
Abstract
Background:
Opiate and benzodiazepine use is associated with increased mortality and poorer transplant outcomes in patients with chronic kidney disease (CKD).
Objective:
To determine the predictors of opiate and benzodiazepine prescription in people with kidney disease.
Design:
Cross-sectional, observational study.
Setting:
Outpatient clinics at Kingston Health Sciences Centre or at affiliated sites as of June 2017.
Patients:
Individuals with CKD being treated at clinics or with various dialysis modalities at Kingston Health Sciences Centre and affiliated sites.
Measurements:
The total number of regular opioid and benzodiazepine prescriptions was recorded for each patient. Patients were stratified based on clinical (eg, dialysis modality) and demographic (sex, age, diabetes mellitus [DM], ethnicity) characteristics, as elicited below.
Methods:
We evaluated opiate and benzodiazepine use by chart review in the following patient groups: conventional hemodialysis (HD) (n = 359), home hemodialysis (HHD) (n = 21), peritoneal dialysis (PD) (n = 95), patients attending the multidisciplinary chronic kidney disease clinic (MCKDC) (n = 322), and kidney transplant (KT) recipients (n = 176). Opiates and benzodiazepines were classified according to the American Hospital Formulary Service system. Patients were also stratified as white (n = 855), indigenous (n = 66), or all others (n = 48).
Results:
The mean age was 66.2 ± 14.9 years, 602 (61.9%) were men, and 439 (45.1%) had DM. Opiates were prescribed to 223 patients (22.9%), most frequently to HD (32.3%), followed by MCKDC (20.8%), HHD (19.0%), PD (14.7%), and KT (12.5%) (P < .001). The independent predictors of opiate prescription included DM (odds ratio [OR], 1.9; 95% confidence interval [CI], 1.4-2.6; P < 0.001), conventional HD (vs all other treatment modalities) (OR, 1.8; 95% CI, 1.3-2.5; P < .001), and female sex (OR, 1.4; 95% CI, 1.0-1.9; P = .041) after adjustment for age and ethnicity (R2 = 0.037, P < .001). Benzodiazepines were prescribed to 106 patients (10.9%), most frequently to HD (15.9%), followed by HHD (9.5%), KT (9.1%), MCKDC (7.5%), and PD (7.4%) (P = .005). The independent predictors of benzodiazepine use included female sex (OR, 2.3; 95% CI, 1.5-3.4; P < .001) and dialysis modality (excluding MCKDC and KT) (OR, 1.8; 95% CI, 1.2-2.8; P = .006) after adjustment for ethnicity, DM, and age (R2 = 0.027, P < .001).
Limitations:
We were not able to ascertain the indication for prescription of these drugs or patient adherence.
Conclusions:
Women with kidney disease are significantly more likely to be prescribed opiates and benzodiazepines than men with kidney disease. Further research is required to determine whether these medications contribute to increased morbidity and mortality in women with kidney disease.
Trial Registration:
This manuscript does not meet the criteria for requiring registration or a statement of written consent from study participants. The previous submission of this manuscript already made mention of Research Ethics Board approval.
Background
Chronic kidney disease (CKD) affects numerous patients across North America, with the US Centers for Disease Control and Prevention estimating that more than 20 million American residents are currently living with CKD. 1 Polypharmacy is frequently observed as these patients are prescribed medications to preserve kidney function, manage comorbidities, and reduce chronic pain. In the Atherosclerosis Risk in Communities Study, a prospective cohort of community-dwelling participants in the United States, more than 35% of patients with CKD used 10 or more pharmaceutical products. 2
Two widely prescribed classes of central nervous system (CNS) active drugs include opioids and benzodiazepines. Opiate use is high in patients with end-stage kidney disease (ESKD). In 1 study that tracked patients awaiting kidney transplant (KT) in the United States, 29% filled opioid prescriptions in the year before their transplant, with the highest levels of use observed in women, whites, those with comorbidities, and patients with longer duration of CKD. 3 In a Canadian study, the reasons for opioid use were musculoskeletal pain (65%), dialysis procedure–related pain (14%), peripheral neuropathy (15%), and peripheral vascular disease (10%). Opiate prescription has been linked to adverse patient outcomes, including mortality and graft loss, 4 in KT patients, as well as increased rates of hospitalization, falls, and altered mental status in hemodialysis (HD) patients. 5 From wave 2 data of the Dialysis Morbidity and Mortality Study published more than 10 years ago, benzodiazepines were prescribed to 14% of incident dialysis patients and more frequently to women, smokers, and people of white race. 6 Benzodiazepine (and zolpidem) use was associated with a 15% higher mortality rate after multivariate adjustment. 6 Recent studies conducted within the general population have shown that women are prescribed opioids 7 and benzodiazepines 8 with greater frequency compared with men.
Opioids and benzodiazepines appear to play a significant role in the pharmacotherapy of CKD, with a recent meta-analysis revealing that up to 36% of patients with CKD are prescribed these agents. 2 Given the documented risks associated with the use of these agents, along with the potential for their abuse amid a national epidemic of illicit opioid use, the need to understand patterns of opioid and benzodiazepine prescription in patients with CKD is more important than ever before. Furthermore, the prescription of these agents in patients with kidney disease may not always be adequate, optimally effective, or appropriate, as 1 study revealed that up to 75% of dialysis patients experienced inadequate pain management, leading to a decreased quality of life. 1 Thus, the current literature suggests variation in prescription practices among different demographic groups amid a broader context of generally inappropriate or ineffective use, if at all, of benzodiazepines or opioids in patients with kidney failure.
Although there is some evidence to suggest demographic trends in analgesic and benzodiazepine prescription for patients with CKD, these data are sparse and patients with earlier stages of CKD, the largest group of patients, have not been considered. In this study, we sought to investigate demographic patterns and predictors for rates of opioid and/or benzodiazepine prescription across a spectrum of CKD disease severity and ESKD treatment modalities.
Methods
Following approval by the Health Sciences and Affiliated Teaching Hospitals Research Ethics Board, we conducted this cross-sectional, observational study by evaluating 973 patients for opiate and benzodiazepine prescription by chart review. Charts were retrieved from patient records at Kingston Health Sciences Centre or at affiliated sites as of June 2017. Collected data included race (white, indigenous, or other), sex, treatment modality, age, presence of diabetes mellitus (DM), and dialysis vintage (subset on dialysis only), as well as the total number of medications and whether or not patients were prescribed opioids or benzodiazepines. Benzodiazepine or opioid “use” was defined as the prevalence of benzodiazepine and opioid regular (not prn) prescriptions found on patient charts in June 2017.
Data were entered into an Excel file and imported into IBM SPSS (Version 24.0 for Windows, Armonk, New York, 2016) for statistical analysis. Following a descriptive analysis (means and standard deviations for continuous data, and frequencies and percentages for categorical data), those prescribed opioids or benzodiazepines were compared with those who were not prescribed either class of drugs using Pearson χ2 tests for categorical data and independent samples t tests for continuous data. Variables were selected for entry into the multivariable models for opioid use and for benzodiazepine use on the basis of clinical relevance, empirical evidence, and a potential association (P < 0.15) on univariate analyses. A P value of .05 was used as the criteria for statistical significance, and no adjustments were made for multiple comparisons.
Results
The sample characteristics of opioid and benzodiazepine users are provided in Table 1 along with the tests of significance. Opiate users were more likely to be prescribed a greater number of medications and were more likely to be women and those with DM. In multivariable logistic regression modeling, the independent predictors of opiate prescription included DM (odds ratio [OR], 1.9; 95% confidence interval [CI], 1.4-2.6, P < .001), conventional HD (vs all other treatment modalities) (OR, 1.8; 95% CI, 1.3-2.5; P < .001), and female sex (OR, 1.4; 95% CI, 1.0-1.9; P = .041) after adjustment for age and ethnicity (R2 = 0.037, P < .001). Benzodiazepine users were also more likely to be prescribed a greater number of medications and were more likely to be women. The independent predictors of benzodiazepine use included female sex (OR, 2.3; 95% CI, 1.5-3.4; P < 0.001) and dialysis modality (excluding multidisciplinary chronic kidney disease clinic [MCKDC] and KT recipients) (OR, 1.8; 95% CI, 1.2-2.8; P = .006) after adjustment for ethnicity, DM, and age (R2 = 0.027, P < .001).
Sample Characteristics by Opiate and Benzodiazepine Use.
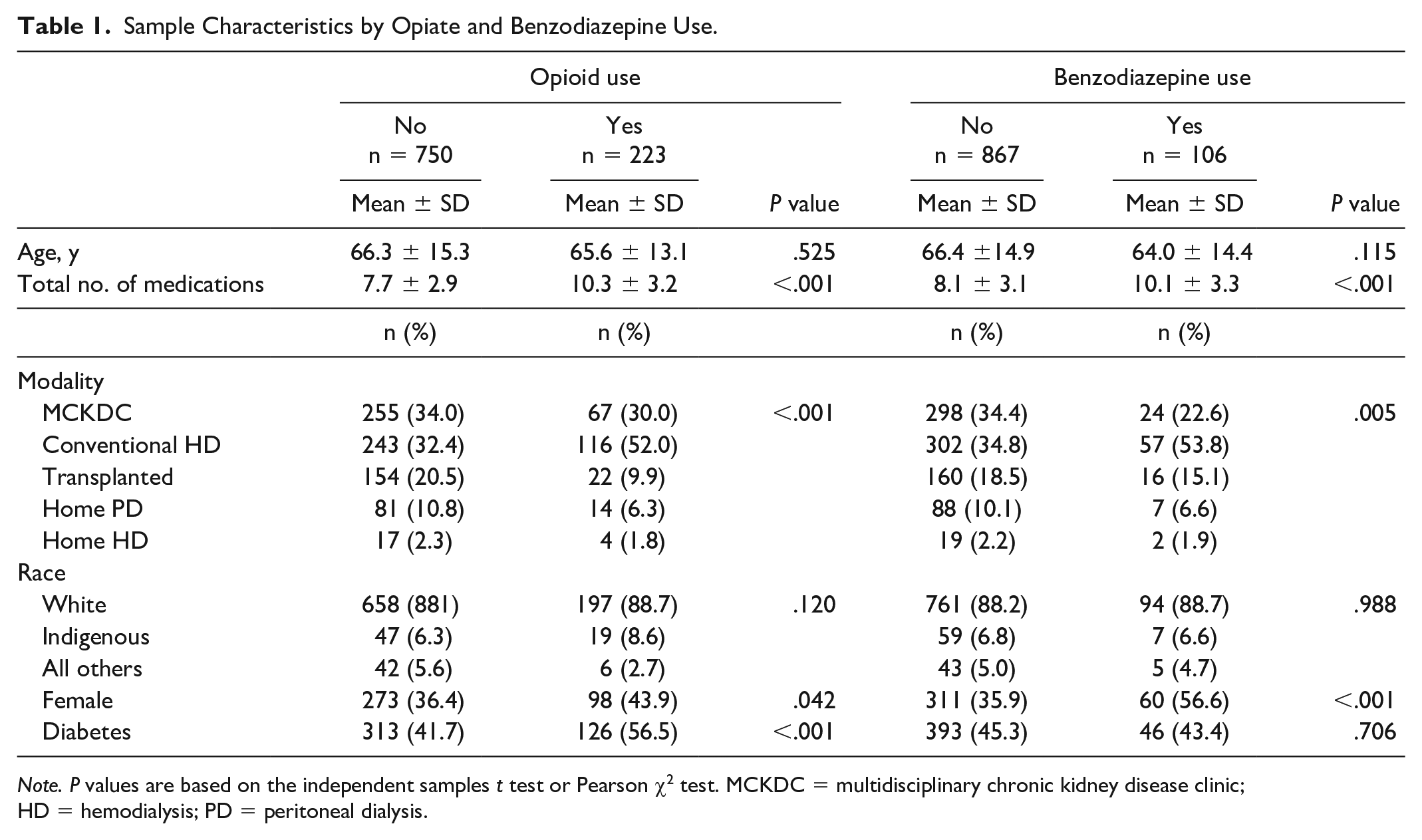
Note. P values are based on the independent samples t test or Pearson χ2 test. MCKDC = multidisciplinary chronic kidney disease clinic; HD = hemodialysis; PD = peritoneal dialysis.
Discussion
Demographic factors may play an important role in determining the rates of opiate and benzodiazepine prescription. Specifically, we report that benzodiazepine and opiate prescription was more frequent in women and in those receiving conventional HD. After adjustment for dialysis modality, ethnicity, DM, and age, women were more than twice as likely to be prescribed benzodiazepines, a class of drugs linked to adverse outcomes including mortality, 6 than men.
Users of opiates and benzodiazepines were prescribed more medications overall, and both classes of drugs were prescribed more frequently in conventional HD patients. It is possible that this may relate to frequent contact with the health care system, although examination of prescription rates among patients attending the predialysis CKD clinics suggests that this pattern of use precedes ESKD. Patients receiving independent dialysis modalities and KT overall had lower rates, possibly reflecting healthier patients. Patients with DM were more likely to be prescribed opiates but not benzodiazepines. Although studies conducted in Canada have suggested that indigenous patients are prescribed opioids at a greater rate, 9 our study did not confirm this. This could be due to the relatively small size of the indigenous patient population under study (n = 66).
Whether women with kidney disease have more indications for prescription of CNS active drugs is not known. What is known is that the use of these drugs is associated with adverse outcomes. It is noteworthy that there is evidence to suggest that men and women on dialysis have similar mortality rates, a finding not typically observed in the general population. Furthermore, women undergoing HD have substantially higher risks of hospitalization and 30-day readmission than men. 10 Efforts to understand the reasons underlying sex differences may help identify targeted interventions to improve the care of dialysis patients. It is worth further evaluation to determine whether prescription of CNS active drugs may contribute, in part, to the large difference in hospitalization rates observed in women receiving HD and the apparent lack of a survival advantage.
There are limitations to our study. The patients included in this single-center study were primarily from rural Eastern and Northern Ontario, regions with particularly high rates of opioid prescription and misuse. 11 Examination of prescription patterns in patients with CKD in other centers and provinces with different prescribing practices and different patient populations could provide further insight into factors that govern benzodiazepine and opiate prescription in patients with kidney disease. It is a major limitation that we were not able to ascertain the indication for prescription of these drugs. In many cases, drugs were prescribed by alternate caregivers. Data linking benzodiazepine and opioid use to adverse outcomes in the elderly are well-described; however, similar data in the subpopulation with CKD are lacking. Furthermore, as benzodiazepine and opioid use among patients in this study was determined by the prevalence of prescriptions on chart review, it was not ascertained whether or not patients were actually adhering to these medication regimes. In addition, although the analysis of differences in prescription was adjusted for certain demographic factors and treatment modalities, other comorbidities that are also adverse consequences or contraindications to benzodiazepine or opioid use (eg, osteoporotic fractures) were not included in the analysis.
Further research is required to examine differences between the sexes in reporting pain and the responses of care providers toward people of either sex when such symptoms are brought to their attention. Ultimately, it will be important to determine whether there are sex differences in the individual indications for these drugs and to develop a framework to systematically deprescribe these agents where possible.
Conclusions
Women with kidney disease are significantly more likely to be prescribed opiates and benzodiazepines than men with kidney disease. Given the association between CNS active drugs and increased mortality, graft failure, falls, and altered mental status, further research is required to determine whether these medications contribute to increased morbidity and mortality in women with kidney disease.
Footnotes
Ethics Approval and Consent to Participate
The study was conducted according to the Declaration of Helsinki and was approved by Queen’s University and Affiliated Teaching Hospitals Research Ethics Board.
Consent for Publication
Consent for publication was obtained from all authors
Availability of Data and Materials
Data and materials will be available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.