
Abstract
Background:
Fatigue and its negative impact on life participation are top research priorities of people on chronic dialysis therapy. Energy management education (EME) is a fatigue management approach that teaches people to use practical strategies (eg, prioritizing, using efficient body postures, organizing home environments) to manage their energy expenditure during everyday life.
Objective:
The aim of this study is to explore whether EME is associated with improvements in fatigue and life participation in adults on chronic dialysis.
Design:
Five single-case interrupted time-series AB studies, and follow-up qualitative interviews.
Setting:
The hemodialysis and peritoneal dialysis units at an academic hospital in Toronto, Canada.
Patients:
In total, 5 patients on chronic dialysis therapy were purposively selected to represent diversity in age, gender, and modality.
Measurements:
Brief questionnaires assessing fatigue and life participation were administered weekly during the baseline and intervention periods. Additional validated questionnaires (the Fatigue Impact Scale, 36-Item Short-Form Health Survey [SF-36] Vitality Scale, and Canadian Occupational Performance Measure) were also administered at baseline and post-intervention.
Methods:
All participants underwent “The PEP Program,” a personalized, web-supported EME program designed to meet the needs of people on dialysis. During the program, participants complete 2 brief web modules about energy management, and then use energy management principles and a problem-solving framework to work on 3 life participation goals during sessions with a trained program administrator. Data were analyzed using visual analysis and the Tau-U statistic for the weekly time-series data, and thematic analysis for the qualitative interviews.
Results:
Three of 5 participants displayed a consistently positive response to the Personal Energy Planning (PEP) program across multiple measures of fatigue and life participation. Tau-U effect size estimates ranged from small to moderate, according to the time-series data. All 5 participants expressed that the program had benefited them in qualitative follow-up interviews, with the most common reported benefit being that the program made day-to-day activities easier. The format of the program was also said to be feasible and convenient.
Limitations:
An exploratory, proof-of-concept study that used a small set of participants and lacked an active control comparison.
Conclusions:
The PEP program might have potential for improving fatigue-related outcomes in people on chronic dialysis. Larger, controlled studies of the program are warranted.
What was known before
Fatigue is a highly common symptom of end-stage renal disease (ESRD) and is a top research priority of patients. Treatments to mitigate fatigue and its negative impact on life participation in this population are currently limited. Energy management education (EME) is an approach to fatigue management that has been found to be effective in other chronic disease populations, but it has never been investigated in the ESRD population.
What this adds
This proof-of-concept study demonstrates the potential for EME to improve fatigue and life participation outcomes in the ESRD population. It shows improved life participation and fatigue outcomes in 3 of 5 participants on chronic dialysis who complete an EME program (The Personal Energy Planning [PEP] Program), and positive reports from all 5 study participants about the feasibility and efficacy of the program. This study lays the groundwork for future investigation into the efficacy of this approach in people with ESRD who experience disabling fatigue.
Introduction
Fatigue is a pervasive symptom of end-stage renal disease (ESRD) that is estimated to be experienced by 7 in 10 people on chronic dialysis therapy. 1 Defined as an “unusual, abnormal or excessive whole-body tiredness, disproportionate to or unrelated to activity or exertion,” 2 fatigue and its negative impact on life participation (ie, the ability to participate in valued day-to-day activities) has been identified as high-priority issues by people on chronic dialysis.3 -5 The purported factors contributing to fatigue in renal disease are multifactorial, including anemia, chronic inflammation, malnutrition, uremia, depression, sleep quality, and physical inactivity.6,7 Viable treatments for fatigue in renal disease are currently well recognized to be limited, 6 as there are few proven pharmacological interventions beyond erythropoietin to target anemia, 7 and multi-level barriers to providing efficacious nonpharmacological approaches such as exercise, which include limited staff expertise, low patient motivation, and patient fatigue. 8
Recently, we proposed the adoption of an energy management education (EME) approach to address these challenges. 9 Energy management education, also known as energy conservation or adaptive pacing, is an established rehabilitative approach that teaches individuals to use strategies to manage their energy expenditure during usual day-to-day activities. Examples of energy management strategies include simplifying activities, using energy-efficient postures, and organizing home/work environments. Energy management education has been found to be effective at improving fatigue-related outcomes in other chronic disease populations including multiple sclerosis (MS)10,11 and cardiac disease,12,13 with its proposed mechanism of action being a reduction in exertional fatigue during everyday life. Given the unusually extensive treatment-related activities required of people on dialysis (eg, attending dialysis sessions, managing multiple medications, closely monitoring food and fluid intake), we purport that they could benefit from learning energy management principles to apply both during these dialysis-related activities and their usual day-to-day tasks.
The Personal Energy Planning (PEP) program is a personalized, web-supported EME program that has been developed for the dialysis patient population with input from patients and clinicians. 9 The program incorporates energy management strategies from existing evidence-based programs, and uses a problem-solving framework (Cognitive Orientation to Occupational Performance [CO-OP]) that has been effective at helping people with various impairments accomplish life participation goals and achieve independence in problem-solving. 14 The PEP program is uniquely targeted at improving life participation, which is a high priority among ESRD patients with fatigue, 3 and does not require structured exercise to achieve improved fatigue management, which has been identified as challenging by patients in previous studies. 8 The usability and acceptability of the PEP program among people on chronic dialysis have been demonstrated in preliminary studies, 9 but its efficacy has yet to be explored. Accordingly, in this proof-of-concept study, we set out to investigate the following research questions:
Methods
Design
We employed a mixed-methods sequential explanatory design 15 (Figure 1), which utilizes quantitative methodology along with qualitative methodology to elaborate on the quantitative findings. The quantitative methodology used was 5 single-case, interrupted time-series AB studies. To establish baseline levels of life participation and fatigue, we administered short questionnaires of fatigue and life participation weekly over a 3- to 4-week baseline observation period (phase A), and during a 6- to 9-week intervention period (phase B), to evaluate changes associated with the PEP program. Additional validated questionnaires of fatigue and life participation were administered before and immediately after the PEP program to cross-validate these time-series data. At study end, all individuals underwent a semi-structured individual interview to provide further insight into their experiences with the intervention.
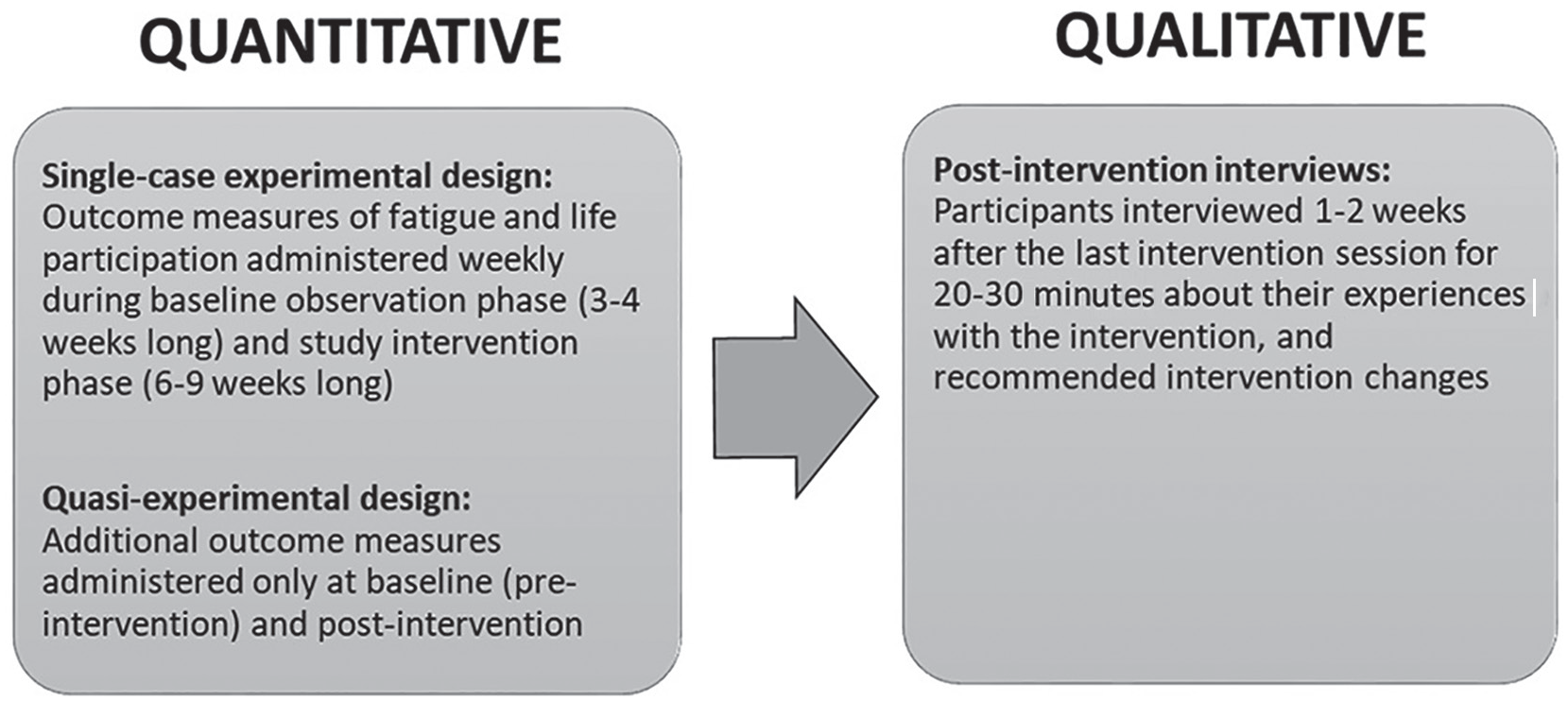
A mixed-methods sequential explanatory study design.
Participants
The study population was comprised of adults aged 18 years or more maintained on chronic dialysis therapy at a large academic hospital in Toronto, Canada. Eligible participants were those who self-reported high levels of fatigue to the clinical teams, and were willing and able to provide informed consent. Purposive sampling was used to select 5 participants who represented diversity in demographic groups (ie, age, gender, and dialysis modality). Patients with scores >3 on the Personal Health Questionnaire -2 depression screening tool; who were unable to read and understand English at a Grade 6 level, or with limited vision preventing them from reading program materials, were excluded. The study was approved by the local hospital Research Ethics Board.
Intervention: The PEP Program
The PEP program has previously been described in detail elsewhere, 9 and additional information is included in Appendix A (Supplemental Material). In brief, the PEP program provides personalized training in energy management. The program consists of 6 to 8 weekly sessions (dictated by each individual’s rate of progress) and is divided into 2 parts. Part 1 involves 2 brief educational web modules that introduce participants to basic concepts related to energy management (eg, prioritizing, simplifying tasks, using assistive equipment, organizing home and/or work environments). Each participant receives orientation to the computer modules and the program workbook during an introductory meeting. The 2 computer modules are then completed by participants, 1 per week, during dialysis sessions or at home according to their preference. Part 2 includes 4 to 6 personalized sessions with a therapist or clinician that are delivered in-person or by telephone according to patient preference. During these 20- to 30-minute sessions, patients choose 3 life participation goals (eg, shower without becoming so fatigued, cook dinner once per week) and are then taught to use a modified version of an established problem-solving framework (the CO-OP) 14 to identify energy management strategies that will help them achieve their goals.
Data Collection
Basic demographic, clinical, and laboratory information about the participants were collected from the clinical charts and confirmed through participant interview.
Fatigue
Fatigue was assessed weekly during the baseline and intervention phases using the Fatigue Severity Scale (FSS). 16 The FSS is a 9-item scale that asks individuals to rate, on a Likert scale from 1 to 7, the severity of their fatigue and its impact on their life during the past week. Item scores are averaged to create a summary score out of 7. The FSS has strong psychometric properties17,18 and has been used in the dialysis population. 19 We cross-validated the FSS data by administering the SF-36 (36-Item Short-Form Health Survey) Vitality Scale 20 and the Modified Fatigue Impact Scale (MFIS) 21 pre- and post-intervention. The SF-36 Vitality Scale is another well-validated measure22,23 that is commonly used in the renal population, while the MFIS is frequently used in EME studies.
Life participation
Life participation was assessed weekly during the baseline and intervention phases, using a short questionnaire created for the study to be brief enough for patients to complete weekly. It included 3 questions that asked participants to rate, on a scale of 1 to 10, how well they managed their fatigue during the past week, how often they had the energy to do the things they needed to do, and how often they had the energy to do the things they wanted to do. Ratings for each question were averaged to create a total weekly summary score out of 10. We cross-validated the life participation questionnaire by administering the performance subscale of the Canadian Occupational Performance Measure (COPM) 24 pre- and post-intervention. The COPM is an established, valid, reliable, and responsive outcome measure 25 that asks individuals to rate, on a 10-point Likert scale, how well they are able to perform each of 3 chosen life participation goals (eg, dressing, cooking).
Life participation satisfaction
Satisfaction with life participation was assessed weekly during the 2 study phases using a single question created for this study. The question asked participants to rate, on a scale of 1 to 10, how satisfied they were with their general fatigue management. We cross-validated this question by administering the satisfaction subscale of the COPM 24 pre- and post-intervention. It asks participants to rate, on a 10-point Likert scale, their current satisfaction with their ability to perform each of 3 chosen life participation goals.
Post-intervention interview
Each participant underwent a semi-structured interview (by J.F.F.) 1 to 2 weeks after completion of the program (interview guide is included in Appendix B, Supplemental Material). Participants were asked to provide further details on their experiences with the PEP program and its impact on their lives, and share any program changes they would recommend.
Data Analysis
The weekly time-series data on fatigue, life participation, and satisfaction with life participation were analyzed using visual analysis and the Tau-U statistic, both recommended approaches for analyzing time-series data.26,27 After graphing the data for each variable on an interrupted time-series scatterplot, changes in the trend direction and level between the baseline (A) and intervention (B) study phases were evaluated using established visual analysis guidelines. 28 The following are the effect sizes between the baseline and PEP: Part 2 phases were then calculated using Tau-U statistics, 26 with values between 0 and .65 considered a small effect size; 65 and .92 a moderate effect size, and >.92 a large effect size. The SF-36 Vitality Scale, Fatigue Impact Scale, and COPM data were analyzed by calculating the change in score from pre- to post-intervention, with interpretation based on published minimal clinically important differences where available. Qualitative interview data were transcribed and analyzed using descriptive thematic analysis. 29
Results
The 5 participants selected to participate in the study, identified as P1 to P5, met eligibility criteria and represented diverse demographic characteristics (Table 1). Three participants (P1, P2, and P3) completed the PEP program during in-center hemodialysis sessions, while 2 (P4 and P5) home dialysis patients completed the program remotely.
Participant characteristics.

Note. HD = hemodialysis ; CAPD = Cycler Assisted Peritoneal Dialysis; ADLs = Activities of Daily Living.
For the reviewers: Specific clinical details cannot be revealed as per privacy restrictions.
Quantitative Findings
Fatigue
Four participants (P1, P2, P3, and P4) displayed improvements in fatigue associated with the PEP program, according to the visual analysis and Tau-U statistics calculated from the weekly fatigue data (Table 2). The effect sizes were small for 2 participants (P1 and P3), and moderate for 2 participants (P2 and P4). Three of these participants (P2, P3, and P4) also demonstrated clinically meaningful improvements from pre- to post-intervention on both the SF-36 Vitality Scale and the Fatigue Impact Scale (Table 3). One participant (P5) demonstrated no positive changes in fatigue on any measures.
Visual Analyses Results and Tau-U Results for Weekly Time-Series Data.
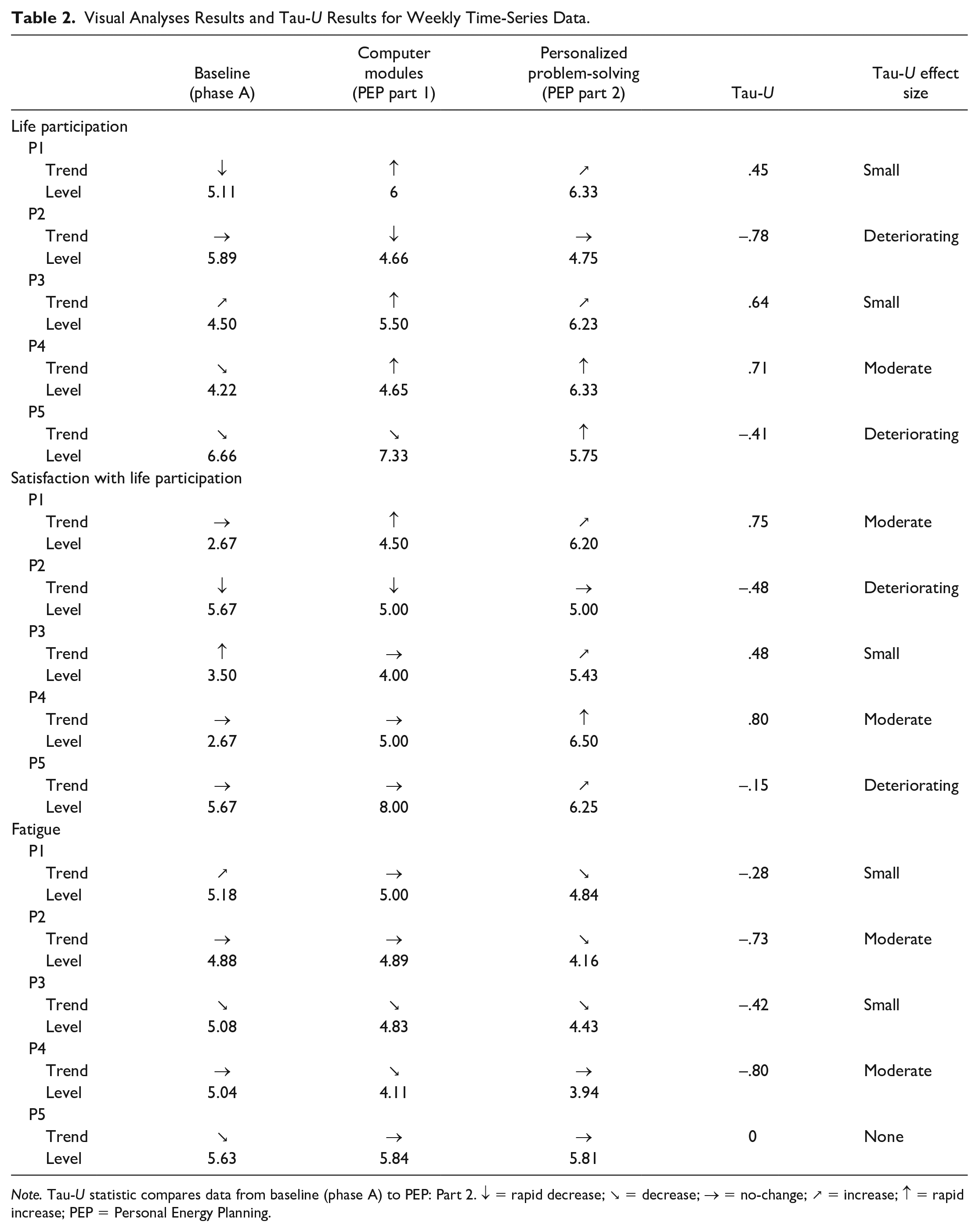
Note. Tau-U statistic compares data from baseline (phase A) to PEP: Part 2. ↓ = rapid decrease; ↘ = decrease; → = no-change; ↗ = increase; ↑ = rapid increase; PEP = Personal Energy Planning.
Changes in Fatigue Scores From Pre- to Post-Intervention.

Note. SF-36 = 36-Item Short-Form Health Survey; PEP = Personal Energy Planning.
Minimally clinically important difference.
Life participation
Three participants (P1, P3, and P4) displayed improvements in life participation associated with the PEP program on all measures (Table 2). The effect sizes were small for 2 participants (P1 and P4) and moderate for 1 participant (P3) according to the Tau-U statistic calculated from the weekly time-series data (see Figure 2 for time-series graph for P3). The same 3 patients also experienced clinically significant improvements (≥2-point increase) on the performance subscale of the COPM from pre- to post-intervention: 2 patients on all 3 goal activities, and 1 patient on 2 of 3 goal activities (Figure 3). Two participants (P2 and P5) demonstrated no improvements on any measures of life participation (see Figure 4 for time-series graph for P2).
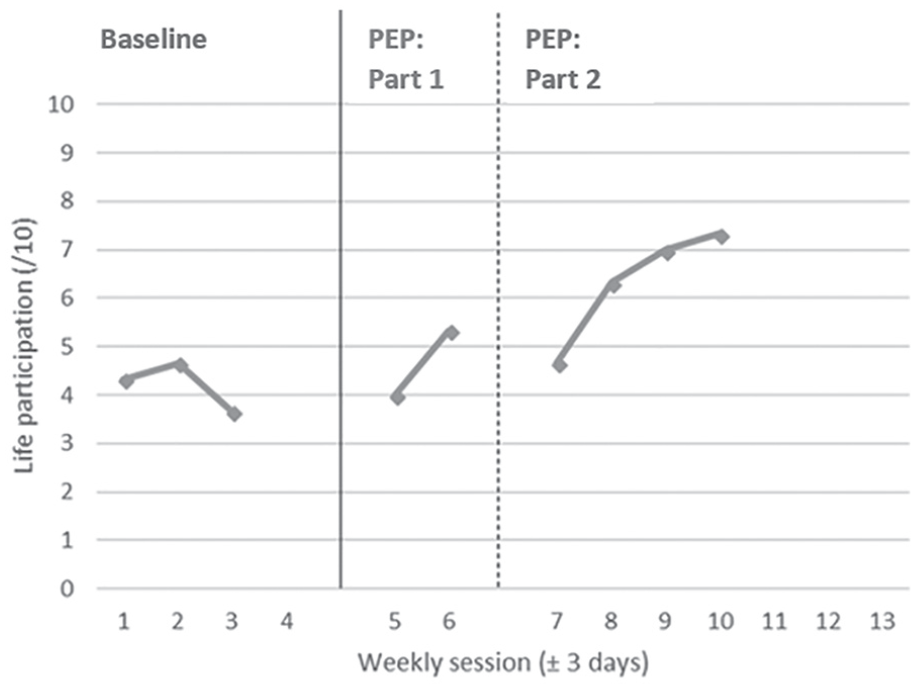
Interrupted time-series graph demonstrating a moderate effect of the PEP program on life participation in P3.

Patient ratings of performance of chosen life participation activities, before and after intervention.

Interrupted time-series graph demonstrating no effect of the PEP program on life participation in P2.
Satisfaction with life participation
Three participants (P1, P3, and P4) displayed improvements on all measures of satisfaction with life participation associated with the PEP program (Table 2). The effect sizes were moderate for 2 participants (P3 and P4) and small for 1 participant (P1) according to the Tau-U statistics calculated from the weekly time-series data. These 3 also demonstrated clinically significant improvements (≥2-point increase) on the satisfaction subscale of the COPM: 2 patients on all 3 goal activities, and 1 patient on 2 of 3 goal activities. Two participants (P2 and P5) demonstrated no improvements in satisfaction with life participation on any measures.
Qualitative Findings
Impact of the program
All 5 participants reported that the PEP program had helped them to manage fatigue more effectively. P3 stated that the PEP program made him feel “more energized,” while P2, P3, and P5 shared that the program had enabled them to cope with daily tasks more easily. P4 expressed that the PEP program had reminded him of what was possible for his life and changed his sense of independence: Well, it was good for the fact that it allowed me to be a bit more independent . . . and it gave me hope . . .that I could actually do things, if I were to manage my other activities, and my other plans . . . (P4)
P1, P2, and P4 expressed that the program had “opened their eyes” and helped them to think more carefully about how they were spending their energy. The participants all expressed that the program had helped them to generate new ideas and strategies for completing their day-to-day tasks. P4 expressed that he was already familiar with most of the strategies covered in the program, but that the program had motivated him to use them. All participants described instances where they had used the energy budgeting strategies from the PEP program to accomplish their pre-selected goals. They also described examples of when they had applied the strategies to work on goals not addressed in the PEP program. For example, P1 shared, If I’m going shopping now or I have to go to a few different places, I just try to organize it so there’s a route, right—not wasting energy.
All participants expressed that they would recommend the program to other people on dialysis. For example, P1 stated, I kinda think everyone in here should go through this. I think it would help everybody. I’m glad I did it.
Program format
The program format was acceptable to all participants. P1 and P2 expressed that they preferred doing the program during dialysis sessions rather than their own time, because it helped to pass the time during dialysis. For example, P2 stated, I think it’s perfect to do it here, because, what do you do with the four hours? You know, at least you have this to look forward to! So it’s very good.
P3, however, expressed that he found the dialysis unit to be noisy and distracting, and that he would have preferred to do the sessions outside of dialysis. P4 and P5, who completed the program from home, endorsed the phone-based format.
All participants felt the web modules were an important part of the program, and were acceptable and easy to use. P1 and P5 stated that they found the pace of the modules good; P4, however, expressed that the modules moved too slowly for him at times. Participants’ viewpoints were also conflicting about whether they used the information from the modules during the personalized portion of the program.
All participants expressed that they valued the personalized, goal-focused portion of the program. For example, P2 expressed that she preferred this section to the computer modules, because it was more applicable to her specific life situation. The participants’ experiences with the CO-OP problem-solving framework used in the program were, however, variable. P3 and P5 felt the framework was a good way to approach problem-solving and reported using it in their day-to-day life. However, P3 also expressed frustrations with the approach, such as finding it difficult to problem-solve about his energy problems by imagining himself doing daily activities. P1 and P4 could not recall the framework at all.
Program limitations
The participants identified few weaknesses and had few recommendations for change. P3 suggested offering the program in a group-based format to provide the opportunity to learn from peers. P4 expressed the importance of being motivated to benefit from the program, and speculated whether this could be a barrier for some patients. He also recommended the program modules be made available on a tablet, to increase convenience. P5 felt that financial budgeting was an imperfect analogy to use to explain how one should manage their energy, and that discrepancies between the 2 should be clarified. He also expressed that the way fatigue was described did not align with his experience of sometimes gaining energy by performing tasks, and suggested this be clarified as well.
Inconsistencies in findings
P2 and P5 were asked to provide further insight into their experiences with the program, because their negative quantitative outcomes were inconsistent with their qualitative reports. P2 seemed conflicted about her experience with the program. She repeatedly emphasized that the program had benefited her. However, she also shared that she felt she was “in a rut,” and that it was not the responsibility of the program to change that. She talked about the need to be motivated to change, and how because she lived alone, her current activity patterns were adequate for her. P5, meanwhile, expressed unreservedly that he did benefit from the program and stated that it had helped him to be able to “do more things.”
Discussion
This is the first study to explore the efficacy of an EME approach for improving fatigue and life participation outcomes in adults on dialysis. Findings from the quantitative component of the study were mixed: 3 participants demonstrated a consistently positive response across multiple outcome measures, while 2 demonstrated an inconsistent or no response. However, all participants identified benefits of the program during qualitative interviews, with the most common reported benefit that it had made their lives and/or their daily activities easier. The format of the program was also largely reported to be feasible and convenient by participants.
The results of this study are early, proof-of-principle evidence that EME can produce meaningful improvements in fatigue-related outcomes in people on chronic dialysis. At present, there are a dearth of feasible, evidence-based interventions to address fatigue in renal patients. 6 Erythropoietin stimulating agents are effective at reducing anemia-related fatigue, 7 but fatigue is also believed to arise due to factors besides anemia in renal disease. 6 Similarly, while exercise training has evidence to support its efficacy,30,31 many dialysis patients report feasibility or other barriers to participating in exercise.8,32 Recent studies have reiterated the profound negative impact of fatigue on patient well-being and life participation, highlighting the need to investigate alternative approaches that can assist dialysis patients with day-to-day fatigue management.3,5 The EME approach is advantageous because it is not specific to any one fatigue etiology but can be used with anyone who experiences physical fatigue. Furthermore, the PEP program been designed to limit potential feasibility and usability barriers in the dialysis population, by using a concise format and simple, easy-to-use program materials. Thus, it may be able to fill an important gap in the care of end-stage renal patients who experience disabling fatigue.
The beneficial effects on fatigue outcomes observed in this study are consistent with previous EME literature from some other chronic disease populations, such as MS.10,11,33 -35 However, the positive changes observed in life participation are relatively novel in the EME literature. 9 We speculate whether this may be due to the problem-solving framework (CO-OP) incorporated into the PEP program, which was included because of its effectiveness at improving life participation in various other populations.36 -39 The CO-OP framework provides a structured, theory-based method for patients to gain independence at generating solutions to their life participation challenges. The improvements we observed in life participation in this study are consistent with 2 other preliminary EME studies that also used problem-solving training approaches to facilitate improvements in the participant’s daily life.12,40 However, despite these promising results, the effect sizes in our study appear to be attenuated compared with previous CO-OP literature.36,38 We speculate whether changes made to the CO-OP problem-solving framework to make it more feasible for people on dialysis might explain the attenuated effect. For example, we used fewer, shorter problem-solving sessions and a visualization-based approach to trialing energy-saving strategies that would still enable participants to complete the program sessions during dialysis. Data from the qualitative interviews suggested that some patients found it difficult to use this modified approach, while some did not recall CO-OP’s problem-solving framework at all. Further consideration of how CO-OP’s core elements could be reinforced in the PEP program, while still maintaining program feasibility for dialysis patients, may therefore be warranted prior to future efficacy research.
It is also notable that although 3 participants displayed positive changes across the study outcome measures, 2 participants did not show consistent improvements associated with the program. One of the participants, on interview, expressed that the program did have a positive impact. However, the other participant was more ambivalent and alluded to a lack of readiness to change. Her comments were consistent with someone at a pre-contemplative level within the Transtheoretical Model (TTM) of Readiness to Change, 41 when individuals are often unaware that a behavior has negative consequences and do not intend to take action to change in the foreseeable future. 41 A modified preliminary approach might therefore be needed for patients who are initially not yet ready to change their fatigue management behaviors. For example, at the pre-contemplative stage, the TTM recommends focusing on increasing the individual’s awareness of their decision-making and highlighting potential benefits of change. 41
We consider the use of a mixed-methods study design and single-case time-series studies to be strengths of this study, as these are both well-established and cost-effective ways to evaluate a new intervention. 27 However, we also acknowledge the preliminary status of this evidence and the need for further long-term follow-up. Other study limitations include the first author both administering the intervention and conducting the study questionnaires, which may have compelled participants to report greater benefit associated with the program than actually experienced. We attempted to minimize this limitation by using multiple assessment approaches to cross-validate and confirm the study findings (eg, questionnaires, qualitative interviews). The small, hand-selected sample of participants included in this study also means there is a need to explore the program in a larger sample of dialysis patients.
Conclusions
This study provides preliminary evidence that an EME program can result in positive fatigue-related outcomes, including life participation, in adults on chronic dialysis. A multi-site pilot randomized controlled trial to further evaluate the feasibility and efficacy of the program is now underway (ClinicalTrials.gov: NCT03825770).
Supplemental Material
Appendix_A_-_Description_of_the_PEP_program – Supplemental material for A Proof-of-Concept Investigation of an Energy Management Education Program to Improve Fatigue and Life Participation in Adults on Chronic Dialysis
Supplemental material, Appendix_A_-_Description_of_the_PEP_program for A Proof-of-Concept Investigation of an Energy Management Education Program to Improve Fatigue and Life Participation in Adults on Chronic Dialysis by Janine F. Farragher, Helene J. Polatajko, Sara McEwen and Sarbjit V. Jassal in Canadian Journal of Kidney Health and Disease
Supplemental Material
Appendix_B_-_Efficacy_Interview_Guide – Supplemental material for A Proof-of-Concept Investigation of an Energy Management Education Program to Improve Fatigue and Life Participation in Adults on Chronic Dialysis
Supplemental material, Appendix_B_-_Efficacy_Interview_Guide for A Proof-of-Concept Investigation of an Energy Management Education Program to Improve Fatigue and Life Participation in Adults on Chronic Dialysis by Janine F. Farragher, Helene J. Polatajko, Sara McEwen and Sarbjit V. Jassal in Canadian Journal of Kidney Health and Disease
Footnotes
Ethics Approval and Consent to Participate
Written informed consent was obtained from all participants in the study. The study was approved by the Research Ethics Board at the University Health Network in Toronto, Canada (Protocol ID: 17-5414).
Consent for Publication
Not applicable.
Availability of Data and Material
The datasets generated and/or analyzed during the current study are not publicly available due to the potential for a breach in participant anonymity but are available from the corresponding author on reasonable request.
Author Contributions
J.F.F. was responsible for study design, data collection, analysis, and manuscript write-up. H.J.P., S.Mc.E., and S.V.J. provided advice on key elements of study design and analysis, and edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was provided trainee support for this work via a Vanier Canada Graduate Scholarship and a KRESCENT Allied Health Doctoral Fellowship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.