
Abstract
Background:
Mortality rates for patients on hemodialysis (HD) continue to be high, in particular, following the long interdialytic period, yet thrice-weekly conventional HD (CHD) is still an almost universal regimen. Alternate-day dialysis (ADD) may have advantages over the current schedule because it would eliminate the long interdialytic break. A preliminary, as yet unpublished, patient simulation and cost-utility analysis compared CHD versus ADD and demonstrated that the economic attractiveness of ADD was sensitive, in particular, to patients’ preference for ADD versus CHD. To date, this preference has not been elicited.
Objective:
To elicit utilities for both CHD and ADD using 3 standard elicitation methods among a prevalent cohort of patients on CHD.
Design:
This study is a single-center survey of patient preferences (utilities).
Setting:
This study took place within the dialysis units of Sunnybrook Health Centre, a university-affiliated teaching hospital in Toronto, Ontario, Canada, which encompasses 174 patients on in-center HD.
Patients:
Those older than 18 years of age, on thrice-weekly HD, were included in this study.
Measurements:
Descriptive statistics were used to summarize patient characteristics and the utility values generated. A multiple linear regression was performed to determine an association between participant characteristics and the utility ratio.
Methods:
Via standardized face-to-face interviews by a single investigator, 3 utility elicitation methods, visual analogue scale (VAS), time trade-off (TTO), and standard gamble (SG), were administered to generate utilities for each patient for their current health state of CHD (thrice-weekly). After completing this task, we provided each patient with a concise summary regarding the current literature on how ADD may impact their health. Finally, patients were asked to envision their health while on an ADD regimen while repeating the VAS, TTO, and SG.
Results:
We recruited 65 participants. The mean utilities of CHD versus ADD were similar for all 3 methods. Visual analogue scale, TTO, and SG had utility values of 0.6 ± 0.2, 0.6 ± 0.3, and 0.7 ± 0.3, and 0.6 ± 0.2, 0.7 ± 0.3, and 0.7 ± 0.3 for CHD and ADD, respectively. The ratio for CHD to ADD was 1.1 ± 0.4, 1.1 ± 0.5, and 1.0 ± 0.2 for VAS, TTO, and SG, respectively.
Limitations:
Small sample size from a single center, where not all participants agreed to participate, wide variability in participant responses and requiring patients to conceptually imagine life on ADD may have affected our results.
Conclusions:
Compared with CHD, there was no difference in the preference toward ADD which demonstrates promise that adopting an alternate-day schedule may be acceptable to patients. Furthermore, with the generation of a utility for ADD, this will allow for more precise estimates in future simulation studies of the economic attractiveness of ADD.
Trial registration:
Not required as this article is not a systematic review nor does it report the results of a health care intervention.
What was known before
Mortality rates for patients with end-stage renal disease on thrice-weekly hemodialysis are high with an increase in frequency of complications experienced after the long interdialytic period. A prior preliminary patient simulation and cost utility-analysis comparing conventional hemodialysis to alternate-day dialysis demonstrated that at a threshold of $100 000 per extra quality-adjusted life year, alternate-day dialysis becomes cost-effective relative to conventional hemodialysis, albeit dependent on patient’s preference to alternate-day dialysis versus conventional hemodialysis.
What this adds
The objective of this article was to elicit utility values for both conventional and alternate-day dialysis using 3 standard elicitation methods among a prevalent cohort of patients on thrice-weekly hemodialysis to provide data for further development of the alternate-day dialysis decision analytic models.
Introduction
Mortality rates for patients on hemodialysis (HD) continue to be high. 1 In particular, patients on conventional HD (CHD) thrice-weekly experience higher risk of sudden cardiac death following the long interdialytic period (Friday-Monday or Saturday-Tuesday),2-4 yet conventional thrice-weekly HD is still an almost universal regimen. Strategies to eliminate the long interdialytic break have been an area of active research. 5
The Frequent Hemodialysis Network (FHN) randomized clinical trials have demonstrated potentially promising results of 6-days-per-week, in-center, HD compared with conventional 3-times-per-week treatment in terms of quality of life (QOL), patients’ perceptions of physical health and physical functioning, and improvement in memory and verbal fluency.5-8 Other FHN studies have demonstrated that these improvements are not without risk. For example, the requirement for vascular procedures to maintain vascular access increases with more frequent HD. 9 Another potential barrier to 6-times-weekly dialysis is travel burden placed on patients. The FHN trials experienced significant difficulties in recruiting the targeted number of study participants.
An alternative to 6-times-weekly HD would be alternate-day dialysis (ADD), in which patients would receive HD every other day. Alternate-day dialysis may have advantages over 6-times-weekly treatment because it would eliminate the long interdialytic break, may be more palatable for patients, may not place much demand on dialysis access and may not be costly. A preliminary, as yet unpublished, patient simulation and cost-utility analysis that compared CHD versus ADD, performed by our group, demonstrated that the economic attractiveness of ADD was sensitive, in particular, to patients’ preference for ADD versus CHD (Unpublished report by James Lineen, David Orlov, and David Naimark, True Alternate-Day Versus Conventional Hemodialysis for Patients With End-Stage Renal Disease: A Cost-Utility Analysis, December 17, 2014, University of Toronto; unreferenced). To date, this preference has not been elicited.
In health economics, patient preference is commonly expressed as a utility which is a numerical value within the range of 0 to 1 that indicates preference for a particular health state relative to the worst possible condition (0, usually representing death) and the best possible condition (1, usually representing perfect health). The objective of this article was to elicit utilities for both CHD and ADD using 3 standard elicitation methods among a prevalent cohort of patients on CHD.
Methods
Study Setting
We conducted a single-center survey of patient preferences (utilities) between February and November, 2019, within the dialysis units of Sunnybrook Health Centre, a university-affiliated teaching hospital in Toronto, Ontario, Canada, which encompasses 174 patients on in-center HD.
Participants
We approached patients to consider participating who were older than 18 years of age, on maintenance in-center HD, on the standard regimen of thrice-weekly treatments, who were proficient in English, and who had the cognitive capacity to participate and consent to the study (the latter 2 criteria were based on the judgment of the primary HD team members).
We excluded HD patients who could not communicate in English, those with severe visual and/or hearing impairment for which obtaining consent or proceeding with the study would not be feasible, and for those who declined to participate or who otherwise could not complete the informed consent form. To restrict the study to patients who would expect to require HD indefinitely, we excluded patients who were both listed for cadaveric transplantation and had been called in for a potential transplant within 6 months (ie, they were called in to the transplant center but the transplant could not proceed for some reason). Moreover, we excluded participants discharged from a hospital admission, those with initiation or dose titration of psychotropic medications, and/or those with a significant life event (ie, death or sickness of a friend or family member) within 1 month of the start of the enrollment window.
Baseline characteristics including age, gender, body mass index (BMI), cause of end-stage renal disease (ESRD; diabetes, hypertension, glomerulonephritis, polycystic kidney disease, other, unknown), and comorbid medical conditions were ascertained from Sunnybrook information systems (SunnyCare and AccuroTM).
Procedure
Individuals were screened by the primary staff nephrologist for each HD shift to determine whether participants were appropriate candidates. If deemed appropriate, an investigator approached each candidate to introduce the study and obtain consent among candidates who agreed to participate. Then, via standardized face-to-face interviews by a single investigator (R.J.S.), the visual analogue scale (VAS), time trade-off (TTO), and standard gamble (SG) methods 10 were administered to elicit utilities for each patient (Supplemental Appendix). We first elicited utilities for the current health state of CHD. After completing this task, we provided each patient with a concise summary, employing nontechnical language, regarding the current literature on how ADD may impact their health: (1) improvement in overall health,5,11-17 (2) improvement in QOL,6,7,11,12,18 (3) improvement with dialysis-related symptoms and time to recovery after dialysis,7,11,12,18 and (4) complications.5,9,19 We then asked the participants to envision their health while on an ADD regimen while subsequently repeating the VAS, TTO, and SG.
Description of the Utility Elicitation Instruments
Visual analogue scale
The VAS is a paper-based instrument whereby the participant marked their assessment of their preference for a health state (CHD followed by ADD) on a scale ranging from 0 to 10 where 0 represents the lowest state of health (death), whereas 10 reflects perfect health. Utility was calculated as the point on the scale divided by 10.
Time trade-off
In the TTO method, each participant was asked to reflect on a health state (CHD followed by ADD) and then choose between 2 hypothetical options: remain in that state for their remaining life expectancy, chosen arbitrarily and hypothetically to be 15 years, or to trade-off a number of years, thus live for a shorter duration, but in perfect health. The time frames were then adjusted with the duration of life in perfect health decreased systematically until the participant’s preference was indifferent regarding the choice between the 2 options. At the point of indifference, the utility was computed as the proportion of the lifespan occupied by complete health. For example, if a participant’s point of indifference is between 10 years of healthy life and 15 years in a state of conventional dialysis, then the utility would be 0.67.
Standard gamble
To determine utilities by the SG, the participant was asked to make a decision between either staying in their current health state on CHD (or their envisioned health state on ADD) versus undergoing a hypothetical therapy. This therapy has 2 possible outcomes. If successful, the participant would be cured and would live in full health. However, if the therapy is not successful, the participant would experience immediate death. The chance of death associated with this hypothetical therapy was varied in an iterative manner until the patient was indifferent between staying in their current health state versus undergoing the hypothetical therapy. The utility was calculated as 1 minus the probability of death at the point of indifference.
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics: means and standard deviations or median and interquartile range (IQR) for continuous variables and percentages for categorical characteristics. To calculate the utility of ADD relative to CHD for each elicitation method and for each participant, the ratio of the utility for ADD was divided by the utility for CHD. These values were summarized with both mean and standard distributions and medians and IQR. Histograms of the ratios across participants and the relative magnitude of mean and median values were used to assess distribution features. The association between participant characteristics (age, gender, and number of comorbid conditions) and utility ratio was performed for each elicitation method using multiple linear regression. All analyses were performed using Microsoft Excel version 15.33 or R version 3.2.3.
Written, informed consent was obtained from each participating patient. The Research Ethics Board of Sunnybrook Health Sciences Centre approved the study.
Results
Patient Characteristics
Between February and November 2019, from a prevalent population of 174 HD patients, 109 patients were excluded as per the inclusion and exclusion criteria, or due to nonconsent. A total of 65 participants were recruited. The mean age of patients recruited was 64.9 ± 15.6 years, with 53.9% male predominance, and with most ESRD attributed to diabetes (37%). There was an average of 5.3 ± 2.4 comorbid conditions (Table 1).
Baseline Characteristics of Patients.

Note. Percentages may not total 100 because of rounding. HD = hemodialysis; BMI = body mass index; ESRD = end-stage renal disease.
Number of any medical conditions listed in the clinical electronic medical record.
Utilities for CHD and ADD
The mean utilities of CHD versus ADD were similar for all 3 methods, VAS, TTO, and SG with similar mean and median values (Table 2). Utilities assessed with VAS showed mean values of 0.6 ± 0.2 and 0.6 ± 0.2 for CHD and ADD, respectively, with a ratio of 1.1 ± 0.4. Time trade-off results showed that patients would trade-off 9 years for CHD and 8 years for AAD with utility values of 0.6 ± 0.3 and 0.7 ± 0.3 for CHD and ADD, respectively, with a ratio of 1.1 ± 0.5. With the SG methodology, patients would take a 30% risk to achieve “perfect” health for either CHD or ADD with utility values of 0.7 ± 0.3 and 0.7 ± 0.3 and a ratio of 1.0 ± 0.2.
Results of All the Utility Assessments.
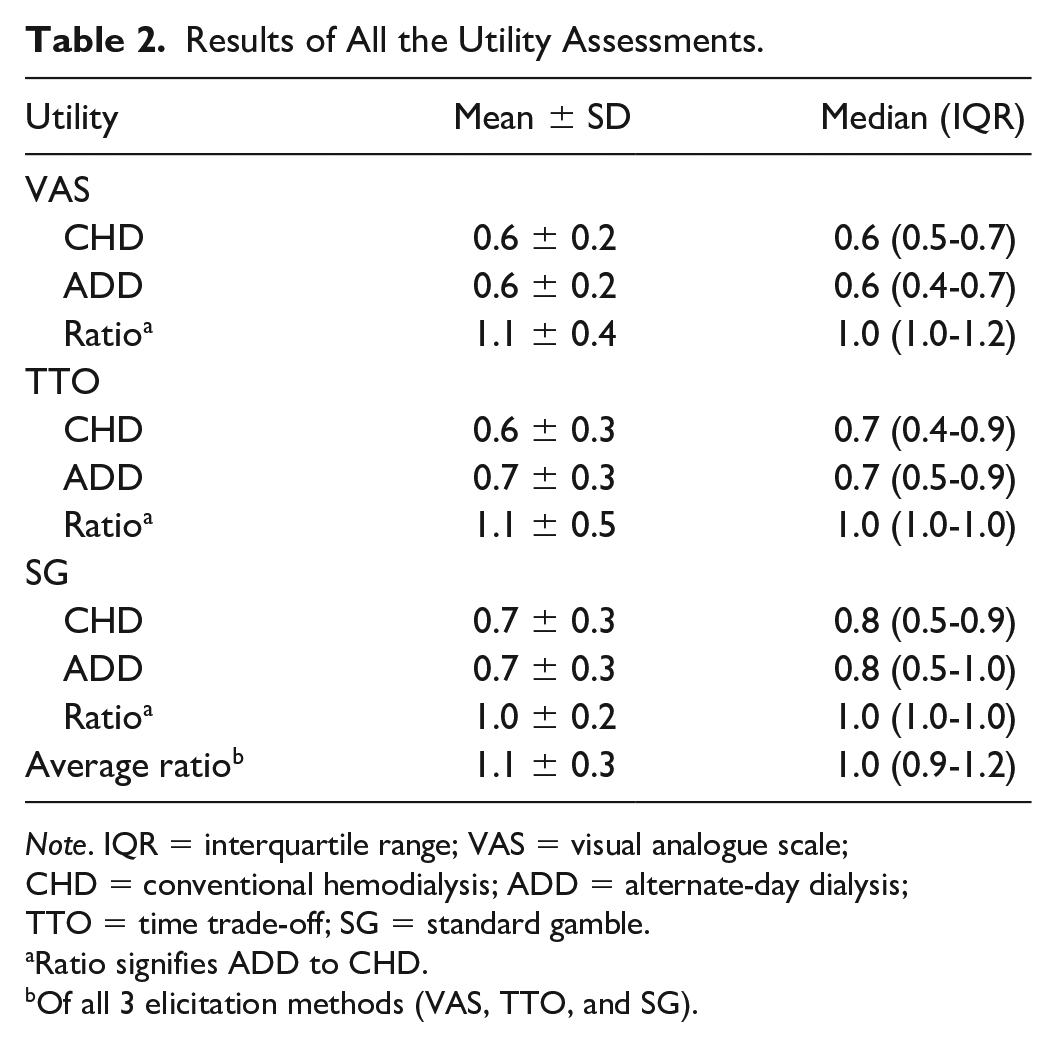
Note. IQR = interquartile range; VAS = visual analogue scale; CHD = conventional hemodialysis; ADD = alternate-day dialysis; TTO = time trade-off; SG = standard gamble.
Ratio signifies ADD to CHD.
Of all 3 elicitation methods (VAS, TTO, and SG).
Histograms generated (Figures 1-3) showed relatively symmetric distributions of the ADD to CHD utility ratios for all 3 elicitation methods. Symmetry was also suggested by similar means and median values for ratios from all 3 elicitation methods. Correlation coefficients were low, 0.2, 0.1, and 0.1 for VAS versus TTO (Figure 4), VAS versus SG (Figure 5), and TTO versus SG (Figure 6), respectively.

Histogram illustrating the alternate-day dialysis (ADD) to conventional hemodialysis (CHD) utility ratios generated with the visual analogue scale.

Histogram illustrating the alternate-day dialysis (ADD) to conventional hemodialysis (CHD) utility ratios generated with the time trade-off.

Histogram illustrating the alternate-day dialysis (ADD) to conventional hemodialysis (CHD) utility ratios generated with the standard gamble.

Utility value ratios—alternate-day dialysis (ADD) to conventional hemodialysis (CHD)—between the visual analogue scale and the time trade-off elicitation methods. Correlation coefficient was low at 0.2.

Utility value ratios—alternate-day dialysis (ADD) to conventional hemodialysis (CHD)—between the visual analogue scale and the standard gamble elicitation methods. Correlation coefficient was low at 0.1.

Utility value ratios—alternate-day dialysis (ADD) to conventional hemodialysis (CHD)—between the time trade-off and the standard gamble elicitation methods. Correlation coefficient was low at 0.1.
Regression analysis demonstrated no significant associations between age, gender, number of comorbid conditions, or dialysis vintage for any of the ratio results (Table 3). The P values for VAS ratio to age, male gender, number of comorbid conditions, and dialysis vintage were .92, .57, .40, and .40, respectively. The P values for TTO ratio to age, male gender, number of comorbid conditions, and dialysis vintage were .25, .45, .43, and .16, respectively. The P values for SG ratio to age, male gender, number of comorbid conditions, and dialysis vintage were .63, .50, .27, and .26, respectively.
Summary of the Regression Analysis Between Age, Gender, Number of Comorbid Conditions and Dialysis Vintage to Utility Ratio results.
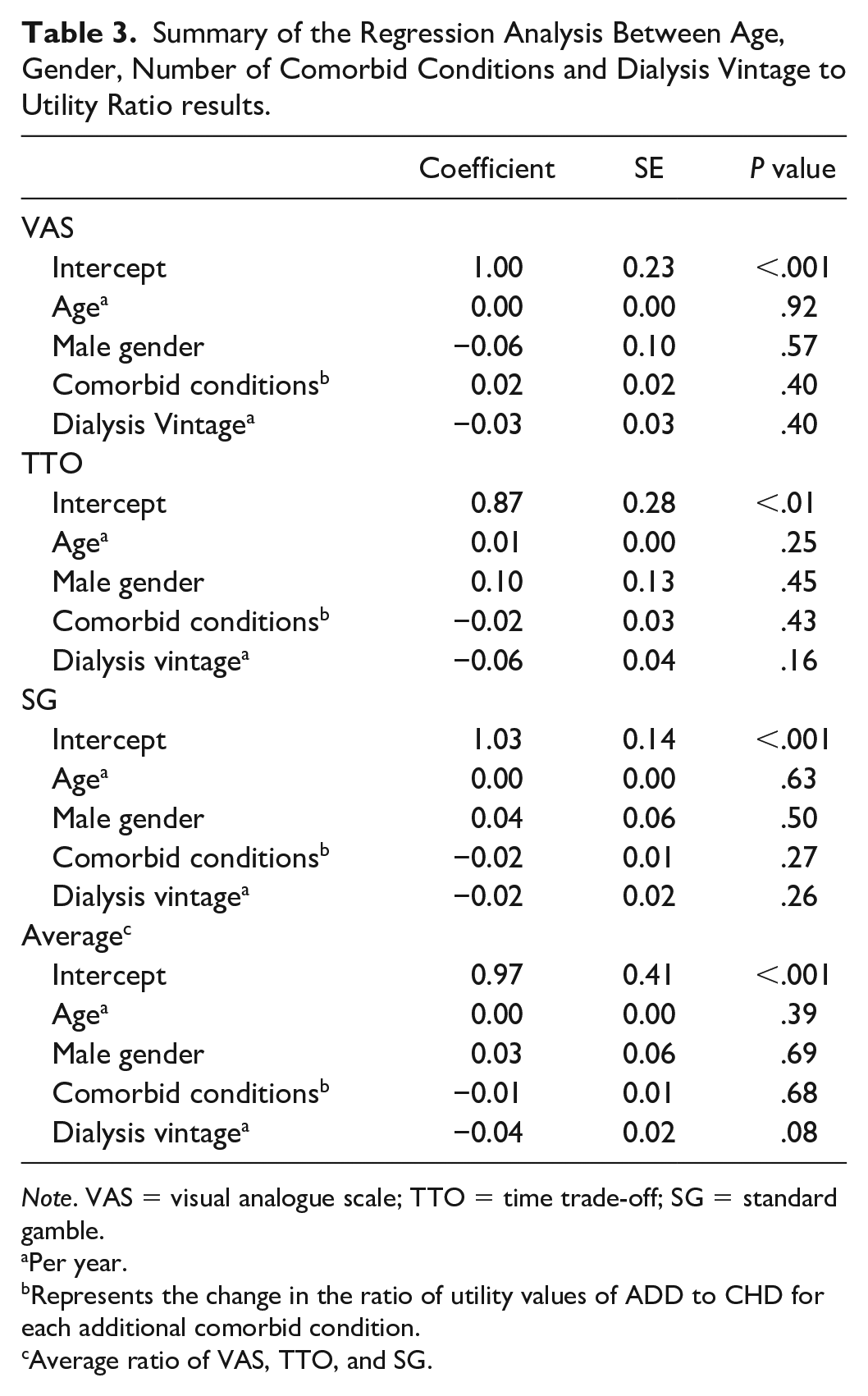
Note. VAS = visual analogue scale; TTO = time trade-off; SG = standard gamble.
Per year.
Represents the change in the ratio of utility values of ADD to CHD for each additional comorbid condition.
Average ratio of VAS, TTO, and SG.
Discussion
In this single-center study of patient preference for conventional versus alternate-day dialysis, interestingly, there was no major difference in the preference of ADD versus CHD in this sample of prevalent patients on maintenance in-center HD, on the standard regimen of thrice-weekly treatments. To our knowledge, these results are the first utility scores generated from a dialysis population regarding an ADD schedule. Furthermore, to validate our findings, our elicited mean utility values for CHD of 0.6 ± 0.3 and 0.7 ± 0.3 for TTO and SG, respectively, were similar to previous values described in literature. A prior systematic review and meta-analysis showed that the utility of HD is 0.61 (95% confidence interval [CI] 0.54-0.68) and 0.75 (95% CI 0.57-0.92) using TTO and SG, respectively. 20
Comparable to the FHN randomized clinical trials of 6-days-per-week of in-center dialysis, 5 a small pilot study comprising 18 patients also demonstrated improved clinical and biochemical parameters with ADD when compared with CHD. 12 This suggests that patients requiring dialysis may experience the benefits of increased number of dialysis treatments, however, in a more attractive ADD schedule. This could lessen the potential roadblock and resistance to the prospect of losing the long interdialytic break; many patients on CHD are highly resistant to the idea of increasing the frequency of their treatment regimens. Yet, our study patients were found to be indifferent to ADD versus CHD, with average utility values for the ratio of ADD to CHD being 1.1 for VAS and TTO and 1.0 for SG. This demonstrates promise that adoption to an alternate-day schedule may be acceptable to patients in our HD unit; however, generalizing this finding to the entire HD population is less clear. The fact that average utility values derived for CHD were similar to prior studies supports the generalizability of our findings. However, there was substantial individual variability in preference, as judged by the variability in utility values, among patients. The source of this heterogeneity remains uncertain as we were unable to determine an association between age, gender, number of comorbid conditions, or dialysis vintage to any of the utility ratio results.
In health economics, programs or strategies are compared in terms of both their expected costs and benefits. The benefit of health care strategies is frequently denominated in terms of quality-adjusted life years (QALYs) which, in simplest terms, is the product of life-expectancy and a preference weight, otherwise known, as a utility, associated with a particular health state or condition. As supported in literature, annual costs for daily HD are substantially less than those for CHD presumably in large part to reducing hospitalizations. 21 A preliminary, as yet unpublished, patient simulation and cost-utility analysis that compared CHD with ADD, performed by our group, demonstrated that at a threshold of $100 000 per QALY, ADD becomes cost-effective relative to CHD but this is dependent, in particular, to patients’ preference for ADD versus CHD. Now that a utility value exists for patient’s preferences for ADD versus CHD, more precise estimates in future simulation studies of the economic attractiveness of ADD may be employed. However, as noted in our study, the results were not strongly correlated among the elicitation method with low correlation coefficients which may suggest generally that utility elicitation should not rely on a single method.
This study has several important limitations which could explain why there was no difference in the utility values between the 2 HD schedules. This includes a small sample size from a single center. Unfortunately, not all potential participants agreed to participate, which may have induced a selection bias and reduced the ability to generalize the results to the entire HD population. A formal sample size calculation was not performed; thus, it is difficult to ascertain whether this study was sufficiently powered to determine an effect between CHD versus ADD. Furthermore, the patients who would benefit the most from ADD (ie, those with difficulties in fluid balance or blood pressure control) may already be on an increased dialysis regimen and thus would have been excluded from this study and not captured in the results. Similarly, those who experience problems with their vascular access tend to be sicker and thus also excluded from the study. The wide variability seen in this study could also account for the indifference seen purely due to participant’s responses canceling each other out. Specific comorbidities were not collected, and there was not a specific set of comorbidities that were counted for each individual patient. Therefore, there may have been a wide variation in the type or number of comorbid conditions depending on the accuracy of the electronic medical record documentation. Finally, we required patients to imagine life on ADD which may have been conceptually too demanding to generate accurate utility values, but currently, ADD is not a common dialysis schedule; therefore, elicitation of utilities from patients who have direct experience with ADD is not feasible.
Strengths of our study include use of well-established methods for eliciting utilities including VAS, TTO, and SG. 10 Furthermore, consistent application of these methods in the sequential order was performed by a single investigator to minimize measurement and question-order bias, respectively, and were elicited from the correct target population (ie, excluded those who expect to be transplanted imminently). Furthermore, because the key question is the preference patients would have for switching from current CHD to a new ADD schedule, we believe that the prevalent CHD population is the most appropriate for this particular utility elicitation.
Conclusion
As compared with CHD, there was no major difference in the preference toward ADD in our HD unit which demonstrates promise that adoption to an alternate-day schedule may be acceptable to our patients. Furthermore, now that a utility value exists in literature for patient’s preferences for ADD versus CHD, this will allow for more precise estimates in future simulation studies of the economic attractiveness of ADD, given current information as well as value-of-information analyses to determine the population-level economic gains that potential randomized trials of ADD versus CHD could produce.
Supplemental Material
uADD_supplemental_appendix_v02_1 – Supplemental material for Preference for Alternate-Day Versus Conventional In-Center Dialysis: A Health Utility Elicitation
Supplemental material, uADD_supplemental_appendix_v02_1 for Preference for Alternate-Day Versus Conventional In-Center Dialysis: A Health Utility Elicitation by Rafael J. Solimano, James Lineen and David M. J. Naimark in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We would like to thank the primary staff nephrologists at Sunnybrook Health Centre, Dr Zahirieh, Dr Hladunewich, Dr Tobe, Dr Oliver, and Dr. Tanna for their support and help in identifying patients for recruitment into this study.
Ethics Approval and Consent to Participate
This study was approved by the Research Ethics Board of Sunnybrook Health Sciences Centre and informed, written, consent was obtained from all study participants.
Consent for Publication
We have the author’s consent for publication.
Availability of Data and Materials
De-identified study data is available by request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.