
Abstract
Background:
Prolonged wait times are known barriers to accessing nephrology care for patients needing more urgent specialist services. Improved process and standardized triage systems are known to minimize wait times of urgent or semi-urgent care in health care disciplines. In Central Zone (CZ) renal clinic, mean wait times for urgent (P1) and semi-urgent (P2) referrals were prolonged before 2014. We also observed prolonged wait times for elective (P3-P5) categories. Improving wait times was identified as an access to care quality improvement focus in CZ renal clinic of the Nova Scotia Health Authority (NSHA).
Objectives:
To describe our new referral process and new triage system, and to examine their effect on number of referrals wait-listed and mean wait times.
Design:
A quasi-experimental design was used.
Setting:
Halifax, Nova Scotia, Canada.
Participants:
Patients referred to Central Zone Renal Clinic between 2012 and 2018.
Measurements:
A time series of referral counts and wait times for each triage category were measured before our interventions and after implementing our interventions.
Methods:
We reviewed our referral processes to identify gaps leading to prolonged wait times. On January 1, 2014, we implemented new administrative procedures: pretriage (standardized referral information form and staff training), triage (standardized clinic intake criteria and new triage guidelines), posttriage (protecting clinic spots for urgent and semi-urgent referrals, wait-list maintenance, and increasing new referral clinic capacity). Data were collected prospectively. Descriptive analysis on mean wait times was done using run charts.
Results:
A 33% reduction in total number of referrals wait-listed was observed over 4.5 years after intervention. Descriptive analysis of the urgent and semi-urgent categories (P1 and P2) revealed a significant shift of mean wait times on run charts after the interventions. Target wait time was achieved in 94% of P1 category and 78% of P2 category.
Limitations:
This type of study design does not exclude confounding variables influencing results. We did not explore stakeholder satisfaction or whether the new referral process presented barriers to resending referrals that had insufficient triage data. The long-term sustainability of adding demand-responsive surge clinics and opportunity cost were not assessed. Our referral process and triage system have not been externally validated and may not be applicable in settings without wait-lists or settings that use electronic, telephone or telemedicine consults.
Conclusion:
Our selective intake of referrals with adequate triage information and referrals needing nephrology consult as defined by our clinic intake criteria reduced number of referrals wait-listed. We saw improved wait times for urgent and semi-urgent referrals with these categories now falling within target wait times for the vast majority of patients. The work of this improvement initiative continues especially for the lower-risk triage categories.
Trial registration:
Not applicable as this was a Quality improvement initiative.
Background
Chronic kidney disease (CKD) is prevalent worldwide. Global CKD prevalence rates have been reported to be 13.4% for stages 1 to 5 and 10.6% for stages 3 to 5. 1 In Canada, nondialysis CKD (stages 1-5 and proteinuria) prevalence was estimated to be 12.5% between 2007 and 2009, representing approximately 3 million Canadians. 2 More recently, the prevalence of stage 3 to 5 CKD in primary care in Canada was estimated at 7.19%, with the highest prevalence occurring in rural settings and among those with multiple comorbidities, especially diabetes mellitus and hypertension. 3 The CKD has consequences with respect to increased cardiovascular morbidity and mortality4-8 requirement for renal replacement therapy (RRT)7,9 and associated burdens and health care costs.10,11
Patients with CKD are often referred from primary care and other specialties to CKD interdisciplinary clinics in Canada. 12 Prolonged wait times have been identified as a barrier to accessing health care system in Canada. 13 In the era of routine estimated glomerular filtration rate (eGFR) reporting by laboratories, earlier recognition of CKD, increased nephrology wait times, and number of unnecessary referrals have been observed, which can affect timely access to nephrology care for patients needing more urgent specialist services.14,15 Improvements in process deficiencies and implementation of triage systems are known to minimize wait times of urgent and semi-urgent care in health care disciplines.13,16,17 Little is known about the potential benefits of standardized triage system and process improvements in nephrology ambulatory care clinics in Canada.18-20 A central referral system and triage guidelines were in place in our renal clinic for several years. In Nova Scotia (NS), automated eGFR laboratory reporting was rolled out in phases throughout the province between 2006 and 2014. The Nova Scotia Renal Program (NSRP) renal clinic referral pathway first became available on a web platform as a reference for health care providers in 2009.
We identified increased CZ renal clinic wait times as an access to care focus for ongoing improvement. Urgent and semi-urgent referrals were of priority concern.
Objectives
In this article, we describe how, beginning on January 1, 2014, Nova Scotia Health Authority (NSHA) Central Zone (CZ) Renal clinic (1) implemented new clinic intake criteria and updated our clinic referral pathway, (2) implemented new standardized triage procedures, and (3) increased capacity to see new referrals. We report the effects of these combined changes on the mean wait times in CZ Renal Clinic.
Methods
Study Population
NS is 1 of 3 Maritime provinces in Canada with a population of approximately 938 972 residents in 2014, which increased to 955 376 by 2018 (1.7% growth). 21 In April 2015, all health authorities in the province were amalgamated into a provincial single publicly funded health authority, the NSHA with 4 geographic management zones: CZ (Halifax area, Eastern Shore, and West Hants), Eastern Zone (Cape Breton, Guysborough, and Antigonish areas), Northern Zone (Colchester-East Hants, Cumberland, and Pictou areas), Western Zone (Annapolis Valley, South Shore, and South West).
The NSHA NSRP has 3 renal centers, namely, Halifax (CZ, Northern Zone), Yarmouth (Western Zone), and Sydney (Eastern Zone). Each renal center primarily sees referrals originating within its zone, although there are areas of overlap at zone boundaries. The zonal distribution of nephrology referrals did not substantially change during the course of this quality improvement initiative which was performed in the CZ Renal Clinic, which is located in a teaching hospital.
Process-Mapping
We outlined a process map, including timelines for new clinic referrals from the point of receiving a referral, administrative procedures after receiving a referral (pretriage, triage, posttriage), and appointment bookings to identify opportunities for improvement and inform our interventions. This led to the identification of reasons for prolonged wait times (Figure 1), areas of possible intervention (Figure 2), and a new process map (Figure 3).

Reasons for prolonged wait times.

Interventions for wait-time improvement.

Referral process map started on January 1, 2014, CZ Renal clinic.
Interventions
Pretriage
All new clinic referrals were received into a central office using a single fax number. A standardized clinic intake form was created to ensure the referral provided adequate information for triaging (Table 1). Missing information was requested from referring physicians using a standardized letter. Wait time was defined from the date of receipt of adequate triage information to the date of clinic visit. Previously, wait time was defined as receipt of any referral information, irrespective of adequacy for triage, and all referrals were wait-listed. Administrative staff were trained to identify high-risk flags for all referrals (including those with inadequate triage information) that would require urgent triage nephrologist review or direct physician-to-physician communication.
Referral Information (Triage Data) for Renal Clinic, Central Zone Nova Scotia Health Authority.

Note. eGFR = estimated glomerular filtration rate; CO2 = carbon dioxide; CT = computed tomography.
Triage Procedures
Triage was distributed among all 11 nephrologists participating in our clinic. Clinic intake criteria were derived by consensus using existing practice guidelines9,22 and clinical experience to determine whether referrals required nephrology consultation. Referrals deemed as not meeting clinic intake criteria were returned to referring physician with reasons for why the referral did not require nephrology consultation, general management advice, resources for CKD monitoring and management, and guidelines for when to refer back to renal clinic as described in our referral pathway (Supplemental Figure 1). 23 In cases of ambiguity, or at the discretion of the triage nephrologist, the referring physician was contacted for further discussion. Referring physicians were invited to call the triage nephrologist if there were further questions or concerns. Referrals triaged to be seen had to meet any one of our intake criteria (Table 2) which were published on the NSHA Renal Program website. 23
Intake Criteria for Renal Clinic, Central Zone Nova Scotia Health Authority.
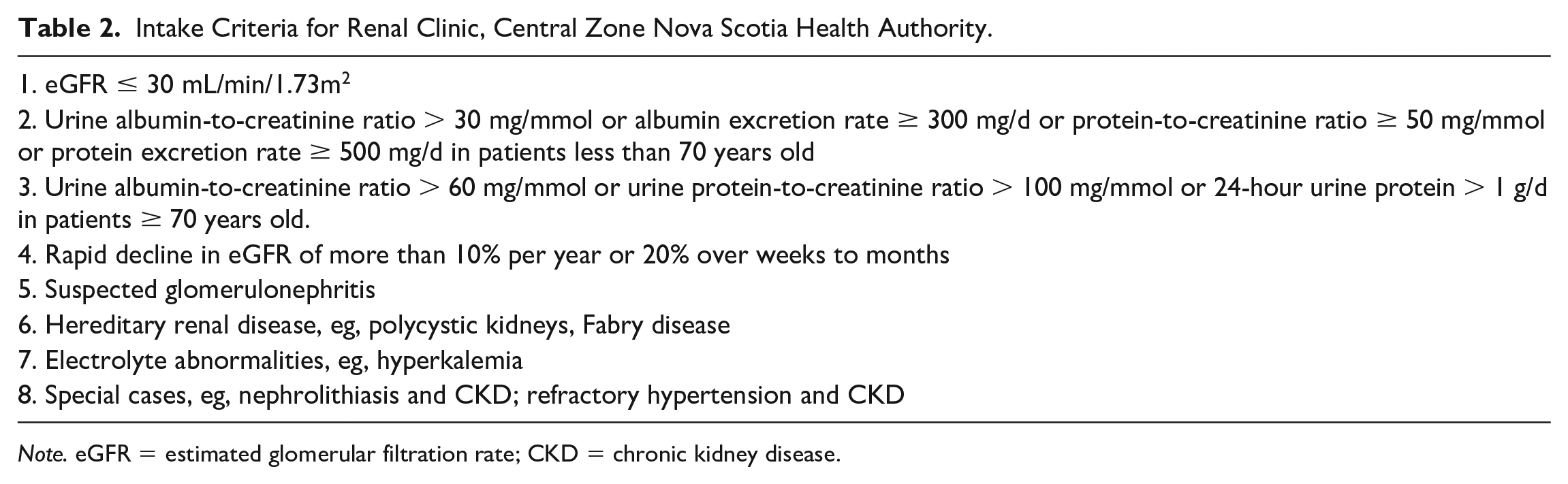
Note. eGFR = estimated glomerular filtration rate; CKD = chronic kidney disease.
Referrals meeting clinic intake criteria were prioritized using our new triage system (Supplemental Table 1). The new triage system (5 categories) was built on modifying the previous triage system (4 categories) to reflect actual triage practices. Criteria for each triage category and appropriate target wait times were defined by consensus among nephrologists to improve consistency of prioritization among various triage nephrologists. In June 2015, we added the Kidney Failure Risk Equation (KFRE) for stage 3-5 CKD patients as a supplementary risk assessment tool to guide triaging; this was subsequently shown in studies to significantly decrease wait times.20,24,25 A 3% risk of kidney failure in 5 years has been proposed, as a threshold for referring to nephrology, and is more discriminating than eGFR criteria alone. 26 In our clinic, patients whose 5-year risk of kidney failure was estimated to be less than 5% were deemed low risk, and could be considered for management in primary care at the discretion of the triage nephrologist. Monitoring for disease progression was requested of referring physicians, who were invited to re-refer with updated information if renal status changed. We reviewed referrals received between January 1, 2014, and December 31, 2014, that did not meet our clinic intake criteria to see whether they were re-referred and triaged to be seen in the subsequent 5 years. We assessed the number of these presenting as late referrals using a late referral definition of 180 days until start of RRT.
Posttriage
Administrative staff aimed to book the referral with the next available nephrologist (or previous nephrologist if it was a re-referral) within target wait time for the triage category. Approximately 3 to 4 clinic appointments were always protected for urgent (P1) and semi-urgent (P2) referrals every week, and if they were not used, could be filled with lower priority referrals.
Patients received written appointment notifications through the mail, and a telephone reminder the day before their appointments. Referrals for patients who missed their initial appointments and did not request rescheduling were returned to referring physician with an invitation to re-refer. Urgent (P1) and semi-urgent (P2) referrals were allowed to miss 3 appointments, elective (P3 and P4) referrals were allowed to miss 2 appointments, and elective (P5) referrals were allowed to miss 1 appointment before the referral was canceled and returned to the referring physician with an invitation to re-refer. The wait-list was reviewed every 6 months by a nephrologist and administrative staff, and deceased patients were removed. Outlying referrals that had been waiting much longer than other referrals in their triage category were periodically reviewed to determine cause for the delay.
To increase clinic capacity for new referrals, we sought to reduce follow-up appointments for low-risk patients whose care could be adequately provided by primary care. Nephrologists were asked to analyze each returning patient for stability and risk of CKD progression. Stable and low-risk patients had their care transitioned back to primary care or where needed to nephrology nurse practitioners in collaborative practice with our group.
A demand-responsive strategy of adding extra clinics to accommodate surges in referral numbers and to clear backlogged referrals was taken. This was done in August 2014 for semi-urgent (P2) referral number surge, August 2017 for increasing P2 wait times, and October 2016 to address backlogged elective (P3) referrals. In July 2017, we introduced new referral quotas for each nephrologist to cope with increased background demands across all triage categories. The quotas were calculated based on expected new referral demands for the upcoming 6-month block based on historical data, and increased by 5% to account for no shows that could not be replaced. The quota was adjusted for full-time or part-time status and other clinical service obligations. Quotas per nephrologist varied from 25 to 50 new referrals per 6-month period. Prior to the quota allocation system, nephrologists booked new referrals in their weekly schedules based on availability of human and clinic space resources; referral demands were not factored in a systematic fashion among all clinicians.
Data Analysis
The data were collected prospectively. Wait-time analysis included quarterly data over a period starting July 1, 2012, and ending September 30, 2018, as obtained from the NSHA Patient Health Systems (PHS). Wait-time analysis did not extend past September 30, 2018, due to major changes in pretriage administrative procedures in Q3 2018/19 such that study conditions were not comparable with previous times. Descriptive analysis was done using run charts.
Results
Wait Times
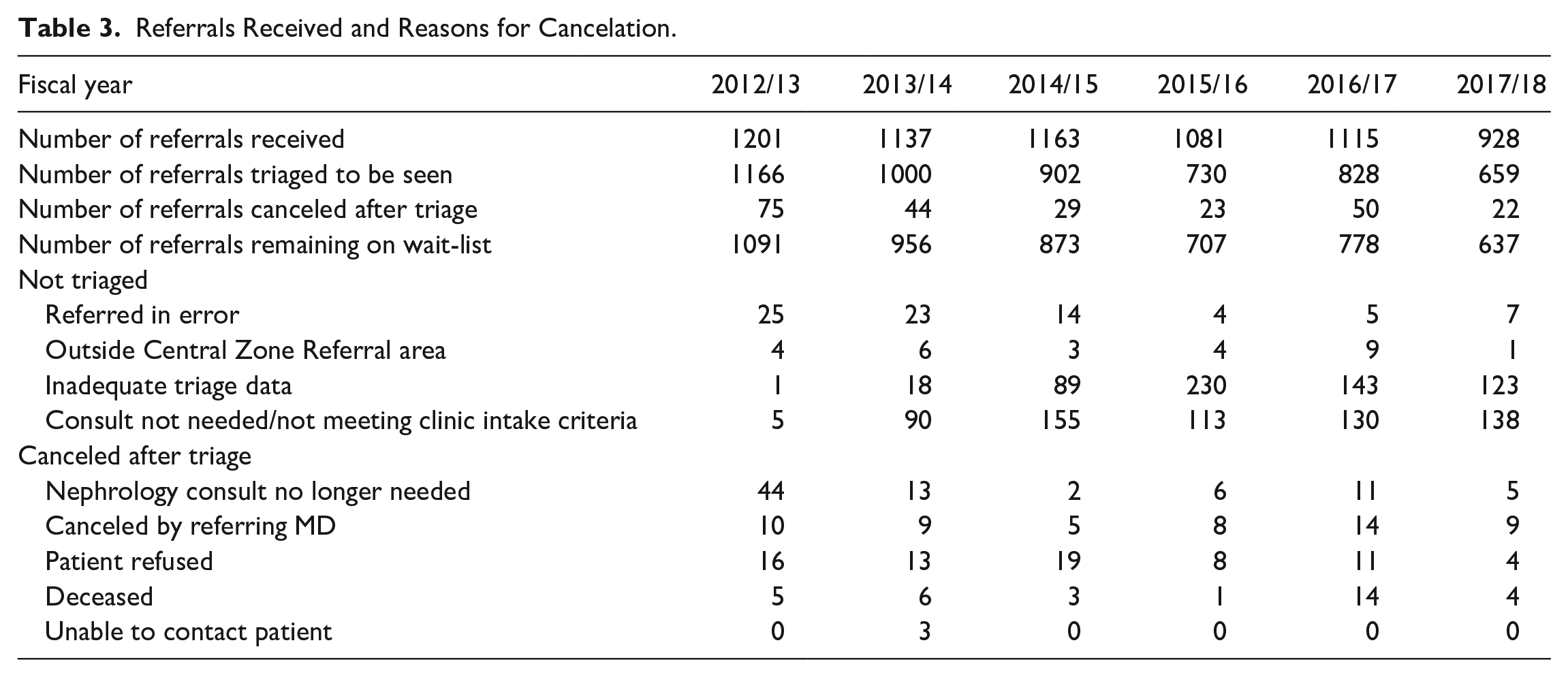
We saw 33% reduction in total number of referrals wait-listed between March 31, 2014, and March 31, 2018 (Figure 4). The reduction in number of wait-listed referrals was due to not wait-listing referrals that did not meet our clinic intake criteria and referrals that were sent with inadequate triage information (Table 3). The P3 category represented the highest frequency of referrals, followed by P2 and P4, whereas the lowest frequency of referrals was seen for P1 and P5 categories (Figures 5-9 and Supplemental Table 3).

Number of new referrals wait-listed to be seen in renal clinic, 2012-2013 to 2018-2019, CZ of NSHA.
Referrals Received and Reasons for Cancelation.

Mean wait time for urgent (P1) referrals from July 1, 2012, to September 30, 2018.

Mean wait time for semi-urgent (P2) referrals from July 1, 2012, to September 30, 3018.

Mean wait time for elective (P3) referrals from July 1, 2012, to September 30, 2018.

Mean wait times for elective (P4) referrals from July 1, 2012, to September 30, 3018.

Mean wait time for elective (P5) referrals from July 1, 2012, to September 30, 2018.
Descriptive analysis revealed a significant shift of mean wait times on run charts of the P1 and P2 categories after the implementation of the interventions (6 or more consecutive data points below the target wait times; Figures 5 and 6). 27 After January 1, 2014, there were 17/18 (94%) data points within target for P1 category and 14/18 (78%) data points within target for P2 category. There was no significant shift of mean wait times for the elective (P3-P5) categories (Figures 7-9). Only 3/18 (16.7%) data points fell within target for P3 category, 0/18 data points fell within target for P4 category, and 1/18 (5.5%) data points fell within target for P5 category. Our no show rate remained stable at 2% to 6.8% since October 2016 when we started tracking it.
Follow-up
Of 165 referrals that were deemed as not requiring nephrology consultation in calendar year 2014 (posttriage system implementation), we found 8 (4.8%) were subsequently re-referred to our clinic in the 5 years of follow-up. Of these re-referrals, 1 patient subsequently required ongoing renal clinic follow-up. Five were seen once in renal clinic and discharged due to stability. Two re-referrals were felt not to need nephrology consultation due to stability and advanced palliative status from comorbid disease. None of the 165 patients triaged as not needing nephrology consultation in 2014 received RRT within the subsequent 5-year observation.
Discussion
Summary
After implementation of our standardized referral information and clinic intake criteria, we observed a 33% reduction in referrals wait-listed for appointments. This was mostly driven by fewer referrals being triaged as a result of inadequate triage information, and a decrease in the number of low-risk referrals being triaged to be seen. There did not appear to be a detrimental effect of deferring nephrology consultation in 5-year follow-up of the initial cohort of low-risk referrals which was not seen. We observed an improvement in mean wait times for urgent and semi-urgent triage categories following interventions that were designed to improve triage efficiency, accuracy, and increase capacity to see referrals.
Interpretation
Centralization of referrals, where referrals are assigned to the first available nephrologist based on priority, has the benefit of controlling wait times for more urgent patients, as higher urgency patients can be seen sooner than in traditional first-come first-served specialist-specific referral systems.17,28 Directed referrals were permitted in our clinic, provided the consultation could be done within target wait time for that triage category. Defining maximum wait times for each triage category can reduce prolonged wait times for lower urgency patients. 29
By standardizing the minimum referral intake information required, we were able to improve the quality of referral information provided and perform timely triage and wait listing. Under the previous system, inadequate triage information resulted in delays in identifying those that did not need clinic appointments, and often this was discovered too late to replace the referral with another that needed to be seen.
There is considerable variation in referral criteria for interdisciplinary CKD clinics throughout Canada.12,30 A recent study showed that not all nephrology referrals recommended by current clinical practice guidelines appear to derive the same benefit from nephrology consultation. 31 We found that a significant proportion of referrals did not meet our clinic intake criteria which target moderate- and high-risk individuals who would benefit from nephrology consultation. We believe this approach allowed nephrology resources to be directed toward higher risk patients who could then be seen in a more timely fashion as has been observed in other Canadian CKD clinics. 20
In the 5-year follow-up period of our study, we found that 4.8% of patients who did not meet our clinic intake criteria were subsequently re-referred. Of these, none presented as late referrals requiring dialysis in less than 6 months from first nephrology exposure. This suggests that a substantial number of patients with mild abnormalities, stable disease, or competing mortality risk who are referred to renal clinic could receive appropriate management in primary care.
Current practice guidelines provide nephrology referral recommendations; however, evidence-based target wait times have not been established.9,22 Consensus-based benchmark wait times were associated with improved access to outpatient nephrology consultations in British Columbia, particularly for highest priority patients suggesting an influence of triaging behavior. 19 Our triage guidelines were implemented to reduce variability in referral prioritization by various users, and target wait times were derived by consensus among participating nephrologists.
The benefits we saw in wait times for urgent (P1) and semi-urgent (P2) categories were generally maintained despite a variation in the number of practicing nephrologists over the course of the study. Better quality of referral information and more precise triage criteria resulted in fewer referrals being classified as urgent or semi-urgent. Some referrals that would have been previously been triaged P2 were likely classified as P3 category. The creation of a P4 category allowed better discrimination among elective referrals, and prevented oversubscribing to the P3 category due to increased confidence that referrals which could wait longer than 90 days (P3) could still potentially be seen sooner than 365 (P5) days.
We observed as others have in other outpatient clinical settings that demand for nephrology services fluctuates and can influence wait times if backlogs accumulate. 32 By adding extra clinics in response to P2 referral number surges (Q2 2014/15), P2 wait times remained within target, and the P3 wait list likely also benefited as wait times remained at target for this group, although the effect was not sustained. Adding surge clinics to address the P3 backlog (Q3 2016/17) maintained wait times for that category; however, this effect was not sustained. The frequency and size of surge clinics that was needed challenged the balance with clinical service demands in other CKD care areas such that their long-term use was not sustainable.
There was no effect of implementing quotas on urgent and semi-urgent referrals, probably due to the fact that these referrals were always seen relatively quickly. Although sufficient follow-up was not available, quotas may have a positive effect on elective P3 and P4 wait times. The effect of quotas may not have been fully realized due to simultaneous reduction in number of full-time nephrologists after their implementation.
In system changes affecting multiple stakeholders, we encountered a period of adjustment, and there were learning curves to accommodate for all involved. Communication with referring clinicians on applicable changes was triggered on a case-by-case basis, usually by a referral that was deemed not to require nephrology consultation or a referral that was sent with inadequate information. This was usually done in writing and where needed by telephone, both of which offered an opportunity for further discussions with referring clinicians. Although not a significant barrier, nephrologists had to become accustomed to the new clinic intake criteria, and both nephrologists and their long-term stable CKD patients had to be comfortable with being discharged from clinic. The frequency with which stable CKD patients were discharged or discharged and subsequently re-referred was not tracked, and therefore, the effectiveness of this strategy on improving wait times is unknown.
Limitations
We did not explore the frequency with which requested referral information presented a barrier to sending a new referral or resending a referral that had previously been canceled. We did not collect data on outcomes of referrals that were not wait-listed due to inadequate triage information. Further to this work, in July 2018, in collaboration with family physician leaders, we developed a nephrology referral form with identical referral information elements, and this was not felt to be onerous by collaborating primary care leaders (Supplemental Table 2). The referral form is being implemented among primary care providers. It includes check boxes of the minimum triage information, laboratory data, and diagnostic imaging reports required. More recently, we are piloting a process of obtaining missing triage laboratory data by sending requisitions directly to the patient after receiving a referral, to reduce chances of missing referrals that need to be seen.
We did not assess compliance with pretriage, triage, and posttriage procedures. It is possible that deviation from these procedures influenced wait times. Other factors contributing to increased wait times such as process inefficiencies, service disruption, and patient scheduling preferences were not studied here.33,34
Differences in the way wait times were measured before and after our quality improvement initiative would have influenced wait times for elective triage categories (P3-P5), as these referrals were only wait-listed after receipt of adequate triage information in the new era. However, the change in how wait times were measured likely had minimal to no effect on urgent and semi-urgent (P1-P2) referrals as high-risk referrals were triaged expeditiously in the same manner pre- and postimplementation of our initiative. Triage of high-risk referrals mostly occurred within a day of referral receipt in both eras, often with efforts made by nephrologists to contact referring physicians by telephone if further information was required.
The opportunity cost of surge clinics on other clinical services, administrative and academic pursuits, and ability to schedule return appointments were not assessed. Ultimately increasing nephrology resources is required for sustainability. The impact of adding the KFRE to our triage procedures on our wait times was not assessed. The KFRE is less applicable for referral indications such as glomerulonephritis, polycystic kidney disease, and recurrent stone disease, and therefore, there remains a role for alternate triage system in these conditions. Telephone consultation was occasionally used for select referrals in our center although frequency was not captured. Our triage and booking system were not validated externally and may not be generalizable to other centers, e.g., those that use electronic referrals, telephone and electronic consultations, and telehealth/telemedicine.35-38 Patient, referring physician, and nephrologist satisfaction with the referral and triage process were not formally assessed, although occasional feedback on a case-by-case basis was received.
Conclusion
There is a global increased demand for nephrology services and gaps in services, facilities, and nephrology workforce. 39 In a resource-limited environment, timely access to nephrology services is a priority for those patients needing it to avoid adverse outcomes. We found that accepting referrals with adequate triage information, standardizing clinic intake criteria, more precise triage criteria, demand-responsive surge clinics improved access for higher risk (P1 and P2) referrals, with the vast majority of these now falling within target wait times. This work of improving access to care continues, especially for elective categories (P3-P5) needing nephrology consultation. Engagement with all stakeholders, including patients, referring clinicians, and nephrologists on strategies to address wait times for these categories, and gathering structured feedback and satisfaction with current processes are vital aspects of furthering this work.
Supplemental Material
Appendix_Figure_1 – Supplemental material for The Impact of a New Triage and Booking System on Renal Clinic Wait Times
Supplemental material, Appendix_Figure_1 for The Impact of a New Triage and Booking System on Renal Clinic Wait Times by Penelope S. Poyah and Tabassum Ata Quraishi in Canadian Journal of Kidney Health and Disease
Supplemental Material
Appendix_Table_1 – Supplemental material for The Impact of a New Triage and Booking System on Renal Clinic Wait Times
Supplemental material, Appendix_Table_1 for The Impact of a New Triage and Booking System on Renal Clinic Wait Times by Penelope S. Poyah and Tabassum Ata Quraishi in Canadian Journal of Kidney Health and Disease
Supplemental Material
Appendix_Table_2 – Supplemental material for The Impact of a New Triage and Booking System on Renal Clinic Wait Times
Supplemental material, Appendix_Table_2 for The Impact of a New Triage and Booking System on Renal Clinic Wait Times by Penelope S. Poyah and Tabassum Ata Quraishi in Canadian Journal of Kidney Health and Disease
Supplemental Material
Appendix_Table_3 – Supplemental material for The Impact of a New Triage and Booking System on Renal Clinic Wait Times
Supplemental material, Appendix_Table_3 for The Impact of a New Triage and Booking System on Renal Clinic Wait Times by Penelope S. Poyah and Tabassum Ata Quraishi in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
Data used in this article are from the Central Zone Renal Clinic Referral Repository and Nova Scotia Health Authority (NSHA) appointment scheduling system Patient Health Systems (PHS) which contain patient record–level information such as when the referral was received, triaged, wait time to initial consultation, appointments scheduled, and return visits. Data on cancelations, no shows, and when the referral is wait-listed for an appointment are also captured. We acknowledge and appreciate the contributions and support of Central Zone (CZ) nephrologists, the NSHA Renal Program, and administrative staff in the support of this quality improvement initiative.
Ethics Approval and Consent to Participate
Due to this project being a quality improvement initiative, minimal to no risk to patients, and aggregate data presentation, patient consent was waived, and it met exemption criteria from formal Research Ethics committee review in our institution.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
Data supporting the findings of this article is not publicly available.
Author Contributions
P.S.P. made a substantial contribution to the design of the work, helped gather and interpret the data, created the figures, and drafted and revised the article critically for important intellectual content. T.A.Q. helped gather the data, create the figures, interpret the data and drafted the abstract.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.