
Abstract
Background:
Unplanned dialysis initiation is common in patients with chronic kidney disease (CKD).
Objective:
To determine common definitions and patient risk factors for unplanned dialysis.
Design:
Systematic review.
Setting:
MEDLINE, EMBASE, and the Cochrane Library were searched from inception to February 2018.
Patients:
Studies that included incident chronic dialysis patients or patients with CKD that cited a definition or examined risk factors for unplanned dialysis were included.
Measurements:
Definitions and criteria for unplanned dialysis reported across studies. Patient characteristics associated with unplanned dialysis.
Methods:
Two reviewers independently extracted data using a standardized data abstraction form and assessed study quality using a modified New Castle Ottawa Scale.
Results:
From 2797 citations, 48 met eligibility criteria. Reported definitions for unplanned dialysis were variable. Most publications cited dialysis initiation under emergency conditions and/or with a central venous catheter. The association of patient characteristics with unplanned dialysis was reported in 26 studies, 18 were retrospective and 21 included incident dialysis patients. The most common risk factors in univariate analyses were (number of studies) increased age (n = 7), cause of kidney disease (n = 6), presence of cardiovascular disease (n = 7), lower serum hemoglobin (n = 9), lower serum albumin (n = 10), higher serum phosphate (n = 6), higher serum creatinine or lower estimated glomerular filtration rate (eGFR) at dialysis initiation (n = 7), late referral (n = 5), lack of dialysis education (n = 6), and lack of follow-up in a predialysis clinic prior to dialysis initiation (n = 5). A minority of studies performed multivariable analyses (n = 10); the most common risk factors were increased age (n = 4), increased comorbidity score (n = 3), late referral (n = 5), and lower eGFR at dialysis initiation (n = 3).
Limitations:
Comparison of results across studies was limited by inconsistent definitions for unplanned dialysis. High-quality data on patient risk factors for unplanned dialysis are lacking.
Conclusions:
Well-designed prospective studies to determine modifiable risk factors are needed. The lack of a consensus definition for unplanned dialysis makes research and quality improvement initiatives in this area more challenging.
What was known before
Unplanned dialysis initiation is common in patients with chronic kidney disease. Determining patient risk factors for this important outcome may help reduce the incidence.
What this adds
High-quality data on patient risk factors for unplanned dialysis are lacking. Well-designed prospective studies to determine modifiable risk factors are needed.
Introduction
Many patients with chronic kidney disease (CKD) start dialysis in an unplanned fashion and/or under urgent circumstances despite regular follow-up by a nephrologist. Most studies report a prevalence of unplanned dialysis between 40% and 60%.1-7 However, the prevalence varies, likely in large part due to inconsistent definitions across studies. An unplanned dialysis start is defined by varying criteria that may include dialysis initiation with a central venous catheter (CVC) as opposed to a permanent access (arteriovenous fistula, arteriovenous graft, or peritoneal dialysis catheter), and/or dialysis initiation during an acute hospitalization, and/or dialysis initiation under emergent circumstances. 7 Unfortunately, there is no established consensus definition.
Unplanned dialysis is of concern because, theoretically, patients forego the opportunity to make an informed, shared decision with respect to timing and modality of renal replacement therapy (RRT). Instead, most centers in North America only offer one option for RRT under urgent conditions: hemodialysis with a CVC. In addition, unplanned dialysis is associated with increased patient morbidity and mortality and added health care costs.4,6-9 Given the high prevalence of unplanned dialysis and association with poor patient outcomes, we conducted a systematic review to determine patient risk factors for this outcome. As a secondary objective, we determined the most common criteria and terminology used to define the outcome. The results of this systematic review should help to inform future studies aimed at reducing the burden of unplanned dialysis starts.
Materials and Methods
Search Strategy
We performed a comprehensive, systematic search of articles published in peer-reviewed journals using MEDLINE, EMBASE, and the Cochrane Library (from inception to February 28, 2018). The search was carried out with the assistance of a librarian experienced in systematic reviews. We used a structured search strategy (outlined in Supplementary Appendix A), based on controlled vocabulary and relevant key terms that were broad to prioritize sensitivity. The references of included articles and existing reviews were scanned for additional studies. There were no restrictions based on study design or language in the search.
Study Selection
There were 2 independent investigators (A.O.M. and A.A.) who screened identified titles and abstracts. Those deemed to be clearly irrelevant were removed on the initial screen. If no abstract was available, the full text was obtained unless the article could be confidently excluded by title alone. Full-text versions of potentially eligible studies were obtained and independently screened by 2 reviewers (A.O.M. and R.H. or A.A.) to determine their eligibility based on the selection criteria. Any disagreements during the screening process were resolved through discussion among the authors in accordance with the selection criteria.
We included retrospective and prospective studies that reported criteria to define unplanned dialysis or characteristics of patients who had an unplanned versus planned dialysis start. We excluded non-English articles, studies published only in abstract form, case reports, narrative reviews, editorials, letters, practice guidelines, and pediatric studies. We excluded studies that focused primarily on late referral to nephrology.
Data Extraction and Synthesis
Two independent investigators (A.O.M. and R.H.) abstracted data using a standardized data abstraction form (see Supplementary Appendix B). The following data were abstracted: study methods, patient characteristics, criteria and terminology used to define unplanned dialysis, and patient characteristics by unplanned versus planned dialysis status. Patient characteristics significantly associated with unplanned dialysis were summarized, along with covariates included in multivariable models to identify independent associations. Statistical significance within studies was defined by individual study methods. Two investigators (A.O.M. and R.H.) independently performed a quality assessment for studies that reported patient characteristics associated with unplanned dialysis. A modified Newcastle-Ottawa Scale (NOS) was used to assess the quality of applicable observational studies. 10 A score was given for the NOS domains of cohort selection and comparability (maximum scores of 4 and 2, respectively). The outcome domain was removed from the NOS, as we did not examine outcomes associated with unplanned dialysis. The reporting of this systematic review is in accordance with PRISMA guidelines (refer to Supplementary Appendix C for details). 11 The methods were all prespecified, and the review protocol was registered with the international prospective register of systematic reviews (http://www.crd.york.ac.uk/PROSPERO; registration no. CRD42016032916). 12
Results
Eligible Studies
Study selection is outlined in Figure 1. The electronic database search identified 2843 records and one further record was identified from other sources. There were 2798 nonduplicate citations. After independently reviewing the title and abstract of all potentially relevant records, 407 articles were retrieved and reviewed in full text. Of these articles, 48 studies were found to meet inclusion criteria.
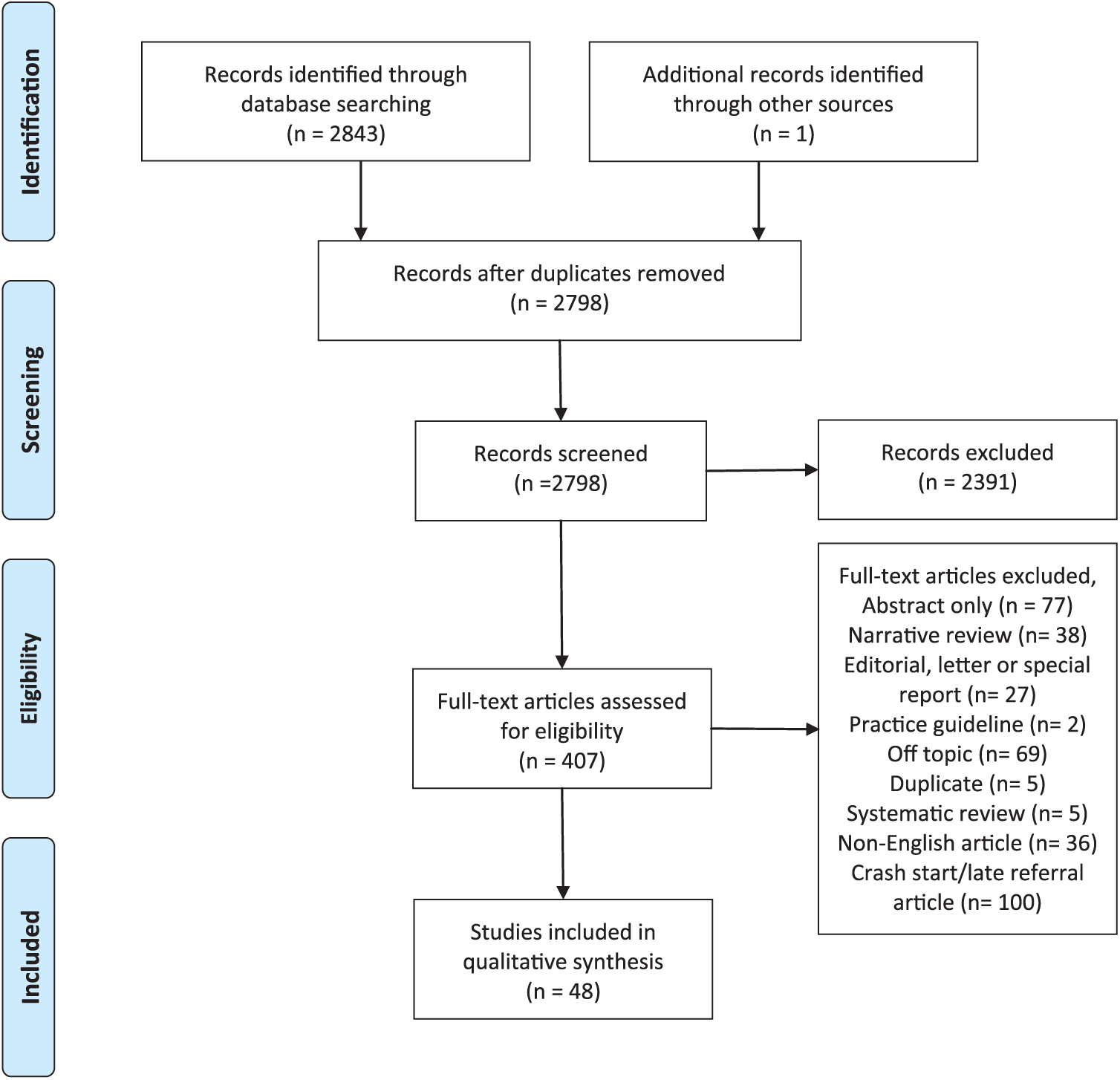
Study selection.
Patient and Study Characteristics
The characteristics of the 48 eligible studies are outlined in Table 1. Eligible studies included incident chronic dialysis patients (n = 42)2-4,6,8,9,13-48 and patients with CKD known to nephrology (n = 6).5,49-53 Study designs included retrospective cohort studies (n = 27),2,3,5,6,14-16,19-24,26,28,31-36,38,47-50,53 cross-sectional studies (n = 2),9,52 prospective cohort studies (n = 17),4,8,17,18,25,27,29,30,37,39-45,51 retrospective before/after studies (n = 1), 46 and unclear design (n = 1). 13 No randomized control trials were found in the search. The majority of studies were conducted in Europe (n = 26; 22 unique cohorts)2,8,9,15-19,22-25,29,30,33,36,40-43,45-48,50,51; 11 studies were conducted in North America3-6,14,21,26,28,31,52,53 (Canada, n = 9; 8 unique cohorts). Study cohort sizes ranged from 43 to 45 785 persons.
Study Characteristics.

Note. RCS = retrospective cohort study; CKD = chronic kidney disease; PCS = prospective cohort study; ESRD = end-stage renal disease; AKI = acute kidney injury; RRT = renal replacement therapy; CrCl = creatinine clearance; HD = hemodialysis; ICU = intensive care unit; CVC = central venous catheter; eGFR = estimated glomerular filtration rate; PD = peritoneal dialysis.
Median age (range).
Patients with type 2 diabetes.
Patients with type 1 diabetes.
Median age (interquartile range).
Mean age (range).
Planned dialysis initiation.
Unplanned dialysis initiation.
Mean age (95% confidence interval).
Terms and Definitions for Unplanned Dialysis
The terminology used to describe an unplanned dialysis start was variable across studies (Table 1). Examples of terminology included unplanned dialysis, urgent dialysis, unscheduled dialysis, and suboptimal dialysis start. Varying criteria were used to define unplanned dialysis; however, all definitions included some consideration of the conditions under which dialysis was started (ie, during a hospitalization or emergently) and/or the access that was used at dialysis initiation (ie, a CVC) (Table 1, Figure 2). The proportion of patients with an unplanned dialysis start differed across studies, ranging from 7% to 100%, but most studies reported a proportion between 40% and 60% (n = 21).2,3,5,6,14,15,19,23,24,26-31,36,38,48,51-53

Definitions for unplanned dialysis among included studies (N = 48).
Patient Risk Factors for Unplanned Dialysis
There were 26 studies (25 unique cohorts) that reported the association of patient characteristics with unplanned dialysis, 21 of which included incident chronic dialysis patients (retrospective cohort study, n = 15; cross-sectional study, n = 1; prospective cohort study, n = 5),2-4,6,8,9,15,19,21-28,31,34,38,39,48 and 5 of which included patients with CKD known to nephrology (retrospective cohort study, n = 3; cross-sectional study, n = 1; prospective cohort study, n = 1)5,49,51-53 (Table 1). Determining patient risk factors for unplanned dialysis was listed as an objective in 12 studies; all of these studies were retrospective or included incident dialysis patients.2-5,19,21,23,24,26,39,48,53
There were 24 studies that reported patient characteristics by unplanned versus planned dialysis status using descriptive, univariate analysis.2-6,8,9,15,19,21-28,34,38,39,48,51-53 Supplementary Table 1 summarizes the characteristics reported across studies and whether the characteristic significantly differed, based on a P value <.05, between patients with an unplanned versus planned dialysis start. All characteristics significantly associated with unplanned dialysis (P < .05) in univariate analysis are summarized in Table 2. The most common risk factors in univariate analysis were (number of studies) increased age (n = 7),3,5,6,24,25,28,38 cause of kidney disease (n = 6),3,5,23,24,48,53 congestive heart failure (n = 5),3,5,9,39,53 cardiovascular disease (n = 7),3-6,9,28,53 lower serum hemoglobin (n = 9),2,3,6,9,15,23,24,27,39 lower serum albumin (n = 10),2,3,6,15,23-25,39,48,53 lower serum calcium (n = 5),6,15,23,24,48 higher serum phosphate (n = 6),2,6,15,24,39,48 higher serum creatinine or lower eGFR/creatinine clearance at dialysis initiation (n = 7),2,6,15,23-25,48 late referral to a nephrologist (n = 6),3-5,27,28,52 lack of dialysis education (n = 6),2,23,24,39,48,53 and not followed in a dedicated predialysis clinic prior to dialysis initiation (n = 5).2,15,24,26,38 There was one study that reported a higher eGFR and lower serum creatinine in patients with an unplanned dialysis start. 53 For cause of kidney disease, polycystic kidney disease, all genetic kidney disease, and glomerulonephritis were less common in patients with an unplanned start.3,15,24,53 Nephrosclerosis, renal artery stenosis, and diabetic nephropathy were more common in patients with an unplanned start.3,5,53
Characteristics Significantly Associated With Unplanned Dialysis in Univariate Analysis.

Note. BMI = body mass index; COPD = chronic obstructive pulmonary disease; CrCl = creatinine clearance; eGFR = estimated glomerular filtration rate; RRT = renal replacement therapy.
Markers indicate statistically significant associations with unplanned dialysis (P < .05).
Study included hospitalized incident chronic dialysis patients ≥70 years with a predialysis CrCl <15 mL/min or creatinine >600 μmol.
Study included patients on home hemodialysis.
Study included patients ≥85 years initiating hemodialysis.
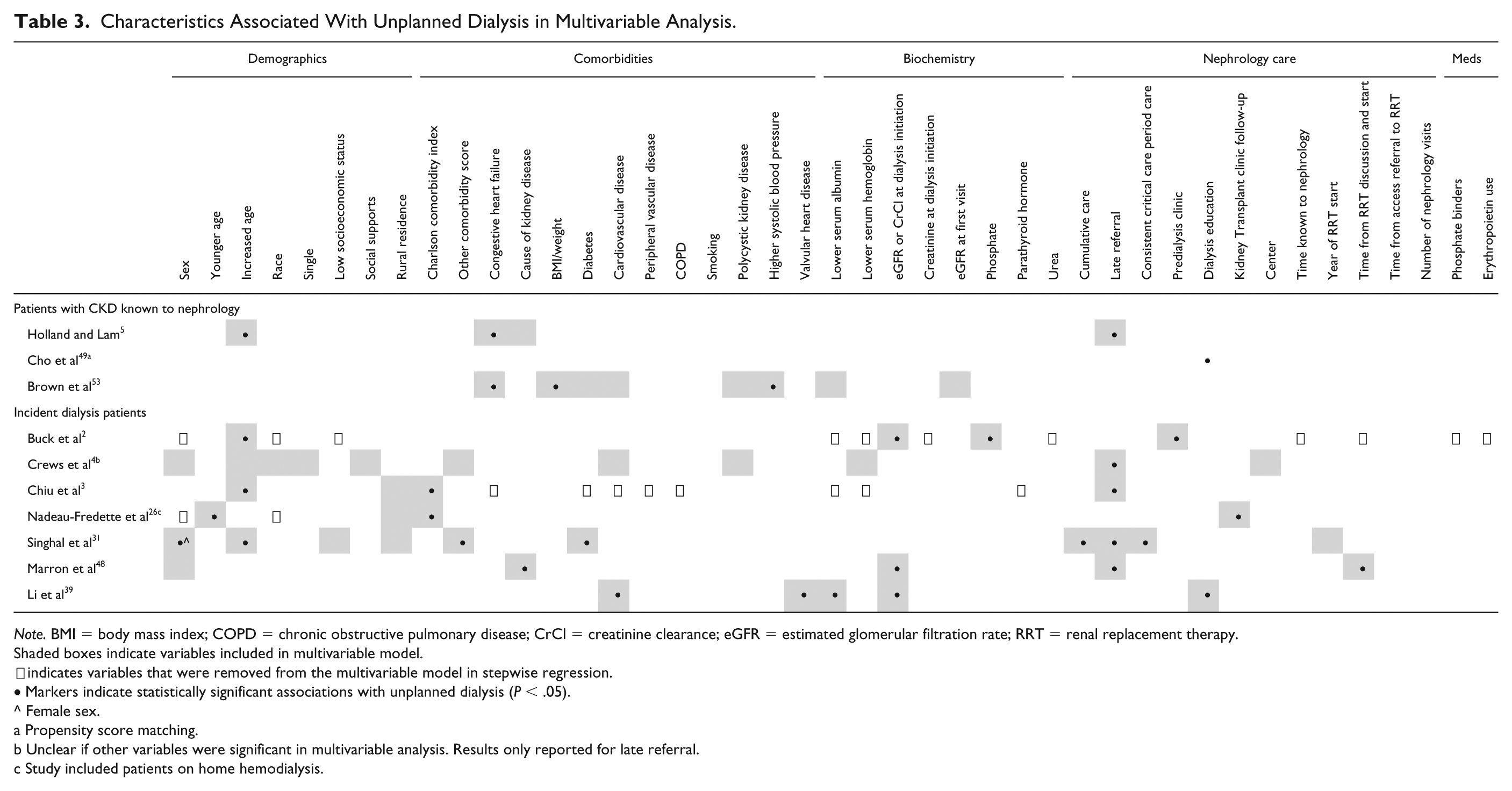
There were 10 studies that used multivariable analysis or propensity matching to examine the association of patient characteristics with unplanned dialysis.2-5,26,31,39,48,49,53 All patient characteristics significantly associated with unplanned dialysis in multivariable or matched analyses (P < .05) are summarized in Table 3. The most commonly reported risk factors were increased age (n = 4),2,3,5,31 increased comorbidity score (n = 3),3,26,31 late referral to nephrology (n = 5),3-5,31,48 and lower eGFR at dialysis initiation (n = 3).2,39,48 Less cumulative nephrology care and less care during the period shortly prior to dialysis initiation (critical period) were significant in adjusted analyses (n = 1), as were other potential markers of quality of care (care in a predialysis clinic [n = 1] and dialysis education [n = 1]).2,31,49
Characteristics Associated With Unplanned Dialysis in Multivariable Analysis.
Note. BMI = body mass index; COPD = chronic obstructive pulmonary disease; CrCl = creatinine clearance; eGFR = estimated glomerular filtration rate; RRT = renal replacement therapy.
Shaded boxes indicate variables included in multivariable model.
indicates variables that were removed from the multivariable model in stepwise regression.
Markers indicate statistically significant associations with unplanned dialysis (P < .05).
Female sex.
Propensity score matching.
Unclear if other variables were significant in multivariable analysis. Results only reported for late referral.
Study included patients on home hemodialysis.
Hughes et al 21 examined potential underlying causes for unplanned dialysis in patients referred to a nephrologist >12 months prior to dialysis initiation and found the following causes of unplanned dialysis: patient-related delays (31%), acute on chronic kidney injury (31%), surgical delays (16%), late decision-making by the nephrologist (8.6%), and other (12.5%). Marron et al 48 also examined reasons for unplanned dialysis and found a similar result, despite being conducted in another country: patient-related delays (36%), acute on chronic kidney injury or more rapid decline in eGFR than anticipated (28%), health care bureaucracy issues (11%).
Assessment of Study Quality
Study quality was assessed for the 26 studies that reported patient characteristics and their association with unplanned dialysis.2-6,8,9,15,19,21-28,31,34,38,39,48,49,51-53 One of the 26 studies was a secondary analysis of the Mendelssohn et al study. 28 Study quality reported using a modified NOS is summarized in Supplementary Table 2. Only one study was awarded all 4 possible points for cohort selection. Unfortunately, this study was not primarily designed to examine risk factors for unplanned dialysis. 51 Most studies lost a point for cohort selection because they were retrospective or included incident dialysis patients. The studies by Nadeau-Fredette et al, 26 Kanno et al, 38 and Loos et al 9 lost 2 points for cohort selection because they only included home hemodialysis and very elderly patients, which are both a select group of patients. There were 16 studies that received 0 points for comparability because the study design or analysis did not address potential confounding, meaning that no form of statistical adjustment or matching was performed.6,8,9,15,19,21-25,27,28,34,38,51,52
Discussion
This systematic review of literature published until February 2018 includes 48 studies that outlined criteria for unplanned dialysis, of which 26 studies reported patient characteristics associated with unplanned dialysis, and 10 studies adjusted for covariates in multivariable models to identify independent associations. Increased age, increased comorbidity burden, late referral to nephrology, and lower eGFR at dialysis initiation were the most common independent risk factors for unplanned dialysis. The published literature is limited by the retrospective, cross-sectional, and often unadjusted, confounded nature of the data, along with varying terminology and criteria used to define unplanned dialysis across studies.
In univariate, unadjusted analyses, a lower hemoglobin, lower serum albumin, higher serum phosphate, lower serum calcium, and lower eGFR at dialysis initiation were often more common in patients with unplanned dialysis starts. However, these characteristics were often not examined in adjusted analyses or did not always persist as risk factors in multivariable analysis.2,3,6,15,23,24 The independent association of factors such as lower hemoglobin, calcium, or higher phosphate with unplanned dialysis is questionable, given that these characteristics may be surrogate markers for poor predialysis care or patient nonadherence, and were only measured once at dialysis initiation. Lower eGFR at dialysis initiation could be due to late referral, a higher rate of eGFR decline, or patient, physician, or system-related delays with respect to RRT preparation. The retrospective nature of the data makes it difficult to comment on the underlying reasons for observed associations.
Increased age was an independent risk factor in 4 studies following adjustment for comorbidity burden and late referral.2,3,5,31 This could be due to physician-related factors; nephrologists may delay discussions about dialysis with elderly patients due to the uncertainty of meaningful survival and quality of life benefits and the high competing risk of death.54-60 As well, the benefits of arteriovenous fistulas in elderly patients are uncertain; therefore, nephrologists may decide that initiation of hemodialysis with a CVC, if needed, is entirely appropriate.61-63 For these reasons, labeling all dialysis starts with a CVC as unplanned is contentious. Increased age may be associated with unplanned dialysis primarily due to increased “planned” CVC use, but studies that included access criteria in the definition for unplanned dialysis did not differentiate between CVC insertions under planned, stable conditions in the outpatient setting versus urgent conditions during a hospitalization.2,3 Differentiating between planned, elective and urgent, unplanned CVC insertions could help to better delineate the association between age and unplanned dialysis. Another potential contributor to the association between increased age and unplanned dialysis could be that elderly patients are at increased risk for acute illnesses and acute kidney injury. 64
The study by Nadeau-Fredette et al 26 included only home hemodialysis patients and was the only study that reported younger age as an independent risk factor for unplanned dialysis. This discrepant result is likely due to the fact that home hemodialysis patients are not representative of the general dialysis population. The study by Nadeau-Fredette et al 26 also reported that patients with a failed transplant were more likely to have an unplanned dialysis start. This was not examined in other studies but is an interesting finding that suggests an important care gap in preparing patients with a failing transplant for dialysis. Increased comorbidity burden and congestive heart failure were reported as independent risk factors in three3,26,31 and two5,53 studies, respectively. This suggests that patients with multiple medical issues, poor cardiac function, and issues with volume overload may require RRT planning at higher levels of kidney function and closer follow-up. Late referral to nephrology was an independent risk factor in 5 studies.3-5,31,48 The definition of late referral varied in these studies from less than 3 months 48 to less than 12 months. 3 This finding supports the complexity of optimal RRT preparation, which may be underappreciated by both patients and physicians. Several studies found that follow-up in a dedicated predialysis clinic and the receipt of dialysis education were less common in patients with an unplanned dialysis start.2,15,23,24,26,38,39,48,49,53 These findings were mostly reported in univariate analysis, but suggest that specialized care and education can facilitate the difficult transition onto dialysis. The finding of diabetic nephropathy and nephrosclerosis being more common than genetic kidney disease or glomerulonephritis in patients with unplanned dialysis starts was mostly reported in univariate analyses and may be explained by the fact that patients with diabetic nephropathy and nephrosclerosis tend to be older and have more comorbidities.
A prior systematic review examined outcomes and costs associated with unplanned dialysis and included literature up to 2008. This previously published review by Mendelssohn et al 7 included 8 European studies and found that unplanned dialysis was associated with increased morbidity and mortality, along with significant health care costs. Our review includes the 8 studies from the Mendelssohn et al review, along with 40 further studies, and is the first systematic review to summarize the published evidence on risk factors for unplanned dialysis.
Our review benefits from a comprehensive, broad search strategy with all methods clearly defined and prespecified. However, the conclusions of our review are limited for several reasons. Only 12 studies actually specified the determination of risk factors for unplanned dialysis as a study objective and none of these studies had prospective follow-up of patients with CKD.2-5,19,21,23,24,26,39,48,53 Due to the retrospective or cross-sectional nature of the published data, results are largely limited to one-time data collection at dialysis initiation and data collected as part of routine clinical care. As well, many studies did not perform adjusted or matched analyses. The variable terminology and criteria used to define unplanned dialysis makes comparisons across studies difficult. Some studies focused solely on dialysis initiations during a hospitalization or under acute circumstances while other studies also included dialysis initiations with a CVC in their definition of unplanned dialysis. As well, not all studies that included incident dialysis patients specified the exclusion of patients with AKI (without prior CKD) requiring dialysis (Table 1). Such patients would obviously require inpatient/urgent dialysis with a CVC but are not of interest when considering the issue of risk factors for planned versus unplanned dialysis. Finally, some studies were conducted more than 10 years ago, and practice patterns with respect to predialysis care and dialysis initiation have changed. In particular, national guidelines have adopted a delayed approach to dialysis initiation, largely based on the results of the Initiating Dialysis Early and Late (IDEAL) Trial.65-67 There may also be regional or country-specific practice patterns and patient population differences that are not fully captured by the published data, ie, there are very little data from the United States published on this topic. 4
Conclusions
High-quality data on patient risk factors for unplanned dialysis are lacking. As a first step toward reducing the incidence of unplanned dialysis starts, well-designed studies to determine modifiable risk factors are needed. Potential modifiable factors could include the timing of RRT education and factors that impact patient adherence and decision-making. The lack of a consensus definition for unplanned dialysis makes research and quality improvement initiatives in this area more challenging.
Supplemental Material
Supplementary_Tables_and_appendix_A,_B,_C_final_CJKHD – Supplemental material for Risk Factors for Unplanned Dialysis Initiation: A Systematic Review of the Literature
Supplemental material, Supplementary_Tables_and_appendix_A,_B,_C_final_CJKHD for Risk Factors for Unplanned Dialysis Initiation: A Systematic Review of the Literature by Rana Hassan, Ayub Akbari, Pierre A. Brown, Swapnil Hiremath, K. Scott Brimble and Amber O. Molnar in Canadian Journal of Kidney Health and Disease
Footnotes
Author Contributions
A.O.M., S.H., and A.A. contributed to conception and design of the study; A.O.M., S.H., A.A., K.S.B., and P.A.B. provided intellectual content of critical importance to the work described; A.O.M. and R.H. interpreted the data; R.H. and A.O.M. drafted the first version of the article and revisions; all authors read and approved the final version of the article.
Availability of Data and Materials
This study is a systematic review of previously published data and materials.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.S.B. reports the receipt of personal fees from the Ontario Renal Network unrelated to this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Amber O. Molnar receives salary support from the KRESCENT Foundation and the McMaster Department of Medicine. The funders had no role in the study or in the writing of this report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.