
Abstract
Background:
Chronic kidney disease (CKD) associates with a significant health care burden with a disproportionate impact on indigenous persons or people living in remote areas. Although screening programs have expanded in these communities, there remains a paucity of evidence-based interventions to enhance clinical renal outcomes in these populations.
Objective:
The objective of this study was to identify evidence-based interventions to enhance renal outcomes in these populations.
Design:
A scoping review was conducted for studies in the Cochrane, MEDLINE, and Embase databases and from major nephrology meetings.
Setting:
Chronic kidney disease, including those on dialysis.
Patients:
Remote or indigenous populations
Measurements:
Studies that performed an intervention that was followed by measurement of renal outcomes or patient-centered outcomes (ie, quality of life) were included.
Methods:
All studies were described by study type, intervention, and clinical outcome, and trends were identified by both authors. Meta-analysis was not conducted due to study heterogeneity.
Results:
Thirty-two studies met inclusion criteria, only 2 (6.3%) of which were randomized controlled trials. Intervention types included multidisciplinary (34.4%), satellite (32.3%), telehealth (25.0%), or other (9.4%). All multidisciplinary interventions were performed in the CKD (non-dialysis) setting and reported improved patient travel time, waiting time, quality of life, kidney function, proteinuria, and blood pressure. Telehealth interventions improved program cost, patient attendance, hospitalization, and quality of life. Satellite interventions were performed in the hemodialysis setting, with 1 study evaluating acute hemodialysis. Satellite interventions improved patient travel time, dialysis clearance, quality of life, and survival, but increased program costs.
Limitations:
The study was restricted to interventional trials assessing clinical outcomes and to studies in developed countries, which likely excluded some research contributing to this field.
Conclusions:
There is significant heterogeneity among studies of interventions for patients with CKD who are indigenous or live remotely. Interventions were more likely to be successful when the remote or indigenous community was included in program development, with a culturally safe approach. More large, high-quality studies are needed to identify effective interventions to enhance clinical renal outcomes in indigenous or remote populations.
Trial Registration:
This trial is registered under PROSPERO, Registration Number 128453.
What was known before
Prior to this review, it was known that chronic kidney disease is a significant health care burden which disproportionately affects both indigenous populations and individuals living in remote regions. This has made the field a growing area of intervention and study, with telehealth and satellite dialysis programs growing to provide care to this area. Although there have been multiple studies of interventions targeting remote populations, these have not been previously reviewed for a global assessment of what interventions work.
What this adds
This review highlights the range of interventions in this area, including multidisciplinary trials targeting non-dialysis-dependent chronic kidney disease, telehealth, and satellite programs. These interventions tend to show improvements in clinical outcomes such as blood pressure. Telehealth and satellite programs are associated with increased patient satisfaction and decreased travel time. Indigenous populations warrant particular focus in this field and interventions in this area must be both clinically effective and culturally safe.
Introduction
Chronic kidney disease (CKD) is a significant health care burden, affecting almost 3 million Canadians and 1 in 10 people worldwide. 1 Chronic kidney disease occurs more commonly and with earlier onset in indigenous communities in developed nations such as Canada, New Zealand, and Australia.2-4 This is likely related to low socioeconomic status and remote location.5,6 Among indigenous and non-indigenous patients, there is an association between remote location and increased rates of CKD; these populations are less likely to receive optimal care and monitoring and more likely to have higher mortality.7,8
Remote and indigenous communities bear a disproportionate burden due to multiple socioeconomic factors, leading to higher rates of hypertension, diabetes, and their sequelae.6,9 They also face decreased access to care due to travel distances, lack of regular access to a nephrologist, and lack of a culturally safe health care infrastructure. 10
Given the disproportionate burden of CKD in remote and indigenous communities, the inferior clinical outcomes, and the unique barriers in overcoming this burden, it is imperative to identify interventions that enhance clinical outcomes in these populations. This is the first scoping review describing interventions to enhance CKD-related clinical outcomes, along the patient experience spectrum from early CKD to provision of renal replacement therapy, in remote and indigenous communities within developed nations.
Materials and Methods
Search Strategy and Study Selection Criteria
A scoping review was conducted using Cochrane, Embase, and MEDLINE databases, with no date restriction, using English only. Search terms included “nephrology,” “kidney disease,” “rural population,” “rural health,” “medically underserviced area,” “health services accessibility,” “aboriginal,” “indigenous,” “rural,” “remote,” “low-resource,” and “underserved.” Conference abstracts were searched from annual meetings of nephrology (American Society of Nephrology 2003-2018, Canadian Society of Nephrology 2012-2018, European Dialysis and Transplant Association 2002-2018, and Australia New Zealand Society of Nephrology 1998-2018). Search terms for conference abstracts were “rural,” “remote,” “indigenous,” and “low-resource.”
Studies were included if the study location was in a country ranked high or very high on the United Nations Development Programme Human Development Index. 11 Cases that were referenced in articles, but not found in the primary search, were hand searched and collected. Initial studies for screening were extracted by N.O. Both authors independently reviewed all abstracts to extract articles for full review.
Studies were included if they were intervention-based trials that measured clinical renal outcomes in patients with CKD. Clinical renal outcomes included progression to dialysis, death due to renal disease, and CKD-related laboratory measures (creatinine, estimated glomerular filtration rate [eGFR], Ca-P product, Kt/V, and albumin). Patient quality of life (QOL) and satisfaction were secondary, non-clinical outcomes that were also included as valid outcomes for this study. Multidisciplinary studies were any that included non-physician providers giving delegated care (eg, nurses, nurse practitioners, dieticians, and community health workers). Studies that evaluated cost as an outcome were also included. Screening studies were excluded unless they evaluated an intervention to modify a CKD-related outcome. Both authors independently reviewed all manuscripts and discrepancies were discussed to reach consensus on article inclusion.
Data Synthesis and Analysis
All studies were described by study type, intervention, and clinical outcome. Study characteristics of interest included study design, country, population studied (indigenous vs non-indigenous, hemodialysis [HD] vs peritoneal dialysis [PD] vs CKD not on dialysis). Intervention characteristics recorded included intervention type. Clinical outcome characteristics included the type of clinical outcome measured, and the effect the intervention had on the clinical outcome. Blood pressure was not considered a renal outcome unless the study population had kidney disease.
Meta-analysis of data was not possible because of the heterogeneous nature of available studies.
Ethics
Ethics approval was not required for this type of study as it included only previously collected data.
Results
Search of MEDLINE, Embase, and Cochrane databases yielded 661 references (Figure 1). These were screened and duplicates removed to yield 59 manuscripts. Additional 23 references were added by hand searching and reviewing references, leaving 82 manuscripts for review. There were 26 studies that met criteria for inclusion in the review. Review of conference proceedings yielded 15 additional studies. Duplicates and screening studies were excluded, yielding 32 unique studies for inclusion in this review.

PRISMA flow diagram for scoping review.
Study Characteristics
The most common study design was cohort (15/32, 46.9%; Table 1), with prospective cohort studies being the most common (12/32, 37.5%). A minority of studies (2/32, 6.3%) were randomized controlled trials. There were equal numbers of observational (6/32, 18.8%) and survey (6/32, 18.8%) studies.
Study Characteristics.

Note. CKD = chronic kidney disease.
Equivalent numbers of studies were performed in Australia and Canada (9/32, 28.1% for both), and in New Zealand, United States, and United Kingdom (3/32, 9.4% for each). Indigenous persons were the study population in 11 (34.4%) of studies. Half of the studies targeted CKD (non-dialysis patients). Only 1 study (3.1%) looked at outcomes in PD patients, and only 1 study (3.1%) evaluated outcomes in patients affected by HD-dependent acute kidney injury (AKI).
The greatest proportion of studies (34.4%) evaluated multidisciplinary interventions, whereas telehealth (32.3%) and satellite clinics (25.0%) made up most remaining studies. All satellite clinic intervention studies examined outcomes in HD patients, whereas all multidisciplinary intervention studies examined outcomes in CKD patients. The single study performed in PD patients was a telehealth intervention.
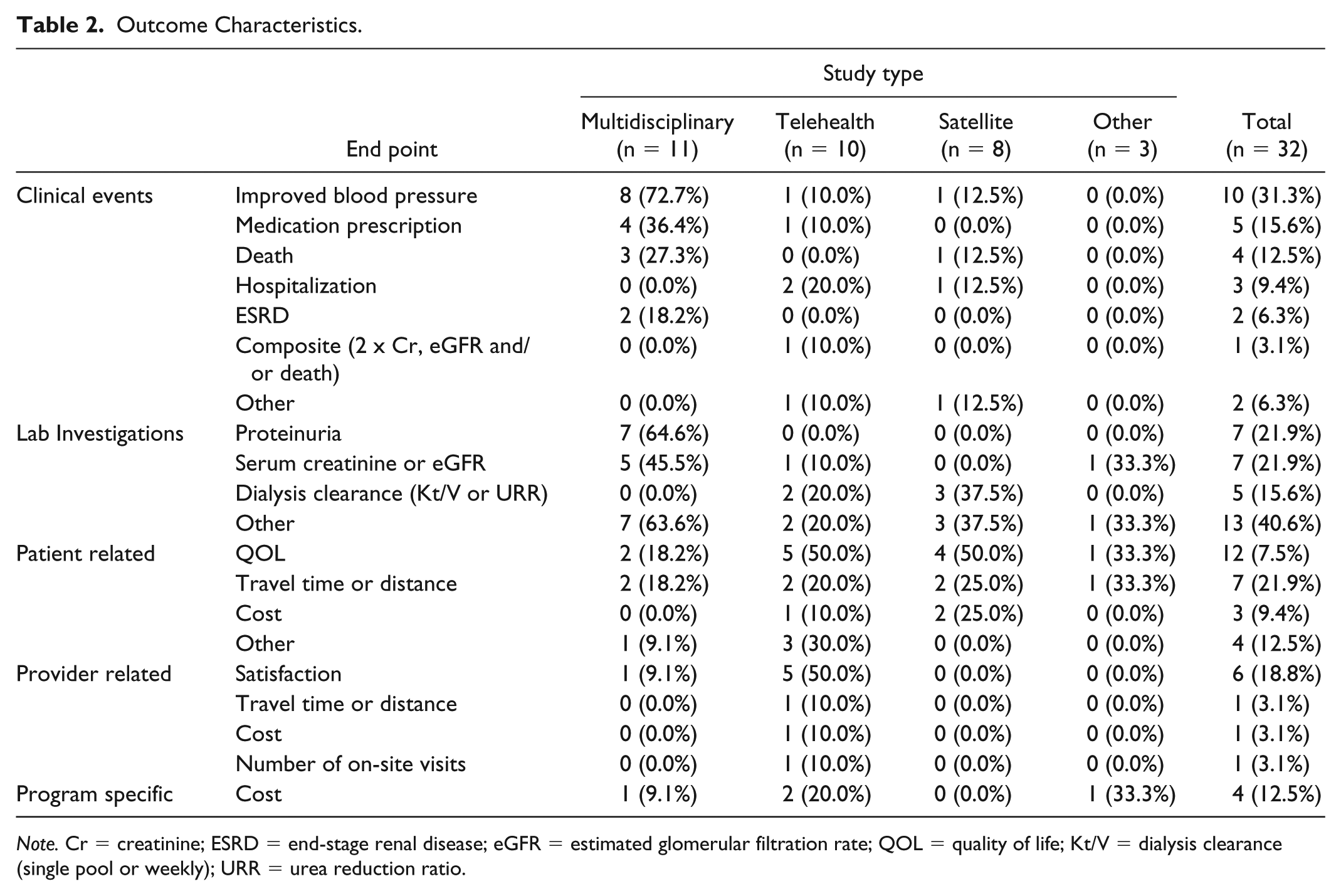
Outcome Characteristics
The most common clinical outcome measured was improvement in blood pressure (10/32, 31.3%) and was usually (8/10) measured by multidisciplinary intervention, such that it was the most common clinical outcome assessed in these studies. Death was infrequently evaluated (4/32, 12.5%). Incidence of end-stage renal disease (ESRD) was measured in 2 (6.3%) studies, both of which were multidisciplinary interventions (Table 2).
Outcome Characteristics.
Note. Cr = creatinine; ESRD = end-stage renal disease; eGFR = estimated glomerular filtration rate; QOL = quality of life; Kt/V = dialysis clearance (single pool or weekly); URR = urea reduction ratio.
The most common lab investigations measured were proteinuria (7/32, 21.9%) and serum creatinine/eGFR (7/32, 21.9%); these were measured with multidisciplinary interventions in CKD patients. Hemodialysis clearance was an outcome in 5 studies (15.6% total, 33.3% HD studies), 2 of which were telehealth and 3 of which were satellite HD studies.
Patient-centered secondary outcomes of interest were also included in this review. These included QOL, satisfaction, costs, and travel time. Patient QOL (12/32, 37.5%) and travel time or distance (7/32, 21.9%) were evaluated at least once in each study type. Patient-associated costs were rarely considered (3/32, 9.4%).
The most commonly described provider-related outcome was satisfaction with the intervention (6/32, 18.8%), most often (5/6) in telehealth settings. Program-specific costs were reported in 4 (12.5%) studies.
Description of Outcomes: Multidisciplinary
Multidisciplinary studies were any which included non-physician providers giving delegated care (such as nurses, nurse practitioners, dieticians, and community health workers). All multidisciplinary interventions were implemented in the CKD setting,8,12-22 with most (9/11, 81.8%) evaluating indigenous populations (Appendix Table A1).8,12-16,18-21 All studies utilizing multidisciplinary interventions for indigenous persons were performed in Australia, New Zealand, or Canada. 18
Components of multidisciplinary interventions were diverse. Specialist consultation was often led in the community by non-MD health professionals.12-18 These clinics may have also included home visits, 17 transportation of patients to pharmacy and lab, 13 or counseling about lifestyle choices.14-17
Nephrology MD specialists were used to advise via telehealth, 12 to travel to multidisciplinary remote clinics, 21 or to suggest medication adjustments. 13 One trial used a team that included a primary care provider MD, nurse practitioner, and diabetes specialist; this team modified antihypertensive therapy, made home visits, and provided culturally appropriate care regarding lifestyle and diet, to an indigenous population. 19
Multidisciplinary interventions showed significant improvements in consultation waiting time, 22 patient travel time, 21 and cost. 22 Program cost savings were in travel costs for providers. Satisfaction among staff and patients is high.8,12,18,20
Kidney function (eGFR or serum creatinine) regressed less,17,19 with decreased renal death. 16 Proteinuria was either unchanged 17 or improved.15,16,19 Kidney function was reported as an improvement in eGFR from before to after intervention 19 or change in eGFR over time compared between intervention and control groups. 17 Blood pressure was significantly improved.8,14,17,19,20 However, improvement in blood pressure was more challenging as CKD progressed. 18 Follow-up was longer than 12 months in only 1 study;15,16 after 3 years of intervention, the community health workers clinic handed over to local community workers. This transition was followed by increased blood pressure, renal death, and overall death.
Mortality was assessed in 2 studies. Researchers used a cluster randomized controlled trial in Thailand to assess the impact of a community-based multidisciplinary team on a composite end point of mortality, cardiac events, ESRD, and 50% increase in serum creatinine. 17 Although none of the individual components reached statistical significance, there was a 42% reduction in the composite end point in the intervention arm.
Hoy et al15,16 conducted the longest multidisciplinary intervention study that evaluated mortality. This 3.5-year study was conducted between 1995 and 1998, with subsequent follow-up in 2003 after handover of the initiative to a remote, Indigenous community in Australia. Systematic titration of medications for blood pressure and diabetes management was combined with risk factor counseling and follow-up with allied health professionals. Nephrologists were involved remotely for consultation. The study showed a 50% reduction in all-cause mortality and 57% reduction in renal deaths over the first study period from 1995 to 1998. However, following project handover to the community, clinical gains declined over time, with increased rates of renal death and overall death. The decline in outcomes may have been due to funding and rapid staff turnover.
Description of Outcomes: Telehealth
Telehealth involved a computerized link from a main central nephrology site to a remote unit with a camera and sound activated. In all studies, the patient was at the remote site with an assistant (health care worker), with clinical and physical exam information communicated to a nephrology specialist at the central site. Physical examination was accentuated in 1 study that evaluated PD patients, with Bluetooth-connected stethoscopes and cameras directed to the patient’s PD catheter exit site (Appendix Table A2). 23
Different telehealth HD models (standard virtual patient rounds vs telecase reviews with multidisciplinary teams) were compared in 1 study, showing no difference in the number of HD sessions, medication changes, or transfers to main hospital per month. 24
Remote patients on PD were targeted in only 1 study, in which in-person appointments at the main center were followed by telemedicine clinics thereafter. The telemedicine intervention associated with longer physician encounters, but patients’ driving time was reduced and QOL improved, with significant improvements in the physical component of QOL. 23
Telehealth for CKD patients25-27 showed benefits in travel time, 25 clinic attendance rates, 27 and QOL. 25 There was no change in burden of kidney disease 25 or a composite end point of doubling of serum creatinine, ESRD, and/or death. 27 Study duration ranged from 2 months 25 to 1 year. 27
Indigenous patients were evaluated with telehealth in only 1 study of satellite HD in New Zealand. 28 Providers and patients were satisfied with the satellite HD intervention, and there were improvements in physician travel time and costs.
Telehealth in HD units has been extensively studied;24,28-32 the most common model replaces physician visits to the satellite HD unit with a link in which an urban-based nephrology physician connects to the rural-based patient in a satellite HD unit.24,28,30-32 Use of this model has high levels of provider and patient satisfaction,28,30-32 with significant travel and cost savings for providers. 28 There were high rates of meeting standard benchmarks for laboratory investigations,24,32 with lower hospitalization rates30,31 and decreased health care-associated cost by US$46 613 per annum. 30
An alternative model replaced patient visits to an urban HD facility for review by a nephrology team, with telehealth connection to a patient at his or her satellite HD unit. 29 This second model improved patient attendance rate while requiring 1 to 11 patients in the telehealth clinic to maintain cost neutrality.
Description of Outcomes: Satellite
All satellite interventions evaluated the impact of a satellite HD unit on renal outcomes (Appendix Table A3).33-40 All studies described a satellite HD unit “spoke” as remote to the main central HD unit “hub,” but closer to patients whose treatments were in the satellite facility. Studies that evaluated telehealth interventions in satellite HD units28,30,31 are described in telehealth intervention, as the intervention in those studies was not the satellite clinic, but rather the telehealth system in the satellite clinic.
The study population included stable HD patients in all studies. However, 1 study evaluated outcomes not only in stable HD patients with acute medical issues but also dialysis-dependent AKI treated in a satellite HD clinic. 37 This intervention decreased transfer to the non-satellite HD facility, decreased travel time for families of patients with AKI requiring HD. Mortality was not compared with a pre-intervention program level; however, mortality of patients with AKI requiring HD was comparable with the published standards.
Satellite HD units show comparable mortality with the published controls when treating dialysis-dependent AKI. 37 On the contrary, satellite HD shows improved survival in rural satellite HD cohorts compared with urban HD units (odds ratio [OR] 0.77, P < .0001) after correcting for multiple demographic and clinical factors. Hospitalization rates may be increased 38 or equivalent. 40
Hemodialysis clearance (dialysis clearance [Kt/V] or urea reduction ratio [URR]) was equivalent 34 or improved in satellite HD units.38,39 There was no statistically significant difference between in-center and satellite HD patients when other laboratory investigations were studied (eg, hemoglobin, calcium, phosphate, albumin, parathyroid hormone [PTH], and HbA1C).33,34,39 Patient QOL was equivalent34,38 or improved.34,36 Improvements in QOL occurred in the dialysis stress domain and in the cost and time associated with transportation to HD.34,37
The cost associated with hospitalization appeared equivalent between satellite and in-center HD patients; 38 however, the total cost for satellite HD (median cost Can$99 888/patient per year, range Can$80 372-215 918) was higher. 35
Description of Outcomes: Other
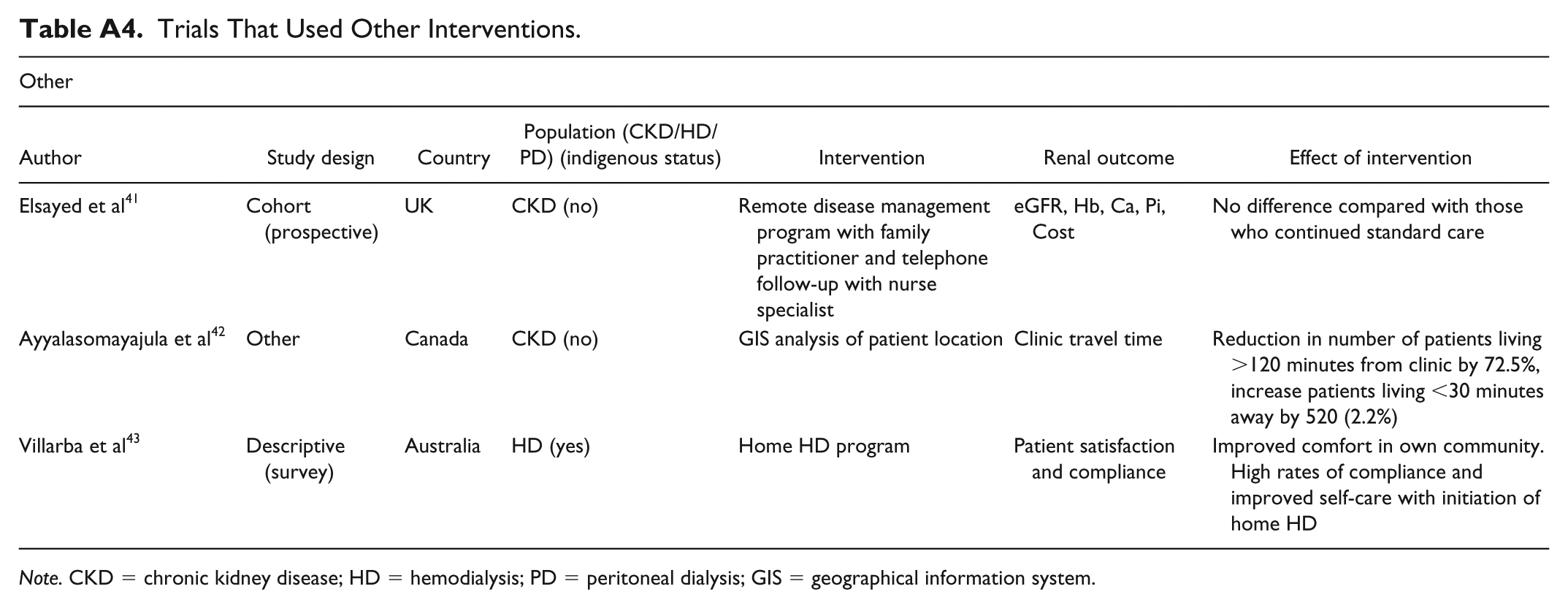
Elsayed et al 41 offered stable CKD patients the choice between continuing standard nephrology follow-up, or a remote, community-based, disease management program created by a consultant nephrologist but implemented and followed by a rural family physician. 41 After 12 months, there was no difference in the laboratory values (mean eGFR, hemoglobin, calcium, and phosphate), but the cost for patients was dramatically reduced in the intervention arm, measured by annual carbon saving of 507 kg CO2 (Appendix Table A4).
Ayyalasomayaiula et al 42 used geographical information system, linked to a laboratory database, to identify locations for hypothetical new clinics that minimize travel time for rural patients with CKD. 42 The technique identified 4 ideal locations for CKD clinics that reduced the number of patients living more than 120 minutes away by 72.5%. When only 2 or 3 clinics were added, changing locations modified the number of patients living more than 120 minutes away by a large range, from 32 to 65%.
Villarba et al 43 evaluated an indigenous community without any dialysis facilities, whose members with ESRD either died or moved permanently outside their community to a non-indigenous community with dialysis facilities. 43 A remote home HD program was developed in cooperation with tribal elders, with strategies to address cultural and language challenges. Study participants reported improved comfort in their own community.
Discussion
Chronic kidney disease affects indigenous and remote persons at a disproportionately high rate, with earlier onset and worse outcomes.2-4,7,8 This is due to decreased access to health care and monitoring, long travel distances, multiple socioeconomic factors, and lack of a culturally safe health care infrastructure.6-10 It is feasible to screen these populations to identify people who might benefit from kidney disease care,8,44-46 but the optimal model to provide this care remains uncertain. This review identifies the best evidence for interventions to enhance renal outcomes in both indigenous and remote persons with kidney disease.
Studies showing positive outcomes in indigenous persons had a couple consistencies. First, successful programs were developed with authorities in the indigenous community. For example, Hoy et al 16 engaged the Tiwi Land Council and Tiwi Health Board to implement a community health workers clinic. Shephard et al 8 formed a partnership with the Umoona Tjutagku Health service to create a management program, named by the indigenous community “The Umoona Kidney Project.” Villarba et al 43 worked with tribal elders to initiate a culturally safe home HD program. 43 Second, interventions were more successful when indigenous patients remained in their own community. This was facilitated by nephrologists, 21 nurse practitioners,12,20 or a multidisciplinary team 19 going directly to the community. Alternatively, health workers were trained and remained in the indigenous community.8,13-16
All studies in indigenous persons were identified in Australia, New Zealand, or Canada. There were no studies from the United States, despite the high rates of ESRD in the American indigenous population. 47 There may be reasons for this geographic pattern of studies. First, the United States is more urbanized than Australia, New Zealand, or Canada. 48 This may decrease the populations available to study in rural or remote communities. Second, for a physician to use and bill for telehealth, patients must be in an approved originating site during the telehealth encounter. 49 These originating sites may be challenging to find in indigenous communities. On February 9, 2018, the Bipartisan Budget Act of 2018 was signed into law, which expanded originating sites. 50 More interventional studies are thus needed in multiple settings to enhance outcomes in this unique population.
Most studies performed in patients with non-dialysis-dependent CKD (11/16, 69%) were multidisciplinary interventions.8,12-22 Despite the diversity of the components of the multidisciplinary intervention, clinical end points were consistently improved, including eGFR, ESRD, and mortality.16,17,20 However, follow-up was greater than a year in only a few studies.8,15,17 In the trial with the longest follow-up, handover of the study to community workers was followed by significant worsening of clinical outcomes, including death. 15 This highlights the importance of implementing and studying long-term sustainable interventions in remote populations, to assure that there is no decay of short-term benefits over the long-term. With increasing evidence for the use of sodium–glucose cotransporter-2 (SGLT-2) inhibitors, there is a continued need to assess the use of evidence-based interventions at a community and population level. The current studies analyzed begin to establish a body of evidence for active interventions in this area. The analysis of prescribing trends, when that data are available, would facilitate an understanding of the degree of knowledge translation to clinical practice across urban and rural communities.
All interventions in remote HD patients involved patients remaining in their community and the delivery of HD services either at28,43 or close to their home.33-41 The provision of HD in units closer to a patient’s home associated with improved dialysis clearance,38,39 QOL,33,36,38 and survival. 40 However, the health care-associated costs of care may be higher than in-center HD, depending on the operating capacity of the satellite HD unit and transportation costs. 35 The prevalence of ESRD continues to expand worldwide, 51 increasing pressure on health care funders to provide patients access to renal replacement close to their home. Although clinical outcomes may be improved with satellite HD units over urban dialysis centers, PD-related or kidney transplantation-related outcomes are equivalent or superior to HD,52,53 at a significantly lower cost.52,54 Thus, growth of ESRD population in remote and indigenous centers might be better managed by expansion of PD and renal transplantation rather than satellite HD centers. Alternatively, if satellite HD units must be built, replacing nephrology team visits with telemedicine may reduce costs. 30
Only 1 study including PD patients was identified in this review. Krishna et al 23 performed QOL surveys in rural PD patients who had transitioned from in-person to telehealth appointments, showing reduced patient travel time and improved QOL with telemedicine. 23 On the contrary, there has been significant technological enhancements in the care of PD patients, with real-time remote monitoring of blood pressure and patient weight being incorporated via internet,55,56 telephone,57-60 tablet, 61 or the PD machine itself.57,58 Photographs or video can also be incorporated. 61 However, evidence for clinical benefit with newer technologies remains sparse. 55 Although these technologies hold a great deal of promise for remote and indigenous persons, more research is required before widespread use can be recommended.
This review has several strengths. First, it identifies characteristics of successful interventions to enhance renal outcomes in indigenous populations. Second, it identifies a range of evidence-based interventions in CKD, HD, and PD that enhance patients’ outcomes in remote areas. Although meta-analysis of the data was not feasible due to the heterogeneity of trials, several important recommendations could be made. There were also important weaknesses. First, this review was limited to interventional trials that described clinical outcomes in renal disease. This limitation may have excluded studies that could improve the strength of the conclusions. On the contrary, we defined the study inclusion criteria to optimize the quality of the studies included. Second, the identified studies were limited to developed nations. However, this was also intentionally chosen a priori, so that recommendations could be generalizable to developed regions with remote and indigenous persons.
This review highlights the need for more research interventions in indigenous and remote communities with kidney disease, with long-term follow-up and measurement of clinical renal outcomes.
Footnotes
Appendix
Trials That Used Other Interventions.
| Other |
||||||
|---|---|---|---|---|---|---|
| Author | Study design | Country | Population (CKD/HD/PD) (indigenous status) | Intervention | Renal outcome | Effect of intervention |
| Elsayed et al 41 | Cohort (prospective) | UK | CKD (no) | Remote disease management program with family practitioner and telephone follow-up with nurse specialist | eGFR, Hb, Ca, Pi, Cost | No difference compared with those who continued standard care |
| Ayyalasomayajula et al 42 | Other | Canada | CKD (no) | GIS analysis of patient location | Clinic travel time | Reduction in number of patients living >120 minutes from clinic by 72.5%, increase patients living <30 minutes away by 520 (2.2%) |
| Villarba et al 43 | Descriptive (survey) | Australia | HD (yes) | Home HD program | Patient satisfaction and compliance | Improved comfort in own community. High rates of compliance and improved self-care with initiation of home HD |
Note. CKD = chronic kidney disease; HD = hemodialysis; PD = peritoneal dialysis; GIS = geographical information system.
Acknowledgements
The authors would like to acknowledge Dr. Michael Green and Dr. Karen Yeates.
Ethics Approval and Consent to Participate
The Health and Science Research Ethics Board at Queen’s University waived the requirement for formal ethics approval since this all data used in this study had been previously collected and published.
Consent for Publication
Consent for publication has been provided by all authors.
Availability of Data and Materials
The data analyzed during this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.