
Abstract
Rationale:
Acute focal bacterial nephritis (AFBN) has mainly been reported in pediatrics. It may be an underdiagnosed condition in adults because it resembles acute pyelonephritis (APN) in its clinical presentation.
Presenting concerns of the patients:
Two young women (25 and 27 years old, respectively) presented with complaints compatible with a diagnosis of APN. However in both, fever was of high grade, persistent for several days in spite of antibiotic administration, and there was demonstrated worsening of the inflammatory biomarkers. A contrast-enhanced computed tomography (CECT) led to the diagnosis in both cases.
Diagnoses:
Contrast-enhanced computed tomography reveals the most sensitive and specific images of AFBN. This includes wedge-shaped lesions with decreased enhancement, which may be focal or multifocal.
Interventions (including prevention and lifestyle):
Antibiotic therapy for at least 3 weeks.
Outcomes:
Resolution of AFBN was obtained after 3 weeks of antibiotics.
Lessons learned:
Our 2 cases illustrate the importance of CECT imaging to confirm the diagnosis of AFBN. Interstitial bacterial inflammation may have a worse prognosis if not diagnosed early and efficiently treated. Unlike APN, the management of AFBN requires at least 3 weeks of antibiotics to prevent the development of renal scarring and renal abscess.
What was known before
The diagnosis of acute focal bacterial nephritis is seldom made because it resembles acute pyelonephritis (APN) clinically. Therefore, patients are managed as in APN, without the need of imaging, and antibiotics are prescribed for a short period.
What this adds
The specific findings of acute focal bacterial nephritis (AFBN) in contrast-enhanced computed tomography may overcome the underdiagnosed condition of AFBN.
Introduction
Acute focal bacterial nephritis (AFBN) or acute lobar nephronia was first described in 1979. 1 It is defined as focal areas of nonliquefactive necrosis in the cortical areas of the kidney.2,3 It is therefore considered to be a complicated form of acute pyelonephritis (APN) and lies on the spectrum between APN and abscess.2,4 To date, it has mainly been reported in children. In adults, it is poorly described in the literature and reported only in small case series.5,6
The diagnosis of AFBN, which resembles APN clinically, can be challenging. Under diagnosis of AFBN could represent a serious issue, as it may expose patients to under treatment and potential further complications.7,8 The use of contrast-enhanced computed tomography (CECT), which demonstrates the most sensitive and specific images of AFBN, may account for the recently reported increased incidence of this disease. 9 In this article, we report 2 cases of AFBN diagnosed by CECT and review the literature of the main differences between AFBN and APN.
Case Presentation
Patient #1
A 25-year-old woman presented with high-grade fever (38.9°C) and flank pain for 3 days. She did not have dysuria. She had been treated with oral antibiotics for the same complaints several days earlier. She had costovertebral angle tenderness. Her laboratory investigations demonstrated leukocytosis (12 800/µL), elevated C-reactive protein (CRP; 215 mg/L) and positive nitrites in the urine with 40 to 50 leukocytes per high-power field. The admission diagnosis was APN. Abdominal ultrasound (Figure 1A) demonstrated a hyperechoic area at the upper pole of the right kidney with mild perinephric fluid and hypoperfusion in the same area by power Doppler (Figure 1B). Based on these imaging findings and the prolonged febrile period, AFBN was suspected and subsequently confirmed by CECT which revealed a wedge-shaped area with decreased enhancement (Figure 2A). The patient’s condition improved with meropenem treatment. Urine and blood cultures isolated an extended spectrum beta-lactamase (ESBL) Escherichia coli. Therefore, we deescalated to ertapenem. The advantages of the latter include its convenience as a single daily-dose outpatient therapy and its excellent perfusion in the kidney. Figure 2B shows the gradual improvement after 2 weeks and 24 days of antibiotic therapy (Figure 2C).

(A) US showing increased echogenicity in the upper pole (arrow). (B) Power Doppler: hypoperfusion in the same area.

(A) CECT showing wedge-shaped area (Arrow). (B) After 2 weeks of treatment. C: At Day 24.
Patient #2
A 27-year-old woman presented with high-grade fever (39.4°C) and back pain with dysuria for 5 days, headache, and nausea. Clinically, she had mild right costovertebral angle tenderness.
Her laboratory investigations demonstrated an elevated CRP (275 mg/L), leukocytosis (20 400/µL), and pyuria. The admission diagnosis was APN, and the patient was started on ceftriaxone. Kidney ultrasound showed a right renal upper pole mass-like lesion with mild perinephric fluid. A CECT was obtained after 48 hours of persistent fever with rising CRP (303 mg/L), revealing multifocal wedge-shaped lesions (Figure 3A). Urine and blood cultures were negative. The patient’s condition improved rapidly after starting meropenem. The typical CECT lesions in a highly septic patient and the fear of ESBL-producing pathogen confined to the kidney justified the use of meropenem which was followed by ertapenem as outpatient therapy. Complete resolution of the lesions was obtained after 3 weeks of treatment (Figure 3B).
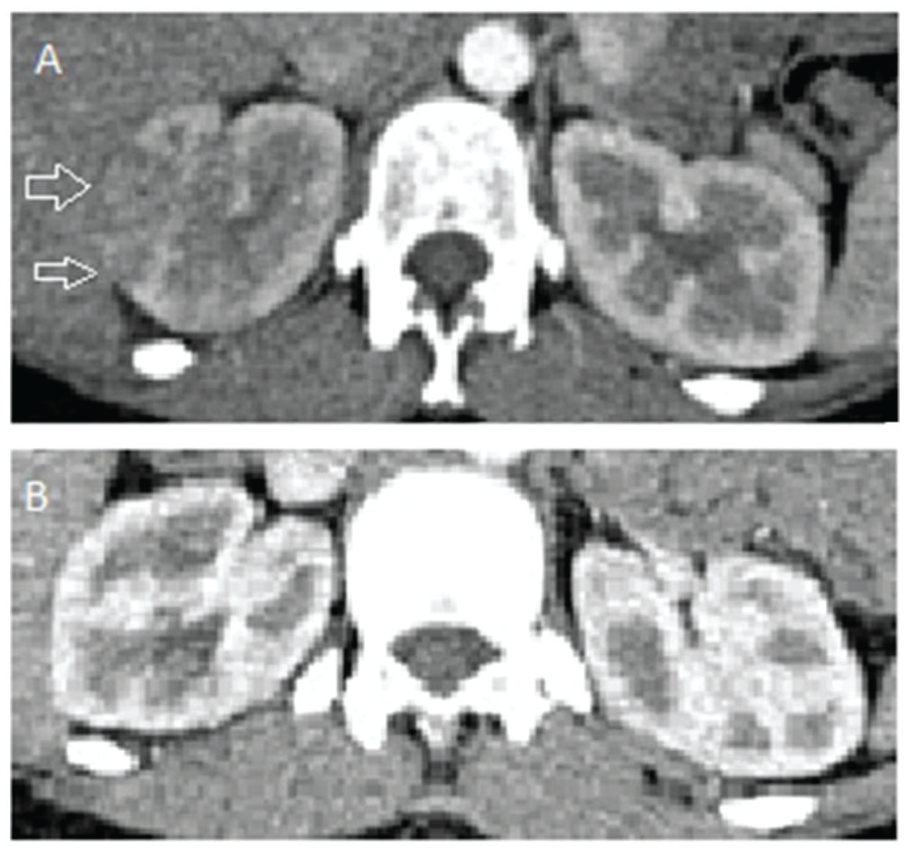
(A) Multiple wedge-shaped lesions (Arrow: multifocal). (B) Complete resolution after 3 weeks of treatment.
Discussion
Acute focal bacterial nephritis resembles APN clinically. In APN, imaging is usually not requested and patients are typically treated as outpatients for a short period of time. 9 Imaging is requested only when nonspecific symptoms dominate the presentation including nausea, severe vomiting, and abdominal guarding, mimicking other clinical conditions.6,9 Therefore, the diagnosis of AFBN may be delayed or even not considered. The latter is highlighted in a recent study where the same expert radiologist retrospectively reviewed the images of 377 patients admitted at one hospital with APN over a 5-year period. Acute focal bacterial nephritis was diagnosed in 57 cases (prevalence of 15.1%) based on the US findings of renal focal mass(es) of decreased, or less frequently increased, echogenicity and decreased vascularity on Doppler or when CECT revealed one or multiple wedge-shaped areas of decreased kidney density. 10
In an effort to help lower the threshold for AFBN suspicion, several studies have compared the symptoms and the inflammatory markers between AFBN and APN. In addition to flank pain, fever was the most consistent differentiating feature where body temperature was higher and more persistent in AFBN and accounted for a longer hospitalization.11-14 Some atypical manifestations were also observed more frequently in AFBN including peri-umbilical pain, right or left lower quadrant pain, and the presence of Murphy’s sign.
C-reactive protein and leukocyte count in blood were also consistently higher in AFBN than APN. 12 Pyuria may be missing in 6% to 25% of cases4,11 because the bacterial infection is speculated to be localized in the parenchymal tissue. 11 Typically, AFBN yields high negative blood culture and low positive urine culture results. In adults, Sieger et al 6 identified a positive urine culture in 60% of cases and a positive blood culture in only 19% of cases. Both can be negative as in our second patient, and thus only high index of suspicion (persistent fever after 48 hours of antibiotic, high leukocyte count, and CRP) led to performing a CECT which confirmed the diagnosis.
Acute focal bacterial nephritis can not only develop in patients with predisposing risk factors including diabetes mellitus, kidney transplant, liver cirrhosis, ureteral stone, vesico-ureteral reflux, or neurogenic bladder but can also occur in immunocompetent patients. The role of oral contraceptive use as a risk factor is reported along with a 75% female predominance for AFBN.5,10
Although the infection is usually ascending, it can be hematogenous as well, and thus can lead to renal scars and renal abscess. 4 E. coli dominates, followed by Klebsiella and Staphylococcus aureus. 13 Kidney ultrasound may show a focal mass with poorly defined margins and is 90% sensitive and 86.4% specific for the diagnosis compared to computed tomography (CT). 4 The presence of perinephric fluid observed in our 2 patients is reported more frequently in cases of AFBN than APN. 10 In contrast to AFBN, renal abscesses have well defined margins and the content shows liquefaction, whereas tumors are more echogenic.15,16 Power Doppler demonstrating hypovascularized zones can be useful in making the diagnosis (Figure 2B).
Contrast-enhanced computed tomography is the gold standard for diagnosing AFBN and typically appears as a poorly defined wedge-shaped lesion with decreased contrast enhancement, and represents the inflammation of a single lobe of the kidney. Multiple lobes can also be affected as in our second case (acute multifocal bacterial nephritis).
The optimal treatment period in adults is not known. In our 2 patients, clearance of the renal lesions of AFBN, documented by CECT, was obtained after 3 weeks at least of antibiotic treatment. This period has been shown to be necessary to achieve a good renal outcome in pediatrics.17,18
A prospective study including 80 children with AFBN compared 2 antibiotic regimens (3 vs. 2 weeks). It showed 17.1% treatment failure in the latter and none in the former. 18 Another study identified 2 distinct CT patterns of AFBN: simple and complicated. In the latter group where all treatment failures were observed, the patients were older and had longer duration of fever. The authors recommend at least 3 weeks of antibiotics in this group. 17 We also believe that such treatment period is needed in adults until a consensus is reached.
On the other hand, as far as we know, no data related to long-term outcomes in treated adults is available.
In conclusion, with certain presenting features, AFBN deserves to be differentiated from APN, as it may expose patients to complications if undertreated. A CECT scan should be considered when patients with presumed APN have persistent high-grade fever and worsening of inflammatory markers. Diagnosis can be confirmed by the typical CECT findings.
Footnotes
Ethics Approval and Consent to Participate
The case report study: “Acute Focal Bacterial Nephritis: Two Cases and Review of the Literature” was approved by the research ethics committee of the University Hospital of Sharjah in the United Arab Emirates.
Consent for Publication
Consent for publication has been provided by all authors.
Availability of Data and Materials
The data analyzed during this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.