
Abstract
Background:
Despite decades of investigation, the balance of clinical risks and benefits of fluid supplementation with starch remain unresolved. Patient-centered outcomes have not been well explored in a “real-world” trial in cardiac surgery.
Objective:
We sought to compare a starch-based fluid strategy with a saline-based fluid strategy in the cardiac surgery patient.
Design:
A pragmatic blinded randomized controlled trial comparing starch-based with saline-based fluid strategy.
Setting:
A large tertiary academic center in London Ontario between September 2009 and February 2011.
Participants:
Patients undergoing planned, isolated coronary revascularization.
Measurements:
Serum creatinine and patient weight were measured daily postoperatively.
Methods:
Patients were randomized to receive 6% hydroxyethyl starch (Voluven) or saline for perioperative fluid requirements. Fluid administration was not protocolized. Co-primary outcomes were incidence of acute kidney injury (AKI) and maximum postoperative weight gain. Secondary outcomes included bleeding, transfusion, inotropic and ventilator support, and fluid utilization.
Results:
The study was prematurely terminated due to resource limitations. A total of 69 patients (19% female, mean age = 65) were randomized. Using RIFLE criteria for AKI, “risk” occurred in 12 patients in each group (risk ratio [RR] = 1.0; 95% confidence interval [CI] = 0.5-1.9; P = 1.00), whereas “injury” occurred in 7 of 35 (20%) and 3 of 34 (9%) of patients in the starch and saline groups, respectively (RR = 2.3; 95% CI = 0.6-8.1; P = .31). Maximum weight gain, bleeding and blood product usage, and overall fluid requirement were similar between groups.
Limitations:
The study had to be prematurely terminated due to resource limitations which led to a small sample size which was not sufficiently powered to detect a difference in the primary outcomes.
Conclusions:
This pragmatic double-blinded randomized controlled trial revealed a number of interesting hypothesis-generating trends and confirmed the feasibility of undertaking a logistically complex trial in a pragmatic fashion.
Introduction
In the context of intravenous volume therapy, the crystalloid vs colloid debate remains unresolved despite decades of investigation and vigorous argument. A number of human and animal studies support the use of colloids indicating improved microcirculatory perfusion and tissue oxygen tension, reduced inflammatory response, and endothelial activation.1-3 A number of studies support the use of crystalloids indicating a lack of incremental benefit for the greater cost of colloids and a potentially increased adverse effect profile of synthetic colloid use, which may include pruritus, coagulopathy, increased blood product transfusion, anaphylaxis, and end-organ dysfunction in some patient groups.4-9
The use of hydroxyethyl starches (HES) in patients with severe sepsis is not recommended or routinely used due to an increased risk of renal dysfunction and death,10-12 as well as an increased risk of bleeding and renal dysfunction when applied to the general intensive care population13-15; however, there is less definitive evidence in the surgical setting.
In the postcardiac surgery population, there is some evidence of decreased duration of inotropic support and less infectious complications following cardiac surgery with the use of HES in a highly protocolized nurse-administered fluid infusion algorithm using invasive monitoring.16,17 In addition, the use of lower molecular weight HES has been associated with fewer bleeding side effects than older generation HES15,16; however, the evidence surrounding its effect on renal function postcardiac surgery have been mixed.16-18 The Starch or Saline After Cardiac Surgery (SSACS) trial is a pragmatic clinician-driven colloid vs crystalloid fluid strategy in the cardiac surgical patient population which seeks to add to this body of literature. We hypothesized that there could be some reduction in renal dysfunction due to improved tissue perfusion and attenuation of weight gain with the use of a synthetic colloid strategy following routine cardiac surgery.
Materials and Methods
Patients
Consecutive consenting patients meeting inclusion criteria were randomized to either the starch (Voluven: 6% HES 130/0.4 in 0.9% saline) or the saline (0.9% saline) group. We included adult patients undergoing primary isolated coronary bypass surgery. For logistical reasons, we excluded those requiring emergent or salvage procedures, defined as those not on the planned daytime operating room schedule. Dialysis patients, and those with acute or chronic preoperative renal failure, defined by a serum creatinine above 180 µmol/L, were excluded. Those with a preoperative metabolic acidosis, defined by a preoperative capillary or arterial blood pH less than or equal to 7.2 and a serum bicarbonate less than 15, were excluded given the potential for developing hyperchloremic acidosis with normal saline. Pregnant patients, patients with active intracranial bleeding, and those with a history of hypersensitivity to starch solutions were also excluded.
Protocol
Computer randomization in blocks of 4 patients, stratified into high-risk and low-risk subgroups, was done by the clinical trials pharmacy at London Health Sciences Centre. The high-risk stratum required the presence of one or more of the following: age >70, diabetes mellitus requiring oral hypoglycemic medications or insulin, preoperative serum albumin <25 g/L, grade III or IV left ventricle (ejection fraction < 35%), or baseline chronic kidney disease stage G3a or greater (estimated glomerular filtration rate [eGFR] < 60 mL/min/1.73 m2). These risk factors were chosen based on validated risk scores for the prediction of acute kidney injury (AKI) after cardiac surgery.19-22 Double-blinded status was ensured by having all solutions repackaged by pharmacy into 250- and 500-mL aliquots, which were labeled only with the patient number and study information, and followed patients throughout the intervention period in a bin that stayed by the patient’s bedside.
Study fluid was started intraoperatively for all intravenous fluid needs except for crystalloid required for the administration of medications. The cardiopulmonary bypass machine prime solution consisted of 500 mL study fluid, with the remainder of the prime being crystalloid. Postoperative volume boluses to support the circulation were as per assigned group, while all maintenance fluid and medication carrier fluid were crystalloid. Fluid use was not mandated or protocolized, but was left to the treating clinicians’ discretion as guided by measurements of central volume and cardiac function such as central venous catheter, point-of-care ultrasound, echocardiography, and chest radiography, in addition to clinical examination. Maximum study fluid usage was 50 mL/kg/d, after which the treating clinician selected a non-starch solution strategy.
The study intervention period terminated at postoperative day 7 or hospital discharge, whichever occurred first. Data collection continued until hospital discharge.
Analysis
Co-primary end points were as follows: (1) incidence of renal dysfunction as defined by achievement or escalation of RIFLE categorization as defined either by estimated glomerular filtration rate eGFR criteria or urine output criteria at any time during the study period 23 and (2) maximum weight gain in kilograms as measured on postoperative days 2, 4, and at discharge (or postoperative day 7 if occurred first) compared with preoperative baseline weight. Secondary outcomes included duration of inotropic or vasopressor support, duration of mechanical ventilation, chest tube drainage, blood product usage, and lengths of stay in the intensive care unit and the acute care hospital. A comparison of the incidence of a composite outcome comprised 10 major postoperative complications (death, stroke, myocardial infarction, prolonged intubation, arrest/arrhythmia, intra-aortic balloon pump placement, renal insufficiency, septicemia, mediastinitis, and reoperation for bleeding) was also planned.
The calculated sample size of 150 patients per group was sufficient to detect an absolute 12.5% decrease in the incidence of renal dysfunction from a baseline incidence of 25% (using an alpha error of .05 and a beta error of .2). Standard descriptive statistics were used for preoperative demographic characteristics. Normally distributed continuous variables were compared between groups using Student t test; non-normally distributed continuous variables were compared using the Mann-Whitney test; categorical variables were compared using Fisher exact test. Results are reported on an intent-to-treat basis.
Results
Of 1002 patients meeting our inclusion criteria during the pilot study enrolment period from September 2009 to February 2011, 81 patients were approached. The low screen ratio was due to inadequate research associate time or patient enrolment in competing studies. Three patients declined participation, and 9 were not randomized due to newly identified exclusion criteria or logistical reasons.
The study was terminated before the anticipated number of patients were randomized due to resource constraints, leaving 35 patients in the starch group and 34 patients in the saline group. Figure 1 depicts patient flow, and baseline demographic characteristics by treatment group assignment are found in Table 1.
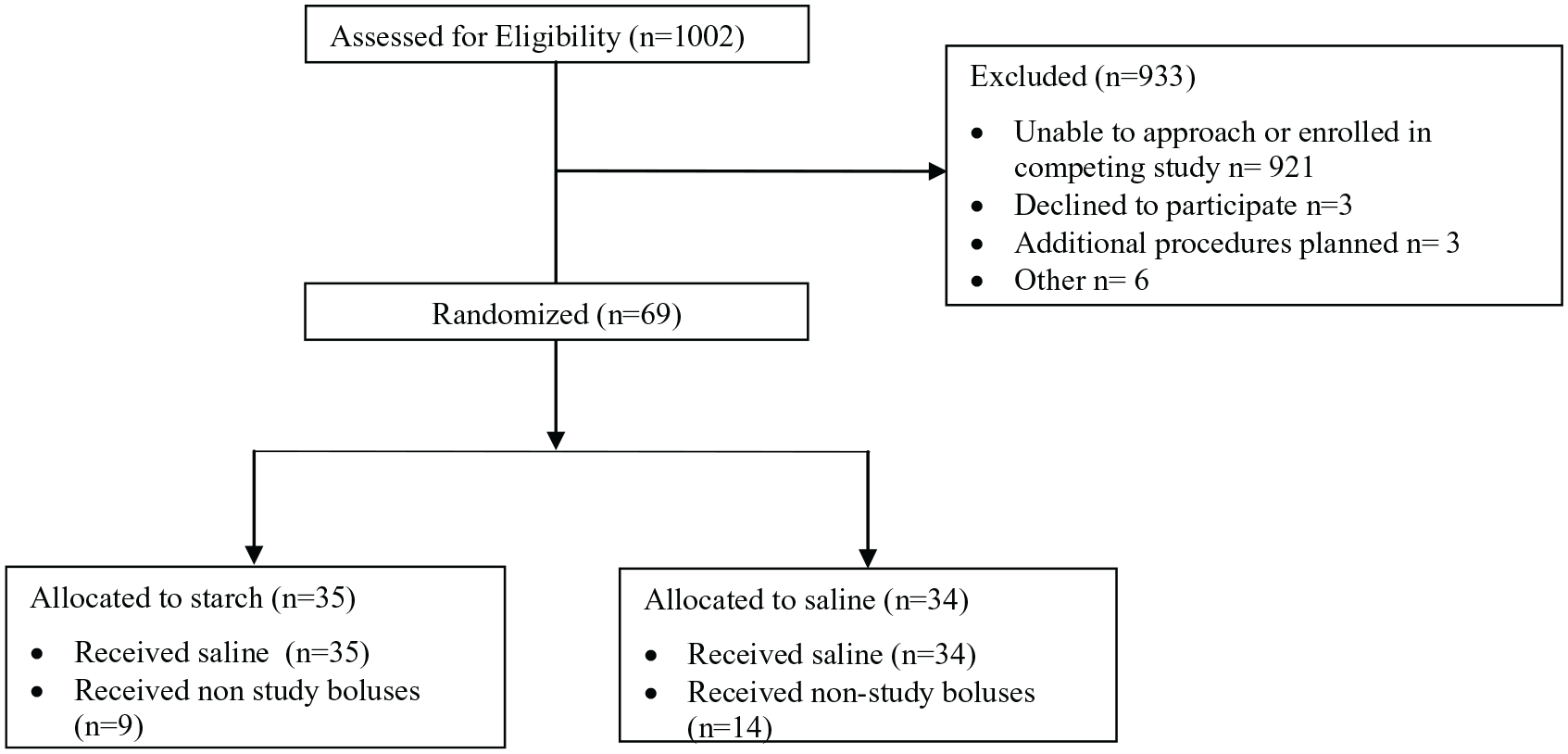
Patient flow diagram.
Demographic Characteristics.
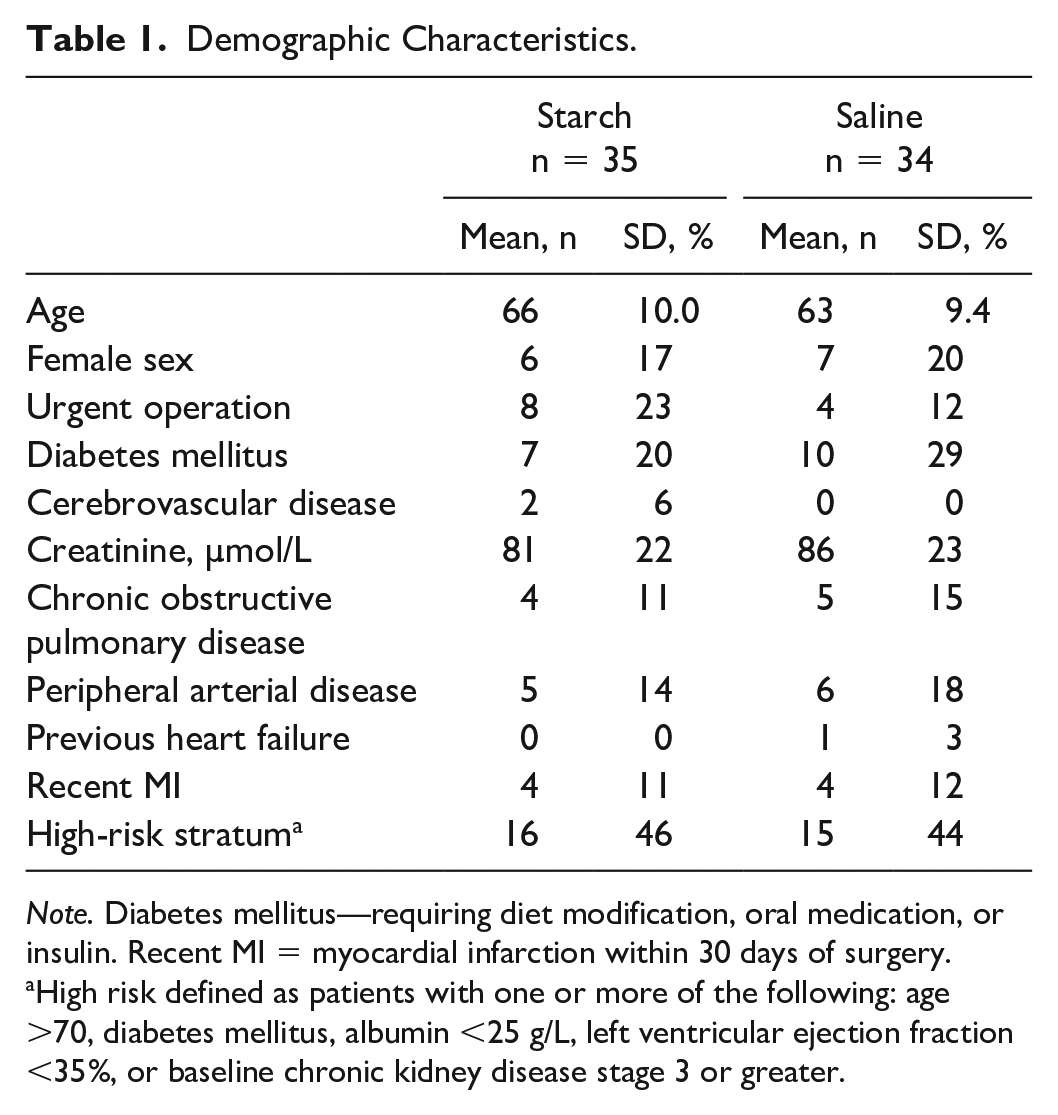
Note. Diabetes mellitus—requiring diet modification, oral medication, or insulin. Recent MI = myocardial infarction within 30 days of surgery.
High risk defined as patients with one or more of the following: age >70, diabetes mellitus, albumin <25 g/L, left ventricular ejection fraction <35%, or baseline chronic kidney disease stage 3 or greater.
Primary Outcomes
Any new postoperative kidney dysfunction by RIFLE criteria was seen in 20 of 35 (57%) patients in the starch group and 15 of 34 (44%) in the saline group. Neither the total incidence of AKI nor comparison of each criterion was significantly different between treatment groups. Maximum postoperative weight gain was similar between groups.
Secondary Outcomes
We did not detect a difference in inotropic or vasopressor requirements between treatment groups, with 8 of 35 (23%) starch patients and 6 of 34 (18%) saline patients requiring more than 4 hours of these medications postoperatively (risk ratio [RR] = 1.3; 95% confidence interval [CI] = 0.5-3.3; P = .77). The median (interquartile range [IQR]) time of mechanical ventilatory support was 5.9 (IQR: 5-8) hours vs 6.6 (IQR: 4-8) hours (P = .54) for the starch and saline groups, respectively. No patients required re-intubation. The median time required in the cardiac surgery intensive care unit was also similar between groups at 15.9 (IQR: 14-21) hours vs 17.0 (14-20) hours (P = .86).
Most departures from protocol were due to unawareness of the study protocol by some clinicians involved in the care of these complex patients, resulting in administration of non-study fluid boluses. Fourteen patients in the saline group received non-study fluid boluses: 8 due to clinician unawareness, and 6 after reaching the maximum daily allotment of study fluid. Of 9 patients in the starch group who received non-study fluid boluses, 5 were due to clinician unawareness, 2 were due to exceeding the daily study fluid allotment, and 2 for undocumented reasons.
Postoperative morbidity and mortality included 1 death and 1 myocardial infarction in the starch group and 1 stroke in the saline group. Atrial fibrillation lasting at least 30 seconds, and requiring treatment with an anti-arrhythmic or anticoagulation medication was seen in 4 of 35 patients (11%) in the starch group and 6 of 34 patients (18%) in the saline group (P = .51). The nadir and timing of anemia was more pronounced and earlier in the starch group, but bleeding and blood product use was similar between the groups, as seen in Table 2. The incidence of our composite outcome was 2 of 35 patients (6%) in the starch group and 1 of 34 patient (3%) in the saline group (P=1.0). The median (IQR) hospital length of stay was 6 (5-8) days and 6 (4-7) days in the starch and saline groups, respectively (P = .40).
Outcomes.

Note. POD = postoperative day number; PRBC = packed red blood cells.
Statistical test:
Fisher exact test.
Student t test.
Discussion
In this pragmatic randomized controlled trial of starch and saline solutions, we found no significant difference in rates of postoperative AKI or weight gain in patients after cardiac surgery. Although the list of investigations and reviews leaning against the routine use of colloids in general critically ill and septic patients continues to grow,4,13,24-26 there remains some equipoise regarding the role of colloids in surgical patients. Cardiac surgery patients in particular require significant amounts of fluid in the perioperative period, and thus there is a need to critically evaluate the risks and benefits of using colloids in this population. While previous trials comparing starch and saline have shown some potential benefit of HES, they have relied on highly protocolized administration, 27 which does not approximate the real-world use of these products.
The SSACS represented a pragmatic randomized controlled trial of starch and saline fluid strategies in coronary artery bypass graft patients which specifically examined adverse renal outcomes. Although the trial was terminated before the expected number of patients were recruited due to resource constraints, it is nonetheless important to present the results of all clinical trials. 28 This trial demonstrated the feasibility of undertaking a logistically complex trial in a pragmatic fashion, and, although it was underpowered to answer the intended research question, represents an important contribution to the larger body of evidence surrounding colloid use.
In this light, notwithstanding the limited sample size, a number of cautious observations can be made. First, the incidence of AKI by any RIFLE criteria was 57% in the starch group and 44% in the saline group. This is a higher incidence than previously reported for isolated Coronary Artery Bypass Grafting (CABG)29,30 because we used RIFLE urine output criteria in addition to the serum creatinine criteria. Although AKI achieving any RIFLE categorization by serum creatinine criteria has been linked with worse outcomes, 29 it remains debatable whether achievement of a RIFLE category by urine output criteria alone is also a risk factor for poor long-term outcomes. There was no difference in the incidence of AKI between fluid groups, which is consistent with previous literature showing no increased risk of AKI with starch-containing solutions compared with crystalloids in postsurgical patients; however, this must be taken in context of the relatively small sample size.13,17
Second, postoperative anemia was more pronounced and was seen earlier (average nadir hemoglobin 80, median day 0) in the starch group as noted in Table 2. This may have been dilutional anemia due to a higher volume of starch solution staying in the intravascular space. 31 This contention is supported by the fact that we did not find any increase in postoperative bleeding as measured by chest tube losses or increased transfusion requirements (as has been seen with older generation starch products). 30 This is consistent with a previous investigation showing a decreased bleeding risk associated with newer starch solutions when compared with older larger molecular weight varieties. 18 The milder, later anemia (average nadir hemoglobin 90, median day 3) in the saline group could be explained by gradual mobilization of fluid back to the intravascular compartment 48 to 72 hours postoperatively.
We did not observe a difference in total fluid requirement between groups, nor did we observe a difference in maximum postoperative weight gain. Although physiological data and some unblinded clinical trials would predict a lower total resuscitative fluid volume when using colloids,29,31,32 in practice, blinded randomized controlled trials have shown a minimal fluid-sparing benefit with the colloid to crystalloid ratio ranging from 1:1.2 to 1:1.4.14,17,24 This is far from the theoretical ratio of 1:3, 33 showing that the theoretical advantage of fluid sparing with the use of colloids is in fact not borne out in reality. This may have important implications, as volume excess and weight gain have been associated with adverse outcomes in a variety of surgical populations.32-34
The major limitation of this work was our inability to carry the trial to completion. The limited number of patients randomized limited the ability to detect smaller effect sizes. Nevertheless, we anticipate these data will be useful for inclusion into systematic reviews. Another limitation was the administration of non-study fluid boluses by clinicians who may not have been aware of the study protocol, an occurrence which would tend to bias toward the null hypothesis. These limitations notwithstanding, this study has the strength of being randomized, and unlike other trials, the intervention solutions were blinded from clinicians, nurses, and research staff, and patient assignments remained concealed during the analysis.
Conclusions
Although early termination of this pragmatic randomized controlled trial comparing 6% HES 130/0.4 with normal saline bolus administration following surgical revascularization was necessitated due to resource constraints, we found a number of interesting trends with respect to postoperative renal function, fluid balance, and anemia. Importantly, we confirmed the feasibility of undertaking a logistically complex trial in a pragmatic fashion, which would have improved translation of results to daily clinical practice. The data from this blinded, randomized trial should be included in future systematic reviews and meta-analyses to improve the estimate of benefit or harm, if any, of starch compared with saline for fluid resuscitation in this cardiac surgical population.
At the current time, we do not recommend routine use of HES over crystalloid solutions for intravenous boluses following coronary artery bypass surgery, but further study to better delineate the risks and benefits of starch solutions in the postcardiac surgery setting may be warranted.
Footnotes
Acknowledgements
The Data Monitoring Committee was comprised by Dr Martin Goldbach, Dr Daniel Bainbridge, Ms Janet Martin, Dr Davy Cheng, and Dr Ron Butler. The investigators would like to thank London Health Sciences Centre Cardiac Anesthetists, Clinical Perfusionists and Jim MacDonald, Clinical Trials Pharmacists, and Cardiac Surgeons Dr Neil McKenzie, Dr Martin Goldbach, Dr Mary Lee Myers, Dr Mackenzie Quantz, Dr Bob Kiaii, and Dr Micheal Chu for their support, involvement, and participation.
Ethics Approval and Consent to Participate
The London Health Sciences Centre/University of Western Ontario Research Ethics Board approved the study protocol and documentation after a full board review. Written consent was obtained from each study participant.
Consent for Publication
All authors consented to the publication of this manuscript.
Availability of Data and Materials
De-identified patient-level and aggregate data are available for future research use by contacting the corresponding author with institutional research ethics board–approved protocols.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this trial was awarded by the Department of Anesthesia & Perioperative Medicine at the University of Western Ontario Internal Research Fund. Research associate human resources were provided by the Division of Cardiac Surgery at London Health Sciences Centre. Aside from providing these supports, the Departments had no role in any aspect of the study, analysis, or reporting of data. This work was supported by the Department of Anesthesia & Perioperative Medicine at the University of Western Ontario Internal Research Fund.
Clinicaltrials.gov ID
NCT00964015