
Abstract
Purpose of review
This article serves to describe the Can-SOLVE CKD network, a program of research projects and infrastructure that has excited patients and given them hope that we can truly transform the care they receive.
Issue
Chronic kidney disease (CKD) is a complex disorder that affects more than 4 million Canadians and costs the Canadian health care system more than $40 billion per year. The evidence base for guiding care in CKD is small, and even in areas where evidence exists, uptake of evidence into clinical practice has been slow. Compounding these complexities are the variations in outcomes for patients with CKD and difficulties predicting who is most likely to develop complications over time. Clearly these gaps in our knowledge and understanding of CKD need to be filled, but the current state of CKD research is not where it needs to be. A culture of clinical trials and inquiry into the disease is lacking, and much of the existing evidence base addresses the concerns of the researchers but not necessarily those of the patients.
Program overview
The Canadian Institutes of Health Research (CIHR) has launched the national Strategy for Patient-Oriented Research (SPOR), a coalition of federal, provincial, and territorial partners dedicated to integrating research into care. Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD) is one of five pan-Canadian chronic kidney disease networks supported through the SPOR. The vision of Can-SOLVE CKD is that by 2020 every Canadian with or at high risk for CKD will receive the best recommended care, experience optimal outcomes, and have the opportunity to participate in studies with novel therapies, regardless of age, sex, gender, location, or ethnicity.
Program objective
The overarching objective of Can-SOLVE CKD is to accelerate the translation of knowledge about CKD into clinical research and practice. By focusing on the patient’s voice and implementing relevant findings in real time, Can-SOLVE CKD will transform the care that CKD patients receive, and will improve kidney health for future generations.
What was known before
The evidence base for informing effective kidney care is limited, and the translation of existing knowledge to routine clinical care is slow. Canada’s Strategy for Patient-Oriented Research (SPOR) has raised awareness of the need to generate knowledge that is more relevant to people affected by kidney disease and to accelerate the translation of evidence into improvement in kidney health and care.
What this adds
Patient-oriented research focuses on priorities and outcomes that matter to patients, seeking to engage them throughout the research process and to generate results that can accelerate improvements in kidney health and care. The Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD) Network embraces a national partnership strategy with researchers, patients, policy makers, and other partners across Canada to transform kidney research and care.
Introduction
Chronic kidney disease (CKD) is a complex disorder that affects more than 4 million Canadians and costs the Canadian health care system more than $40 billion per year. 1 The majority of people with CKD have multiple comorbidities, placing them at high risk for complications. However, people with CKD are often excluded from clinical studies related to kidney disease. 2 Given this, the evidence base for guiding care in CKD is small, and even in areas where evidence exists, uptake of evidence into clinical practice has been slow.
Compounding these complexities are the variable prognoses among patients with CKD and difficulties predicting who is most likely to develop complications over time. As such, health care professionals are unable to accurately inform patients of pertinent information such as time to dialysis or death and trajectories of disease progression. Although progress has been made, many knowledge gaps remain, notably the underlying disease mechanisms, the epidemiology and burden in different locations, and genetic and environmental interactions.
Clearly these gaps in our knowledge of CKD need to be filled, but the current state of CKD research is not where it needs to be. A sufficient number of mechanistic targets have yet to be identified, and many trials have failed due to poor study design or challenges with recruitment. Much of the existing evidence base addresses the concerns and curiosity of researchers but does not necessarily align with the areas of highest priority to patients. 3
Aligning research with patient needs and accelerating the translation of evidence into practice are now prerequisites for several health research funding competitions in the United Kingdom and the United States.4-6 In Canada, the Canadian Institutes of Health Research (CIHR) has launched the national Strategy for Patient-Oriented Research (SPOR), a coalition of federal, provincial, and territorial partners dedicated to integrating research into care. The ultimate objective of SPOR is to foster evidence-informed and patient-centered care by bringing innovative diagnostic and therapeutic approaches to the point of care, so as to ensure greater quality, accountability, and accessibility of care. As part of SPOR, CIHR is funding provincial SUPPORT (Support for People and Patient-Oriented Research and Trials) Units and national networks that will help advance patient-oriented research. 7
Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD) is one of 5 pan-Canadian chronic disease networks supported through SPOR. The vision of Can-SOLVE CKD is that by 2020, every Canadian with or at high risk for CKD will receive the best recommended care, experience optimal outcomes, and have the opportunity to participate in studies with novel therapies, regardless of age, sex, gender, location, or ethnicity. The network is led by a steering committee that includes a broad range of patients affected by a representative mix of medical conditions, policy makers, researchers, and charitable foundations. Its co-principal investigators are Dr Adeera Levin (University of British Columbia) and Dr Braden Manns (University of Calgary).
This article serves to describe the Can-SOLVE CKD Network, a program of research projects and infrastructure that has excited patients and given them hope that we can truly transform the care they receive.
Network Objective
The overarching objective of Can-SOLVE CKD is to accelerate the translation of knowledge about CKD into clinical research and practice. To fulfill this objective, a coast-to-coast partnership of patients, health care providers, policy- and decision-makers (herein referred to as policy makers), and researchers will build on key existing human resources, core infrastructure, and research partnerships to create a sustainable network.
Network Development
The Can-SOLVE CKD Network builds on an existing collaborative community that has emerged in Canada over the last 15 years and is committed to improving the quality of care and outcomes for CKD patients. Two planning conferences, in 2000 and 2007,8,9 involved key stakeholders from the kidney community. The first led to the development of a national interdisciplinary training program (Kidney Research Scientist Core Education and National Training [KRESCENT], www.krescent.ca) 10 for allied health professionals, basic scientists, and clinician scientists. The second conference led to the formation in 2010 of the CAnadian KidNey KNowledge TraNslation and Generation NeTwork (www.CANN-NET.ca) 11 to enhance collaboration and exchange of information between researchers and knowledge users. The Can-SOLVE CKD Network, with its broad engagement of key stakeholders, is well positioned to consolidate and leverage these activities to overcome the limitations of existing networks and address the needs of all people with CKD, extending the benefits to Canadians with other chronic diseases.
Patient-Oriented Research Program
The goal of patient-oriented research is “to better ensure the translation of innovative diagnostic and therapeutic approaches to the point of care, as well as to help the provinces and territories meet the challenge of delivering high quality, cost-effective health care.” 12 Patient-oriented research focuses on priorities that are important to patients, engages patients in the research process, and produces information that can be used in meaningful ways to improve health care practice.
Using an established patient priority-setting framework by the James Lind Alliance, 13 a 3-year national process of patient consultation was undertaken to identify the top 10 research priorities of individuals with early or more advanced CKD, their families, and care providers (Figure 1).9,14,15 Since the inception of the Can-SOLVE CKD Network in March 2014, patients have continued to meet regularly with researchers and policy makers. Two workshops were held with more than 30 patients, caregivers, Indigenous peoples, researchers, and policy makers to finalize research priorities using a modified Delphi process. These priorities informed the development of 18 multidisciplinary research projects spanning biomedical first-in-human studies, clinical research trials, population health research, and knowledge translation (KT). This research agenda forms the foundation of the network.

Can-SOLVE CKD patient-oriented priority-setting process.
The highest priority areas identified by patients and policy makers were those pertaining to early diagnosis and prognosis—improved understanding of pathobiology and stratifying patients based on risk (Theme 1); treatment options for CKD and comorbidities, and how best to address physical and emotional symptoms (Theme 2); and optimal models of care in chronic disease (Theme 3). Table 1 illustrates research priorities and projects that patients and policy makers included within each theme, connected by a common focus on stratification and personalization. Two examples of the research projects conducted under Can-SOLVE CKD are described in Table 2. Others are available at www.cansolveckd.ca.
Can-SOLVE CKD Research Themes, Priorities, and Projects.
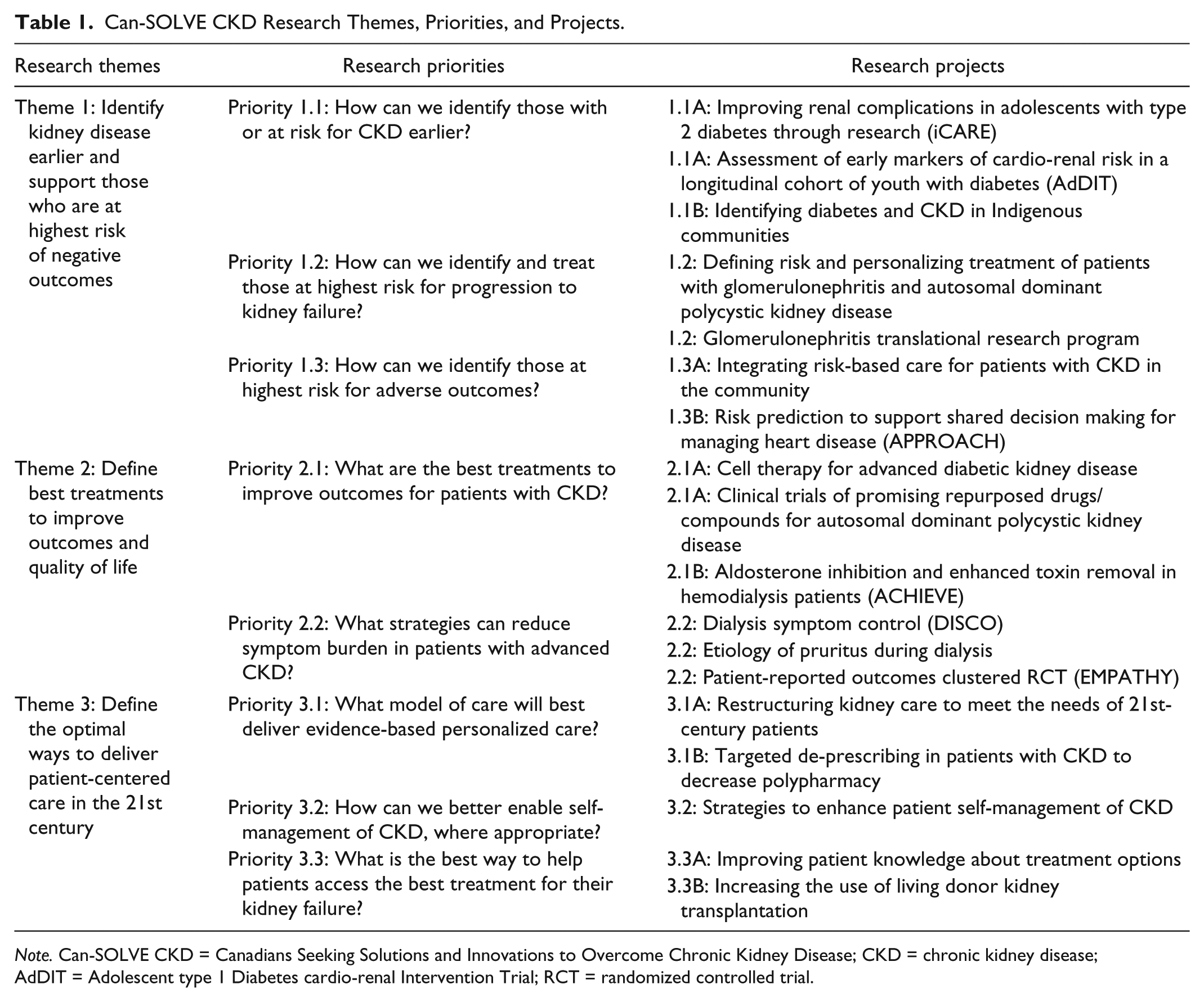
Note. Can-SOLVE CKD = Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease; CKD = chronic kidney disease; AdDIT = Adolescent type 1 Diabetes cardio-renal Intervention Trial; RCT = randomized controlled trial.
Examples of Selected Can-SOLVE CKD Research Projects.

Note. Can-SOLVE CKD = Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease; CKD = chronic kidney disease.
As the network executes the projects, patients have been integrated into the research teams, bringing the patient voice to all aspects of the research: design, development, recruitment, implementation, and KT. This partnership is a new way of doing research, requiring a culture change for all involved. To help effect this change, Can-SOLVE CKD has hosted 2 training workshops to help enable a truly effective and meaningful partnership. To date, 56 network members have received training in patient-oriented research at sessions facilitated by Can-SOLVE CKD.
Core Infrastructure
The network’s sustainability plan includes creating core national infrastructure for research, KT, and training. The national KT network for patients with kidney failure (www.cann-net.ca) will be expanded, as will the scope of a national network of multidisciplinary CKD clinics. 16 These resources will be key to disseminating results of Can-SOLVE CKD studies. A repository for biosamples across diabetes, glomerulonephritis, and polycystic kidney disease17-19 will be created to support collaborative research. Current research training programs will grow. All resources will be united to create core infrastructure that is greater than the sum of its parts (Table 3).
Network Core Infrastructures.

Note. Can-SOLVE CKD = Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease; PKD = polycystic kidney disease; AdDIT = Adolescent type 1 Diabetes cardio-renal Intervention Trial; KT = knowledge translation; CKD = chronic kidney disease; CNTN = Canadian Nephrology Trials Network; KRESCENT = Kidney Research Scientist Core Education and National Training.
Partnerships
Engaging the partners noted in Table 4 will transform care for CKD patients across Canada. National and international disease-based advocacy and patient groups, health charities, provincial kidney care programs, community organizations, professional societies, and research and training networks are all essential to the network’s success and are represented on the Can-SOLVE CKD Steering Committee. In addition to CIHR, the network is funded by more than 30 funding partners, from foundations to individual donors, with donations ranging from several thousand to several million dollars. Many organizations are committing in-kind resources to facilitate network activities.
Can-SOLVE CKD Partners.

Note. Can-SOLVE CKD = Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease; KFOC = Kidney Foundation of Canada; CKD = chronic kidney disease; CSN = Canadian Society of Nephrology; IPERC = Indigenous Peoples’ Engagement & Research Council.
Policy Makers
Policy makers are also integral partners and engaged in all aspects of the work: identifying health issues of strategic importance, designing and implementing interventions, and translating findings into practice. The network has strong links with policy makers across Canada and a track record of influencing health care policy.38,39 This partnership and experience will maximize the likelihood that network innovations will be scaled up if study findings are positive, or modified or discontinued if they are not shown to be effective, thus reducing costs to the health care system. Furthermore, policy makers from Indigenous communities are involved in all aspects of the initiative.
Patient-Oriented Research Training and Mentorship
To implement a patient-oriented research network requires training of all involved—patients, researchers, policy makers—in this new way of conducting research. The Can-SOLVE CKD Network will leverage KRESCENT, the existing and highly successful national transdisciplinary program for kidney scientists (www.KRESCENT.ca), to deliver a robust, innovative, and structured teaching/mentoring program that will revolutionize kidney research training for all stakeholders in Canada by:
Training patients and their informal caregivers to engage as full partners in the Can-SOLVE CKD Network, and to serve as mentors for other patients, ensuring program sustainability. This will be done in conjunction with the standardized national “Foundations in Patient-Oriented Research” developed by a CIHR reference group.
Training researchers to develop expertise in patient-centered research and how to work in research teams effectively with patients. This will involve researchers from multiple disciplines conducting research of relevance to Can-SOLVE CKD, including translational scientists capable of commercializing innovative discoveries, and clinical researchers able to assess the quantitative and qualitative impact of novel treatments and education on outcomes important to patients.
Training nephrology health care providers to develop skills in patient engagement and patient-oriented care. Workshops in patient-oriented care for Canadian nephrology fellows and other health care trainees attending the nephrology trainee pre-course will take place at the Canadian Society of Nephrology (CSN) annual meeting.
Training policy makers on key aspects of the full spectrum of patient-oriented research, including the use of health research data to produce evidence-based policy. This will also enable input from health care policy makers to inform future Can-SOLVE CKD priority research questions.
Knowledge Translation
Effective KT is the foundation of the Can-SOLVE CKD Network. The evidence generated will be shared with a broad spectrum of end-users, enabling its application in real-world settings and ensuring a return on investment. The network uses an integrated KT approach whereby key end-users, including patients, caregivers, clinicians, and health policy- makers, are involved from research inception through to the dissemination and implementation of results. This approach emphasizes regular interactions with key stakeholders across all phases and also ensures that specific audiences are targeted for knowledge dissemination at the end. The team will build on the successes of CANN-NET, which has implemented a series of national KT initiatives using educational tools aimed at patients and providers as well as a broad range of implementation strategies.40,41
Governance
As a patient-oriented research network, Can-SOLVE CKD comprises several committees and councils. The organizational structure is developed around patients, as depicted in Figure 2, including both the Patient Council and the Indigenous Peoples’ Engagement & Research Council (IPERC). At least 2 patients serve on all Can-SOLVE CKD committees, thus enabling bidirectional communication between committees, the Patient Council and IPERC.

Can-SOLVE CKD organizational chart.
The Patient Council is the core and the heart of Can-SOLVE CKD. The Council is co-chaired by 3 patients with unique lived experience of CKD (Table 5). Membership includes a broad range of patients affected by a representative mix of medical conditions (eg, diabetes, heart disease, polycystic kidney disease) as well as caregivers and kidney donors. Representation is diversified in terms of age, sex, geography, and ethnic and cultural background.
Can-SOLVE CKD Patient Council Co-chairs.

Note. Additional patient profiles are available at https://cansolveckd.ca/patient-partners/patient-stories.
IPERC serves to guide the conduct of the network’s activities in accounting for the unique aspects of patient-oriented research involving First Nations, Inuit, and Métis people. Using an ethical framework that encompasses the principles of ownership, control, access, and possession, IPERC’s mandate is to ensure that Can-SOLVE CKD appropriately incorporates, addresses, and respects the unique needs and perspectives of Indigenous peoples.
All committees report to the Steering Committee through the respective committee co-chairs. The Steering Committee is ultimately accountable to the Board of Directors of the CSN and the Kidney Foundation of Canada (KFOC). Committee Chairs are nominated by the respective committees and appointed by the Executive Committee. The Can-SOLVE CKD International Research Advisory Committee (CIRAC) provides advisory support to the network, and the Core Operations Team provides the infrastructure support to keep the network functioning on a day-to-day basis.
Tracking the Impact of Can-SOLVE CKD
Network activities will be tracked and reported according to a performance measurement framework with a series of process and outcome measures. For example, performance-management research-to-impact frameworks are described by the Canadian Academy of Health Sciences and Alberta Innovates Health Solutions.42,43 Examples of these measures include number of patient partners engaged; experiences of patients engaged in research teams; percentage of partners trained in patient-oriented research; numbers of Indigenous people screened, triaged, and treated; number of living donor and preemptive kidney transplants; and uptake of home therapies as measures of informed decision making and an appropriately resourced health care system. The network will also begin to track patient experiences formally and regularly as part of routine care.
Conclusion
The Can-SOLVE CKD Network will provide the infrastructure necessary to drive patient-oriented research and implement evidence into clinical practice. By linking patients, caregivers, policy makers, researchers, and clinicians, the network promotes a cultural shift from care which is disease-centered and provider-focused to care which is patient-centered, informed by evidence, and coordinated across the health care system.
By focusing on the patient’s voice and implementing relevant findings in real time, Can-SOLVE CKD will transform the care that CKD patients receive, and will improve kidney health for future generations.
Footnotes
Acknowledgements
The authors thank all patients, researchers, policy makers, health care professionals, and other partners who inspire and support this network.
Ethics Approval and Consent to Participate
No ethics approval or consent to participate was required for this publication.
Consent for Publication
All authors read and approved the final version of this manuscript.
Availability of Data and Materials
No primary data is presented in this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Canadian Institutes of Health Research through the Strategy for Patient-Oriented Research (SPOR). Additional funding is provided by more than 30 partners, including provincial kidney care agencies, universities, industry, and private donors.