
Abstract
Background:
Erythropoiesis-stimulating agents including epoetin alfa have been a mainstay of anemia management in patients with chronic kidney disease. Although the standard practice has been to administer epoetin alfa to patients on hemodialysis (HD) intravenously (IV), subcutaneous (SQ) epoetin alfa is longer acting and achieve the same target hemoglobin level to be maintained at a reduced dose and cost.
Objective:
The primary objective of this study was to determine the economic benefits of change in route of epoetin alfa administration from IV to SQ in HD patients. The secondary objectives were (1) to determine the differences in epoetin alfa doses at the pre-switch (IV) and post-switch period (SQ) and (2) to determine serum hemoglobin concentration, transferrin saturation, ferritin level, IV iron dose and cost in relationship to route of epoetin alfa administration.
Design:
This retrospective observational study included patients who transitioned from IV to SQ epoetin alfa.
Setting:
Two HD sites in southern Saskatchewan (Regina General Hospital, and Wascana Dialysis Unit, Regina) and 2 sites in northern Saskatchewan (St. Paul’s [SPH] Hospital, and SPH Community Renal Health Center, Saskatoon).
Patients:
The study includes 215 patients who transitioned from IV to SQ and were alive at the end of 12-month follow-up period.
Measurements:
We calculated the dose and cost of different routes of epoetin alfa administration/patient month. Also, serum hemoglobin, markers of iron stores (transferrin saturation and ferritin), IV iron dose, and cost were determined in relation to route of epoetin alfa administration.
Methods:
Data were gathered from 6 months prior (IV) to 12 months after switching treatment to SQ. The paired t-test and Wilcoxon signed-rank test were used to compare variables between pre-switch (IV) and post-switch (SQ) period.
Results:
The median cost (interquartile range) of epoetin alfa/patient-month decreased from (CAD508.3 [CAD349-CAD900.8]) pre-switch (IV) to (CAD381.2 [CAD247-CAD681]) post-switch (SQ) (P < .001), a decrease of 25%. The median epoetin alfa dose/patient-month reduced from (38 500 [25 714.3-64 166.5] international unit) pre-switch to (26 750.3 [17 362.6-48 066] IU) post-switch (P < .001), a decrease of 30.51%. The mean hemoglobin concentration (± standard deviation) for patients in both periods remained stable (103.3 ± 9.2 vs 104.3 ± 13.3 g/L, P = .34) and within the target range. There were no significant differences in transferrin saturation, ferritin, and IV iron dose and cost between the 2 study periods.
Limitations:
We were unable to consistently obtain information across all the sites on hospitalizations, inflammatory markers, nutritional status, and gastrointestinal bleeding. In addition, as our study sample was subject to survival bias, we cannot generalize our study results to other populations.
Conclusions:
We have shown that administering epoetin alfa SQ in HD patients led to a 30.51% reduction in dose and 25% reduction in cost while achieving equivalent hemoglobin levels. Given the cost sparing advantages without compromising care while achieving comparable hemoglobin levels, HD units should consider converting to SQ mode of administration.
Trial registration:
The study was not registered on a publicly accessible registry as it was a retrospective chart review and exempted from review by the Research Ethics Board of the former Regina Qu’Appelle Health Region.
What was known before?
Despite data to suggest that there is dose sparing advantage of subcutaneous (SQ) epoetin alfa when compared to intravenously (IV) epoetin alfa, in achieving equivalent hemoglobin levels, most of the Canadian dialysis units continue to use the IV route.
What this adds?
Our study adds to the evidence that SQ epoetin alfa has significant dose and consequently cost-sparing advantages without compromising clinical care and achieves similar hemoglobin levels.
Introduction
Erythropoiesis-stimulating agents (ESAs) were introduced in the treatment of anemia in 1989 and it immediately led to a marked decline in the number of blood transfusions and improved quality of life in patients across the spectrum of chronic kidney disease (CKD). However, higher doses of ESAs have been demonstrated to be independent predictors of mortality, cardiac events, and thrombovascular events across all hematocrit categories in hemodialysis (HD) patients.1-6 The cost of epoetin alfa is dose dependent and it additionally raises the overall cost of care of patients who require renal replacement therapy.7,8 Several studies from the mid 1990s have shown that the required doses of epoetin alfa were lower when administered subcutaneously (SQ).9,10 These studies led to guidelines by National Kidney Foundation (NKF, 1997) and Kidney Disease Outcomes Quality Initiative (KDOQI, 2001) recommending the use of SQ over intravenous (IV) as considerable cost savings could be achieved without compromising care.11,12 The much more recent Canadian Society of Nephrology Commentary on the 2012 KDIGO Clinical Practice Guideline for Anemia in CKD also advocates for use of SQ epoetin alfa. 13
In 2002, 7 cases of pure red cell aplasia (PRCA) were reported in Canada after 80 000 patient-years of exposures to the drug. 14 PRCA was felt to be linked with SQ administration of epoetin alfa. 15 As the number of cases continued to surge, almost all HD units in Canada converted patients to IV route of administration. These clinical occurrences led to change in guidelines in 2006 and led to HD units converting exclusively to IV route of administration.16,17 It was subsequently identified that polysorbate 80 from uncoated rubber stoppers in pre-filled syringes rather than the route of administration was the most plausible cause of immunogenicity.18,19 Once the manufacturer altered the syringes from uncoated to fluoro-resin-coated stoppers, it led to a substantial decrease in the incidence of PRCA. Despite near elimination of PRCA and the evidence that delivery of epoetin alfa via SQ is less expensive,20-22 most of the Canadian centers continue to use the IV route. 21
Given the dose sparing advantages of SQ epoetin alfa administration, we decided to gradually transition our patients to SQ and examined the cost of IV versus SQ treatment. The primary objective of this study was to determine the economic benefits of change in route of epoetin alfa administration from IV to SQ in HD patients at 4 major dialysis units in the province of Saskatchewan, Canada. The secondary objectives were (1) to determine the differences in epoetin alfa doses at the pre-switch (IV) and post-switch period (SQ) and (2) to determine serum hemoglobin concentration, transferrin saturation (Tsat), ferritin level, IV iron dose and cost in relationship to route of epoetin alfa administration.
Methods
Study Design and Patients
A policy decision was made to switch from IV to SQ epoetin alfa in March 1, 2015 at 2 HD sites in southern Saskatchewan (Regina General Hospital, Wascana Dialysis Unit, Regina) and at 2 sites in northern Saskatchewan (St. Paul’s Hospital [SPH] and SPH Community Renal Health Center, Saskatoon) in July 1, 2016. We conducted a retrospective observational study at the above 4 HD units in the Saskatchewan Health Authority among patients who transitioned from IV to SQ epoetin alfa between September 2014 and July 2017. The study was exempted from review by the Research Ethics Board (REB) of the former Regina Qu’Appelle Health Region (REB-17-105).
Patients who met all the following eligibility criteria were selected for our study. Inclusion criteria were (1) age >18 years, (2) receiving in-center HD for at least 6 months, (3) anemia of CKD requiring epoetin alfa therapy, and (4) on IV epoetin alfa for at least 6 months prior to study initiation. Exclusion criteria were (1) receiving HD with acute kidney injury, (2) patients not receiving epoetin alfa, (3) on darbepoetin irrespective of route of administration, (4) patients already receiving SQ epoetin alfa therapy, (5) receiving home HD or peritoneal dialysis, (6) documented hematologic condition that can cause anemia, and (7) died or underwent kidney transplant during the study period.
The Regina renal program has a collaborative prescriptive authority agreement for anemia management with certified renal pharmacists. Anemia is monitored based on KDOQI and Kidney Disease: Improving Global Outcomes (KDIGO) anemia guidelines from 2012.23,24 These guidelines recommend that ESAs should be initiated when hemoglobin is <100 g/L and that iron be administered if the Tsat is ≤30% and ferritin is ≤500 μg/L and considering the risk versus benefit of continuing iron when serum ferritin is >800 μg/L. Our institutional target hemoglobin levels based on the guidelines were set at 95 to 115 g/L. Our hemoglobin target remained the same throughout the entire study period. Epoetin alfa (Eprex®; Janssen-Ortho Inc., Toronto, Canada) was started after iron repletion at a dose of 50 to 100 international unit (IU)/kilogram (kg)/week and the dose was adjusted based on the response. Dialysis nurses administered IV or SQ epoetin alfa during HD sessions. The dose on conversion remained unchanged from IV to SQ. Patients also received IV iron sucrose (Venofer®; Luitpold Pharmaceuticals, Inc., New York, USA) and IV sodium ferric gluconate complex (Ferrlecit®; Sanofi-Aventis Inc., Quebec, Canada), as prescribed on HD sessions. None of our patients received oral iron.
Data Collection
The data were gathered from 6 months prior to 12 months after switching treatment, from the dialysis electronic medical records—Medical Information Quality System (MIQS, Denver, Colorado, USA). This included demographic information, post-dialysis weight, type of vascular access (HD catheter, arteriovenous fistula [AVF], and arteriovenous graft [AVG]), actual duration of each HD session and the number of sessions per month. Additionally, serum hemoglobin, markers of iron stores (Tsat and ferritin), parathyroid hormone (PTH), and measure of dialysis adequacy ([KT/V] and urea reduction ratio [URR]) was ascertained and averaged over a period of a month. The actual delivered doses of epoetin alfa, route of administration, frequency of administration, actual delivered doses of IV iron sucrose, and IV sodium ferric gluconate (administered during a HD session) was also ascertained from MIQS. We calculated the epoetin alfa and IV iron costs based on the provincial drug plan reimbursement rates in 2014 to 2017 which was CAD14.25 per 1000 IU for epoetin alfa, CAD0.375 per milligram (mg) for iron Venofer, and CAD0.274 per mg for iron Ferrlecit; costs of the medications did not change during the study period. To mitigate the effect of short-term variations, all repeated measures for each patient within a given quarter (12-week interval) were averaged to obtain one quarterly mean value.
Outcomes
The primary outcome was the difference in the median cost of epoetin alfa per patient per month between pre-switch period (more than 6 months) to 12 months post-policy switch. The secondary outcomes were the differences in median doses of epoetin alfa/IV iron per patient per month between pre- and post-switch periods.
Statistical Analysis
Months 1 to 6 were defined as the pre-switch period (P1 = period of IV usage) and month 0 (time of switch) and months +1 to +12 were defined as the post-switch period (P2 = period of SQ usage). We also further subdivided the P1 into 2 time periods (quarters) (pre-Q 1: [months −1 to −3], pre-Q2 [months −4 to −6]) and the P2 into 4 quarters (post-Q1 [months +1 to +3], post-Q2 [months +4 to +6], post-Q3 [months +7 to +9], post-Q4 [months +10 to +12]) to quantify temporal trends. Variables were reported as count (%), mean ± standard deviation (SD) or medians with interquartile range (IQR) as appropriate. For each patient, the mean dose per month was calculated pre-switch and post-switch. Similarly, for each patient, the mean cost per month was calculated pre-switch and also post-switch. Then, we performed Wilcoxon signed-rank test for median dose and cost per patient per month. Differences in other variables between pre-switch and post-switch period were assessed using the paired t-test and Wilcoxon signed-rank test, as appropriate. We also determined epoetin alfa dose and cost at 3 serum hemoglobin ranges: low (<95 g/L), target (95-115 g/L), and high hemoglobin (>115 g/L). Differences in variables across these 3 subgroups were assessed using Mann-Whitney U test. The significance level was set as α = .05. Statistical analyses were performed with Stata Statistical Software, Release 16 (StataCorp, College Station, Texas).
Results
Of 408 dialysis patients in the 4 units, 215 patients met the study criteria. Table 1 illustrates the baseline demographic and characteristics of patients. At baseline, the mean age ± (SD) was 58.66 ± 15.57 years and 56% were men. Mean total time on HD per month ± (SD) was 48.0 ± 8.81 hours. More than half of patients (57.68%) had AVF as vascular access for HD. Table 2 shows that the median cost (IQR) of epoetin alfa/patient-month decreased from (CAD508.3 [CAD349-CAD900.8]) pre-switch (IV) to (CAD381.2 [CAD247-CAD681]) post-switch (SQ) period (P < .001), a decrease of 25%. The median epoetin alfa dose/patient-month in the pre-switch period (38 500 [25 714.3-64 166.5] IU) decreased compared to the post-switch period (26 750.3 [17 362.6-48 066] IU) (P < .001), a decrease of 30.51%. The mean hemoglobin concentration for patients in both periods remained stable (103.3 ± 9.2 vs 104.3 ± 13.3 g/L, P = .34) and within the target range. Likewise, there were no significant differences in the levels of markers of iron stores (Tsat and ferritin) between the 2 study periods. Similarly, median IV iron dose administered in the 2 periods was not significantly different. The median cost of IV iron remained similar in P1 and P2. Additionally, URR and KT/V measures remained stable between pre- and post-switch period (Table 2).
Baseline Characteristics.

Note. Total number of patients: 215.
Comparison of Pre-Switch and Post-Switch Period.

Note. Pre-switch period = months −1 to −6 (intravenous epoetin alfa period); post-switch period: months +1 to+12 (subcutaneous epoetin alfa period); P = period; IQR = interquartile range; IV = intravenous; mg; CAD = Canadian dollar.
The pattern of changes in epoetin alfa dose and cost remained the same after subgroup analysis in pre- and post-quarters. Median epoetin alfa dose/patient-month decreased from (38 000 [24 000-61 333] IU) pre-Q1 to (28 000 [17 333-50 667] IU) post-Q1 (P = .008); similarly, there was a decrease in median epoetin alfa dose per patient-month from pre-Q2 (39 000 [25 714-65 000] IU) to post-Q2 (28 000 [17 333-49 619] IU) (P < .001). Epoetin alfa dose/patient-month started to decrease immediately following the switch in the route of administration and there was a steady decrease until the completion of the study period. As expected, the cost of epoetin alfa/patient-month proportionately declined subsequent to the switch (Figures 1 and 2). The proportion of patients successfully maintaining hemoglobin within the range of 95-115g/L was approximately similar across different months of the study (ranged from 58.8 to 66.9%) (Figure 3).
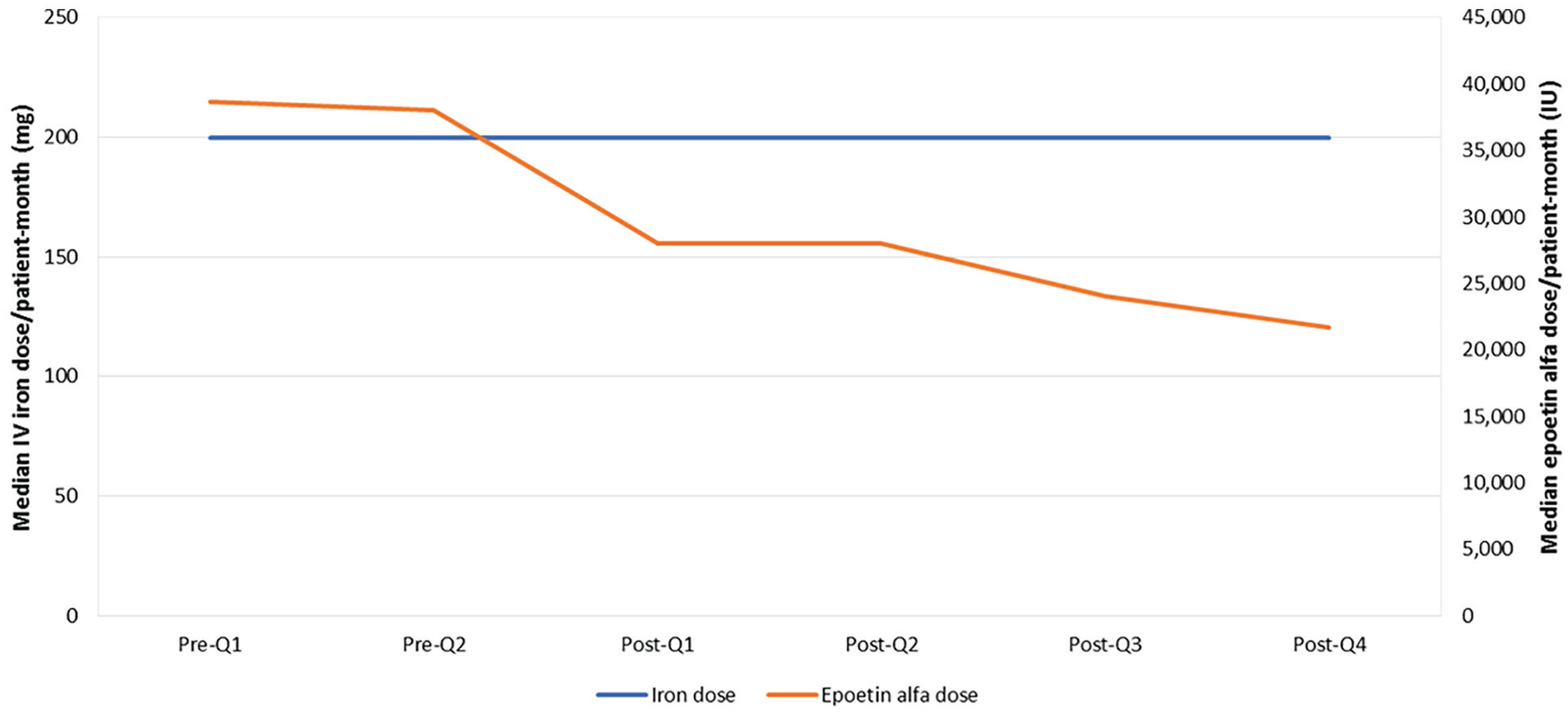
Epoetin alfa and intravenous iron doses/patient-month over the study period.

Epoetin alfa and intravenous iron cost/patient-month over the study period.
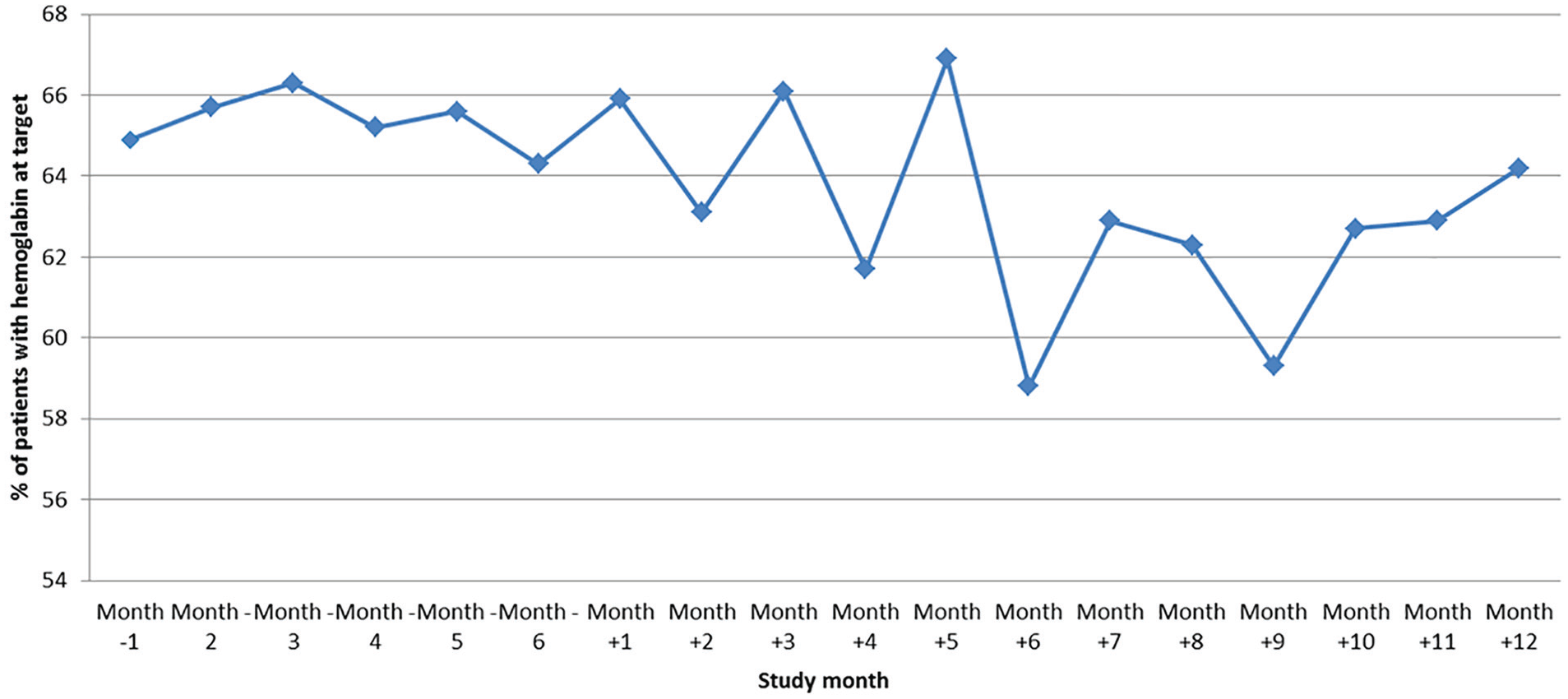
Proportion of patients with hemoglobin at target over the study period.
While the monthly median dose of IV iron, KT/V and URR in patients in pre-Q1 and those in post-Q1 were not significantly different, larger dose of epoetin alfa was required for patients at pre-Q1 compared to post-Q1 (at all hemoglobin levels: low, target, high). For instance, the median of epoetin alfa dose per month in patients with hemoglobin concentration at target in pre-Q1 (34 928.57 [21 785.71-53 000] IU) was significantly higher as opposed to those in post-Q1 (26 000 [17 333.3-43 333.3] IU; P < .001; Table 3 and Figure 4). Similarly, the monthly median dose of epoetin alfa required to maintain hemoglobin within the target range in patients in pre-Q2 was significantly higher (37 166.5 [23 333-64 285.71] IU) than patients in post-Q2 (26 285.71 [17 333-43 809.52] IU; P = .002 (Figure 4). Overall, patients at all hemoglobin levels (low, target, high) received significantly higher median epoetin alfa dose per month in pre-Q2 compared to patients in post-Q2. In addition, in the second quarter 25% and 75% quartile doses/patient-month at all levels of hemoglobin responses were lower when epoetin alfa was administered SQ rather than IV (Figure 4).
Pre- and Post-Quarter 1.

Note. Pre = pre-quarter 1 (months −1 to −3: the first 3 months of intravenous epoetin alfa); post = post-quarter 1 (months +1 to +3: the first 3 months of subcutaneous epoetin alfa); IQR = interquartile range; Hb = hemoglobin; g/L: gram/liter.

Median epoetin alfa doses/ patient-month in pre-quarters and post-quarters by hemoglobin levels.
Discussion
In this retrospective analysis, we report a 30.51% reduction in the dose of epoetin alfa when given SQ to achieve equivalent hemoglobin levels in patients undergoing HD. Epoetin alfa is an expensive medication and the price is directly proportional to the dose. While we predominantly looked at the economic impact of the route of administration, it is widely recognized that increased exposure of epoetin alfa to achieve hemoglobin targets are associated with increased risk of cardiac events, hypertension, and seizures.5,25,26 Additionally, in patients on dialysis, epoetin alfa has been shown to increase the risk of vascular clotting by stimulating vascular smooth muscle cell proliferation27-29 and increasing platelet activity.30-32 While no apparent reason has been shown to account for hypertension and cardiac events, it is possible that the non-erythropoietic impact of epoetin alfa such as increased blood viscosity and volume, particularly at high pharmacologic blood levels, could play a role. 33
It is well known that epoetin alfa pharmacokinetics and activity differ depending on the route of administration. Epoetin alfa has a half-life of 6 to 8 hours when given IV and a half-life of 19 to 24 hours when given SQ. 34 The longer half-life results in prolonged occupancy of erythropoietin receptors with increased proliferation of erythroid progenitors in the bone marrow and possibly decreased destruction of newly formed red blood cells. 35 Thus, it leads to more prolonged and sustained response, to attain equivalent hemoglobin levels.35-37 Multiple factors impact the level of hemoglobin apart from the route of administration. They include small solute clearance, 38 duration of therapy, 38 iron stores, 39 higher PTH levels, 40 inflammation, 41 and blood loss. 42 As our study took place in an era of proactive aggressive iron loading, we wondered if the reduction in epoetin alfa dosing coincided with higher iron stores. A meta-analysis of 7 studies showed that the use of optimal IV iron can reduce ESA requirements by 23% when compared to sub-optimal iron usage in adult HD patients. 43 However, data from our study revealed that the iron stores (TSAT and ferritin) were similar between the IV and SQ groups. There were also no differences in the duration of therapy and small solute clearance (KT/V). Similarly, there was no difference in the amount of blood lost through clotting of systems while on dialysis.
Several studies from the mid 1990s have shown that the required doses of epoetin were lower when administered SQ.9,10 These studies led to guidelines by NKF (1997) and KDOQI (2001) recommending the use of SQ over IV as considerable cost savings could be achieved without compromising care.11,12 However, the rise in the reported cases of PRCA led to a change in guidelines in 2006 and led to units changing exclusively to IV route. Despite caution suggested by Normal Hematocrit Study with higher doses of epoetin alfa, 26 there was a tendency by programs to prescribe higher doses of ESAs to increase exercise tolerance, reduce cardiac events, and improve quality of life. 44 In 2006, an analysis of a randomized controlled trial in patients with CKD showed that higher epoetin alfa doses led to increased incidence of cardiac events, strokes, and clotting of the arteriovenous access. 45 The realization that higher epoetin alfa exposure led to worse outcomes led to a change in guidelines for hemoglobin targets, but there was no consensus on epoetin alfa doses to achieve those targets. Wright et al in a study from 2015 showed that doses of >300 IU/kg/week to achieve therapeutic hemoglobin were more likely to lead to adverse events. 46 Despite this compelling evidence, very few centers have changed their practice to SQ administration and it has been largely driven by nursing convenience and patient comfort. However, patients starting dialysis from the CKD clinics might find the transition seamless compared to the ones who are on HD and receiving IV epoetin alfa. The concern about pain might be exaggerated as Kaufman et al showed that only a minority of patients had greater than mild discomfort when the medication was administered SQ. 35 Patient acceptance with injection site discomfort and education regarding better clinical outcomes on lower doses of epoetin alfa are likely to be key factors for a successful transition to SQ.
The typical costs (CAD) of epoetin therapy run between 5000 to 10 000 per patient per year.7,8 We show a 27% reduction in (mean) dose and 28% reduction in (mean) epoetin alfa cost. Our data are approximately similar to Wright et al who showed a 25% reduction in dose, but lower than from the Department of Veterans Affairs trial which showed a 32% reduction in cost.35,46 Of the 107 patients treated by the SQ route, the average weekly dose of epoetin was 32% lower than treated by the IV route (mean ± SD, 95.1 ± 75.0 vs 140.3 ± 88.5 IU/kg of body weight per week, P < .001); 99% of the participants in the Veterans Affairs study were men and the average difference in the dose was 2671 IU/week. 35 Similarly, 64 patients in a study from Manitoba, Canada when converted from SQ to IV epoetin alfa demonstrated an increase in the dose of epoetin from 7567.7 to 10 229.2 IU/week. 47 From the same center, a study by Raymond et al compared SQ to IV epoetin alpha and demonstrated the dose increased by 26% (mean ± SD, 10 425 ± 7330 vs 13 125 ± 8638 IU/week, P < .0001). 22 Moist et al compared 303 patients who were switched from SQ to IV epoetin alpha and showed an increase in the dose of 24.5 IU/kg/week. 21 McFarlane et al. looked at the cost at a single site in Ontario, Canada and reported an additional cost of CAD66 500 per 100 patients when converted from SQ to IV. 20 The (mean) cost of epoetin alfa per patient per year in our study when given IV was CAD8088 (CAD) and was once converted to SQ was CAD5817 while achieving equivalent hemoglobin levels, a saving of CAD2271 per year. Our results are nearly similar to the savings shown by Kaufman et al (USD1110 per patient per year, which is equivalent to CAD2276 in 2019). 35 Based on these values, if we extrapolate our savings to 900 prevalent patients to SQ epoetin alfa, we can realize a cost saving of CAD2 043 900 (CAD) per year. It is important to reiterate that the reduction in the mean dose of epoetin alfa per patient per month on conversion remained similar (IV vs SQ) in all the hemoglobin subcategories: <95 g/L (65 941 vs 52 717 IU), 95 to 115 g/L (42 120 vs 29 619 IU) and (35 289 vs 17 651 IU) for hemoglobin >115 g/L. Furthermore, the mean dose per patient per month and cost of epoetin alfa reduced immediately after conversion (38 007 IU) and continued to persist till the fourth quarter (29 352 IU) in the last quarter suggestive that epoetin alfa accumulates when given SQ and leads to consistently low doses.
Our study has a few limitations. We were unable to consistently obtain information across all the sites on hospitalizations, inflammatory markers, nutritional status, and gastrointestinal bleeding. The presence of the data would have further strengthened our findings. We did not capture data on demographics, co-morbidities, and laboratory values which would have been helpful in interpretation of the results. In addition, our study sample was subject to survival bias. We cannot generalize our study results to other populations as we only selected patients who were alive over the 12-month post-switch period. Our study sample might be under-representative of the HD population who switched to SQ epoetin alfa. We might have obtained different study findings if we have included both alive and deceased patients in the data analysis.
Conclusions
We have shown that administering epoetin alfa SQ in HD patients led to a 30.51% reduction in dose and 25% reduction in cost while achieving equivalent hemoglobin levels. Given the cost sparing advantages without compromising care while achieving comparable hemoglobin levels, HD units should consider converting to SQ mode of administration.
Footnotes
Acknowledgements
The authors wish to acknowledge the contribution of Verna Bloom and Holly Haugen from St. Paul’s Hospital, Saskatoon and Natalie Sinclair from Regina General Hospital.
Author Contributions
B.P. conceived and designed the study. He assisted with the drafts and edited the final manuscript. M.J. wrote the initial draft and assisted with data analysis. J.T., L.G., and J.K. assisted with manuscript drafts. F.A. performed the statistical analysis. All authors read and approved the final manuscript. Each author contributed important intellectual content during manuscript drafting or revision, accepts personal accountability for the author’s own contributions, and agrees to ensure that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Ethics Approval and Consent to Participate
The study was exempted from review by the Research Ethics Board (REB) of the former Regina Qu’Appelle Health Region (REB-17-105).
Consent for Publication
Not applicable as there is no patient identifying information in this manuscript.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.