
Abstract
Background:
Patients with chronic kidney disease (CKD) are asked to choose a renal replacement therapy or conservative management. Education and knowledge transfer play key roles in this decision-making process, yet they remain a partially met need.
Objective:
We sought to understand the dialysis modality decision-making process through exploration of the predialysis patient experience to better inform the educational process.
Design:
Qualitative descriptive study.
Setting:
Kidney Care Centre of London Health Sciences Centre in London, Ontario, Canada.
Patients:
Twelve patients with CKD, with 4 patients on in-center hemodialysis, home hemodialysis, and peritoneal dialysis, respectively.
Measurements:
Not applicable.
Methods:
We conducted semistructured interviews with each participant, along with any family members who were present. Interviews were transcribed verbatim. Conventional content analysis was used to analyze the transcripts for common themes. Representative quotes were decided via team consensus. A patient collaborator was part of the research team.
Results:
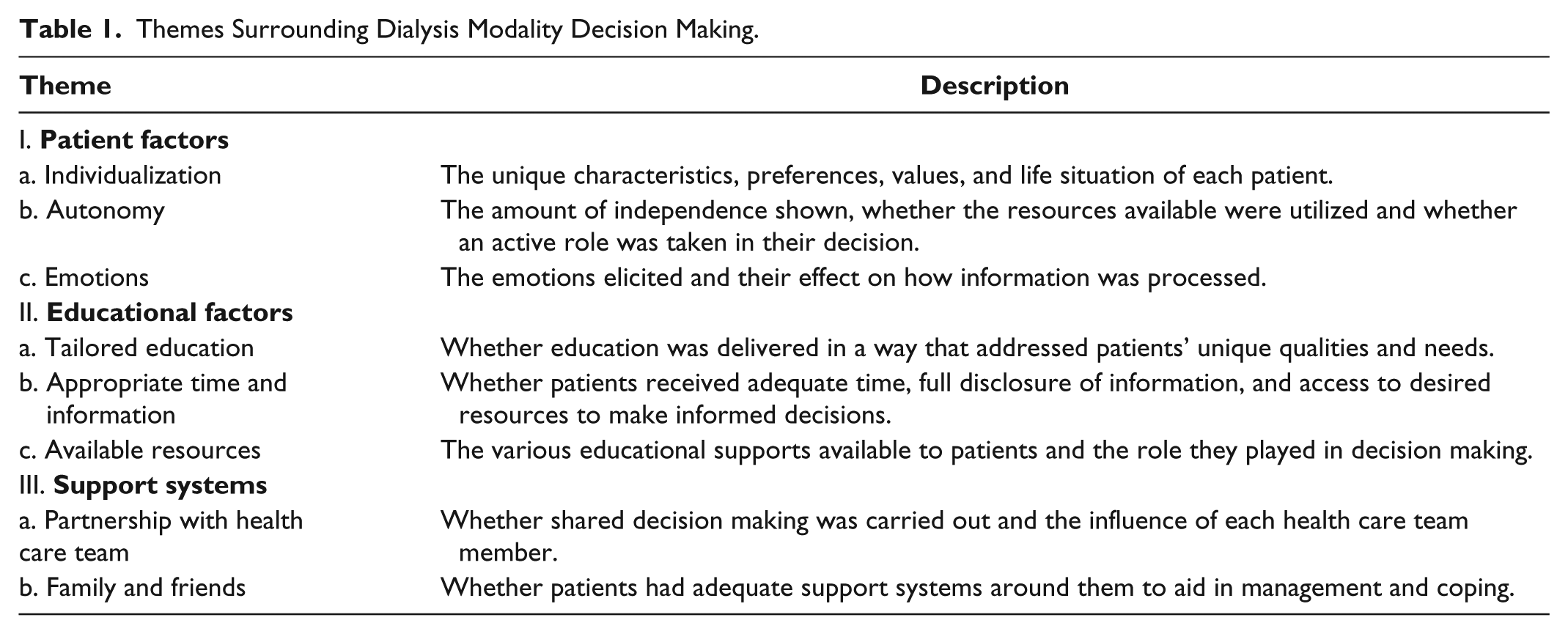
Three themes influenced dialysis modality decision making: (i) Patient Factors: individualization, autonomy, and emotions; (ii) Educational Factors: tailored education, time and preparation, and available resources; and (iii) Support Systems: partnership with health care team, and family and friends.
Limitations:
Sample not representative of wider CKD population. Limited number of eligible patients. Poor recall may affect findings.
Conclusions:
Modality decision making is a complex process, influenced by the patient’s health literacy, willingness to accept information, predialysis lifestyle, support systems, and values. Patient education requires the flexibility to individualize the delivery of a standardized CKD curriculum in partnership with a patient-health care team, to fulfill the goal of informed, shared decision making.
What was known before
There are barriers to effective education at the patient, provider, and systemic levels. Patient engagement is optimized when education is tailored on an individual level. Patients attempt to maintain their predialysis quality of life when they make treatment decisions.
What this adds
Three elements that influence patient decision making are patient factors (individual values and life situations, amount of autonomy and emotions elicited), educational factors (tailored information, an appropriate amount of time and information and the resources available and utilized), and support systems (relationship with the health care team and the aid of family and friends). These elements must be navigated by health care professionals to optimize informed, shared decision making.
Introduction
Patient decision making is informed by the treatment’s risks and benefits and impact on quality of life. When decisions are not aligned with patient values, patients are less motivated to follow treatment, experience decisional conflict and regret and place blame on clinicians.1,2 Patients with chronic kidney disease (CKD) must decide between transplantation, in-center hemodialysis (IC-HD), home hemodialysis (Home-HD), peritoneal dialysis (PD), or conservative management. Patient characteristics and values, including autonomy, adaptability, and willingness to accept information are known to influence decision making.3-5
Patients evaluating the CKD educational and decision-making process identify a lack of understanding of differences in modality options and disclosure of the burden of dialysis.6-12 Patient-related challenges include limited health literacy, cognitive decline, depression, comorbidities, and cultural differences.1,7,13 This provided a rationale to include an evaluation of health literacy in our participants, to deepen our understanding of their treatment decisions. Provider challenges include time and resource constraints, inadequate interdisciplinary care models, and lack of awareness of the patient-related challenges.1,2,13-16 There has been some success in early CKD education, utilizing decision aids and engaging in shared decision making.2,10,14 Several studies have explored the predialysis period with an intention to understand patient decision-making, and common themes have emerged including the need to maintain quality of life, the importance of individualization, adequate information, and whether support systems were in place to effectively cope with the illness experience.3,12,17-20 While it is known that education plays a large role in modality decision making, we identified a perceived gap in the educational needs of patients and the corresponding predialysis education programs, with evidence that patients often have a diminished or simplified view of their options.12,21,22 Knowledge of these experiences will inform knowledge transfer and patient-informed decision making.
We conducted 12 in-depth, semistructured interviews with patients who initiated dialysis within 6 months of the interview, to deepen the understanding of the factors that result in patient-informed treatment decisions through the exploration of patient experiences. We explored participants’ satisfaction with the education they received, while identifying educational needs, and the influence of the educational process in their dialysis modality decision making within the broader context of the predialysis experience. While the alternative of conservative management was screened for, these decisions were not explored in depth. 23
Materials and Methods
A qualitative descriptive study was conducted with a sample of 12 participants between August-September 2016. 24 Eligible participants were patients with CKD on either IC-HD, PD, or Home-HD who started dialysis within 6 months of the study and were >18 years of age, fluent in English, and able to participate in an open-ended interview. The sample was derived from the Kidney Care Centre in London, Canada, with approximately 300 patients on dialysis. The study was approved by the Western University Health Science Research Ethics Board (HSREB# 108223). CKD education was provided by the multidisciplinary team. Educational supports included the Kidney Foundation of Canada binder, Living With Kidney Disease, 4th edition, 4 multimodal small group classes, patient partners, and a list of trusted CKD online resources. 25 The 4 classes covered self-management, living with CKD, stages of change, videos and demonstrations of each dialysis modality, a patient panel, vascular access, and a tour of the dialysis unit.
Twenty-six eligible participants were identified by the dialysis nurse case manager, with 16 screened by B.P.C. by convenience with a Letter of Information, and 4 refusing to participate. Four patients from each dialysis modality provided verbal and written consent and were interviewed, along with any family members present. One participant had been on dialysis slightly longer than 6 months at the time of interview, however was included due to the time limit of the study and we did not believe it would impact recall significantly. Sample size was determined utilizing the principal of theoretical saturation. 26 An interview guide was created based on patient themes previously identified, exploring how patients receive information, its influence on their decisions, and how the current educational supports could be improved.9,11,27 All interviews were conducted by B.P.C., who had no role in patient care. Patients completed a demographic survey, including a 3-Item Brief Health Literacy Screen (BHLS) scored on a 5-point Likert scale 28 (Online Appendix). Scores of 3 to 9 indicate lower subjective health literacy and scores of 10 to 15 indicate higher subjective health literacy.29,30 A 30- to 60-minute semistructured interview using the AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You) protocol was conducted with patients/family members. 31 Family members were able to be active participants with their responses included in the analysis unless there was discrepancy between their response and the participant’s. Interviews were audio-recorded and transcribed verbatim. Two reviewers (B.P.C. and L.H.) analyzed the transcripts independently, using conventional content analysis. 32 Keywords, phrases, and descriptions were analyzed and categorized into themes. Quotes were extracted to best represent the patient voice and were matched to themes through team consensus.
In line with Canada’s Strategy for Patient-Oriented Research (SPOR), 1 patient on dialysis was part of the research team. M.S., a patient collaborator, reviewed the protocol, interview script, analysis process, and manuscript. An independent analyst (L.E.G.) with expertise in patient experiences, and M.S., deemed our analysis and themes credible through peer debriefing. 32
Results
The demographic survey revealed 7 male participants and 5 female participants, with 75% self-identifying as Caucasian, and an age range of 23 to 77 years, with a median age of 62 years. The highest levels of education attained included high school (33%), college (50%), and postgraduate degree (17%), with participants scoring between 8 and 15, with a mean of 12.67/15 on the 3-Item BHLS. Three overarching themes influenced the modality decision-making process: (1) Patient Factors (individualization, autonomy, and emotions), (2) Educational Factors (tailored education, appropriate time/information, and available resources), and (3) Support Systems (partnership with health care team (HCT) and family/friends). Table 1 describes the subthemes and the meaning of the content.
Themes Surrounding Dialysis Modality Decision Making.
Patient Factors
Patients identified the need for HCTs to consider them an expert on their values and needs in modality decision making.
Individualization
Individual circumstances including transportation, level of activity, living situation, and support systems were at the core of many modality decisions.
The fact that I live by myself and I am really not medically inclined at all, made me choose [IC-HD] . . . I just didn’t feel comfortable to be able to do it by myself at home. If I had a partner, it would have been different . . . I think I would have gone for the peritoneal
To consider a home modality, patients perceived themselves as self-sufficient, had support available, and/or preferred a modality that fit with their life situation. One patient chose home-HD because “. . . my lifestyle, I am very independent and really didn’t want to be tied to a clinic.”
Autonomy
Patients possessed varying levels of independence, ability and willingness to engage, and preferred different quantities of information. Some patients relied on their HCT to make treatment decisions, while others made their own decisions.
. . . the more information you have, it is important. Even though the doctors are helping you, if you don’t help yourself you are not going to go anywhere.
On the contrary, one patient downplayed the information stating, “I think people really make decisions on a gut basis more than a lot of information.”
Emotions
Patients without adequate understanding of their current health state experienced fear, denial, regret, anger, and shock. This patient started dialysis emergently, after a long history of diabetes: I never had any problem in my life, my health very good you know? I am eating good, and then hear “by the way you have kidney problem” . . . I was really mad . . . I start in the dialysis unit. Every day I cry like 3 hours a day . . .
Another patient felt misled as to the immediacy of dialysis, as explained by their family member: . . . they told us it could be a couple months [until PD] and then it was . . . like 3 weeks. So when I got the call . . . I kinda wanted to cry too because it was like, boom! . . . It was kind of a shock.
This lead to the patient feeling regret as they had initially wished to pursue “natural ways”. Emotions influenced decision making and impacted patients’ processing of information.
I didn’t want to know certain things. I just knew I had to have dialysis and that was enough for me.
Educational Factors
The content and format of education delivered to patients influenced decision making, with individual patient factors impacting the effectiveness of the educational support.
Tailored education
Patients tended to receive information more effectively, with active engagement and motivation to learn when provided in accordance with their preferred learning styles.
They gave him a [KFoC Binder] and it was like, really a 23-year-old doesn’t really want to sit and read a big book. I mean, us as adults don’t like to either.
Demographic and generational variance was apparent in the way certain participants wished to receive information.
Quite a few people don’t know how to use a computer. There are older people or people who have eyes issues . . . I want to get all the information about kidney, but I personally wouldn’t just buy a computer.
Patients’ requests to improve the current educational support included more face-to-face education from clinicians and patients, videos on dialysis, online educational classes, and written information via pamphlets. Available resources were not always apparent to the patients: “I like the idea of a patient partner, that would have been really cool.”
Appropriate time and information
Providing time and repeated exposure to information enhanced patient-informed decision making.
. . . we were really well equipped by the time we got home and on our own that we were really quite confident and quite capable of doing [Home-HD] ourselves.
The appropriate amount of time differs among patients. When not given enough time, patients felt rushed, barraged with information, and overwhelmed.
Well, it was just that I had to make a decision and it was like somebody was tapping their foot saying, “you’ve got to make a decision now.”
Patients also reported feeling they did not receive balanced information in terms of both the benefits and drawbacks of each modality and desired a more pragmatic approach.
Basically it boils down to that they don’t want to scare the patients . . . I have had doctors tell me one thing and because I have been through it, I knew they were trying to fluff it up so you wouldn’t feel bad . . . the patient’s not making an informed decision. They are only hearing one side of it.
One patient had 2 clinicians providing information, one presenting options in a hopeful manner, while the other was more realistic about life on dialysis. The patient preferred the latter approach: Well, because I think as an autonomous person, I should have all the information and not just the rose-colored glasses information . . .
Available resources
Educational supports utilized by patients had a significant impact on their perception of each modality. However, not all resources were accessed, even when offered. The resources used by patients are highlighted in Table 2. The multidisciplinary teams were influential in supporting patients through the predialysis period and in dialysis modality choice. Patients benefited from group learning and the shared patient experiences and perceptions.
Well, I think the classes here . . . really sharpened you up . . . you had no idea what you were getting into until you went to them. And when they had the [patients] that already went through it, they are talking about it, it really helped out a lot.
Educational Resources/Approach Utilized by Patients.

Note. KFoC = Kidney Foundation of Canada Binder; CKD = chronic kidney disease; HCT = health care team; ✓ = yes, used resource/education method; X = no, did not use resource/education method; N/A = does not have internet; Blank = no response/no mention in interviews.
The hemodialysis unit tour helped set expectations, ease fears, and increase comfort levels. The KFoC binder and CKD websites appeared to play a larger role in improving patients’ understanding of CKD, the modality options available, and prompting questions to ask the HCT, rather than directly impacting their modality decision.
Support Systems
Patients reported consistently utilizing the HCT, family, and friends as an educational resource; therefore, it is important to understand these experiences as highlighted in Table 2.
Partnership with HCT
Nephrologists play a significant role in modality education and decision making. When a trusting partnership was established, patients had an enhanced sense of importance, control, and respect. When patients felt like valued members of the HCT, they were more likely to be receptive to information, be engaged in their care, and participate in shared decision making.
I really appreciated [the doctor’s] trust in me to assess myself and how much I could tolerate . . . his manner in general has always been “this is a partnership” . . . I mean the choice about [Home-HD] it was always my choice . . . I think his manner is really a model of how to engage patients in their own care.
Yet when there was not a sense of partnership, the opposite was found: “I feel like I was kinda forced. Because they really pushed for me to start dialysis. Each appointment they kept asking me.”
Patients were less likely to identify other HCT members as vital to decision making; however, when able, feedback was generally positive. Patients stated the case manager was an important educator, the social worker helped them cope and ease fears, and nurses provided emotional support.
Family and friends
Patients relied on family and friends, and lack of support often influenced the decision for IC-HD over a home-based therapy. Some patients relied on family members to educate them as one patient acknowledged, “My sister is also a Nephrologist so I talk a lot with her.” Other patients relied on family solely for moral support and assistance with dialyzing. Patients reached out to friends who had past experiences with CKD and dialysis. These supports influenced dialysis modality decisions, gave insight into the dialysis experience, and aided in the coping process.
. . . when I read [KFoC Binder] I ring people I know are in the medical field . . . my sister, my niece, my nephew. I would call them and I would say “what does that mean?”
Discussion
Dialysis modality decision making is a complex process requiring a skilled HCT and an appropriate educational process that can be individualized for patients and their supports. Our study explored patients’ learning and decision experiences, after they had made their dialysis modality decision. Their insights provide valuable information to inform the CKD education process to better inform decisions and outcomes. We identified 3 main elements to consider when establishing patient-informed decision making: patient factors, educational factors, and support systems. Specifically, patient-informed decision making requires nephrologist and HCT engagement and mutual trust with the patient, with the focus on maintaining patient quality of life and predialysis lifestyle, while acknowledging that individualization, autonomy, and emotion influence modality choice. These findings support and are consistent with many of the themes that are present throughout the literature on what influences decision making in the predialysis period.2,3 The maintenance of predialysis quality of life is a key factor when implementing any treatment intervention and achieving patient buy-in; therefore, this is essential to consider with dialysis modalities.1,3,8,17
Our study identified variability in preference for independent (autonomous) decision making. The amount of information patients desired also differed across the sample, regardless of their level of education and health literacy score. This highlights the importance of rechecking patient preferences with every visit. The use of decision aids increases autonomy in patients and brings about shared decision making between them and the HCT.2,14 Patients’ level of engagement and acceptance of information from the HCT and family and friends impacted their level of autonomy. Emotions influence knowledge transfer and informed decision making. Fear and denial were associated with a lack of understanding of their CKD and the need for treatment, negatively influencing patients’ willingness to receive information and make subsequent decisions. This is consistent with the finding that emotions interfere with knowledge acquisition and perception of the dialysis experience. 33 Fearful people tend to perceive higher risks.34,35 The HCT must identify and acknowledge these emotions through screening questions on coping before actively engaging in informed decision making, which may require social work intervention or postponing important treatment decisions. 11
Educational time and resources, tailored to patient preferences, are important to patient engagement in decision making.1,2,7,13,14,36 Patients require sufficient time and information to understand what modality best aligns with their lifestyle and to feel prepared to initiate dialysis. There is not one curriculum that can be applied to all patients, and the HCT must tailor based on the patients’ needs and requests. The HCT is also challenged in predicting the CKD progression trajectory. The literature suggests initiating modality education at least 9 to 12 months prior to the estimated start of dialysis.10,16 If education is initiated closer to the start of dialysis, the patient may be symptomatic or cognitively impaired, which is not conducive to informed decision making. 37 Patients reported not having access to certain available resources as well as not wanting all resources. This highlights the need for a flexible CKD education curriculum and a “library” of resources that can be tailored for each patient.21,38 Patients also asked for a pragmatic approach to modality information with full disclosure on the risks as well as the benefits. Clinicians are often limited in their ability to communicate individualized patient risks and outcome probabilities especially in the elderly.27,14 In addition, better role clarification is required as patients were not always able to identify HCT members and their roles. The group classes received positive feedback providing peer support, hope for the future, and self-management skills. 39 Previous studies report that participation in a treatment options class and early predialysis education results in more patients choosing home-based dialysis therapy.4,9,15,21,40 Research shows classes should include caregiver-focused information and coping skills.10,36,41
The CKD patient population is very diverse, with different ethnic, religious, and socioeconomic contexts, comorbidities, education level, and health literacy, all presenting their own unique challenges to effective education.3,11,28,42,43 Health literacy is a known barrier to effective education, and while our study is not quantitative in nature, it is interesting to note that participants with high subjective health literacy were present in all 3 modality groups. We believe that future studies looking at the correlation between health literacy and choice of renal replacement therapy would be worthwhile. Our sample had an adequate level of health literacy and education, were predominantly Caucasian, with a median age of 62, which is not representative of the CKD population at large and may contribute to our findings.7,28,44,45 However, a higher level of education and health literacy may have been beneficial, given that the nature of our study required patients to articulate experiences and medical decisions.
Our results show that establishing a patient-physician partnership through shared decision making is vital. Patients were more receptive and engaged when they felt part of the HCT. For shared decision making to be optimal, patients must receive and comprehend the appropriate knowledge.2,14,43,46 Research has shown there are various behavioral stages of change that affect how ready a patient is to make treatment decisions.47,48 Loiselle et al have recently identified 5 stages of decisional needs that patients with CKD journey through during the decision-making process. 33 More research is needed to determine what CKD and renal replacement therapy education is appropriate for patients at each stage of CKD progression. Our findings confirm prior research, suggesting patients who have an adequate support system from family or friends are more likely to choose home-based therapy over IC-HD. 4 It is important for clinicians to identify patients’ support systems and engage them in modality decision making.
Our research makes a novel contribution through the evaluation of educational needs and identification of educational methods that can be implemented to improve patient-informed decision making. Suggestions to improve CKD education delivery during the predialysis period, based on our interviews, are listed in Table 3. Patients strongly encourage attendance at group classes and that CKD education be more accessible outside of clinic. Videos of a “daily routine” for each modality assist with the visualization of the lived experience and are perceived as beneficial. 11 More patient partners were requested, offering more practical and authentic information from someone with lived dialysis experience.11,37 We would encourage CKD clinics to expand their educational approach to incorporate innovative methodologies, such as those outlined by Woods and Rosenberg. 49 It is vital that educational interventions constantly be evaluated so that innovations can be made to optimize the transfer of knowledge. 50
Suggestions for Improving CKD Education Delivery.

Note. CKD = chronic kidney disease.
Assessing patient readiness to receive information is a key first step and patients must be given adequate time to reflect on their own values and goals and be given the support needed to align their treatment decision with these values and goals. This is a challenge for CKD HCTs who are also charged with managing the CKD disease process and the comorbidities attached to the patient. A shared approach to develop flexible educational tools, decision aids that facilitate patient readiness and informed decision making on dialysis modality is needed. We have recently reviewed the influencers of renal replacement decision making and found that comprehensive education programs through multidisciplinary teams are vital to overcoming educational barriers and bringing about shared decision making. 51 A standardized CKD education plan that is delivered in an individualized manner should be the ultimate goal in predialysis CKD management. Through our narrative review, we have also found that patient-important outcomes are underreported and that incorporating patients into the research process itself can help inform methodology to incorporate the patient perspective. 51 We have taken this novel approach with the involvement of M.S., a patient on dialysis, which we believe has enriched our findings through the prioritization of CKD patients’ lived experiences.
Limitations
Our sample size was relatively small (n = 12) with adequate health literacy and our study was done at one point in time, meaning our findings may not be reflective of experiences in the wider CKD population. In addition, our inclusion criteria resulted in a limited number of eligible patients and unintentional bias could have been introduced. Interviewing health care providers in the clinic may have further enriched our findings. Lastly, participant responses may have been affected by poor recall of information that occurred during their predialysis period.
Conclusion
Modality selection is a complex process requiring an individualized approach for each patient. Patients’ decisions on renal replacement therapy are influenced through their own preferences and values, the education delivered to them, and the support systems available to them. Patient education can be improved through the standardization of a CKD curriculum and the establishment of a patient-HCT partnership. Consideration of each patient’s unique situation and values will allow educational challenges to be identified and overcome, achieving informed, shared decision making.
Footnotes
Acknowledgements
The authors thank the patients who participated in the study for sharing their time and experiences. They also thank Kerri Gallo who helped facilitate the study, Carolyn Ingram who provided a list of eligible participants, Kim Nitz who transcribed the interviews, and the various nurses who helped facilitate patient interviews.
Ethics Approval and Consent to Participate
Ethics approval was obtained from Western University Human Research Ethics Board (Review Number 108223).
Consent for Publication
Consent for Publication was acquired by the corresponding author from all co-authors.
Availability of Data and Materials
Data and materials are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Schulich Research Opportunities Program award.