
Abstract
Background:
People undergoing chronic dialysis are at an increased risk of active tuberculosis (TB). In 2012, the Canadian province of British Columbia began systematically screening people initiating dialysis for latent TB using interferon-gamma release assay (IGRA), and treating when appropriate.
Objective:
The objective of this study was to compare active TB rate in people who initiated dialysis and were screened using an IGRA compared with those not screened during the same period.
Design:
Retrospective cohort study.
Setting:
British Columbia (BC), a Canadian province of 5.0 million people with an active TB incidence of 5.1 per 100 000 population.
Participants:
All people in BC who initiated at least 90 days of dialysis between January 2012 and May 2017 were included in the study. People were excluded if they were <18 years of age or had a prior history of active TB diagnosis or treatment for latent TB.
Methods:
A retrospective cohort was created of British Columbians who initiated dialysis between 2012 and 2017. Individuals were stratified into a screened and nonscreened group. Multivariable Cox regression was used to determine the association between latent TB screening and the development of active TB. The primary outcome was incident active TB, either microbiologically confirmed or clinically diagnosed.
Results:
Of the 3190 people included in the study, 1790 (56.1%) were screened, of which 152 (8.5%) initiated latent TB treatment postscreening. During follow-up, incident active TB was diagnosed in 6 (0.3%) of the 1790 people screened, compared with 11 (0.8%) of the 1400 people who received no screening. In multivariable analysis, latent TB screening and treatment was associated with a significant reduction in the rate of active TB (adjusted hazard ratio = 0.3, 95% confidence interval = 0.1-0.8; P < .01).
Limitations:
This was an observational retrospective study and the potential for unmeasured confounding should be carefully assessed.
Conclusions:
These findings suggest that systematically screening and treating people initiating dialysis can significantly decrease the rate of active TB in this high-risk population. Given the importance of screening high-risk groups, the results from this analysis could inform scale-up of TB screening in dialysis programs in other low incidence regions. Trial registration is not applicable as this was a retrospective cohort analysis and not a randomized trial.
Introduction
Tuberculosis (TB) is the leading cause of death from a single infectious disease agent worldwide, ranking higher than HIV. 1 The World Health Organization (WHO) estimates that in 2018, more than 10 million people were affected by active TB, resulting in an estimated 1.2 million deaths. 1 In response to this public health emergency, WHO introduced the EndTB Strategy which aims to reduce the global TB burden by approximately 90% from 2015 to 2035. 2 In countries with a low TB incidence, such as Canada and the United States, this translates to an incidence of <1 case per million persons. 3 In the absence of new technologies such as effective vaccine, innovative programs that systematically screen and treat latent TB (defined as a stated of persistent immune response to Mycobacterium tuberculosis antigens in the absence of clinical symptoms) 4 in high-risk groups will be essential for reaching these TB elimination targets.
People with chronic kidney disease (CKD) requiring dialysis are at high risk of progressing from latent to active disease. 5 In this population, rates of active TB have been estimated to be up 10 times higher than in the general population. 5 This increased risk appears to be related to the impaired cellular immunity that people with CKD experience and is further compounded by comorbid conditions such as diabetes and demographic factors such as age.6-8 To reduce the risk of active TB in this specific population, in 2012, the Canadian province of British Columbia (BC) began systematically screening and treating when appropriate, all people in the province initiating chronic dialysis for latent TB using interferon-gamma release assay (IGRA). While program rollout began in 2012, full provincial implementation was not complete until late 2016. Prior to 2012, there was no systematic TB screening for people initiating dialysis in BC, and screening and treatment practices varied across the province.
In this study, we sought to take advantage of the gradual rollout and evaluate the effectiveness of systematic latent TB screening and treatment in people initiating dialysis, by comparing the rate of active TB in people who initiated dialysis and underwent latent TB screening with an IGRA to those not screened during the same period.
Methods
Data Source
We performed a retrospective cohort study examining the effectiveness of a systematic latent TB screening and treatment program for people initiating dialysis in British Columbia, Canada. This study was approved by the University of British Columbia Research Ethics Board (H14-01977).
Demographic and clinical data on people initiating dialysis in BC were extracted from the Patient Outcome and Management Information System (PROMIS), which is maintained by BC Renal. 9 BC Renal is a government organization that coordinates, monitors, and funds the delivery of care to people with CKD within BC. PROMIS is an obligatory, prospective database that captures real-time demographic and procedural data for all people in BC who are undergoing dialysis.
Information about active and latent TB diagnosis and treatment was obtained from the BC Provincial TB Registry housed at the BC Centre for Disease Control (BCCDC). 10 The BCCDC is the centralized public health agency that is responsible for the diagnosis and treatment of most of the people diagnosed with active and latent TB in BC. The Provincial TB Registry includes diagnostic and treatment data for all people in BC diagnosed with active TB. Mandatory notification by public health partners and routine reporting from the centralized provincial mycobacteriology laboratory and provincial pharmacy make the active TB registry virtually complete.
Receipt of IGRA was assessed using data from the Sunquest Laboratory Information System, which is maintained by the BCCDC Public Health Laboratory. The BCCDC Public Health Laboratory began IGRA screening in select high TB risk groups in 2009 and received funding for IGRA testing in people initiating dialysis as part of this systematic screening program.
Study Population
From PROMIS, we extracted a retrospective cohort of all people in BC ≥18 years of age, who initiated at least 90 days of hemodialysis or peritoneal dialysis between January 1, 2012 and May 31, 2017. The TB and IGRA data were linked from the TB Registry and the Sunquest Laboratory Information System, respectively, using Personal Health Numbers (PHNs), which are unique lifetime identifiers assigned to BC residents. People without a PHN (ie, non-BC residents) were excluded from analysis as their data could not be linked. People with a history of active TB diagnosis or latent TB treatment prior to dialysis initiation were also excluded as they would not be eligible to receive an IGRA.
Exposure
We defined people who received an IGRA (either a QuantiFERON TB Assay or TB T-Spot Assay) within 365 days of dialysis initiation, regardless of previous tuberculin skin test (TST) history, as being screened. People who had no history of TST or IGRA were classified as not being screened. People who received an IGRA at any point outside of the 365-day screening window or only received a TST at any time point were excluded from the primary analysis but included in subsequent sensitivity analyses, as detailed below.
Outcomes
The primary outcome was defined as the first episode of any form of active TB notified in the TB Registry, either microbiologically confirmed or clinically diagnosed. The diagnosis and clinical information of all people diagnosed with active TB were verified by reviewing individual medical records. Other outcomes of interest included the number of people who initiated latent TB treatment after dialysis initiation and the time interval between dialysis initiation and active TB diagnosis.
Statistical Approach
The date of dialysis initiation was set as the index date and person-time was collected until the date of incident active TB diagnosis, death, transfer out of province, or date of data extraction (December 12, 2018), whichever came first.
Descriptive statistics were used to compare the demographic and clinical characteristics of people who were or were not screened with IGRA. Incidence rates for active TB were calculated per 1000 person-years with 95% confidence intervals (CIs) based on a Poisson distribution. Multivariable Cox proportional hazards regression was used to determine the association between the IGRA screening process and active TB. We measured and adjusted for several covariates, extracted from PROMIS, that are known to increase the risk of active TB in the dialysis population: ethnicity, age at dialysis initiation, and comorbid conditions at the time of referral to BC Renal. A complete list of comorbid conditions included is shown in Table 1 of the Supplementary Appendix. In the model, ethnicity was coded as either white or nonwhite to account for low cell counts in certain ethnic subgroups. The Schoenfeld residuals test was used to assess the proportional hazards assumption.
Baseline Demographic and Clinical Characteristics of Individuals Included in the Study, by Screening Category.

Note. Values are counts (%), unless otherwise noted; Q = quartile.
Immune-suppressing conditions defined as transplant prior to dialysis start date, rheumatoid arthritis, systemic lupus erythematosus, Wegener’s granulomatosis, inflammatory bowel disease, polyarthritis nodosa, renal limited vasculitis, Goodpasture’s syndrome, Henoch-Schönlein purpura, progressive systemic sclerosis, Sjogren’s syndrome, cryoglobulinaemia Takayasu’s arteritis, Kawasaki disease, systemic vasculitis secondary to drugs, or any other connective tissue disease as defined by BC Renal.
To assess the reliability of our findings, we performed a series of sensitivity analyses that were defined a priori. First, we included people who received a TST at any point prior to their censor date. Due to the much wider variability in TST timing than in IGRA timing, this group was classified as not being screened in our sensitivity analysis. Next, we included all people who received an IGRA prior to their censor date, regardless of IGRA timing.
All analyses were conducted in R-Studio (Version 3.4.1) using the Survival package.
Results
Between January 1, 2012 and May 31, 2017, 3190 people initiated at least 90 days of dialysis in BC and met the inclusion for our study (Figure 1). In all, 1790 people (56.0%) were screened with IGRA, whereas 1400 (44.0 %) received no screening. People screened with IGRA were more likely to be younger, of nonwhite ethnicity, and have a renal transplant postdialysis initiation. People screened were also less likely to have an immune-suppressing comorbid condition at dialysis initiation (Table 1). The median duration between dialysis initiation and first IGRA screening was 16 days (Q1-Q3: 6.0-70.8), and the majority (86.4%) of people screened had a negative IGRA result (Table 2). Demographic and clinical characteristics stratified by IGRA result are presented in Table S2 of the Supplementary Appendix.

Study flowchart.
Screening and Latent Tuberculosis Treatment Details.
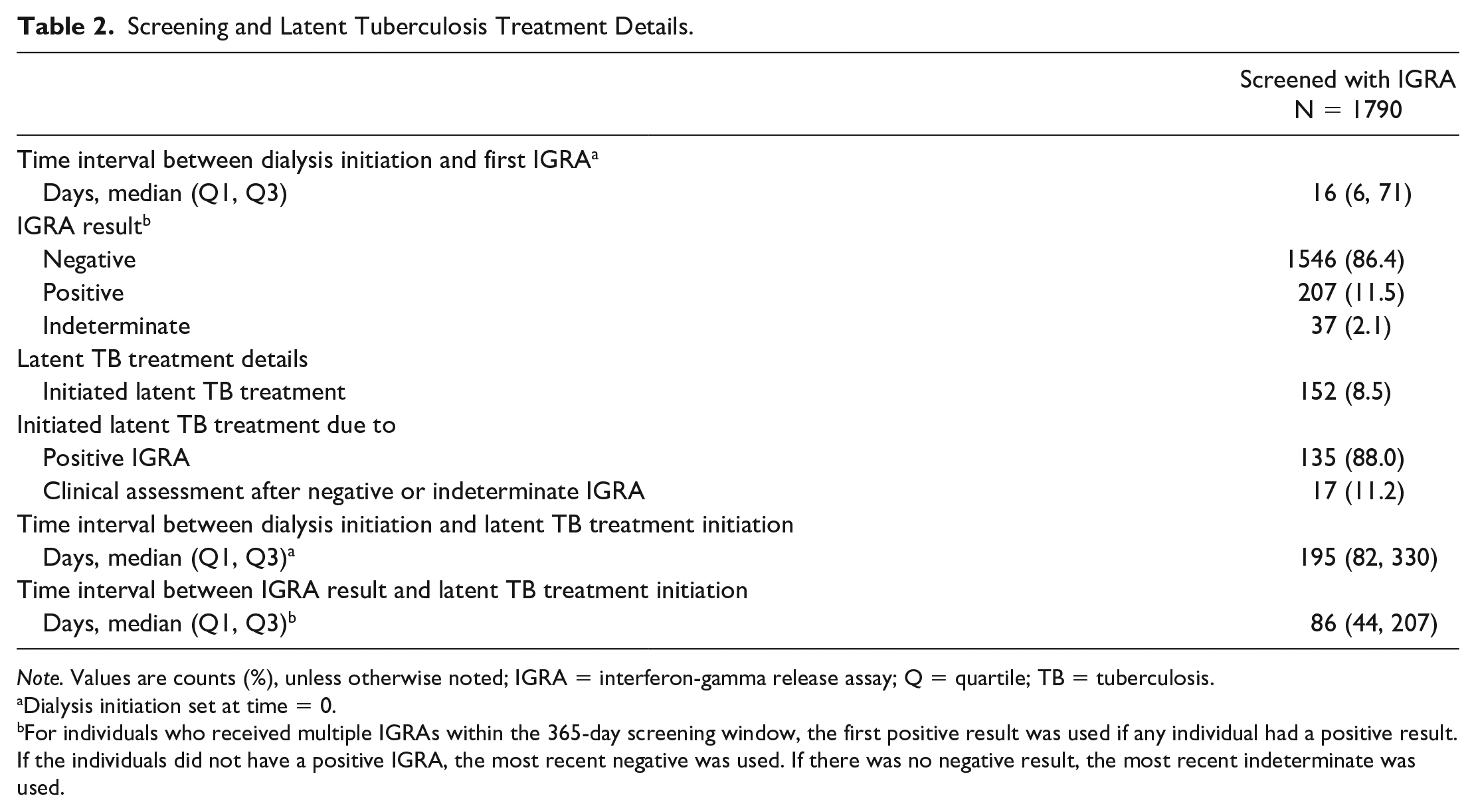
Note. Values are counts (%), unless otherwise noted; IGRA = interferon-gamma release assay; Q = quartile; TB = tuberculosis.
Dialysis initiation set at time = 0.
For individuals who received multiple IGRAs within the 365-day screening window, the first positive result was used if any individual had a positive result. If the individuals did not have a positive IGRA, the most recent negative was used. If there was no negative result, the most recent indeterminate was used.
Of the 1790 people screened, 152 (8.5%) initiated latent TB treatment postscreening. Of those, 135 (88.8%) began treatment after a positive IGRA, whereas 17 (11.2%) began treatment based on clinical assessment after a negative or indeterminate IGRA (Table 2). As per Canadian TB Standards, these 17 people were considered to be at a very high risk of infection that latent TB treatment was given presumptively. The median duration between dialysis initiation and latent TB treatment initiation was 195 days (Q1-Q3: 82-330). Of people not screened, only 1 (0.1%) person initiated treatment for latent TB, which was started post renal transplant.
Incident active TB was diagnosed in 6 (0.3%) of 1790 people screened during follow-up compared with 11 (0.8%) of 1400 people not screened, for an incidence rate of 1.2 (95% CI: 0.4-2.3) and 2.6 (95% CI: 1.4-4.5) per 1000 person-years, respectively. The cumulative active TB incidence in people who received screening compared with those who were not screened is shown in Figure 2. In multivariate analysis, the adjusted hazard ratio (aHR) for active TB in the screened group, as compared with the nonscreened group, was 0.3 (95% CI: 0.1-0.8) (Table 3). Overall, 10 (58.5%) people were diagnosed with pulmonary TB, and the median duration between dialysis initiation and incident active TB diagnosis was 300 days (Q1-Q3: 81-420). Clinical characteristics and treatment outcomes of those who developed active TB are presented in Table 4. Of the 152 people who initiated latent TB treatment postscreening, none developed active TB.

Cumulative active TB incidence in people who received no screening compared with those who were screened with IGRA.
Cox Proportional Hazard Model for Individuals Who Received No Screening Compared With Individuals Who Received an IGRA Within 365 Days of Dialysis Initiation.
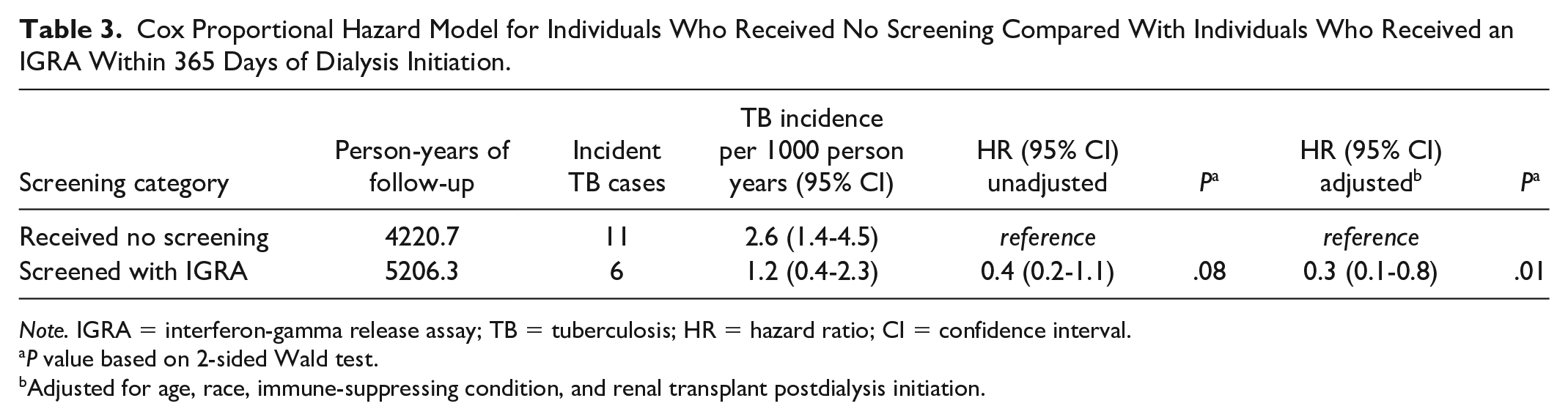
Note. IGRA = interferon-gamma release assay; TB = tuberculosis; HR = hazard ratio; CI = confidence interval.
P value based on 2-sided Wald test.
Adjusted for age, race, immune-suppressing condition, and renal transplant postdialysis initiation.
Clinical and Diagnostic Characteristics of People Who Developed Active TB.

Note. Values are counts (%), unless otherwise noted; TB = tuberculosis; IGRA = interferon-gamma release assay; Q = quartile.
Both individuals with positive IGRAs were offered latent tuberculosis infection therapy but declined.
The results of our sensitivity analyses were consistent with the main findings. When including all people who only received a TST in the nonscreened group, regardless of their TST result, the HRs remained consistent (aHR: 0.4, 95% CI: 0.1-0.9). In this group, 4 people initiated treatment for latent TB post-TST and none developed active TB. When we included all people who received an IGRA outside of the 365-day screening window, the aHR was 0.3 (95% CI: 0.1-0.8).
Discussion
In this study, we demonstrated that the systemic screening and treatment of people initiating dialysis for latent TB was associated with a 70% decrease in the likelihood of developing active TB, when compared with people not screened during the same period. Moreover, no active TB was observed among those who received latent TB treatment. Latent TB treatment regimens and outcomes are described in a related study. 11 In brief, we found that despite the advanced age, frequent comorbid conditions, and potential drug-drug interactions common in people undergoing dialysis, approximately 80% of people in our study who initiated latent TB treatment, successfully completed treatment. 11 In our study population, among those who had a positive IGRA and did not initiate latent TB treatment, the probability of active TB was approximately 3%.
Recently, WHO latent TB guidelines placed a strong recommendation on systematic screening and treating of latent TB in people undergoing dialysis; however, there are minimal data on the impact of such programs at a population level. 3 Much of the literature surrounding the impact of latent TB screening has focused on the effectiveness of latent TB treatment primarily in people living with HIV or in contacts of people diagnosed with pulmonary TB.12-15 Our study provides important data on the epidemiological impact of systematically screening and treating people undergoing dialysis and supports current recommendations.3,4,16 To date, there have only been 2 other studies looking at the impact of latent TB treatment in dialysis populations.17,18 Similar to our findings, both studies noted a decrease in TB incidence in those who were screened and received latent TB treatment.17,18 However, both studies were small trials based in high-TB incidence regions, and their results may not be generalizable to regions with a low-TB incidence. Given the large sample size and general population-based nature of our study, our findings may be relevant to dialysis programs in other low-TB incidence regions.
In our study population, more than one-quarter of the active TB was diagnosed within the first 3 months of dialysis initiation. These findings are consistent with other studies which show that most of the active TB is diagnosed within the first year of dialysis initiation.17-19 In this population, timely screening and assessment seems vital as people undergoing hemodialysis with active TB pose a substantial risk to other patients and health care workers, given the frequency and proximity of shared air space. 20 Without effective TB screening and prevention strategies, dialysis units can serve as means of ongoing TB transmission and subsequent TB cases.
In people undergoing dialysis, the diagnosis of active TB is often difficult because of extrapulmonary involvement and nonspecific symptoms that may mimic uremia, such as fever, anorexia, and weight loss.21,22 This atypical presentation may often lead to a delay in diagnosis and therapy, as well as potential onward transmission. Thus, clinicians should have a high degree of suspicion and consider the possibility of active TB whenever interacting with patients undergoing dialysis presenting with general symptoms such as fever, weight loss, and/or lymphadenopathy.21,22
While chest radiography, sputum smear microscopy, and mycobacterial culture are all part of the standard testing algorithm for active TB, immune-based tests for identification of LTBI, including the TST and the IGRA, have become a core component of latent TB testing. 4 The TST appears to be associated with higher rates of false-negative results in dialysis populations due to the high prevalence of anergy in the people undergoing dialysis. 22 The IGRA is reported to be more sensitive in the dialysis population, while offering a comparable level of specificity. 23 Furthermore, under most scenarios in dialysis patients, screening with an IGRA has been shown to be more cost-effective than the TST. 19 Based on the evidence from these studies, along with the convenience of drawing IGRAs as part of an initial dialysis bloodwork protocol, the BC screening program elected to use a universal IGRA screening approach to ensure that the cascade of care for this population was optimal.
Unfortunately, both the IGRA and the TST have important limitations, particularly concerning poor predicative value in people undergoing dialysis. While rates of false negatives may potentially be lower with IGRA, in our cohort, of the 1546 people who screened negative with an IGRA, 4 went on to develop active TB, highlighting the importance of multifactorial assessment beyond IGRA values alone, including assessment of TB exposure history and review of chest imaging. Of the 4 people who screened negative and went on to develop active TB, all were males above the age of 55, and 3 were on hemodialysis, and had diabetes. None had further immune-suppressing comorbid conditions.
Our study had several limitations. Primarily, this study was an observational retrospective study, and as with all observational studies, the potential for unmeasured confounding should be carefully assessed. Particularly, we were unable to control for country of birth as this information is not collected in PROMIS. While we were not able to include country of birth in our analysis, we did attempt to control for this by adjusting for ethnicity as a proxy which may have introduced misclassification bias. We were also unable to control for HIV status, which is another well-known TB risk factor. 1 While people undergoing dialysis are routinely screened for HIV, this information was not available in our data linkage. It is possible that there was a higher prevalence of HIV infection in the unscreened cohort and could have contributed to the increased TB risk. In BC, however, the prevalence of HIV infection is 5.1 per 100 000 population, and HIV-TB coinfection is uncommon in dialysis populations and is therefore unlikely to have affected our results.24,25 Finally, the objective of our study was to evaluate the impact of systematic screening, but not determine the optimal CKD stage to initiate latent TB screening. The pathophysiology of CKD-related immunodeficiency suggests that people with nondialysis-dependent CKD may also be at an increased risk for TB and may benefit from latent TB screening and treatment.26,27 However, further research is required to determine the optimal approach to screening in people with progressive CKD, approaching dialysis. 19
Conclusions
Our results indicate that systematic latent TB screening and treatment is associated with a significant decrease in active TB in people initiating dialysis. Given the importance of latent TB screening and treatment for high-risk groups in low TB incidence countries, our findings may be useful to inform scale-up of latent TB screening and treatment in dialysis programs in other low incidence regions.
Supplemental Material
Johnston_SupplementaryAppendix – Supplemental material for Effectiveness of Latent TB Screening and Treatment in People Initiating Dialysis in British Columbia, Canada
Supplemental material, Johnston_SupplementaryAppendix for Effectiveness of Latent TB Screening and Treatment in People Initiating Dialysis in British Columbia, Canada by Kamila Romanowski, Caren Rose, Victoria J. Cook, Inna Sekirov, Muhammad Morshed, Ognjenka Djurdjev, Adeera Levin and James C. Johnston in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We would like to acknowledge Leslie Chiang and Dr. Brett Baumann for their assistance with initial data cleaning, Fay Hutton, Sandra Peroff, James Tao, and Yin Chang for their assistance with data extractions, and Dr. Jonathon Campbell for feedback on the manuscript. We would also like to acknowledge the numerous people from BC Renal, the BCCDC Public Health Laboratory, and the BCCDC Provincial TB Services who contribute to the coordinated effort of screening people undergoing dialysis for TB, as well as the British Columbians on dialysis who contributed data toward this study. Findings from this study will be presented as a short oral abstract at the 50th Union World Conference on Lung Health, October 30 to November 2, 2019 in Hyderabad, India.
Ethics Approval and Consent to Participate
This study was approved by the University of British Columbia Research Ethics Board (H14-01977). Participant informed consent for was not required for this study.
Consent for Publication
All authors consented to this manuscript being published.
Availability of Data and Materials
The data that supported the findings of this study may be made available on request from the corresponding author upon reasonable request and institutional REB approval. Identifying/confidential patient data, however, will not be shared.
Author Contributions
J.C.J., V.J.C., A.L., and K.R. contributed to study concept and design. K.R., C.R. contributed to statistical analysis. K.R., C.R., V.J.C., I.S., M.M., O.D., A.L., and J.C.J. contributed to interpretation of data. K.R. contributed to initial draft of the manuscript. C.R., V.J.C., I.S., M.M., O.D., A.L., and J.C.J. contributed to critical revision of the manuscript for important intellectual content. K.R., C.R., V.J.C., I.S., M.M., O.D., A.L., and J.C.J. contributed to final approval of version to be published. J.C.J. contributed to study supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.C.J. is supported by the Michael Smith Foundation for Health Research, which had no role in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.