
Abstract
Background:
Recent studies have demonstrated that measurement of areal bone mineral density by dual-energy x-ray absorptiometry (DXA) predicts fractures in patients with chronic kidney disease (CKD). However, whether fracture risk prediction through bone mineral density (BMD) is enhanced due to the assessment of biochemical markers of chronic kidney disease and mineral and bone disease (CKD-MBD) or clinical risk factors is not clear. We hypothesized that in a select cohort of patients managed in a CKD clinic, that combining T-Scores with biochemical markers would optimize fracture discrimination than using DXA alone.
Objective:
To examine the relationships among BMD, biochemical markers of CKD-MBD, and fracture risk across Kidney Disease Improving Global Outcomes (KDIGO) glomerular filtration rate (GFR) categories G3a to G5.
Design:
Retrospective study.
Setting:
Patients were recruited from the multidisciplinary CKD clinic, Regina General Hospital, Canada.
Patients:
A total of 374 patients who received a DXA scan upon initial referral to Regina Multidisciplinary CKD Program from January 31, 2001 to January 31, 2010, were included in this study. The patients were followed for a total of 5 years.
Methods:
We conducted a retrospective review of 374 consecutive patients who underwent DXA imaging at the point of entry into our multidisciplinary CKD program. Areal BMD, T- and Z-Scores were obtained at the lumbar spine, total hip, mean of left and right femoral neck, and the one-third radius. We collected data on demographic, cross-sectional biochemical markers of mineral metabolism and fractures (identified through self-reported questionnaires, hospital electronic medical records, and physician billing records). We were able to gather data on 8/11 variables of Fracture Risk Assessment (FRAX) tool.
Results:
In our cohort, 14.3% of GFR categories G3a and G3b, 15.7% of GFR category G4, and 19.7% of GFR category G5 experienced a clinical fracture during the study period. On multivariate analysis, each decline of 1.0 SD in total hip BMD T-Score was associated with a significant increase in the risk of fracture (OR = 1.46, 95% confidence interval [CI], 1.12-1.89). Adding CKD-MBD markers and clinical risk factors did not further contribute to the model. Low BMD was the only independent risk factor for fracture in patients with CKD.
Limitations:
Self-reporting by patients and administrative records were used to identify fractures. We did not perform spine imaging to ascertain morphometric vertebral fractures. We were unable to gather all 11 variables of FRAX score and information on ethnicity. We were unable to capture site of fracture (hips, spine, etc) from billing records. Albumin excretion rates were not collected at baseline. Treatment of the underlying bone disease with pharmacotherapeutic agents may have attenuated patients’ fracture risk and thus underestimated the association between BMD and future fracture.
Conclusions:
Our findings confirm that BMD predicts fracture. The addition of cross-sectional CKD-MBD parameters and clinical risk factors to BMD did not add to fracture prediction. Prospective studies should investigate the utility of longitudinal biochemical markers on improving fracture risk assessment.
What was known before
There is emerging evidence that bone mineral density predicts fractures in patients with chronic kidney disease.
What this adds
Measurement of bone mineral density at the spine, hip, and femoral neck predicted future fractures. However, fracture prediction by total hip T-Score was not improved by adding clinical risk factors and markers of chronic kidney disease and mineral and bone disease to the risk-prediction model.
Introduction
Patients with chronic kidney disease (CKD) are at an increased risk for bone fractures.1-4 Fracture prevalence rates are more than 2-fold higher when glomerular filtration rate (GFR) is less than compared to when is greater than 60 mL/min/1.73m2, 5 and fracture risk increases further as kidney function declines.1,6 In 2010, after hip fracture, health-care-associated costs among patients with non-dialysis-requiring CKD were estimated to exceed $600 million, and the risk of mortality was more than double of that for the general population. 7 Therefore, the substantial medical and economic burden of fractures makes it crucial to identify CKD patients at high fracture risk.1,2
Optimal methods to assess fracture risk in CKD patients are not well defined. Recently, two prospective studies in patients with moderate- to end-stage kidney disease supported the use of measuring areal bone mineral density (BMD) through dual-energy x-ray absorptiometry (DXA) to identify patients at risk for fracture.8,9 These studies reported that fracture risk increased with low BMD, that BMD predicted fracture similarly in patients with and without CKD, and that the World Health Organization (WHO) T-Score thresholds for predicting risk could be applied to CKD patients. However, similar to the general population, there are limitations to the use of DXA as a fracture risk classification tool. In severe CKD, the sensitivity of BMD for fracture discrimination varies widely (between 20% and 80%), with many patients sustaining fractures despite normal or high BMD.10-13 Thus, to improve the sensitivity of BMD testing for fracture risk classification, there is interest in using clinical risk factors to predict risk, and several studies suggest that the Fracture Risk Assessment (FRAX) tool classifies risk in CKD patients.14,15 Owing to the lack of large prospective cohorts of CKD patients which measure skeletal outcomes, no study has assessed whether or not combining areal BMD and clinical risk factors for fracture with biochemical markers of CKD-mineral and bone disease (CKD-MBD) improves the sensitivity of fracture risk screening.
Between 2001 and 2010, the institutional policy in our multidisciplinary CKD clinic was to refer all patients for BMD testing by DXA. In the following investigation, we hypothesized that BMD testing at entry in our CKD clinic would predict future fractures and that the addition of biochemical markers of CKD-MBD (parathyroid hormone [PTH], alkaline phosphatase [ALP], calcium, and phosphorus) would improve the sensitivity of BMD for fracture prediction. To test our hypothesis, we evaluated 374 consecutive CKD patients who underwent a DXA scan between 2001 and 2010 and who were followed longitudinally to examine relationships between BMD, biochemical markers of CKD-MBD, and fracture risk across Kidney Disease Improving Global Outcomes (KDIGO) GFR categories G3a to G5.
Methods
Eligibility Criteria
Between January 31, 2001, and January 31, 2010, a total of 473 patients were referred to the Regina Multidisciplinary CKD program. Of these, 431 patients were G2 to G5ND (not on dialysis). Guidelines at the time suggested performing routine BMD tests in patients with GFR categories G3a through G5ND regardless of fracture-associated risk factors. This was performed in 407 (G3-5ND) patients, but we were able to collect data in 374 patients and are the subject of this study. Patients with a previous history of fracture at the time of the referral to the program also received a DXA scan and were included in the analysis. Any patient found to be meeting criteria for low bone mass or osteoporosis through DXA and/or a previous history of fracture was referred to a metabolic bone disease specialist for further management. Ethical approval to conduct this research was granted by our Institutional Research Ethics Board (approval iD: REB-11-21).
Measures
Bone mineral density measurements were made on a single device (GE Lunar Corp, Madison, WI, USA) at the lumbar spine, total hip, mean of left and right femoral neck, and the one-third radius. We assessed the areal BMD (g/cm2) and T-Scores using the National Health and Nutrition Examination Survey reference population. We also used the WHO definitions of BMD categories: normal bone density (T-Score ≥ –1.0), low bone mass (T-Score between −1.0 and −2.5), and osteoporosis (T-Score ≤ –2.5).
We included both atraumatic and traumatic fractures in this analysis, as previous investigations have reported that their exclusion may result in under-reporting of fragility fractures. 16 Fractures were identified using a combination of self-reported interviews at the time of undergoing DXA scans, hospital records from the emergency room or in-patient stay, office visits with specialists dealing with fractures collected from the Medical Information Quality database (MIQS), which is a repository for all nephrology-related information in our institution. For patients outside of our geographic area of our Institution, billing records of family physicians and specialists were obtained from the provincial Ministry of Health. Linkage was made through Health Insurance Card number, a unique number assigned by our provincial ministry of health used for billing all insured services. As fractures result in pain and associated with high recall, we felt that they were less likely to be underreported. Baseline fractures included patients with a history of fractures at the time of DXA scan. We did not include multiple fractures per patient in this report. Fracture was coded as a binary variable.
Laboratory measures were extracted from the MIQS database. The closest values within 12 months of the DXA scan were obtained for baseline creatinine, which we used to calculate eGFR in mL/min/1.73m2 by the 4-variable Modification of Diet in Renal Disease formula, and markers of CKD-MBD (total serum calcium, phosphorus, PTH, and total ALP). From January 2001 to May 2012, PTH levels were analyzed using the Immulite 2000 Intact PTH assay, a solid-phase, 2-site chemiluminescent enzyme labeled immunometric assay (CMIA). From May 2012, we used ARCHITECT Intact PTH assay (Abbott Diagnostics, Abbott Park, IL, USA), a two-step sandwich immunoassay using CMIA.
Patient demographics and clinical risk factors for fracture were collected from MIQS and included age, sex, body mass index (BMI), comorbid conditions (diabetes), glucocorticoid use, current smoking status, cause of renal disease, family history of fractures, and personal history of a bone fracture. Data on ethnicity was not collected. For women, we also recorded menopausal status and use of hormone replacement therapy.
Statistical Analyses
Variables related to kidney function and risks of fracture were selected a priori as potential covariates. Heavily skewed continuous data were transformed using the natural log. We chose to evaluate fracture as our primary outcome a priori. The relationship between clinical risk factors and total hip T-Score was examined using a linear trend analysis in analysis of variance and cross-tabulation. Multiple regression was used to examine the adjusted association between all the covariates and total hip T-Score.
We tested for the presence of multicollinearity using variance inflation factors (VIFs). A VIF above 4 would require further investigation. The final model including all covariates did not show any signs of serious multicollinearity. A series of logistic regression models were developed to examine the relationship between BMD and risk factors associated with fracture risk. The initial model examined total hip T-Score as a univariate predictor of fracture. A sequential multivariable model adjusted for eGFR (per mL/min/1.73 m2), clinical risk factors (age, sex, BMI, smoking, family history of fracture, history of fracture, and prednisone use), biochemical markers of CKD-MBD (calcium [per mmol/L lower], phosphate [per mmol/L higher], ALP [per U/L higher], and intact PTH [per pmol/L higher]). To examine whether total hip BMD was similarly associated with fractures by CKD severity, we tested a total hip T-Score by eGFR interaction within the final multivariable-adjusted model. In companion analyses, we also tested the final model using the T-Scores from femoral neck, spine, and one-third radius to compare across sites. Missing data were imputed with multiple imputations using PROC MI in SAS, Version 9.3 (SAS Institute Inc, Cary, NC, USA). Statistical analyses were conducted with SPSS, Version 17.0 (SPSS Inc, Chicago, IL, USA). All statistical tests were 2-sided, and a P value < .05 was considered statistically significant for all analyses including interaction terms.
Results
Clinical Characteristics of the Study Population
A total of 374 patients were included in this analysis. Fifty-nine (16%) of the patients had a fracture during the 10-year follow-up period. Patients with fractures had lower GFR mL/min/1.73m2 (SD: 26.4 [1.7] vs 28.3 [0.7]), more females (50.9% vs 36.8%) and lower mean femoral neck and total hip T-Scores (–1.92 [0.15] vs −1.56 [0.06] and −1.45[0.16] vs −0.97 [0.07]), respectively (Table 1).
Clinical Characteristics of Study Participants by Incident Fracture Status.

Note. Continuous variables given as mean (standard deviation) for normally distributed variables and median (interquartile range) for nonnormally distributed variables. Categorical variables presented as No. (%). GFR = glomerular filtration rate; PTH = parathyroid hormone.
Clinical characteristics of study participants across total hip T-Score categories (≥–1.0, between −1.0 and −2.5, ≤–2.5) are shown in Table 2. Compared to those with a T-Score ≥ –1.0, participants with T-Score ≤ –2.5 were older (64.3 years vs 73.2 years, P = .0001), had lower BMI (32.3 vs 25.3, P < .0001), lower eGFR (30.5 vs 25.8, P = .0015), higher PTH (8.6 vs 11.2 pmol/L, P = .0015), and more incident fractures (13.3% vs 31.7%, P = .0119).
Clinical Characteristics of Study Participants by Total Hip T-Score Category.

Note. Continuous variables given as mean (standard deviation) for normally distributed variables and median (interquartile range) for nonnormally distributed variables. Categorical variables presented as No. (%). GFR = glomerular filtration rate; IQR: interquartile range; PTH = parathyroid hormone.
Clinical characteristics of study participants based on KDIGO GFR categories are shown in Table 3. Compared to those with GFR categories G3a to G3b, participants with GFR category G5ND had lower T-Scores (–0.82 vs −1.49, P = .0008), lower levels of serum calcium (2.35 vs 2.23, P ≤ .0001), and higher levels of serum phosphorus (1.16 vs 1.54, P ≤ .0001) and PTH (6.7 vs 11.7, P ≤ .0001; Table 3).
Clinical Characteristics of Study Participants by KDIGO GFR Categories.

Note. Continuous variables given as mean (standard deviation) for normally distributed variables and median (interquartile range) for non-normally distributed variables. Categorical variables presented as No. (%). KDIGO = Kidney Disease Improving Global Outcomes; GFR = Glomerular Filtration Rate; BMD = bone mineral density; ALP: alkaline phosphatase; IQR: interquartile range; PTH = parathyroid hormone.
Total Hip BMD as a Predictor of Incident Fracture
Relationships between each lower SD in total hip T-Score and incident fracture were determined (Table 4). In an unadjusted model, each lower SD in total hip T-Score was associated with a 46% higher odds of incident fracture (OR = 1.46; 95% confidence interval [CI], 1.12-1.89). In the second model, with the additional adjustment for eGFR, the odds of fracture remained significant at 1.44 (95% CI, 1.1-1.87). In the third model, after adjustment for clinical risk factors (age, sex, BMI, family history of fracture, previous history of fracture, smoking, and prednisone use), the odds of fracture remained similar (OR = 1.48; 95% CI, 1.09-2.02). In the fourth model, we included biochemical markers of CKD (calcium, phosphorus, ALP, and iPTH), and the odds of fracture remained the same (OR = 1.46; 95% CI, 1.12-1.9). In the final model, despite combining eGFR, clinical risk factors and biochemical markers of CKD-MBD, the relationship between total hip T-Score and incident fracture remained unchanged (OR = 1.47; 95% CI, 1.07-2.03). In Table 5, the association of T-Scores with incident fractures was compared between the total hip, femoral neck, lumbar spine, and distal radius in adjusted models. The odds of fracture per 1 SD lower in T-Score were similar for hip and femoral neck.
Relationships Between Total Hip T-Score and Incident Fracture.
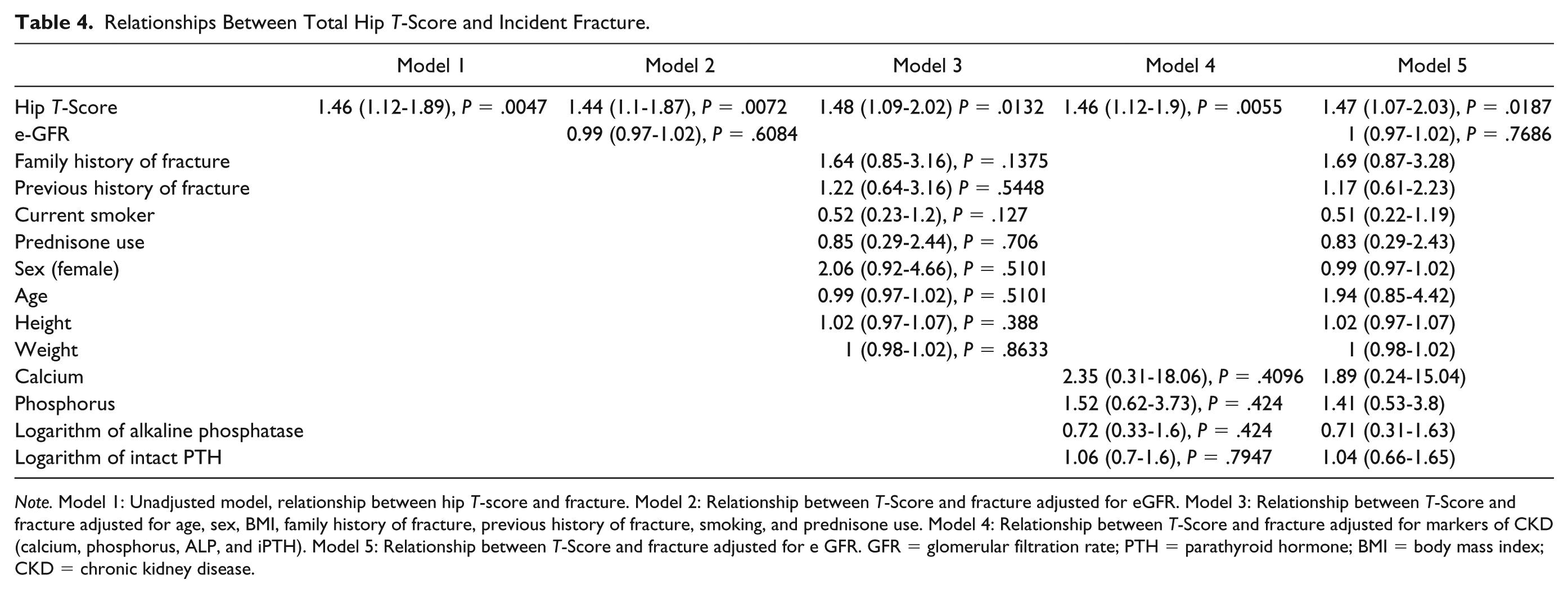
Note. Model 1: Unadjusted model, relationship between hip T-score and fracture. Model 2: Relationship between T-Score and fracture adjusted for eGFR. Model 3: Relationship between T-Score and fracture adjusted for age, sex, BMI, family history of fracture, previous history of fracture, smoking, and prednisone use. Model 4: Relationship between T-Score and fracture adjusted for markers of CKD (calcium, phosphorus, ALP, and iPTH). Model 5: Relationship between T-Score and fracture adjusted for e GFR. GFR = glomerular filtration rate; PTH = parathyroid hormone; BMI = body mass index; CKD = chronic kidney disease.
Adjusted Association of T-Scores at Different Sites With Incident Fracture in CKD Patients.

Note. Models are adjusted for age, sex, diabetes, BMI, calcium, phosphate, alkaline phosphatase, intact PTH, and eGFR. CKD = chronic kidney disease; CI = confidence interval; BMI = body mass index; PTH = parathyroid hormone; GFR = glomerular filtration rate.
Discussion
This investigation tested the utility of adding clinical risk factors and cross-sectional biochemical markers of CKD-MBD to measurement of BMD for fracture prediction in patients managed in a real-world CKD program. Consistent with our hypothesis, we found that measurement of BMD at the spine, hip, and femoral neck predicted future fractures. Contrary to our hypothesis, we did not find that fracture prediction by total hip T-Score was improved by adding clinical risk factors and markers of CKD-MBD to the risk-prediction model. We also confirmed findings from other studies that lower T-Scores are associated with lower GFR independent of age, 3 and that fracture incidence and prevalence is higher in patients with more severe kidney disease.4-6
Naylor et al 1 reported 3-year cumulative fracture incidence rates based on sex and eGFR, ranging from 1.6% for men with eGFR > 60 mL/min/1.73 m2 and 9.6% for women with eGFR < 15 mL/min/1.73 m2. In contrast, 16% of our patients had a cumulative fracture incidence over 10 years. In contrast to Naylor et al, 56% of our patients were in G4 and G5. Sixteen percent of patients with G4 and 20% of patients in G5ND had a fracture over a 10-year follow-up period. Based on the distribution of sex and category of CKD in our cohort, our fracture incidence rates are consistent with those reported in the Ontario data sets. Only recently has measurement of BMD by DXA been proven to predict fractures in patients with CKD. In patients with predialysis CKD and on hemodialysis, prospective studies have demonstrated that lower BMD at the hip and forearm predict future fractures and that the WHO T-Score thresholds are acceptable to fracture risk classification.9,17,18 Our study obtained measures of BMD at entry into our CKD program irrespective of clinical risk of fracture and followed patients prospectively based on the severity of their underlying kidney disease. Fracture events were ascertained and confirmed through review of patient-reported outcomes and fracture-associated doctor visits recorded in our electronic health record. Thus, our study is unique and advances the field of fracture risk screening in CKD in that it is the first report from a CKD program and demonstrates the real-world benefit of measuring BMD at the point of entry to the general nephrology clinic irrespective of fracture risk. We believe that this type of study design provides accurate validation of the utility of measuring BMD for fracture risk screening in CKD patients.
We found that lower BMD was associated with both baseline and incident fractures. Similarly, cross-sectional studies in CKD patients have reported that fractures occurred despite normal or high BMD.11,19,20 Furthermore, in the general population, half of all fragility fractures occur in patients with BMD above the osteoporotic threshold. For this reason, the FRAX tool was developed. The FRAX incorporates 11 clinical risk factors for fracture, with or without BMD, to predict 10-year absolute risk of hip and major osteoporotic fracture. The FRAX tool was demonstrated to improve the sensitivity of fracture risk prediction through DXA. 17 In patients with CKD, a recent study had reported that FRAX discriminated and predicted fractures. 21 However, whether the combination of clinical risk factors with BMD improves predictive discrimination is not clear.22,23 Therefore, we tested whether combining a subset of the clinical risk factors in FRAX (age, sex, race, weight, height, family history of fracture, glucocorticoid use, and smoking history) with BMD at the total hip would improve fracture prediction. We found that none of the clinical risk factors predicted fracture. Although reasons for the lack of association between fracture and clinical risk factors cannot be mechanistically explored in this epidemiologic investigation, one can hypothesize that in renal osteodystrophy, the underlying defects in bone quality due to uremia override those due to classical clinical risk factors. This hypothesis needs to be tested in prospective studies.
Renal osteodystrophy is a complex heterogeneous disorder of the bone which is due to abnormal calcium and phosphate metabolism, decreased calcitriol synthesis, increased PTH levels, metabolic acidosis, and defective bone mineralization. 18 Studies have found that elevated levels of PTH predict bone loss in patients with CKD 24 and that cross-sectional measure of ALP predicts fractures in patients on dialysis.9,25 Our CKD program measured cross-sectional levels of CKD-MBD biochemical markers, including PTH, ALP, calcium, and phosphorus as parts of a CKD management protocol. In this investigation, we included in our prediction models those CKD-MBD measures that were obtained within 12 months of BMD, and we did not find that they were associated with either baseline or incident fractures. The lack of association between markers of CKD-MBD and fracture may be due to their dynamic nature. Markers of CKD-MBD change in response to disease severity and to treatment with vitamin D, calcimimetics, antiresorptives, and osteoanabolic agents. Therefore, it is likely that the cross-sectional biochemical measures of CKD-MBD included in our prediction models did not reflect their overall skeletal effect during the course of treatment for hyperparathyroidism or CKD-MBD. In light of our findings, future work should test whether serial measures of CKD-MBD markers are predictive of fracture events. Indeed, a previous study had used time-averaged levels of CKD-MBD markers to reflect the dynamic properties of PTH on the skeleton. 20
Limitations
We retrospectively collected data from paper charts and MIQS which limited us to imaging within the Regina Qu’Appelle Health Region (RQHR). For events that occurred outside of the geographic area of RQHR, billing records from the Ministry of Health were obtained. Self-reporting by patients and administrative records were used to identify fractures, and we did not perform spine imaging to ascertain morphometric vertebral fractures. Although it may have underestimated risk, fracture is an event that results in pain and high recall, and it is unlikely that we would have underascertained clinical fracture events. Short of radiological confirmation, we used all available resources at hand to capture most of the fractures. Despite our best attempts, there is a likelihood of recall bias. We did not have data on serial measurements of BMD. Although we were unable to determine if changes in measurements of CKD-MBD over the course of care in the CKD program affected fracture risk, our study does inform our community on the clinical significance of a single BMD measurement over the medium- to long-term period.
We were also unable to determine the exact site and date of fracture, as we were dependent on self-reported questionnaires before the DXA scan, hospital electronic medical records, and billing information from the Ministry of Health. As we collected the data, most of the paper charts have been archived by the Health Region, a new electronic health record for the region was introduced in 2014, and not all of the electronic data were transferred. It will be unfortunately be very hard to retrieve additional data. We did not collect data on markers of bone resorption; however, ALP is a useful marker of bone formation in patients with CKD, 23 and as the prevalence of glucocorticoid use was low, it is unlikely that uncoupling of remodeling activity was common for our patients. Data on patient’s albumin excretion rates was not collected at baseline. Albuminuria has been identified as an independent risk factor for fracture,26-28 but data on albumin excretion rates was not collected at baseline. Although we used laboratory data obtained within 12 months of DXA, most laboratory data were obtained within 6 months of imaging. Although we were unable to collect the entire set of FRAX variables to include in our models, we did include a subset (8/11) of the FRAX variables in logistic models and tested their association with fracture. We did not capture data on ethnicity in our cohort. Our findings may have been biased by referral of all patients with previous fractures or osteoporosis to a metabolic bone disease specialist for management. Treatment of the underlying bone disease may have attenuated patients’ fracture risk and thus underestimated the association between BMD and future fracture. Furthermore, referral and treatment may have negated the utility of cross-sectional measures of PTH, ALP, calcium, and phosphorus to predict incident fractures.
Conclusions
In conclusion, this is the largest Canadian cohort of CKD patients with DXA scans to our knowledge. We found that BMD predicts fractures across the spectrum of CKD and that in the context of a CKD program, combining BMD with clinical risk factors and cross-sectional markers of CKD-MBD does not improve fracture risk prediction. As fractures lead to significant morbidity and mortality, we believe that there is a role for BMD testing in CKD programs. Future research is needed on the utility of serial measures of CKD-MBD biomarkers and BMD to predict fractures in CKD patients. The major strength of our study is that the population is a large unbiased cohort of patients with CKD who underwent measurement of BMD by DXA per CKD-MBD treatment protocol, regardless of history of fracture.
Footnotes
Acknowledgements
The authors wish to acknowledge Dr Jennifer St Onge, PhD from Research and Performance Support, Regina General Hospital, for her contribution. They also wish to acknowledge Dr David McCutcheon, Vice President Medicine, Regina Qu’Appelle Health Region, for reviewing the manuscript.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Research Ethics Board of Regina Qu’Appelle Health Region (approval iD: REB-11-21).
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Author Contributions
B.P. conceived, designed, and drafted the study. N.T. and C.Y.N. assisted with the drafts. T.F. performed the statistical analysis. T.L.N. contributed to the drafts and edited the final manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.