
Abstract
Background:
Pragmatic cluster randomized trials (CRTs) offer an opportunity to improve health care by answering important questions about the comparative effectiveness of treatments using a trial design that can be embedded in routine care. There is a lack of empirical research that addresses ethical issues generated by pragmatic CRTs in hemodialysis.
Objective:
To identify stakeholder perceptions of ethical issues in pragmatic CRTs conducted in hemodialysis.
Design:
Qualitative study using semi-structured interviews.
Setting:
In-person or telephone interviews with an international group of stakeholders.
Participants:
Stakeholders (clinical investigators, methodologists, ethicists and research ethics committee members, and other knowledge users) who had been involved in the design or conduct of a pragmatic individual patient or cluster randomized trial in hemodialysis, or their role would require them to review and evaluate pragmatic CRTs in hemodialysis.
Methods:
Interviews were conducted in-person or over the telephone and were audio-recorded with consent. Recorded interviews were transcribed verbatim prior to analysis. Transcripts and field notes were analyzed using a thematic analysis approach.
Results:
Sixteen interviews were conducted with 19 individuals. Interviewees were largely drawn from North America (84%) and were predominantly clinical investigators (42%). Six themes were identified in which pragmatic CRTs in hemodialysis raise ethical issues: (1) patients treated with hemodialysis as a vulnerable population, (2) appropriate approaches to informed consent, (3) research burdens, (4) roles and responsibilities of gatekeepers, (5) inequities in access to research, and (6) advocacy for patient-centered research and outcomes.
Limitations:
Participants were largely from North America and did not include research staff, who may have differing perspectives.
Conclusions:
The six themes reflect concerns relating to individual rights, but also the need to consider population-level issues. To date, concerns regarding inequity of access to research and the need for patient-centered research have received less coverage than other, well-known, issues such as consent. Pragmatic CRTs offer a potential approach to address equity concerns and we suggest future ethical analyses and guidance for pragmatic CRTs in hemodialysis embed equity considerations within them. We further note the potential for the co-creation of health data infrastructure with patients which would aid care but also facilitate patient-centered research. These present results will inform planned future guidance in relation to the ethical design and conduct of pragmatic CRTs in hemodialysis.
Trial Registration:
Registration is not applicable as this is a qualitative study.
Introduction
Fewer trials are conducted in nephrology than in any other internal medicine specialty. 1 The trials that have been conducted are limited by poor recruitment, inadequate sample size, nonadherence to the allocated therapy, missing data, and reliance on surrogate outcomes.1-6
The cluster randomized trial (CRT), in which intact groups (such as all patients within a dialysis facility) are randomly allocated to study arms, 7 has been proposed as a potentially useful design that may facilitate the conduct of more pragmatic trials in hemodialysis.8,9 For example, cluster (rather than individual) randomization may better mimic the clinical (“real-world”) context in which treatments will be used, may promote adherence to the intervention due to the universal adoption of an intervention at the site, and may reduce the complexity of allocating multiple individuals within the same facility to differing interventions. 7 Moreover, it may not be possible to evaluate certain interventions in an individually randomized trial due to the mechanism of delivery or logistical infeasibility. When routinely collected data are available for outcome assessment, cluster randomization may facilitate the cost-efficient inclusion of whole clusters, potentially increasing generalizability. 10
However, CRTs may not be appropriate in all circumstances; cluster randomization introduces methodological issues, such as the need for larger sample sizes, due to the fact that outcomes are correlated within clusters, making CRTs statistically less efficient than patient randomized trials. 11 In addition, CRTs are more prone to bias than patient randomized trials. Consequently, there must be a clear justification for the use of a CRT design.12,13
Pragmatic CRTs may also raise ethical challenges, and particularly so in the context of hemodialysis. 7 For example, in a CRT the unit of allocation may be the hospital or dialysis center, the intervention delivered to health professionals, and data are collected from patients. The multi-level nature of the trial may, therefore, complicate questions regarding who are research participants and from whom informed consent is required. 13 Existing research ethics guidelines, developed with explanatory, patient randomized, trials in mind, provide little guidance on such issues 14 and are thus difficult to interpret and apply to pragmatic CRTs.15-17
Furthermore, while guidelines do exist for CRTs broadly, 13 there may be additional challenges when conducting pragmatic CRTs in the hemodialysis context. A recent ethical analysis used the Time to Reduce Mortality in End-Stage Renal Disease (TiME) trial as a case study for a preliminary exploration of ethical issues in pragmatic CRTs in hemodialysis. 7 The authors identified seven key ethical issues: justification of the use of cluster randomization, the adoption of individual-level interventions as local standard of care, the complexity of benefit-harm analyses, the role of gatekeepers and their responsibilities, how informed consent is approached (including the potential for waivers of consent), the role of notification, and the potential inclusion and protection of vulnerable participants.
While empirical research exploring ethical issues in pragmatic trials, and CRTs more broadly, has begun to emerge,18-23 there is a paucity of research with those who are actively involved in the design and conduct of pragmatic CRTs in hemodialysis. The aim of the present study was to address this gap and identify stakeholder perceptions of ethical issues in pragmatic CRTs in hemodialysis.
Methods
We conducted semi-structured interviews with key stakeholders in the design and conduct of pragmatic CRTs in hemodialysis. Potential interviewees were eligible if they had been involved in the design or conduct of a pragmatic individual patient randomized trial or CRT in hemodialysis, or their role would require them to review and evaluate pragmatic CRTs in hemodialysis. These inclusion criteria and sample frame were chosen to ensure that participants would be familiar with pragmatic and cluster trials, compared with clinical trials more generally, and consequently that the identified challenges would be grounded in experience. Patient partners were not included in the present study, but were the subject of a separate study which used a scenario-based group-discussion approach to elicit their perspectives. Given the differences in design and data collection, patient perspectives will be reported elsewhere.
Identification and Recruitment
Participants were identified through a range of sources including (1) our study team’s professional network, (2) a search of the clinicaltrials.gov website to identify principal investigators of ongoing CRTs in hemodialysis, (3) authors of published CRTs or CRT protocols in hemodialysis settings identified from a recent systematic review, 24 (4) publicly available information on funded hemodialysis trials, or (5) other publications discussing pragmatic trials or CRTs in hemodialysis settings. Sampling was not limited by geography or publication year. Only English-speaking participants were eligible.
Sample Size
We purposively sampled individuals to obtain a broad range of perspectives based on role, jurisdiction, and clinical interests in hemodialysis. Based on prior experience, logistical considerations, and likely saturation of themes,25-29 our target sample size was 12 to 20 participants.
Data Collection
Data were collected through semi-structured interviews. The interview guide was informed by prior work on the ethics of CRTs 20 and pragmatic trials, 30 as well as a review of the literature. We piloted the interview guide with members of the team. The interview covered (1) experiences of trials in hemodialysis settings, CRTs, or pragmatic trials; (2) existing ethics resources used (generally) and those which would be valuable for pragmatic CRTs in hemodialysis settings; and (3) specific ethical issues arising from pragmatic CRTs in hemodialysis. Given the semi-structured nature of the interviews, and the differing stakeholder roles, the interview guide was adapted depending on participant role. Novel topics or themes were explored with in-depth questioning. A copy of the interview guide template is provided in Supplementary File 1.
All interviews were conducted by a member of the team (S.G.N.) with experience and training in qualitative research methods. Interviews were conducted either in person or by telephone.
Interviews were audio-recorded with consent; if someone consented to participate but did not wish to be recorded, contemporaneous notes were taken. Audio-recordings were transcribed verbatim by a professional transcription service. Two individuals did not wish to be recorded, and field notes were taken with consent. Transcribed, interviews and field notes were de-identified and interview participants assigned a unique identifier. Participants whose interviews were transcribed were subsequently provided with a copy of their interview transcript, which allowed them to verify its accuracy and provide any additional comments. One participant provided comments on their transcript and these were included within the final documentation for analysis. Final copies of transcribed interviews and field notes were imported into qualitative data analysis software (NVivo 11) 31 to assist with coding.
The study was approved by the Ottawa Health Sciences-Research Ethics Board (Ref: 20180133-01H).
Data Analysis
The examination of the interview transcripts followed a thematic analysis approach.32,33 Initial coding used a codebook developed for a previous study of ethical issues in pragmatic trials 30 which was then expanded in an inductive manner, based on additional issues identified in the transcripts. Issues were then grouped into larger themes organized around a core concept (such as challenges with informed consent). 34 Transcripts were coded by one researcher (S.G.N.) and verified by a second (K.C.). Any discrepancies were discussed until consensus was achieved. Coding was conducted using the constant comparison method to compare and modify themes across interviews.35,36
Results
From 28 invitations, a total of 16 interviews were conducted with 19 individuals (response rate 66%). One interview involved a group of 3 individuals, and another involved 2 individuals. Interviews took place between November 2018 and April 2019. Interviews were 64 minutes in duration on average (range: 31-78 minutes). A total of 14 interviews (involving 17 individuals) were audio-recorded.
Participants’ experience spanned a wide array of trial designs and hemodialysis interventions, including exercise, hemodialysis duration, professional education, and drugs. Most participants were based in North America (16 of 19; 84%), with clinical investigators comprising almost half of the sample (8 of 19; 42%). Eleven interviewees were female (58%). Table 1 provides a description of participant demographics.
Participant Demographics (N = 19).

A common point of discussion, albeit not specific to pragmatic CRTs in hemodialysis, was the need to develop a research culture in nephrology. Participants indicated that many treatments in nephrology are opinion-based or supported by low-quality evidence. Strongly held beliefs regarding treatments supported by low-quality evidence was identified as both a source of variation in practice and an impediment to the conduct of pragmatic CRTs.
Ethical issues raised by pragmatic CRTs in hemodialysis were identified within six themes: (1) patients treated with hemodialysis as a vulnerable population, (2) appropriate approaches to informed consent, (3) research burdens, (4) roles and responsibilities of gatekeepers, (5) inequities in access to research, and (6) advocacy for patient-centered research and outcomes (see Table 2).
Key Themes.
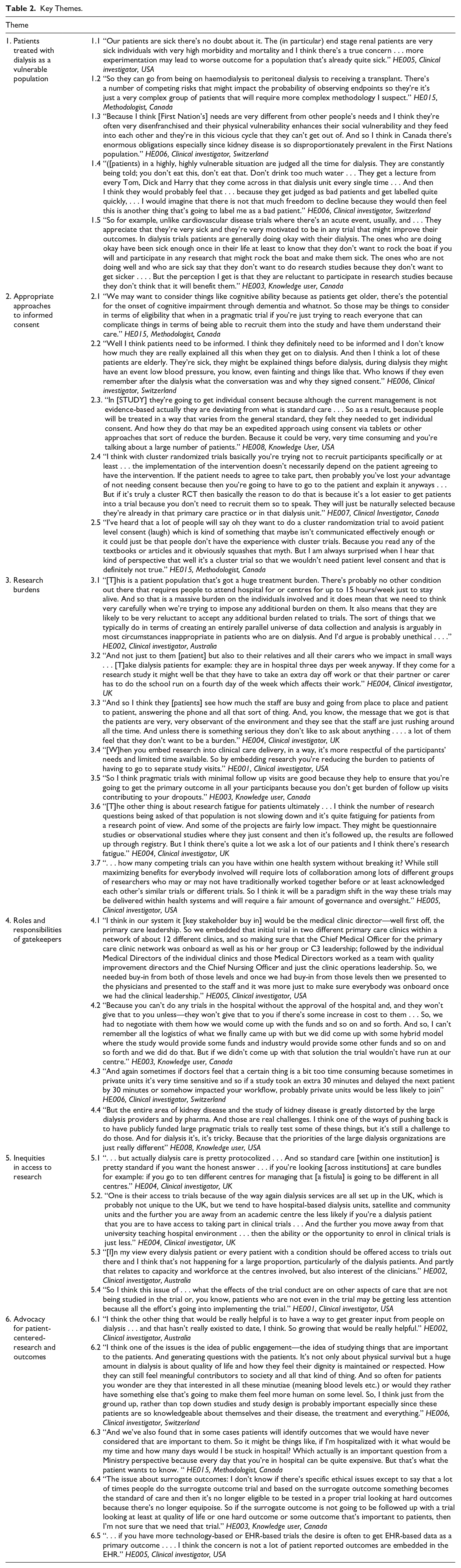
Patients Treated With Hemodialysis as a Vulnerable Population
Participants viewed patients treated with hemodialysis as complex and vulnerable because of co-morbidities and general ill health. In part this was due to the care trajectories that patients receiving hemodialysis experience because of their underlying kidney disease (Quotes 1.1-1.2), as well as care needs due to other health conditions (eg, diabetes, cancer). Several participants indicated that patients may be vulnerable due to cognitive impairment, which is prevalent in patients undergoing hemodialysis treatment. Participants also indicated that some patients receiving hemodialysis, such as Indigenous Peoples, may be vulnerable due to social and system-level factors (Quote 1.3).
Participants noted that patients receiving hemodialysis face constant judgment; they are subject to both clinical and personal evaluation on a regular basis. One participant highlighted how patients are viewed as “good” and “bad” based on their compliance with clinical recommendations. As a result, some participants questioned whether such judgments could lead patients to feeling obligated to participate in research (Quote 1.4).
Others observed how some patients undergoing hemodialysis live in a state of precarious medical stability. Such patients may be reluctant to participate in a trial so as not to disrupt that stability, or as one participant put it, so as not to “rock the boat” (Quote 1.5).
Appropriate Approaches to Informed Consent
Participants questioned when it is appropriate to deviate from written informed consent for participation in pragmatic CRTs. They asked, under what circumstances are different approaches appropriate, and when is the use of a waiver of consent acceptable?
As noted above, participants reported the prevalence of cognitive impairment in the hemodialysis population. This raised concerns about vulnerability, eligibility for research, and ability to provide informed consent (Quote 2.1). Cognitive impairment is an issue for trial eligibility in terms of initial recruitment, but also retention, as incident cases of impairment may occur over the course of the trial. The loss of decision-making capacity was flagged as an issue of concern for continuing informed consent (Quote 2.2).
Factors impacting the perceived need for informed consent included risks of the study intervention, study deviations from routine clinical care, research burdens on patients, as well as the approach to informed consent and its feasibility (Quote 2.3). Some participants associated the use of a CRT with alternate approaches to consent (eg, verbal consent only) or waiver of consent (Quote 2.4), whereas others believed that written informed consent is required (Quote 2.5). Indeed, most participants identified the need for further guidance on informed consent.
Research Burdens
Participants identified the burdens of research participation as an issue for pragmatic CRTs in hemodialysis, noting that trials can pose burdens to patients, family, friends, caregivers, and clinical care staff (Quotes 3.1-3.2). Some commented that additional workload for clinical staff may be a reason for patients to decline research participation (Quote 3.3).
Participants emphasized that design features which are more closely aligned with the clinical care context could reduce system-level burdens (by minimizing organizational and setting-related workload) and patient-level burdens (by not requiring additional visits for follow-up or tests for data collection) (Quotes 3.4-3.5). Making use of routinely collected patient data and samples was one example given to reduce patient burden.
However, participants raised two cautionary notes. First, the widespread adoption of pragmatic CRTs may lead to a higher volume of research and this may impact the capacity of hemodialysis facilities to conduct further research. Second, multiple ongoing trials in a hemodialysis unit may lead to “research fatigue” among patients and health care providers and affect their willingness to participate in research (Quotes 3.6-3.7).
Roles and Responsibilities of Gatekeepers
Participants recognized that various stakeholders act as gatekeepers in pragmatic CRTs, and these gatekeepers facilitate the implementation of the trial. Participants identified clinicians as key gatekeepers insofar as they facilitate the recruitment of patients and the conduct of the trial. Other gatekeepers identified by participants included dialysis center managers, regional managers within health systems, nurses, and allied health professionals (see, for example, Quotes 4.1-4.2). Gatekeeper support was deemed a key predictor of success for a pragmatic CRT.
Pragmatic CRTs conducted in for-profit hemodialysis facilities face additional challenges (Quotes 4.3-4.4). Participants noted in a for-profit dialysis facility there are potential conflicts among the facility’s clinical functions, its responsibilities as a business, and the needs of a trial.
Inequities in Access to Research
While some participants said that within-center clinical care is highly protocolized, others reported substantial variation in care between centers (Quote 5.1). Participants identified equitable access to research as an ethical issue. Both the organization and funding of hemodialysis care were thought to impact access to trial participation. For example, trials may not be as accessible to patients in satellite centers or community settings as they are in academic hospitals (Quotes 5.2-5.3). Other participants questioned whether an ongoing trial could negatively affect nonparticipating patients due to trial demands on resources such as health provider time (Quote 5.4).
Advocacy for Patient-Centered Research and Outcomes
The final theme identified was the need for patient-centered research and the use of patient-centered outcomes. Participants indicated that training and resources to support patient-centered research are needed (Quotes 6.1-6.2).
The importance of patient-relevant outcomes in research was highlighted often by participants (Quote 6.3). Traditional research endpoints, such as mortality, are commonly infeasible in hemodialysis given the timeframe of trials. This has led to the use of surrogate endpoints such as biomarker levels with variable clinical utility. As a result, treatments are often adopted in practice without evidence of impact on patient-relevant outcomes (Quote 6.4).
Another barrier to patient-centered research is that patient-relevant outcomes are not captured in routinely collected data sets (Quote 6.5). To capture patient-centered outcomes, additional efforts may need to be made to collect these directly from patients participating in a pragmatic CRT. However, this is in tension with the pragmatic aim of relying on routinely collected data and using existing staff and data infrastructure for outcome assessment.
Discussion
In the present study, we interviewed a range of stakeholders involved in hemodialysis research to identify ethical issues in pragmatic CRTs. Much of the discussion was prefaced by concerns regarding the lack of high-quality trial evidence, and the potential for strongly held opinions to impede trials. Participants identified six themes: patients being treated with hemodialysis as a vulnerable population, appropriate approaches to informed consent, research burdens, roles and responsibilities of gatekeepers, inequities in access to research, and advocacy for patient-centered research and outcomes.
These findings should be considered within the limitations of the study. First, while the response rate of those invited was almost 70%, the sample was largely drawn from the United States and Canada. While this reflects the geography of completed trials in hemodialysis, almost 85% of the articles in a recent systematic review were from the United States, United Kingdom, or Australia and New Zealand, 24 participants from other countries may have raised additional issues informed by their own regulations and health care systems. Second, the interviews were only conducted in English, and non-English speakers may have contributed additional perspectives. Third, our sample did not include nurses or research coordinators. Given their day-to-day interactions with patients, we believe future studies seeking to further our analyses should include nurses and research coordinators. Finally, no patients or families were included in this study. Given the complexity of the study designs for pragmatic CRTs we adopted a different vignette-based approach to engage patients and this work will be reported separately.
Many of the six themes identified are consistent with previous ethical analyses of pragmatic CRTs in hemodialysis (see Table 3).3,7,37 However, participants identified issues of equity in access to research, and the need for patient-oriented research and patient-centered outcomes, as key themes. These issues have been emphasized to a lesser degree in the literature compared with other themes identified, such as informed consent.
Comparisons of Ethical Issues Raised in Recent Analyses.

The ethical principle of justice requires fair participant selection procedures. Injustice occurs when patients are unduly excluded from research participation, leading to systematic gaps in knowledge and evidence-based treatments. Unlike previous work on the ethics of pragmatic CRTs,3,7,37 our study identified equitable access to pragmatic CRTs as a key ethical issue.
This lack of discussion within previous analyses is surprising given the established literature illustrating that participants recruited to trials testing hemodialysis interventions may not reflect the broader clinical population from which they are drawn38,39 and broader inequities in hemodialysis care.40-42 Notably, patients enrolled in hemodialysis trials have also been found to be younger and have fewer comorbidities than patients in the clinical setting, 43 with many trials systematically excluding patients above the age of 65. 6 The relatively high prevalence of cognitive impairment in patients being treated with hemodialysis presents a special challenge for pragmatic CRTs: there is a need to balance individual rights and respect for persons with social justice concerns and the inclusion of patients normally excluded from trials.7,37,44,45
We believe that equity requires greater efforts to ensure that both trial participants and hemodialysis facilities are representative of the target clinical population and setting for treatments. Going forward, pragmatic CRTs should avoid excluding patients, such as those with comorbidities or lacking decision-making capacity, who would likely receive the treatment in clinical practice. The need to include a broader patient population and diverse hemodialysis facilities is consistent with recent statements by funders to ensure equity considerations in health research. 46
Our study also indicates the perceived need to develop and embed patient-relevant outcomes within pragmatic CRTs in hemodialysis. Participants highlighted the problems associated with the use of surrogate outcomes for mortality due to the cost of trials large enough to detect mortality outcomes. Indeed, the inclusion of patient-relevant outcomes has been low: a recent scoping review found that only 23% of registered randomized controlled trials relevant to dialysis addressed an important research topic as established by a priority setting partnership, 47 and only 16% of the trials assessed clinical outcomes as part of the primary outcome of the study.
This highlights the need for the creation of networks of hemodialysis facilities that can serve as a platform for large, pragmatic CRTs. The feasibility of pragmatic CRTs may be further enhanced by making use of routinely collected clinical data and reducing the need for dedicated research personnel. Second, the identification of other patient-relevant outcomes in hemodialysis trials is a key priority. Patient outcomes are beginning to receive attention in the literature 48 and recent efforts to standardize outcomes for nephrology trials have included patients, family members, and other caregivers. 49 Other examples include work by BC Renal Agency 50 and Ontario Renal Network 51 and through which the Edmonton Symptom Assessment Scale (ESAS) (known as My Symptom Checklist) is reported and recorded in routine care.
Despite this, few studies in nephrology report patient engagement and there is a lack of experience and knowledge about how to engage patients. 52 A lack of awareness and resources have been identified as key barriers to greater patient involvement in kidney research. 53 We suggest that the co-creation of health data infrastructure with patients is essential to patient-centered research and the capture of patient-centered outcomes. Furthermore, we advocate for the active dissemination of best practices, the development of tools, 53 and continued investment in initiatives such as Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD) 54 (Canada) and the Kidney Patient Involvement Network53,55 (UK).
Finally, we note that our study failed to identify some ethical issues reported by other publications. Discussion of methodological aspects of CRTs was notably lacking in our study. Participants did not discuss the need to justify cluster randomization or controversies in the adoption of individual-level interventions as the local standard of care.7,37,56 The analyses by Dember et al and Goldstein et al, both used the TiME trial 57 as a case study, and this may have shaped their findings. In the present study, individuals drew upon their own experiences with a range of different trials, which included a variety of interventions that differed from the TiME trial intervention (see Table 3 for a comparison of issues raised).
Conclusions
The treatment of patients who require hemodialysis lacks an adequate evidence base and further research is urgently needed. Pragmatic CRTs offer a methodological approach to address these concerns. However, if such trials are to proceed ethically a variety of ethical issues must be addressed, including patient vulnerability; appropriate informed consent; the burdens of research on patients, families, and clinical staff; and gatekeeper roles and responsibilities. Our study highlights that greater attention needs to be paid to inequities within research and the ongoing need to advocate and provide resources for patient-centered research and outcomes.
Supplemental Material
Supplementary_Material_CJKHD – Supplemental material for Ethical Issues in the Design and Conduct of Pragmatic Cluster Randomized Trials in Hemodialysis Care: An Interview Study With Key Stakeholders
Supplemental material, Supplementary_Material_CJKHD for Ethical Issues in the Design and Conduct of Pragmatic Cluster Randomized Trials in Hemodialysis Care: An Interview Study With Key Stakeholders by Stuart G. Nicholls, Kelly Carroll, Charles Weijer, Cory E. Goldstein, Jamie Brehaut, Manish M. Sood, Ahmed Al-Jaishi, Erika Basile, Jeremy M. Grimshaw, Amit X. Garg and Monica Taljaard in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We would like to thank the interviewees who agreed to take part.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Ottawa Health Sciences Research Ethics Board (REF: 20170435-01H) and all individuals provided informed consent to participate in the study.
Consent for Publication
All authors have approved the manuscript for publication.
Availability of Data and Materials
The data sets generated and/or analyzed during the current study are not publicly available due potential identifiability.
Author Contributions
M.T., C.W., J.M.G., and A.X.G. conceived the project idea and co-led the funding application. S.G.N., K.C., M.T., J.C.B., C.W., C.E.G., E.B., M.S. developed the interview guide and E.B., M.S., A.A-J., A.X.G., J.M.G., C.W., and M.T. facilitated recruitment. S.G.N. conducted the interviews. S.G.N. and K.C. conducted the analysis. S.G.N. wrote the initial draft of the manuscript with input from M.T. and K.C. S.G.N., K.C., C.W., C.E.G., J.C.B., M.S., A.A-J., E.B., J.M.G., A.X.G., M.T. all contributed critical revisions and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.W. receives consulting income from Cardialen, Eli Lilly & Company, and Research Triangle Institute (RTI) International.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the SPOR Innovative Clinical Trial Multi-Year Grant, “An Integrated Platform for Innovative Pragmatic Cluster-Randomized Registry Trials in Hemodialysis” provided by the Canadian Institutes of Health Research (CIHR) (competitive, peer-reviewed). J.M.G. holds a Canada Research Chair in Health Knowledge Transfer and Uptake. AXG is supported by the Dr. Adam Linton Chair in Kidney Health Analytics and a Clinician Investigator Award from the Canadian Institutes of Health Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.