
Abstract
Purpose:
Low socioeconomic status, race, ethnicity, and rural/remote populations are all associated with disparities in access, care, and outcomes for chronic kidney disease (CKD). There have been different interventions supported by Canadian renal programs to address these disparities. This article reviews the evidence for impact of strategies to reduce inequities experienced by vulnerable populations living with or at risk of CKD and to collate and share interprovincial targeted interventions through the newly formed “Canadian Senior Renal Leaders Community of Practice” focused on translating evidence into clinical practice and policy.
Source of Information:
A literature search of Medline, CINAHL, PubMed, and Google Scholar from 2008 to 2018 identified 13 reports of processes and interventions that have been implemented in Australia, Canada, and the United States to reduce inequities in CKD care and can be categorized into 3 broad areas: (1) early screening and prevention, (2) disease management and dialysis, and (3) pretransplant. Web sites from each Canadian jurisdiction and from Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD) Network were used to assess the current state of Canadian initiatives.
Methods:
Reviews were completed to gather information on renal initiatives for vulnerable populations, including (1) identification of populations that experience disparities in access to care or in outcomes in the context of CKD prevention and treatment and (2) interventions that have been implemented to reduce disparities in access, care, and outcomes for vulnerable populations with CKD. A current state summary of Canadian initiatives related to vulnerable populations was conducted through a review of publicly available information, including a review of renal program Web sites and a review of current projects related to vulnerable populations that are part of Can-SOLVE CKD. Can-SOLVE CKD is a Canadian Institutes of Health Research Strategy for Patient-Oriented Research (CIHR-SPOR) funded research network to transform the care of people affected by kidney disease.
Key Findings:
Interventions to improve inequities in access to CKD screening, disease management, and care are successful when developed with community engagement, provided to the patient in their own environment, and tailored to specific populations. Many provincial renal programs have implemented initiatives to support vulnerable populations with or at risk of CKD. Current projects funded through CIHR SPOR focus on underserved populations and involve partnerships with Indigenous populations. Many renal programs in Canada had or were in the process of implementing interventions to support vulnerable populations with CKD; however, information about the initiatives were not readily available online despite a strong interest and opportunity to support interprovincial knowledge sharing. Despite this common interest, little information is systematically shared between Canadian jurisdictions to support interprovincial sharing to promote evidence-informed policy and program development. Efforts will be made through the newly formed Canadian Senior Renal Leaders Community of Practice to collaborate and share learnings to inform future program and policy development, implementation, and evaluation.
Limitations:
As this was not a systematic review, literature search only encompassed studies published in English between 2008 and 2018. It is possible that populations and interventions were overlooked during the search and through the screening process. Furthermore, the controversial definition of “vulnerable” and literature that only came from Canada, the United States, and Australia limits the generalizability of this review.
What was known before
Racial, ethnic, and socioeconomic disparities are well recognized in chronic kidney disease (CKD) populations. Interventions to improve access to and outcomes of CKD care for vulnerable populations have been implemented within and outside of Canada and are influenced by demographics and geography. A review of broad scope interventions that aim to address CKD care disparities—their lessons and learnings—would be valuable to inform consistent policy and program development across Canadian renal programs.
What this adds
Our review provides a summary of which groups experience disparities in access to care or in outcomes in the context of CKD prevention and treatment and highlights what interventions have been implemented to reduce these disparities, both within and outside of Canada. We highlight other clinical and policy areas of interest to Canadian clinical and administrative leaders that will be explored in future.
Introduction
In 2017, senior executives from adult nephrology programs and networks across Canada formed a national Community of Practice. The Community of Practice provided a national forum for senior leaders within provincial renal health care agencies, health authorities, strategic networks and programs to (1) engage in group strategy discussions in areas of common interest, (2) provide a national knowledge transfer forum to inform evidence-based policy and program development, and (3) support cross-jurisdictional quality improvement and performance measurement. Administrative and physician strategic leaders were identified for each jurisdiction.
Initial thematic areas were put forward for topics of interest. Meeting the chronic kidney disease (CKD) care needs of vulnerable populations was the highest ranked theme by participants. The group sought to (1) identify which populations experience disparities in access to care or in outcomes in the context of CKD prevention and treatment, (2) conduct a literature review of interventions that have been implemented to reduce disparities in access, care, and outcomes for vulnerable populations with CKD, (3) establish a current state of provincial initiatives related to vulnerable populations through a review of publicly available information, including a review of renal program Web sites, and (4) review projects related to vulnerable populations that are part of the CAN-SOLVE CKD (Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease) Network, currently funded through the Canadian Institutes of Health Research, Strategy for Patient-Oriented Research (CIHR-SPOR). 1
Methods
Literature Review
A rapid evidence review on access to CKD care in vulnerable populations was performed in July 2018. The purpose of this review was to summarize the evidence on vulnerable populations in the context of CKD and to identify interventions that have been implemented in Canada, the United States, and Australia to improve access and outcomes to CKD treatment in these vulnerable populations. The review focused on two research questions:
Search Strategy
A literature search was conducted on June 20, 2018, by Knowledge Resource Services (KRS) within the Knowledge Management Department of Alberta Health Services (AHS). KRS searched databases for English language papers published from 2008 to 2018 and included Medline, CINAHL, PubMed, and Google Scholar. Search strategy involved combinations of keywords and subject headings that targeted the definitions of “vulnerable” as described by Waisel 2 and focused on CKD and renal insufficiency. The term “vulnerable” was used to describe the populations that experience disparate health care access and that may be socially or economically disadvantaged 2 ; however, the term is inconsistently defined and used heterogeneously in public health. 3 The search strategy was designed to include Indigenous population, those of low socioeconomic status (SES), ethnic and racial minorities, gender/sexual minorities, among others. Like “vulnerable,” “race” and “ethnicity” are also complex terms. 4 It is important to include them as they are a source of health disparity in jurisdictions where the majority population is white and English-speaking. 4 Here, “race” refers to groupings based on skin color or ancestry, whereas ethnicity refers to cultural background or spoken language. The full search strategy is included in the appendix. As the literature review was originally written in August 2018, the search was limited to the previous 10 years (2008-2018) to ensure that interventions were relatively recent. Reports were limited to publication in English.
Articles identified by KRS in their search were screened in two phases by title and abstract against the inclusion/exclusion criteria listed in Table 1 below. The first phase of screening was to eliminate articles that did not describe a defined population affected by disparities in access to CKD care. The second phase was to identify reports that described both a disadvantaged population and an intervention to reduce disparities in access.
Inclusion and Exclusion Criteria for Screening Results From the Literature Search.

Note. CKD = chronic kidney disease.
Inclusion and Exclusion Criteria
Titles and abstracts of the search output were screened and evaluated using the selected full-text publications for final article selection and the predefined inclusion and exclusion criteria. The criteria are defined in Table 1. Eligible populations included both individuals at risk of developing CKD and individuals who have already developed CKD. Reports were included if they described an intervention that specifically was intended to improve access to the CKD continuum of care. Reports were excluded if they did not describe an intervention or if the outcomes of the intervention were not stated. There were no jurisdictional limitations.
Jurisdictional Scan of Provincial Health Initiatives Targeting Vulnerable Populations and CAN-SOLVE CKD Projects
A Canadian jurisdictional scan was conducted to supplement the results of the literature search. The scan included a Web review of provincial renal programs and projects underway by CAN-SOLVE CKD. A review was undertaken of publicly available information from each provincial jurisdiction in July and August 2018. This review consisted of a search targeting resources available on the Internet that pertained to health programs with a specific focus on those initiatives that targeted vulnerable populations. The search was organized by province and included Web resources for provincial agencies and departments across Canada such as health authorities, social services, health and wellness, and health and community services (see Table 3 for Web sites accessed). Key data points that were collected included the name of the agency, the name of the initiative, objectives of the initiative (as presented through Web resources), the definition of vulnerable populations (where available), and necessary sources/references. Only English Web sites were included. The information on reviewed provincial and federal initiatives involving vulnerable populations was collated and summarized, and can be viewed in Table 3.
Research initiatives that are part of the CAN-SOLVE CKD Network were reviewed to identify any projects currently underway that are primarily focused on vulnerable groups and reducing disparities to CKD care. Summary descriptions of the projects were reviewed and captured if they identified a specific population that is at a disadvantage for CKD care (eg, ethnic minorities, Indigenous populations, rural/remote, low SES) and was explicitly referenced within their study description.
Results
Literature Search
A total of 228 articles were identified by KRS with references and abstracts provided for further review. One study was found through Google when searching for an article identified in the literature search. A total of 151 studies were excluded in the first round of screening, and 77 articles were included in the review. Thirteen studies described an intervention to improve access to CKD care and were used in the qualitative synthesis; 51 studies were included as a high-level overview of populations that experience disparities in CKD outcomes or in access to CKD care; and 13 were excluded following full-text review (Figure 1). Although jurisdictional boundaries were not included as a screening criteria, articles describing the results of CKD interventions were only identified from Canada, the United States, and Australia. See Table 2 for a summary of the 13 studies included in the qualitative synthesis.

PRISMA flow diagram of the identified studies. 52
Data Extraction Table of Included Studies.
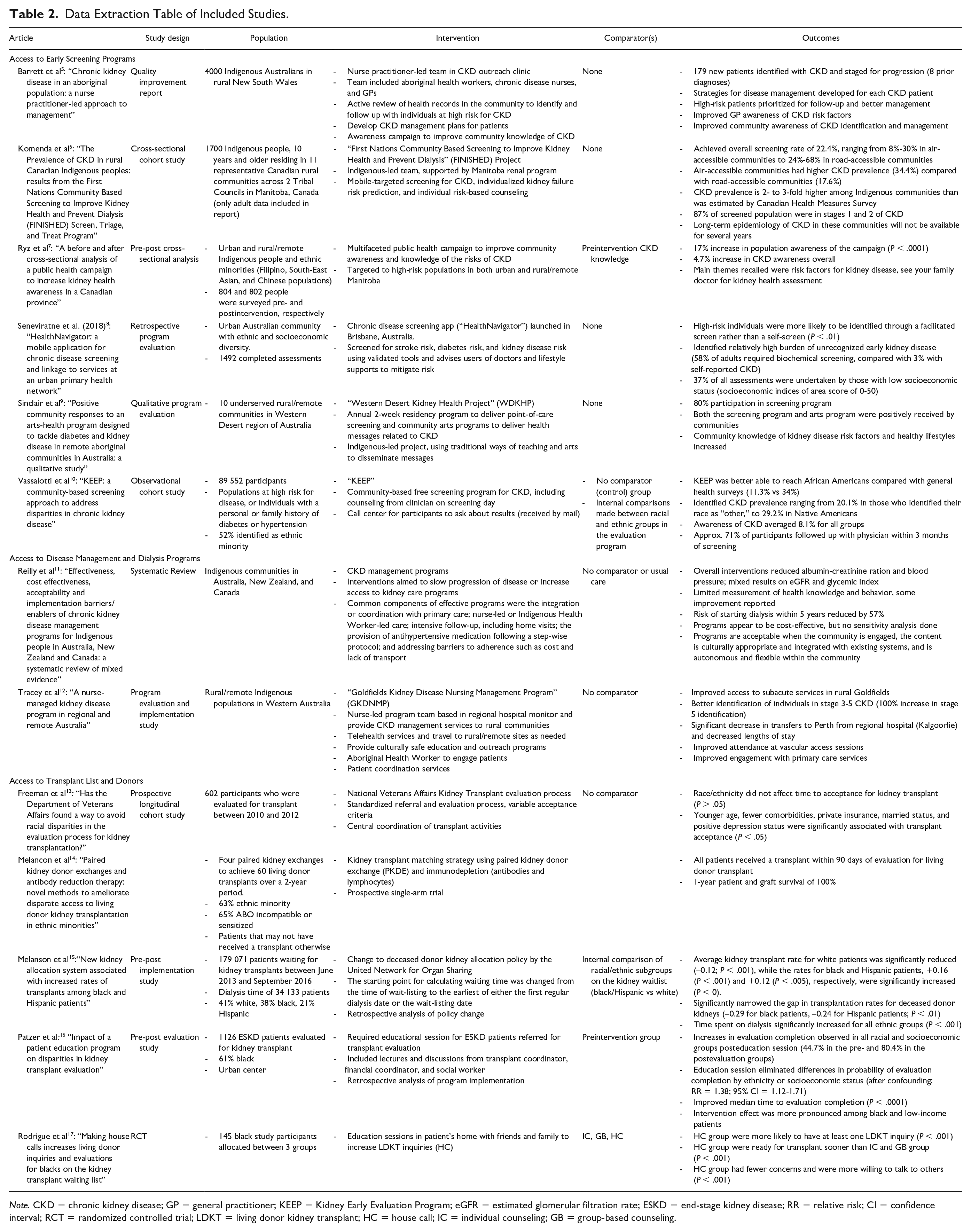
Note. CKD = chronic kidney disease; GP = general practitioner; KEEP = Kidney Early Evaluation Program; eGFR = estimated glomerular filtration rate; ESKD = end-stage kidney disease; RR = relative risk; CI = confidence interval; RCT = randomized controlled trial; LDKT = living donor kidney transplant; HC = house call; IC = individual counseling; GB = group-based counseling.
Web Search
Generally, the vulnerable population definitions were homogeneous, speaking of services to people of First Nations, Inuit, Metis, and urban Indigenous backgrounds. Inclusion of people of recent immigrant status or homelessness was more variable. This review highlighted 15 provincial initiatives and 1 federal initiative targeting “vulnerable populations” and “susceptible populations.” The majority of these initiatives targeted First Nations and Indigenous populations affected by chronic disease.
Disadvantaged Populations in CKD Care
In general, the populations that are disadvantaged with respect to CKD care are the same groups that are otherwise generally disadvantaged in health care. 18 Specifically, the literature focuses on disparities experienced by those with low SES, racial/ethnic minorities, Indigenous populations, rural/remote populations, with somewhat less evidence related to CKD care disparities for undocumented immigrants, the unemployed, and those with substance misuse problems. Often, these populations intersect and are associated with other risk factors for CKD such as smoking, obesity, and diabetes, thus compounding the vulnerability of these groups.19-21
Disparities exist across the continuum of care for CKD, regardless of jurisdiction. Inadequate access to early screening and prevention has been noted in low SES populations in the United States 22 ; ethnic minority populations in the United States23-25; and in Indigenous populations in Canada and Australia.5,9,26-28 These populations also experience disparities in access to all renal replacement therapies, as do rural/remote populations, undocumented immigrants, the unemployed, and substance misusers. It has been shown that disadvantaged populations experience reduced access to and worse outcomes from dialysis treatments.11,29-34 Once on dialysis, these populations wait longer for pretransplant evaluation,14,33-39 and have consistently lower rates of transplant from both deceased and living kidney donors.14,42-45 Furthermore, disadvantaged populations also may experience inadequate posttransplant care and have fewer end-of-life care discussions.44-46
Interventions to Improve Access to CKD Care
Disparities in access to CKD care lead to poorer treatment outcomes and increased mortality rates in these vulnerable populations.49-51 Interventions to improve access to care fall into three categories along the care continuum: early screening and prevention, disease management and dialysis, and pretransplant. The literature describing interventions for rural disease management and screening/prevention activities came largely from Australia and Canada, rather than from the United States. The reports describing interventions are detailed in Table 2. Early screening programs were often mobile and implemented in rural/remote communities, and tended to be successful when developed with community engagement, and education strategies and individualized counseling were included to complement the program activities.5-10
Effective disease management programs for vulnerable populations were able to engage and treat the patient in their own environment; thus, these programs leveraged telehealth technology, allied health professionals, and community members to support patients. 12 Effective programs for Indigenous people were integrated with primary care, were led by either nurses or Indigenous health workers, included intensive follow-up, provided antihypertensive medication to participants, and improved treatment adherence by mitigating transportation and cost barriers to care. 11 Overall, these programs were able to significantly reduce clinical signs of kidney disease, such as creatinine levels and blood pressure. 11
Reports on limiting the disparities in access to kidney transplantation were from the United States and focused on ethnic minority groups (specifically, African American and Hispanic populations), rather than rural/remote communities. Transplant access was often improved using educational strategies or policy changes rather than using health promotion strategies.14,36 On the policy side, these included standardizing transplant referral and eligibility processes 13 ; on the education side, these included engaging the patient and the patient’s social network to discuss transplantation. 17
This review highlighted the lack of long-term evaluations of access improvement interventions along the continuum of CKD care. Outcomes used in the included studies were largely focused on the short term. They included process outcomes (eg, number of screens undertaken or completed), engagement outcomes, or short-term epidemiological outcomes (eg, percent positive screens compared with hypothesis). The studies were limited in their measurement of health outcomes such as incident CKD, incident end-stage renal disease, glomerular filtration rate progression, emergent dialysis starts (“crash starts”), incident planned dialysis starts, and transplant rates. Instead, reports more often measured program-related and process outcomes, such as screening rates or patient satisfaction. Although these are useful pieces of information, they can only support inferences about the long-term effect of the intervention on CKD outcomes in vulnerable populations.
Web Review of Provincial Renal Programs
It was clear that publicly available information told an incomplete story, based on the internal knowledge of work underway or in development within specific jurisdictions. For example, information on the Manitoba-based Kidney Check Program was readily available; while the Ontario adoption was well underway, it was not publicly reported. Furthermore, Saskatchewan conducts such work regionally or locally, and is not reported in provincial public Web forums.
A second common theme was the focus of most provinces on First Nations, Inuit and Metis communities, patients with chronic diseases and complex health conditions. Many provinces emphasized the importance of cultural competency, cultural safety, access issues, and promoting equity for all people. Cultural competency courses are available online by British Columbia and Ontario, both at no cost. Some provinces provided detail of a number of different approaches to these issues, but not on how the approaches were integrated from the patient’s perspective or how they specifically applied to provincial renal programs. These initiatives and the Web sites accessed can be found in Table 3.
Web Sites Accessed for the Review of Provincial Health Initiatives Targeting Vulnerable Populations.

Note. BCCSU = British Columbia Centre on Substance Use; AHTF = Aboriginal Health Transition Fund; ePSWs = enhanced-skill Personal Support Workers; RN = registered nurse; OPHS = Ontario Public Health Standards.
CAN-SOLVE CKD
Of the 18 Can-SOLVE CKD research projects, two identified specific populations that are at a disadvantage for CKD care (eg, ethnic minorities, Indigenous populations, rural/remote, low SES) and of special interest to their study. Both projects related to Indigenous health. Broadly, the two respective projects seek to (1) identify diabetes and CKD in Indigenous communities, and (2) improve Indigenous patient knowledge about treatment options. Kidney Check, is a screening initiative in Indigenous communities in five provinces across Canada with a goal of decreasing the burden of CKD and kidney failure in these communities. 53 The second project involves working in partnership with Indigenous patients and families who have or are affected by CKD to develop a unique suite of educational approaches for treatment options for failing kidneys specifically for the Indigenous population. 54
While not calling out vulnerable populations explicitly, several CAN-SOLVE research projects include interventions for managing diabetes and other comorbidities frequently linked with CKD which may disproportionately impact vulnerable populations.
Discussion
Although this review sought to understand broadly what different groups experience disparities and what interventions provinces and other jurisdictions have implemented to address these, there are important limitations and risks when vulnerable populations are grouped together. The term “vulnerable populations” for the purposes of this review captured low-income populations, Indigenous populations, ethnic minorities, and rural/remote populations. The search strategy developed for this review was thorough but not systematic, so it is possible that some populations were missed in this review. Elderly populations, language minorities, and specific racial minorities were not specifically included in the search strategy so the interventions identified in the scoping review may not reflect their experiences with CKD care. Even for the populations that were included in the search strategy, how each of these populations and individuals within them experience CKD care—their inherent or experienced challenges, barriers and advantages—is, of course, very different.
Diseases of aging (eg, diabetes, cardiovascular disease, chronic obstructive pulmonary disease [COPD]) often disproportionally affect vulnerable or socially disadvantaged populations. 18 Although comparing different diseases was outside the scope of this review, there is existing literature that examines interventions related to cardiovascular disease for vulnerable populations. 55 The systematic review published by Walton-Moss 55 examining vulnerable populations in cardiovascular diseases found remarkable similarities between the populations (racial and ethnic minorities, those with low SES, rural populations) and interventions (education and counseling interventions conducted by health care workers). For type 2 diabetes, the same pattern was seen in a study of community-based interventions in the United Kingdom. 56 In this study, community outreach interventions, interventions involving peers, and interventions that were relevant and accessible to the target population were identified as key success factors. 56
As described earlier in this review, it is important to note that the term “vulnerable populations” itself has been criticized. It has been argued that the term “underemphasizes the multi-dimensional processes that cause unequal distributions of material, cultural, social and political resources.” 57 Furthermore, it has been noted that the characterization of susceptibility and vulnerability can be disempowering and can further contribute to an “us” and “them” power imbalance. 58 How to effectively implement provincial policies that effectively reduce disparities in care is a challenge facing all renal programs and governments across Canada, and this labeling may be a barrier itself in thinking about how to improve care. Although no explicit jurisdictional limitations were placed on the literature search, articles that included both a defined population and a specific CKD intervention were exclusively from Canada, the United States, and Australia—all English-speaking countries with highly developed health care systems, limiting the generalizability of the results to Quebec (which is primarily francophone).
As our review has found, partnership-building is a key and necessary component to initiatives involving First Nations, Inuit, and Métis communities. Can-SOLVE CKD can leverage existing health services and research partnerships to improve kidney care in underserved populations, while leveraging the engagement and patient-oriented research strategies to improve the knowledge translation element of CKD care. 59 This model helps improve the relevance, accessibility, and acceptability of CKD interventions. For example, the implementation of CKD screening in both Ontario and Manitoba is built entirely on a foundation of trust and partnership with First Nations communities. Within Can-SOLVE CKD, the Indigenous Peoples’ Engagement and Research Council (IPERC) was established to ensure that the network “appropriately incorporates, addresses and respects the unique needs and perspectives of Indigenous peoples.” 60 To further support respectful and effective partnership-building, the IPERC commissioned a working group to develop Wabishki Bizhiko Skaanj (wah-bish-kih biish-ih-goo skaa-nch), a learning pathway to enhance researchers’ knowledge and awareness of racial biases, Indigenous voices and stories, the impact of colonization on Indigenous health, and culturally safe health research practices.
While initiatives have been implemented in Canada to reduce the disparities in access to and treatment of CKD, up-to-date information about these initiatives are not consistently available, despite the strong clinical and administrative interest in translating knowledge into clinical practice and policy. Members of the Canadian Senior Renal Leaders Community of Practice have committed to increased interprovincial collaboration and knowledge transfer. Sharing and disseminating practical tools such as business cases, toolkits, and evaluation frameworks could strengthen and expedite more consistent broad-scale policy and program implementation across provincial borders and help guide investment. CAN-SOLVE will be an important contributor and partner in building evidence, and their own efforts are guided by a Knowledge User and Translation Committee.
The Community of Practice has identified several other opportunities for increased collaboration, and these will be areas of focus for the group moving forward. These include building strategic influence in health policy with provincial Ministries of Health, approaches to sustainability for renal services, developing national quality indicators for renal care, and identifying effective upstream strategies to prevent CKD.
Conclusion
Interventions to improve inequities in access to CKD screening, disease management, and care are successful when developed with community engagement, provided to the patient in their own environment, and tailored to specific populations. Many provincial renal programs have implemented initiatives to support vulnerable populations with or at risk of CKD. Despite this common interest, little information is systematically shared between Canadian jurisdictions to support interprovincial sharing to promote evidence-informed policy and program development. Efforts will be made through the newly formed Canadian Senior Renal Leaders Community of Practice to collaborate and share learnings to inform future program and policy development, implementation, and evaluation.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.