distance between these centers is not the only variable considered in making this decision. To our knowledge, previous studies have not assessed transplant center-level factors associated with the use of HMP.
We also found that the use of HMP was associated with longer CIT. It remains to be determined whether prolonged CIT is a cause and/or consequence of the use of HMP. Similar to our findings, a meta-analysis performed in 2016 reported that the use of machine perfusion is associated with longer CIT (23.4 vs19.5 hours for HMP and cold storage, respectively). 33 A more recent study also reproduced these results. 25 In clinical practice, surgeons might offer HMP for kidneys with prolonged CIT to reduce their risk of DGF. In addition, surgeons might also consider the use of HMP more often in high-volume centers where kidney transplantation is often delayed by another surgery.
While some organ procurement organizations systematically use HMP in ECDs, 26 this may not be feasible in all jurisdictions. For example, procurement surgeons may have limited time to install HMP being busy with another organ transplantation. In the province of Quebec, the surgeons who recover the organs are most often different from the ones who accept the kidney offer and perform the kidney transplantation. While the surgeons transplanting the kidneys have access to ECD status and donor information relevant to kidney quality, the ones recovering the organs may not, especially since the latter may be involved in transplanting nonrenal organs. In the absence of a systematic communication channel between the surgeons recovering and transplanting the kidneys, the opportunity to place the kidney on HMP at procurement can be lost. A more comprehensive assessment and establishing systematic communication between the teams involved in recovering and transplanting the kidneys might be necessary to favor the use of HMP in patients at higher risk of DGF or future graft dysfunction, such as ECDs or those with prolonged CIT.
These findings should be considered in the context of prior research. In our study, the use of HMP was not associated with any of the donors’ characteristics, even in univariate analysis. Recent studies have shown that organs from older donors or those with higher creatinine levels were more likely to receive HMP.25-27,34,35 In our study, ECDs were not more likely to be offered HMP compared with standard criteria donors, despite results from previous studies showing a more pronounced benefit in this population. The absence of systematic communication between recovering and transplant teams or the absence of ODO oversight in the use of HMP may explain these differences. In other provinces, such as Ontario, HMP is systematically used in ECD unless CIT is expected to be short. As for recipient characteristics, we found that easily identifiable factors for DGF such as race and CIT were associated with HMP use in univariate analysis, findings that were also reported by Buchanan and colleagues. 28 However, race was no longer significant in our multivariate model. Others have reported that the use of HMP was associated with donor race, BMI, ECD, recipient race, higher HLA mismatches and longer dialysis vintage time, as well as warm ischemia time,28,34 results that we did not replicate.
Our study has several strengths. We performed a multicenter study including detailed data on the use of HMP and most factors known to be associated with DGF, namely, CIT and ECD. Our study highlights the barriers to the use of HMP in clinical practice despite evidence supporting its beneficial effect on DGF and graft survival. Limitations to our study include its small sample size from 1 dedicated donor unit, which may limit the generalizability of our results. In addition, our study included only NDD, which precludes any conclusion on the use of HMP in DCD in our province. We collected data on transplant centers, but did not capture specific data on surgeons’ experience and personal or logistic reasons for using or not HMP for each transplantation, such as operating room availability or surgeon’s work schedule. As with any observational study, unmeasured confounding between donor characteristics, recipient characteristics, KTR centers, and the use of HMP could have occurred.
Conclusions
This study shows that the use of HMP was only 60% over the study period and varies largely across centers, despite multiple studies showing that its use is associated with better graft survival in the first years after transplantation. The use of HMP was strongly associated with the transplant center where the surgeons practiced, suggesting that surgeon preference or training plays an important role in determining the use of HMP. HMP use may also reflect local conditions at the transplant center such as operating rooms availability. HMP at the time of organ procurement might also be limited by logistic issues such as difficulty in returning the device to the dedicated donor unit. Further studies aimed at determining the reasons underlying the barriers precluding the use of HMP could help increase its use. Guidelines and oversight by a medical/surgical committee at the ODO level may also help physicians deciding when the use of HMP should be prioritized, as is the case in other Canadian provinces.
Footnotes
Acknowledgements
J.B. and H.C. received salary support from the Fonds de la Recherche du Québec–Santé.
Ethics Approval and Consent to Participate
The ethics committees of each institution approved the study (MP-32-2015-1132). Written consent was waived given the retrospective observational nature of the study.
Consent for Publication
All authors have provided consent for publication.
Availability of Data and Materials
The datasets used and/or analyzed for this study are not available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the CNTRP CHUM Astellas Canadian National TRANSPLANT Research Program Research Innovation Grant funded by the Center hospitalier de l’Université de Montréal (CHUM) and Astellas and jointly established by CHUM, Astellas and the Canadian National Transplant Research Program. The funding agencies did not have any role in study design; collection, analysis, and interpretation of data; writing the manuscript and the decision to submit the report for publication.