
Abstract
Background:
Fistula creation is recommended to avoid the use of central venous catheters for hemodialysis. The extent to which timing of fistula creation minimizes catheter use is unclear.
Objective:
To compare patient outcomes of 2 fistula creation strategies: fistula attempt prior to the initiation of dialysis (“predialysis”) or fistula attempt after starting dialysis (“postinitiation”).
Design:
Cohort study.
Setting:
Five Canadian dialysis programs.
Patients:
Patients who started hemodialysis between 2004 and 2012, who underwent fistula creation, and were tracked in the Dialysis Measurement Analysis and Reporting (DMAR) system.
Measurements:
Catheter-free fistula use within 1 year of hemodialysis start, probability of catheter-free fistula use during follow-up, and rates of access-related procedures.
Methods:
Retrospective data analysis: logistic regression; negative binomial regression.
Results:
Five hundred and eight patients had fistula attempts predialysis and 583 postinitiation. At 1 year, 80% of those with predialysis attempts achieved catheter-free use compared to 45% with post-initiation attempts (adjusted odds ratio [OR]preVSpost = 4.67; 95% confidence interval [CI] = 3.28-6.66). The average of all patient follow-up time spent catheter-free was 63% and 28%, respectively (probability of use per unit time, ORpreVSpost = 2.90; 95% CI = 2.18-3.85). This finding was attenuated when accounting for maturation time and when restricting the analysis to those who achieved catheter-free use. Predialysis fistula attempts were associated with lower procedure rates after dialysis initiation—1.61 procedures per person-year compared with 2.55—but had 0.65 more procedures per person prior to starting dialysis.
Limitations:
Observational design, unknown indication for predialysis and postinitiation fistula creation, and unknown reasons for prolonged catheter use.
Conclusions:
Predialysis fistula attempts were associated with a higher probability of catheter-free use and remaining catheter-free over time, and also resulted in fewer procedures compared with postinitiation attempts, which could be due to timing of attempt or patient factors. Catheter use and procedures were still common for all patients, regardless of the timing of fistula creation.
What was known before
Predialysis fistula attempts are recommended by guidelines to avoid exposure to central venous catheters, but the extent to which they mitigate catheter use is unknown.
What this adds
Patients with predialysis attempts spent more dialysis time catheter-free. However, catheter usage was common in both groups (between 37% and 72% of follow-up time spent with a catheter in place) and as many as 20% to 55% of patients who received a fistula attempt did not use it within 1 year of starting dialysis.
Introduction
Arteriovenous fistulas (“fistulas”) are considered the preferred form of vascular access for hemodialysis due to lower rates of complications and mortality compared with central venous catheters (“catheters”).1-4 The Canadian, American, and European guidelines recommend the creation of a fistula prior to the initiation of hemodialysis to minimize exposure to catheters.5-7
The advantage of predialysis fistula attempts is that they allow time for the fistula to mature so the access is ready for use at the start of hemodialysis. 8 However, as many as 20% of people who have a fistula created prior to the initiation of hemodialysis will not use it due to death or lack of progression of their chronic kidney disease. 9 Many predialysis fistula attempts fail and patients start hemodialysis with a catheter or their fistula fails over time, requiring a second attempt and/or supplemental catheter use. 10 Finally, many urgent dialysis starts have no opportunity to create a predialysis fistula, and half of all fistula attempts occur after starting hemodialysis. 11 The extent to which predialysis and postinitiation fistula creation minimizes catheter use and their attendant complications is unknown. Insufficient information is available to prepare patients for their hemodialysis experience when choosing a fistula as their vascular access modality, including fistulas created after dialysis initiation.
We sought to describe the outcomes of patients who underwent predialysis fistula creation compared to those who had an attempt after the start of dialysis, with respect to the probabilities of achieving independent fistula use, remaining catheter-free over time, and the rate of access-related procedures. We hypothesized that a predialysis fistula attempt would be associated with more favorable outcomes, but anticipated high catheter use regardless of the timing of fistula creation. This exploration into 2 different patterns of care and their consequences (as opposed to fistula patency and functionality) may help guide clinical decision-making, inform the patient-physician conversation regarding modality choice, and help to set realistic expectations.
Methods
Patient Population
This study included incident hemodialysis patients between January 1, 2004, and May 31, 2012, aged 18+ years, who received at least one fistula attempt. Focusing on fistula creation strategies, we excluded patients who started on, or transitioned to, peritoneal dialysis (PD) within 6 months and those who started dialysis with an arteriovenous graft. To increase generalizability, we also excluded patients with a life expectancy of less than 1 year due to metastatic cancer or other terminal illnesses, based on a review of the patient record.
Data Source
We conducted a retrospective cohort study using data from the Dialysis Measurement Analysis and Reporting (DMAR) system collected while it was operational in 5 Canadian dialysis programs (Southern Alberta Renal Program, Manitoba Renal Program, Sunnybrook Health Sciences Centre, London Health Sciences Center, and The Ottawa Hospital). Detailed baseline data were captured including demographics, comorbidities, laboratory values, and predialysis care. Access-related procedures and changes in patient status were collected longitudinally. All information was entered by trained staff and double-reviewed by experts to ensure accuracy and consistency in coding. We followed participants from dialysis start until the first of transplant, recovery of kidney function, transfer out of the dialysis program, transfer to PD (after 6 months), death, or the end of follow-up (August 31, 2012).
Predictor: Timing of Fistula Creation
The main predictor of interest was timing of fistula creation. Patients were categorized based on whether their first fistula creation attempt occurred before or after initiation of dialysis (“predialysis” or “postinitiation” group).
Primary Outcome: Catheter-Free Use
The primary outcome for this study was catheter-free use, defined as independent use of a fistula for hemodialysis (ie, without a catheter in place). We measured catheter-free use in 2 ways: (1) whether catheter-free use of a fistula was achieved—cumulative incidence of use over time and binary use (yes/no) by 1 year in patients with 1 year of follow-up, and (2) the probability that the fistula was used catheter-free during each day of follow-up. We recorded movement of patients in and out of periods of catheter-free use by tracking catheter insertions and removals. We allowed multiple fistula attempts when calculating catheter-free use. For example, if a patient’s predialysis fistula failed but they received a second attempt, any catheter-free use of the second fistula was included.
Secondary Outcome: Access-Related Procedures
We analyzed the rate of access-related procedures from the start date of dialysis. Procedures were then subcategorized as catheter-related or fistula-related. We defined access-related procedure rates as the number of procedures per person-year of follow-up from dialysis start. Because fistula patency is not assessed until after commencing dialysis, we did not include interventions occurring prior to dialysis in rate calculations. We did present the counts of those procedures separately, to study the procedural burden experienced by patients who received a predialysis fistula. The initial catheter insertions or fistula creations required for starting hemodialysis were considered predialysis procedures (ie, all patients had at least one predialysis procedure). Surgical explorations prior to fistula creation may have occurred before dialysis start in the postinitiation group.
Statistical Analysis
We summarized patient characteristics by the timing of fistula creation using standard methods (eg, means and percentages), as appropriate.
We described the crude probability of catheter-free use and proportion of time spent catheter-free. We looked at the cumulative incidence of achieving catheter-free use treating death, transplant, recovery of kidney function, and starting PD as competing risks. In this survival analysis, we censored observations that were still event free at study end or when the study participant was transferred to another program. We used the Fine and Gray model to estimate subhazard ratios (SHRs) for initial catheter-free use. We also studied the probability of achieving catheter-free use of a fistula by 1 year after hemodialysis start in participants who were still under observation at 1 year. We used binary logistic regression to estimate odds ratio (OR) of use at 1 year. We then analyzed the probability of catheter-free use for each day of follow-up using logistic regression of repeated Bernoulli trials within subject, using robust variance methods to account for the within-subject dependencies.
Crude procedure rates and counts with 95% confidence intervals (CIs) were described using Poisson regression. To obtain incidence rate ratios (IRRs), we modeled procedure rates using negative binomial regression to account for overdispersion.
We adjusted all regression models for age, sex, a history of diabetes mellitus, or cardiovascular disease (including coronary artery disease, congestive heart failure, cerebrovascular disease, and peripheral vascular disease), and whether the patient started dialysis as an inpatient. We also assessed for confounding effects of body mass index (BMI), cancer, estimated glomerular filtration rate (eGFR), starting in an intensive care unit, length of predialysis care, and anatomical location of first fistula creation attempt.
Sensitivity and Subgroup Analyses
We conducted several subgroup and sensitivity analyses to create more comparable groups to explain why differences may have occurred. We repeated the analysis of the proportion of time spent catheter-free starting follow-up from the date of fistula attempt (postinitiation group), and again from 3 months after the attempt (both groups) to allow for fistula maturation before starting the clock. This analysis showed whether postinitiation fistulas ever “caught up” to the success of their predialysis counterparts. We also restricted the analysis of the proportion of catheter-free use to those who achieved it at some point during follow-up. This analysis removed some unmeasured patient confounders, as all patients were healthy enough and followed for a sufficient duration of time, to achieve a functioning fistula.
Finally, we examined outcomes in prespecified groups to account for the additional urgent starts in the postinitiation group, including those who started dialysis as an outpatient and those with at least 4 months of predialysis care.
We used Stata 14 to conduct all analyses (www.stata.com). Research ethics approval and waiver of patient consent were obtained from each of the 5 participating programs.
Results
A total of 1091 patients with a fistula attempt met criteria for inclusion in the study (Figure 1). Five hundred and eight participants had predialysis fistula attempts, while 583 had postinitiation attempts. The predialysis group were an average of 3 years older, had a higher BMI, and longer predialysis care (see Table 1). The postinitiation group had more than double the inpatient starts, including a higher percentage of starts in an intensive care unit. The 2 groups did not differ by sex, eGFR at dialysis start, anatomical location of their first fistula creation attempt, or the presence of diabetes mellitus, cardiovascular disease, or cancer.

Cohort creation.
Patient Characteristics.
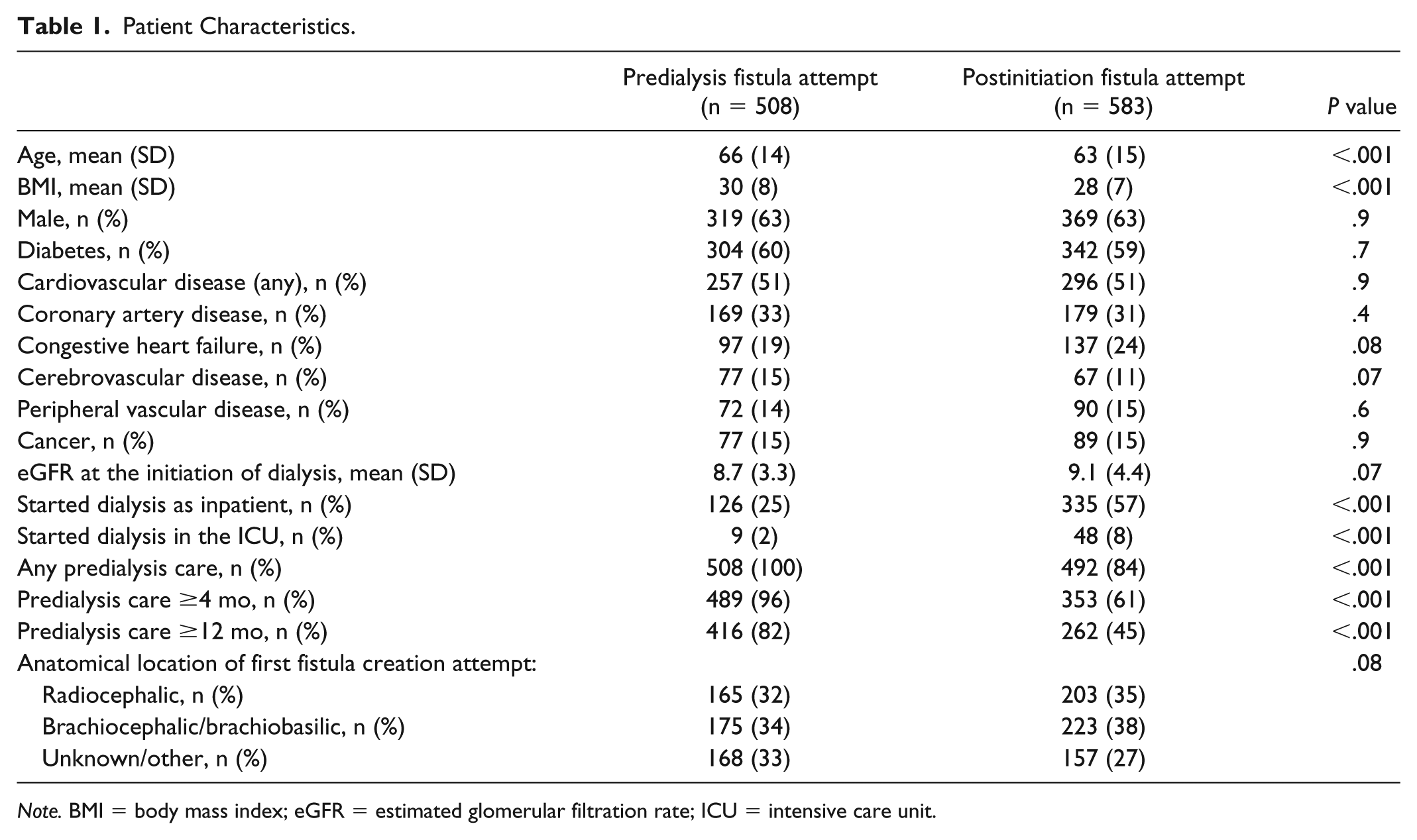
Note. BMI = body mass index; eGFR = estimated glomerular filtration rate; ICU = intensive care unit.
Median patient follow-up time was nearly 2 years, and was 4 months shorter for the predialysis group. Predialysis fistula attempts occurred a median time of 5 months (median = 4.7, interquartile range [IQR] = 2.3-11.7) prior to starting dialysis. Postinitiation fistula attempts occurred a median of 3 months (median = 3.3, IQR = 1.8-6.2) after starting dialysis. Reaching the end of the study period was the most common reason for termination of follow-up (60%), followed by death (25%), receipt of a kidney transplant (7%), transfer to another program (5%), switch to PD (2%), and recovery of kidney function (1%), and did not differ by group.
Catheter-Free Use
Sixty-four percent of patients achieved catheter-free use at some point during follow-up (81% of predialysis fistulas and 50% of postinitiation fistulas). Of those who achieved catheter-free use, the median time from dialysis start to use was zero months for the predialysis group (median = 0, IQR = 0-0)—thus if fistula use was achieved, most patients started dialysis using their fistula—and 9 months (median = 9.3, IQR = 6.5-13.3) for the postinitiation group. Figure 2 shows the cumulative incidence of patients achieving catheter-free use over time. At 6, 12, and 24 months, the probabilities of use were 76%, 79%, and 82% for the predialysis group, and 10%, 37%, and 54% for the postinitiation group, respectively (SHRpreVSpost = 3.08; 95% CI = 2.62-3.62).

Cumulative incidence of patients who achieved catheter-free fistula use across time.
Seven hundred and forty-nine patients had at least 1 year of follow-up. At 1 year, 80% of the predialysis group (n = 278/346) achieved catheter-free use, compared with 45% of the postinitiation group (n = 181/403) (ORpreVSpost = 4.67; 95% CI = 3.28-6.66).
On average, the predialysis group spent 63% of their follow-up time catheter-free, compared with 28% in the postinitiation group (Figure 3). Modeled probability of achieving catheter-free use over time was almost 3 times greater for the predialysis group (ORpreVSpost = 2.90; CI = 2.18-3.85). This effect was attenuated when allowing up to 3 months for fistula maturation (ORpreVSpost = 1.78; CI = 1.30-2.44), but remained significant. A similar attenuation occurred when comparing only those who achieved catheter-free use (ORpreVSpost = 2.06; CI = 1.51-2.82). The association between predialysis fistula attempts and greater proportions of time spent catheter-free was no longer significant when restricted to those who achieved catheter-free use and had at least 3 months for maturation (80% for the predialysis group and 73% for the postinitiation group; ORpreVSpost = 1.10; CI = 0.74-1.62).

Percentage of hemodialysis time spent catheter-free for all patients.
Access-Related Procedures
On average, the predialysis group had 1.61 procedures per person-year after the start of dialysis, while the postinitiation group had 2.55 procedures per person-year (see Table 2). A predialysis fistula attempt was associated with lower overall procedure rates (IRRpreVSpost = 0.65, CI = 0.58-0.73), catheter-related procedures rates (IRRpreVSpost = 0.62, CI = 0.52-0.74), and fistula-related procedures rates (IRRpreVSpost = 0.68, CI = 0.60-0.77). Considering the procedures prior to dialysis, the predialysis fistula group received on average 0.65 more procedures per person than the postinitiation group (1.65 vs 1.00).
Rates and Counts of Access-Related Procedures.
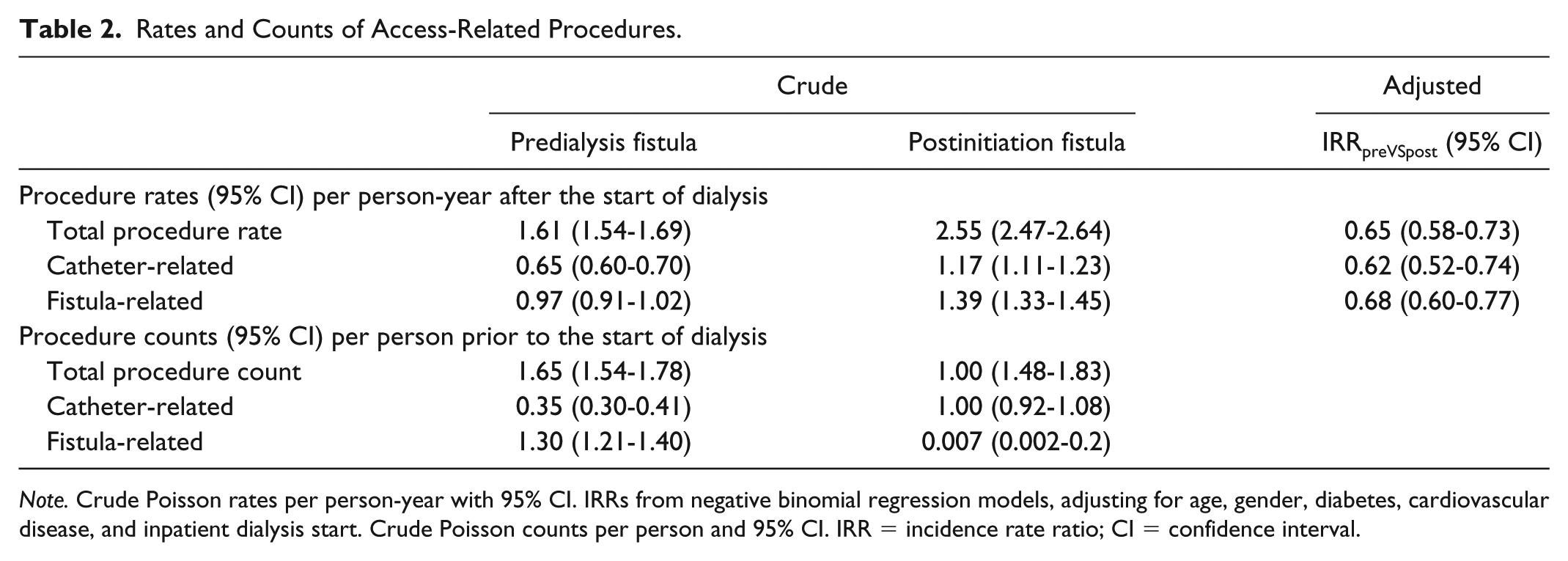
Note. Crude Poisson rates per person-year with 95% CI. IRRs from negative binomial regression models, adjusting for age, gender, diabetes, cardiovascular disease, and inpatient dialysis start. Crude Poisson counts per person and 95% CI. IRR = incidence rate ratio; CI = confidence interval.
Other Analyses
Restricting the cohort to those who initiated dialysis as outpatients or who had 4 months of predialysis care had no significant effect on our findings (ORs remained favorable to the predialysis group). We found no evidence of confounding for BMI, cancer, eGFR at dialysis initiation, starting in an intensive care unit, length of predialysis care, and location of first fistula creation attempt.
Discussion
Patients who received postinitiation fistula attempts had a lower probability of catheter-free use compared with patients who had predialysis fistula attempts. After a postinitiation fistula attempt, patients had a 50% to 54% chance of achieving catheter-free use and spent less than a third of their dialysis time catheter-free. While timing of attempt may be important, the observed differences between these 2 strategies are likely also due to a combination of patient factors and the time required for fistula maturation.
The increased exposure to catheters in those with a postinitiation fistula attempt is likely the result of the delay in fistula creation and inherent differences in patients attempting a fistula prior to dialysis. The additional analyses we conducted clarify this issue to the extent possible. Across time, the likelihood of achieving catheter-free use improved, but remained lower for the post-initiation group by 20% to 30%. Allowing up to 3 months for fistula maturation conservatively increased the proportion of time spent catheter-free, suggesting only some of the overall differences can be attributed to timing of fistula attempt. Restricting the analysis to only those who achieved catheter-free use also improved estimates, suggesting unmeasured patient factors that prevent a fistula from successfully maturing partially explain our findings. When both patient factors and timing were accounted for, the difference in probability of catheter-free use over time was no longer significant, suggesting there may be nothing fundamentally superior about a predialysis attempt. However, we cannot rule out an effect of timing of fistula creation. Counter to expectations, 12 restricting the analyses to those who started dialysis as outpatients or with predialysis care did not reduce the relative difference between the predialysis and postinitiation groups; therefore, our findings were not explained by the different number of urgent starts.
Few research studies have used catheter-free use to measure fistula success. If the main reason to attempt fistula creation is to avoid catheter-related complications, then the proportion of time on dialysis spent without a catheter in place is an important outcome measure. 11 Yet, research in this area remains largely focused on measures such as patency rates, 13 which are arguably less patient-oriented and meaningful than catheter-free days. This study provides unique insight into the burden of catheter use with different fistula creation strategies. Our findings suggest a predialysis attempt is a superior strategy in this regard. However, if a predialysis fistula is not an option (eg, urgent starts), our study describes the limited extent a postinitiation attempt mitigates catheter use. Furthermore, even predialysis fistula creations had a relatively low proportion of time spent catheter-free—about two-thirds of follow-up time. When we restricted our analysis to those who achieved catheter-free use, the groups were more similar. Much of the prior literature supporting fistulas is based on comparing patients with functioning fistulas with patients with other forms of access in place. 4 It appears the outcomes of patients who are able to achieve a functioning fistula are better. Unfortunately, there is a sizable risk that a fistula will never function and we cannot reliably identify patients in whom fistula attempts are more likely to succeed.
Fistulas have been described as having advantages in terms of decreased patient morbidity and increased patient survival rates.2,4 However, the benefits of fistulas over other forms of access have yet to be definitively established in controlled clinical trials. We believe this is a necessary step before firm conclusions can be made. 14 If the superiority of fistulas is confirmed in clinical trials, deciding on the timing of a fistula attempt is still not straightforward. Prior research shows that 20% of patients with predialysis attempts never start dialysis due to death or nonprogression of their kidney disease. 9 Simulated data are conflicting with regard to the effect of timing of fistula creation on life expectancy, and certain populations may benefit from different creation strategies.15,16 The potential benefits of fistulas, including our findings in terms of catheter-free use, should be considered alongside this other information when patients and providers make decisions about the choice of vascular access and timing of access creation.
Our study found relatively high procedure rates, regardless of the timing of fistula creation. Patients have identified hemodialysis access–related complications and procedures as research priorities, 17 as they often experience “unpreparedness” and “insecurity” regarding the complications they will face. 18 Being fully informed may improve patient confidence and their ability to cope. 18 Our findings suggest patients who receive a fistula can expect an average of 2 procedures per year, in addition to procedures prior to starting dialysis (ie, the fistula creation or catheter placement to initiate hemodialysis). An earlier predialysis fistula attempt may further increase the number of procedures a patient experiences before dialysis. 19 A systematic review showed that 40% of fistulas require at least one intervention within their first year, and fistula performance appears to decline over time. 10 This information can help patients set realistic expectations when they choose a particular vascular access strategy.
The primary strengths of our study are the granularity and the quality of the data provided by the DMAR system. Data collection occurred prospectively at 5 large dialysis programs, reflecting diversity in practice, and underwent review to ensure data accuracy. Information such as comorbidities was referenced from a source document for consistent definitions. Detailed information on procedure types, indications, and dates were collected, allowing for a longitudinal picture of the whole course of dialysis therapy.
The primary limitation of our study is its observational design. This limitation impacts any causal inferences drawn from our study (ie, superiority of predialysis fistulas), but not the description of our outcome measures (ie, time spent catheter-free). Selection bias has been shown to influence the causal results of observational studies in this patient population.20,21 There may be differences between the type/course of renal disease, or patient characteristics, such as vessel size, for candidates who undergo a predialysis versus postinitiation fistula attempt that were not accounted for in our study design. The sensitivity and subgroup analyses we conducted attempted to parse out this bias. However, limited follow-up times may have influenced our results in ways not accounted for by the data. In addition, the fact that a smaller proportion of dialysis patients undergo fistula creation in the participating dialysis programs compared with other jurisdictions worldwide may influence the observed results, but this is representative of current Canadian practice and likely represents a more positive view if these centers are more selective when referring patients for a fistula attempt. Certain clinical factors such as fistula maturation were not tracked, and our method of data collection precluded an in-depth investigation into the causes of catheter use (eg, delayed maturation, failed cannulation, or patient wishes). Nonetheless, the quality and the granularity of detail regarding vascular access collected during this time period makes the data uniquely valuable to address certain research questions.
In conclusion, predialysis fistula attempts are associated with a higher probability of catheter-free use and fewer procedures compared with postinitiation attempts, which can likely be attributed to both timing and patient factors. However, catheter use and procedures are still common in both groups. These findings can be used to guide the discussion between patient and provider when selecting an access strategy.
Footnotes
Author Contributions
P.R., R.R.Q., and A.C. contributed to research idea and study design; R.R.Q. and M.J.O. contributed to data acquisition; A.C., P.R., R.R.Q., M.J.O., S.H., L.M., P.B., L.M., A.X.G., and N.N.L. contributed to data analysis/interpretation; A.C. and P.R. contributed to statistical analysis; R.R.Q. and P.R. contributed to supervision or mentorship. Each author contributed important intellectual content during article drafting or revision and accepted accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Ethics Approval and Consent to Participate
Ethics approval was obtained separately at all participating sites.
Consent for Publication
All authors have reviewed a final version of the manuscript and have consented to publication.
Availability of Data and Materials
Data and materials can’t be made publicly available due to restrictions on its disclosure and use.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Oliver and Quinn disclose they are co-inventors of the Dialysis Measurement Analysis and Reporting system.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (CIHR) (funding reference nos. 130514 and 119366, and CIHR application no. 406897). R.R.Q. and P.R. were supported by CIHR, the Ashford Foundation for Medical Research, and Medical Services Incorporated. N.N.L was supported by a KRESCENT New Investigator Award. A.X.G. was supported by a CIHR Clinician Investigator Award and the Dr Adam Linton Chair in Kidney Health Analytics. The funders had no role in the study design; collection, analysis, and interpretation of the data; writing of the report; and the decision to submit the report for publication were independent from the funding sources.