
Abstract
Background:
Bone mineral density (BMD) decreases postrenal transplantation. Evidence demonstrating the effects of bisphosphonates on BMD and fracture risk beyond 1-year posttransplant is sparse in existing literature, but remains essential to enhance clinical outcomes in this population.
Objective:
Our study aimed to systematically review and meta-analyze the current literature on the use of any bisphosphonate in the adult renal transplant population beyond the first year of renal transplant to determine its effect on BMD and fracture incidence.
Design:
We conducted a systematic review and meta-analysis of primary research literature that included full-text, English-language, original randomized clinical trials (RCTs) and observational studies.
Setting:
Patient data were primarily captured in an outpatient setting across various studies.
Patients:
Our population of interest was patients older than 18 years who received deceased/living donor kidney transplantation and any bisphosphonate with a follow-up greater than 12 months posttransplantation.
Measurements:
The primary outcome was change in BMD from baseline. Secondary outcomes were the incidence of fractures and effects of other confounders on bone health.
Methods:
We included RCTs and observational studies that satisfied our inclusion criteria. Each study was analyzed for risk of bias and data were extrapolated to analyze for overall statistical significance accounting for heterogeneity of studies.
Results:
Sixteen studies (N = 1762) were analyzed. The follow-up ranged from 12 to 98 months. There was a nonsignificant improvement in BMD with bisphosphonate treatment persisting into the second and third years posttransplant at the lumbar spine. The calculated standardized mean BMD difference was −0.29 (−0.75 to 0.17), P = .22. Only 5 studies reported a total of 43 new fractures. Prednisone (P < .01), low body weight (P < .001), low body mass index (P < .01), and male gender (P < .05) correlated with reduced lumbar and femoral BMD.
Limitations:
Limitations of this review include the use of BMD as a surrogate outcome, the bias of the included studies, and the incomplete reporting data in numerous analyzed studies.
Conclusions:
We demonstrate no statistically significant benefit of bisphosphonate treatment on BMD beyond the first year postrenal transplantation. Despite heterogeneity of treatment, a differential nonsignificant improvement in lumbar spine BMD was consistent and may be clinically relevant.
Trial Registration:
PROSPERO CRD42019125593
What was known before
Rapid bone loss occurs in the first year postrenal transplantation but is a chronic disease. Existing systematic reviews identify a benefit of bisphosphonates in reducing bone mineral density (BMD) loss in the first 12 months posttransplant.
What this adds
This current review adds there is no statistically significant benefit to bisphosphonate treatment on BMD beyond 1 year postrenal transplantation.
Introduction
End-stage renal disease (ESRD) is associated with renal osteodystrophy (osteitis fibrosa, adynamic bone disease, and osteomalacia).1-4 A well-functioning renal allograft ameliorates many metabolic abnormalities associated with the development of mineral and bone disorders (MBDs) of ESRD. However, renal transplant recipients are particularly susceptible to bone damage due to a multitude of factors including preexisting bone disorders, immunosuppression, and alteration in the renal-bone metabolism axis.5,6
Bone mineral density (BMD) measured by dual-energy X-ray absorptiometry (DEXA) has been shown to decrease below 2 standard deviations (SDs) posttransplantation, 7 with estimated 3%-7% loss in the lumbar spine in the first year.8-11 Ongoing vertebral bone loss (approximately 2%/yr) has been demonstrated in longitudinal evaluation of BMD in 70 renal transplant recipients. 12
There are few studies demonstrating that low BMD predicts fractures in renal recipients. Akaberi et al 13 showed that low hip BMD predicted fractures in 238 renal recipients. The prevalence of fractures in the posttransplant population is up to 4-fold greater than pretransplant statistics, ranging widely between 5% and 44%, likely due to variations in observation time, definitions of fractures included, and the presence of diabetes.14-17
There is currently no established strategy for the prevention of posttransplant osteopenia and osteoporosis. Bisphosphonates, which inhibit osteoclast activity, are widely accepted as a treatment for osteopenia and osteoporosis in the general population. 18 They have also been shown to protect against bone loss in the renal transplant recipients,1,7,19,20 although a specific risk is the potential to exacerbate a baseline low-turnover adynamic state.1,21,22
The currently available research on bisphosphonate use in the renal transplant population is limited to analysis of randomized clinical trial (RCTs) within the first year posttransplant18,23-25 The first year posttransplant is wrought with confounding factors including the physiologic adjustments in metabolism, the uremic effects of ESRD, the fluctuant nature of the posttransplant course, and aggressive immunosuppression.
Our study aimed to systematically review and meta-analyze the current literature on the use of any bisphosphonate in the adult renal transplant population beyond the first year of renal transplant to determine its effect on BMD and fracture incidence.
Methods
Eligibility Criteria
We conducted a systematic review and meta-analysis of primary research literature that included full-text, English-language, original RCTs and observational studies. Our population of interest was patients older than 18 years who received deceased/living donor kidney transplantation and any bisphosphonate with a follow-up greater than 12 months posttransplantation (Figure 1). Supplemental Table S1 summarizes the inclusion and exclusion criteria of our review.

Summary of study timelines in postrenal transplant patients on bisphosphonate therapy.
Search Strategy
Electronic searches were performed in MEDLINE, EMBASE, and the Cochrane Register of Controlled Trials (CENTRAL) between 1946 and 2017 (Figure 2). A sample search strategy is outlined in Supplemental Figure 1.

Schema of literature search.
Data Extraction and Outcome Measures
Each included study was assessed in conjunction by 2 authors (A.L. and A.W.) for data extraction (Tables 1-4). The primary outcome was the change in BMD from baseline. The secondary outcomes were the incidence of fractures and the effects of other confounders that may modify the risk of osteoporosis and fractures.
Duration of Bisphosphonate Therapy and Follow-up in Postrenal Transplant Patients.

Note. IU = international unit; IV = intravenous; NS = normal saline; BMD = bone mineral density. White is RCT, Grey shaded region is Observational trials.
Baseline Characteristics of Included Studies.

Note. IU = international unit; NA = not applicable; IV = intravenous; BMD = bone mineral density; NS = normal saline; NCRR = National Center for Research Resources; NIH = National Institutes of Health.
Change in Bone Mineral Density in Postrenal Transplant Patients Between Bisphosphonate and Control Groups.

Note. BMD = bone mineral density; I = intervention; C = control; n = number; AMTD = adjusted mean treatment difference; CI = confidence interval. White is RCT, Grey shaded region is Observational trials.
Fracture Incidence in Postrenal Transplant Patients Between Bisphosphonate and Control Groups.

Note. I = intervention; C = control; BMD = bone mineral density; PTH = parathyroid hormone; HR = hazard ratio; CI = confidence interval. White is RCT, Grey shaded region is Observational trials.
Bias Assessment
Articles were independently assessed by each reviewer (A.L. and A.W.), and dichotomized to low/high risk of bias based on standardized scoring systems. An RCT was considered low risk if it satisfied a score of 8 or more based on the Cochrane Risk of Bias Tool Criteria (Supplemental Table S2). 43 An observational trial was considered low risk if it satisfied a score of 3 or more based on the Newcastle-Ottawa Criteria (Supplemental Table S3). 44
Statistical Analysis
A standardized mean difference (SMD) and its 95% confidence interval (CI) were calculated to account for heterogeneity of different units of pre- and posttransplant measurements. 45 Using the 95% CIs, the SDs were then derived. 46 Subsequently, forest/funnel plots were created using the Cochrane Collaboration RevMan v5.3 software. 46 A random effects model was used to account for clinical heterogeneity of the meta-analyzed studies. Values of I 2 >50% and P < .10 were considered to indicate significant heterogeneity.
Results
Description of the Search
The search strategy yielded 1084 articles between 1946 and 2017. All titles and abstracts were reviewed independently by 2 authors (A.L. and A.W.) in accordance with inclusion criteria (Figure 2). Thirty-five articles were fully reviewed. Fourteen articles were differentially categorized between reviewers. These were independently reviewed and resolved by a third author (D.T.W.) to ascertain eligibility.
Description of Studies
Sixteen studies met full inclusion criteria (Table 1), including 8 randomized trials26-33 and 8 observational studies.34-41 Two RCTs28,30 and 7 observational studies,34-36,38-41 were considered to have low risk of bias (Supplemental Figures S2 and S3).
The total sample size was 1762 patients; 683 patients were treated with bisphosphonates while the remaining were allocated to various comparison groups. Bisphosphonates used included alendronate, alendronate/risedronate, pamidronate, zolendronate, ibandronate, and etidronate. Comparators included no therapy, calcium and/or vitamin D, calcitriol, placebo, an alternative bisphosphonate, and no control group. Baseline characteristic data of each study are summarized in Table 2.
From the RCTs, 226 patients were prescribed a bisphosphonate with a concomitant treatment with Ca and/or vitamin D in 212 patients. Bisphosphonate-treatment duration ranged from 1 to 24 months, with a follow-up duration of 12 to 24 months (Table 1). From the observational studies, 457 patients were prescribed a bisphosphonate. Of these patients, 223 had a concomitant treatment with Ca and/or vitamin D. Precise treatment was not clearly specified in an additional 624 patients. The range for bisphosphonate treatment was 12 to 36 months with a follow-up duration of 12 to 98.4 months (Table 1).
BMD measurement was performed using DEXA in all studies, with results most often expressed as T-scores representing the number of SDs that the measurement falls from the mean of a young population. A T-score of −1 to −2.5 describes osteopenia and less than −2.5 is diagnostic of osteoporosis. 47 Results were also reported as bone mineral content or Z-scores that describe the number of SDs from the mean value of gender and age-matched adults (Z-score less than or equal to −2 suggests abnormal bone loss).
Change in BMD
One year posttransplant
Thirteen studies demonstrated at least one site of improvement in BMD, while the other 3 studies30,32,36 showed nonsignificant changes. However, only 2 studies28,39 were able to capture patient data from the immediate peri-transplant period. At 12 months posttransplant, Walsh et al 28 identified a significant change in BMD in the intervention group vs control group, at the lumbar spine, +2.3% vs −5.7%, adjusted mean treatment difference (AMTD) 7.78%, P < .001. T-scores were also significantly different in the intervention vs control group at both the lumbar spine (−0.13 ± 0.73 vs −0.51 ± 0.66, P < .05) and the femoral neck (0.13 ± 0.55 vs −0.22 ± 0.69, P < .05) at 12 months. 39 Both intervention groups showed significant improvement with bisphosphonate persisting into the second28,39 and the third year 39 posttransplantation at the lumbar spine, with no significant difference at the femoral neck (Table 3).
One year postinitiation of bisphosphonate
Thirteen studies captured BMD data at least 12 months postinitiation of bisphosphonate treatment. Only 2 of these studies did not exhibit a significant increase in BMD 32 or Z-score 30 in the intervention vs control group in the lumbar spine at 12 and 32 months posttreatment. 32
Unlike the lumbar spine, all studies showed minimal change in BMD measurements at the femoral neck except for 3 studies31,33,39 that showed a significant change (Table 3). Result interpretation of the significantly different Z-scores between groups posttreatment was inconclusive in the study by Tillmann et al 34 as pretreatment measurements were also different. Cruz et al 40 also found different T-scores at the femoral neck posttreatment (change in T-score +1.6% ± 0.6%, P < .001), but did not provide raw data of the control group to allow for comparison.
Using the calculated SMD between the intervention (bisphosphonate) and control groups, Figures 3 and 4 summarize the study findings that include pre and postbisphosphonate treatment information on BMD, at the lumbar spine and femoral neck, respectively. Data from 4 RCTs29,31-33 and 3 observational studies34,38,41 were included in analysis. There is a nonsignificant improvement in BMD favoring the use of bisphosphonates, as evidenced at both the lumbar spine and femoral neck. There was no statistical heterogeneity noted when a random effects model was used. The funnel plot demonstrates reasonable dispersion (Supplemental Figure S4).
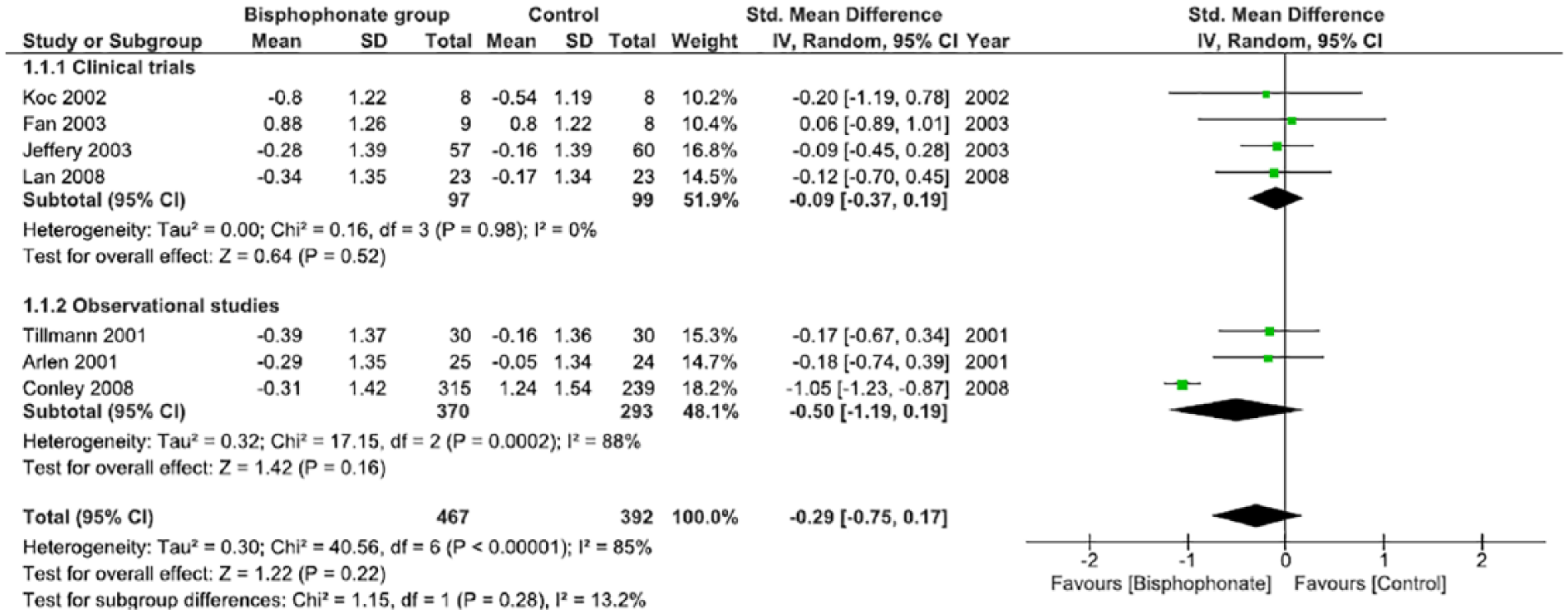
Change in bone mineral density at the lumbar spine in postrenal transplant patients between bisphosphonate and control groups.

Change in bone mineral density at the femoral neck in postrenal transplant patients between bisphosphonate and control groups.
Fracture Incidence
Fracture incidence was low but only reported in 5 studies28,30,36,38,41 with a total of 43 new fractures. Conley et al 38 reported benefit from bisphosphate treatment and decreased fracture rates (hazard ratio [HR] = 6.7, 95% CI = 6-6284, P < .01), despite only a small subset of patients (n = 3) with baseline osteoporosis at the femoral neck. Conley et al 38 noted that bisphosphonate treatment was associated with decreased probability of fracture-free survival (HR = 0.40, 95% CI = 0.29-0.73, P = .001) in the initial analysis, even though treatment was associated with significant reduction in bone loss at the femoral neck (HR = 1.56, 95% CI = 1.21-2.06, P < .001) and lumbar spine (HR = 1.48, 95% CI = 1.13-1.98, P < .01). However, after adjusted analysis, no association was identified between bone loss and fractures regardless of the bisphosphonate treatment. 38
Confounding Factors Affecting BMD
Immunosuppression
Four studies32,35,37,39 examined the effects of steroids on bone health. At baseline, patients with osteoporosis received a greater cumulative steroid dose than patients with osteopenia (1326.5 mg vs 724.5 mg; P < .01). 37 In a univariate analysis, prednisolone use was associated with osteoporosis (odds ratio [OR] = 5.18; 95% CI = 1.6-16.4, P < .01). 37 Jeffery et al 32 described prednisone as an independent predictor of low BMD (multivariate, P < .01). Alternatively, Naylor et al 35 found greater glucocorticoid exposure was not associated with a significant change in BMD at the lumbar spine, total hip, and femoral neck (P > .05), regardless of whether the patient had received osteoporosis treatment before. Similarly, no BMD differences were observed, 1 year posttransplant, in recipients receiving steroids. 39 The effects of cyclosporine on BMD were examined in 2 studies37,39 and demonstrated no effects up to 1 year posttransplant.
Body mass index
Three studies32,35,39 found that low body weight (P < .001) and body mass index (BMI) (P < .01) were correlated with reduced lumbar and femoral BMD in a univariate analysis. 32 Greater BMI was associated with a better BMD.35,39
Gender
Five studies32,34,35,37,39 examined the role of gender in BMD posttransplantation. Only one study 32 identified a baseline association between female gender and reduced lumbar and overall BMD (P < .05). The other studies found no significant difference in gender with respect to change in BMD, although bone density may change differentially depending on site in males and females.35,37 Alendronate increased the BMD at the lumbar spine and the hipbone in males (P < .05), but only at the lumbar spine in females (P < .05). 37 Male gender was also associated with a greater improvement in lumbar spine BMD in patients receiving osteoporosis treatment (P < .01). 35
Diabetes
Three studies32,37,39 examined the role of diabetes in bone loss, but none investigated the duration or control of diabetes pretransplantation. One study 32 identified pretransplantation diabetes as an independent risk factor for low BMD (P < .001), while the other 2 found a greater reduction in T-score at the lumbar spine in nondiabetic recipients (−0.52 ± 0.67 vs −0.15 ± 0.50, P < .01). 39 Consequently, diabetes was not a significant predictive factor in BMD (OR = 0.6). 37
Hemodialysis (HD) pretransplant
Only one study examined the impact of pretransplant HD duration on BMD. 39 The mean change reduction in T-score at the lumbar spine in the first year posttransplant was significantly greater in recipients who had been on HD for ≥12 months compared with those who had experienced dialysis <12 months (−0.67 ± 0.79 vs −0.39 ± 0.57, P = .001). 39
Smoking
In a multivariate analysis, 37 smoking was not a risk factor of BMD change posttransplantation (see Supplemental Table S2).
Discussion
This systematic review and meta-analysis is the first to investigate the bisphosphonate effects on increasing BMD and fracture prevention beyond the first year postkidney transplantation. A recently published meta-analysis by Wang et al 25 demonstrated that bisphosphonate treatment in general had a beneficial effect on BMD changes at both the lumbar spine and femoral neck, which is congruent with previous studies and established practice guidelines. 48 Although prior studies have shown that the most rapid decrease in lumbar spine BMD occurs within the first year posttransplantation (estimated at 3%-7%), we recognize declining BMD to be a problem of longer chronicity, often confounded by several factors unique to the immediate posttransplant period.8-11,25
In our study, we demonstrate no statistically significant benefit of bisphosphonate treatment on BMD beyond the first year posttransplant. There was heterogeneity in studies’ treatment choice and duration, but a nonsignificant improvement in lumbar spine BMD was consistently seen, while the effect appeared inconsistent in the femoral neck. Two studies28,39 captured peri-transplant patients’ data providing a baseline comparison, and both groups showed significant improvement with bisphosphonate treatment at the lumbar spine and femoral neck beyond 1 year posttransplant, when treatment was initiated at the time of transplantation and lasted for at least 1 year. This significant improvement persisted into the second28,39 and third year 39 at the lumbar spine but not at the femoral neck.
As bone loss progresses beyond the first year posttransplantation,9,12 we also analyzed the effects of bisphosphonates on BMD at least 12 months posttreatment initiation, regardless of the time from initial transplantation. Although bisphosphonate protocols varied widely across studies, 11 studies26-28,31,33,34,36,37,39-41 identified a significant increase in BMD at 12 months posttreatment as compared with baseline.
This review demonstrated no statistically significant change in BMD beyond 1 year with bisphosphonates. Thus, the benefit of bisphosphonates may be only evident within 1 year of transplant. This is an important observation, as the protective effect may be limited to the time with highest corticosteroid dosing, and other pre- and posttransplant factors such as inflammation or bone disease. This likely indicated that there is no benefit to bisphosphonate use in renal transplant recipients beyond 1 year posttransplantation.
Despite the significant changes found with the bisphosphonate treatment at the lumbar vertebral levels, only 3 studies31,33,39 displayed improvement at the femoral neck level. Although this does not translate directly to a lower fracture risk, this may extrapolate into ongoing hip fracture risks with greater protective effect at the lumbar spines in this population. This is a clinical consideration when risk-stratifying patients based on their BMD and fracture risks posttransplant. A significant limitation is that none of the studies captured fracture incidence as the sole primary outcome, likely given the paucity of fracture events.
Only one study 38 was able to interpret fracture results beyond reporting incidence and found no difference (HR = 0.40; 95% CI = 0.29-0.73, P = .001) in fracture rate after bisphosphonate treatment in their adjusted analysis. 38 Thus, the clinical significance of bisphosphonate therapy on patient morbidity with fracture prevention remains to be established.
Steroid use in both the early and long-term posttransplant periods has been shown to cause increased bone loss. 37 Specifically, prednisone doses of >7.5 mg/d results in trabecular bone loss in most patients. 41 Calcineurin inhibitors have also been implicated in bone loss in animal models. 37 While all studies that examined steroid use reaffirmed their deleterious impact on bone health, the effect of bisphosphonates in patient populations that had received higher cumulative steroid doses was not congruent. Only Huang et al 37 was able to demonstrate that bisphosphonates resulted in a greater improvement in BMD at the lumbar spine in those with osteoporosis at baseline versus osteopenic patients.
Previous systematic reviews on a similar population highlighted limitations of few studies and small sample sizes. Thus, the wide scope of literature analyzed in this study sought to address this by including both observational and randomized control trials with appropriate bias analysis. A second strength of this study is our focus on long-term effectiveness of bisphosphonate treatment. It is important to recognize that the predominant population to which these data apply is well beyond the initial 12-month posttransplant and that these are the patients who carry the burden of bone disease. Our findings on bisphosphonate treatment in BMD preservation beyond 12 months posttransplant highlight limited evidence supporting the use of bisphosphonates on renal osteodystrophy.
Limitations of this review include the use of BMD as a surrogate outcome, the bias of the included studies, and the incomplete reporting data in numerous analyzed studies. The most clinically relevant outcome is the incidence of fractures. Our review assessed BMD as the primary outcome, acknowledging that BMD is not an accurate indicator of clinically meaningful patient outcomes and quality of life. Other indicators, such as bone biopsy, should be considered as a surrogate outcome in the future, keeping in mind that biopsy is expensive, invasive, and biopsy-based treatment guidelines are not yet available. We had limited information on the bone turnover state of patients to identify patients who would potentially benefit from anti-resorptive therapy. Last, we recognize that high risk of bias was identified in 44% of our included studies. We elected to include these studies given the limited sample size of the renal transplant population. The conclusions drawn from this review, however, did not change based on this bias assessment.
In conclusion, our review finds no statistical evidence for improvement in BMD in renal transplant patients beyond the first year posttransplantation with the use of bisphosphonates. We detected a differential improvement in BMD favoring the lumbar spine more so than the femoral neck, which may have clinical implications despite nonsignificance. However, the limitations of this review highlight the need for randomized control trials in patients with quantified bone turnover status evaluating fracture risk. Also quantifying other surrogate outcomes such as bone biopsy is necessary to provide more definitive evidence for the use of bisphosphates for current practice guidelines. In our future work, we plan to explore the evidence on the safety profile of bisphosphonates in this unique population with a focus on graft function. Finally, anti-resorptive and anabolic therapies are alternatives to bisphosphonates in bone mineral diseases in the general population and investigation into the use of these therapies in the renal transplant population is an avenue to further treatment options.
Supplemental Material
updated_supplementary_file – Supplemental material for Effect of Bisphosphonates on Bone Health in Adult Renal Transplant Patients: Beyond the First Year Posttransplant—A Systematic Review and Meta-Analysis
Supplemental material, updated_supplementary_file for Effect of Bisphosphonates on Bone Health in Adult Renal Transplant Patients: Beyond the First Year Posttransplant—A Systematic Review and Meta-Analysis by Alyssa Lip, Ashley Warias, M. Khaled Shamseddin, Benjamin Thomson and D. Thiwanka Wijeratne in Canadian Journal of Kidney Health and Disease
Footnotes
List of Abbreviations
AMTD, adjusted mean treatment difference; BMD, bone mineral density; BMI, body mass index; CI, confidence interval; CKD, chronic kidney disease; DEXA, dual energy X-ray absorptiometry; ESRD, end-stage renal disease; MBD, mineral and bone disorders; RCT, randomized control trial; SD, standard deviation.
Ethics Approval and Consent to Participate
No ethics was required as our study reviewed existing literature.
Consent for Publication
AL and AW independent screened and reviewed all articles. AL and AW are the primary authors of this manuscript. MKS, BT, and DTW provided supervision and clinical expertise. All authors have consented for publication.
Availability of Data and Materials
All data is provided in the article and supplementary tables. Primary data can be obtained directly from the original articles.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.