
Abstract
Background:
Acute kidney injury (AKI) is common in the kidney transplant population.
Objective:
To derive a multivariable survival model that predicts time to graft loss following AKI.
Design:
Retrospective cohort study using health care administrative and laboratory databases.
Setting:
Southwestern Ontario (1999-2013) and Ottawa, Ontario, Canada (1996-2013).
Patients:
We included first-time kidney only transplant recipients who had a hospitalization with AKI 6 months or greater following transplant.
Measurements:
AKI was defined using the Acute Kidney Injury Network criteria (stage 1 or greater). The first episode of AKI was included in the analysis. Graft loss was defined by return to dialysis or repeat kidney transplant.
Methods:
We performed a competing risk survival regression analysis using the Fine and Gray method and modified the model into a simple point system. Graft loss with death as a competing event was the primary outcome of interest.
Results:
A total of 315 kidney transplant recipients who had a hospitalization with AKI 6 months or greater following transplant were included. The median (interquartile range) follow-up time was 6.7 (3.3-10.3) years. Graft loss occurred in 27.6% of the cohort. The final model included 6 variables associated with an increased risk of graft loss: younger age, increased severity of AKI, failure to recover from AKI, lower baseline estimated glomerular filtration rate, increased time from kidney transplant to AKI admission, and receipt of a kidney from a deceased donor. The risk score had a concordance probability of 0.75 (95% confidence interval [CI], 0.69-0.82). The predicted 5-year risk of graft loss fell within the 95% CI of the observed risk more than 95% of the time.
Limitations:
The CIs of the estimates were wide, and model overfitting is possible due to the limited sample size; the risk score requires validation to determine its clinical utility.
Conclusions:
Our prognostic risk score uses commonly available information to predict the risk of graft loss in kidney transplant patients hospitalized with AKI. If validated, this predictive model will allow clinicians to identify high-risk patients who may benefit from closer follow-up or targeted enrollment in future intervention trials designed to improve outcomes.
What was known before
Acute kidney injury is common in the kidney transplant population and is associated with an increased risk of graft loss.
What this adds
This study serves as a first step toward identifying kidney transplant patients with acute kidney injury who are at highest risk for graft loss.
Background
Studies in patient populations excluding kidney transplant recipients show that acute kidney injury (AKI) affects between 2% and 12% of all hospitalized patients1-5 and is associated with an increased risk of subsequent chronic kidney disease (CKD) and death.6-13 Emerging data suggest that AKI and CKD are closely interconnected syndromes, with each being a risk factor for the other. Importantly, increased vigilance and monitoring of AKI survivors is being recognized as a key step to improving outcomes. 14 Predictive models have been developed in the general population to identify individuals at highest risk of developing advanced CKD following AKI. 15 These predictive models could be used to better identify which patients require follow-up by a nephrologist post AKI or for targeted enrollment of patients in interventional trials with the goal of improving patient outcomes post AKI.
The consequences of AKI in the kidney transplant setting are less known. Two recent studies suggest that AKI is associated with an increased risk of subsequent graft loss and death.16,17 However, we currently cannot predict which AKI patients are at greatest risk for graft loss. In this study, we aimed to derive a predictive model to quantify the risk of graft loss following an episode of hospitalized AKI in kidney transplant recipients. We modified the model into a simple scoring system based on readily available data so that it could be easily implemented in clinical practice. Our goal is to guide and improve the care of kidney transplant patients following AKI by identifying those at highest risk for graft loss.
Methods
Design and Setting
We conducted a population-based retrospective cohort study in the province of Ontario, Canada, using Ontario’s linked health care administrative databases and laboratory data from Southwestern Ontario and Ottawa, Ontario. Residents of Ontario have universal access to hospital care and physician services under a single provincial payer system, which provides a comprehensive set of health administrative data. The availability of laboratory data was limited to Southwestern Ontario and Ottawa, Ontario. The study was conducted according to a prespecified protocol approved by the Ottawa Hospital Research Ethics Board. The reporting of this study follows the TRIPOD (Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis) Statement for multivariable prediction models (Online Appendix 1). 18
Data Sources
We ascertained patient characteristics, laboratory data, and outcome data by linking 8 databases using encrypted unique identifiers. We identified kidney transplant recipients using the Canadian Organ Replacement Register (CORR), which captures all kidney transplants in Ontario. 19 Laboratory data were obtained from the Ottawa Hospital Data Warehouse (OHDW) for Ottawa patients, and Cerner and Gamma-Dynacare for Southwestern Ontario patients. OHDW houses inpatient and outpatient lab information for individuals who had blood work drawn at any one of three hospitals in Ottawa, Ontario. Cerner is a hospital network in Southwestern Ontario, housing inpatient and outpatient lab data from 12 hospitals. Gamma-Dynacare is a laboratory service provider that contains outpatient lab information for individuals who had blood work drawn at any one of their 148 collection sites in Ontario. Demographics and vital status information were obtained from the Ontario Registered Persons Database (RPDB) (which records the sex, birthdate, and death date of all Ontarians) and CORR. Diagnostic and procedural information from all hospitalizations was determined using the Discharge Abstract Database (DAD), which captures demographic, diagnostic, and procedural information for all Ontario hospitalizations. Information was also obtained from the Ontario Health Insurance Plan database, which contains all health claims for inpatient and outpatient physician services. Outcome data were obtained using RPDB, CORR, and the Ontario Renal Reporting System (ORRS). ORRS captures demographic, diagnostic, and renal replacement therapy information for all Ontarians with end-stage renal disease. We have previously used these databases to research renal health outcomes and health services.20-22 Whenever possible, we defined patient characteristics and outcomes using validated codes (Online Appendix 2).
AKI
We used the Acute Kidney Injury Network (AKIN) staging system to define AKI. 23 The urine output criteria for the AKIN staging system were not used as these data were not available in our databases. The peak creatinine during a hospital admission was used to define the presence or absence of AKI and the AKIN stage.
Study Cohort
We included kidney transplant patients with in-hospital AKI (based on AKIN stage 1 or greater) and the following characteristics: (a) first-time kidney only transplant recipients, (b) hospital admission occurring 6 months or greater from the transplantation date, (c) at least 1 serum creatinine value available during the hospital admission, (d) discharge date prior to the end date of laboratory data availability (December 31, 2012, for Ottawa and March 31, 2012, for Southwestern Ontario), and (e) serum creatinine data available anytime between 2 weeks and 6 months prior to the admission date to determine baseline creatinine. If multiple baseline creatinine values were available, the most recent test result was used. Creatinine values drawn less than 2 weeks prior to admission were excluded because the patient could have been unwell at the time of the blood work; the result may therefore not reflect a true baseline value but possibly the beginning of the AKI episode. Hospital admissions less than 6 months post transplant were excluded to help avoid AKI secondary to postoperative complications, delayed graft function, and early acute rejection. Based on lab data availability, we excluded patients with a kidney transplant date prior to January 1, 1996 (Ottawa) and prior to April 1, 1999 (Southwestern Ontario). Only the first admission with AKI was included in the analysis.
Outcomes
The primary outcome was graft loss (defined by a return to dialysis or repeat kidney transplant) with death as a competing event. A composite endpoint comprising graft loss or death was also examined. Patients were followed until December 31, 2013. This was the final date for which outcome data were available.
Statistical Analysis
We analyzed the data using competing risk regression using the Fine and Gray method. 24 We created models that examined covariates associated with time to graft loss (death as a competing event) and with time to death (graft loss as a competing event) (time to death results presented in Online Appendix 3). Observation of patients started when they were diagnosed with AKI and ended when patients died, had graft loss, or were censored at the study end date. We used Cox regression analysis to determine the independent association between potentially prognostic covariates and time to graft loss or death (results presented in Online Appendix 3). The following prespecified variables were included in all regression models: age (by decade), year of kidney transplant (1996 to 1998 and 2010 to 2012 were grouped together due to a lower number of patients during these time periods), time on dialysis prior to transplant, time from transplant to admission with AKI, baseline estimated glomerular filtration rate (eGFR; calculated using the CKD-Epi equation 25 ), AKIN stage, recovery from AKI, congestive heart failure (CHF) and diabetes status, and type of kidney donor (living vs deceased). Complete recovery from AKI was defined by a last available admission creatinine less than 26.5 µmol/L above the baseline value. A look-back period of 3 years from date of admission was used to determine comorbid conditions.
We used fractional polynomial functions to determine the best linear or nonlinear form for continuous variables.26-28 Donor type was the only covariate with missing values, with less than 2% of observations having a missing value. Therefore, missing values for donor status were imputed using a logistic regression model derived from the cohort to predict donor status. The competing risk model examining the outcome of graft loss was used to create the risk score. Covariates with a P value ≤ .05 and AKI-specific covariates were kept in the model. Certain covariates with a P value > .05, such as type of donor, were retained in the model, as they were thought to be clinically significant based on prior data.29,30
Details pertaining to the creation and assessment of the risk score are available in Online Appendix 4. The risk score was derived using methods described by Sullivan et al. 31 A concordance statistic was calculated using the methods described by Blanche et al. 32 Due to the small size of the final cohort, we did not divide the cohort into derivation and validation groups. A bootstrapping procedure was used to internally validate the risk score and determine optimism. To maintain patient privacy, small cells ≤5 were suppressed. We conducted all analyses with the SAS software, version 9.4 (SAS Institute Inc, Cary, North Carolina).
Results
Our cohort included 315 patients (Table 1, Supplementary Figure 1). The mean (SD) age was 55.1 (12.9) years, with most patients being male (62%) and White (77%). The median (interquartile range [IQR]) length of hospital stay was 42-8 days. The median (IQR) time from transplant to first hospitalization with AKI was 2.1 (0.9-4.4) years. Most patients had reduced baseline kidney function (the median [IQR] baseline eGFR was 46 mL/min/1.73 m2 [34.0-60.4]). The majority of patients (76.2%) experienced mild AKI (AKIN stage 1). No patients required acute dialysis. The median (IQR) rise in creatinine for AKIN stages 1, 2, and 3 was 44.2 µmol/L (35.4-70.7), 132.6 µmol/L (114.9-150.3), and 238.7 µmol/L (168.0-327.1), respectively. The median (IQR) ratio of peak creatinine to baseline creatinine for AKIN stages 1, 2, and 3 was 1.4 (1.3-1.5), 2.2 (2.1-2.5), and 3.0 (1.7-3.5), respectively. One hundred seventy-one patients (54% of the cohort) had subsequent admissions to hospital with AKI.
Baseline Characteristics of Study Cohort.
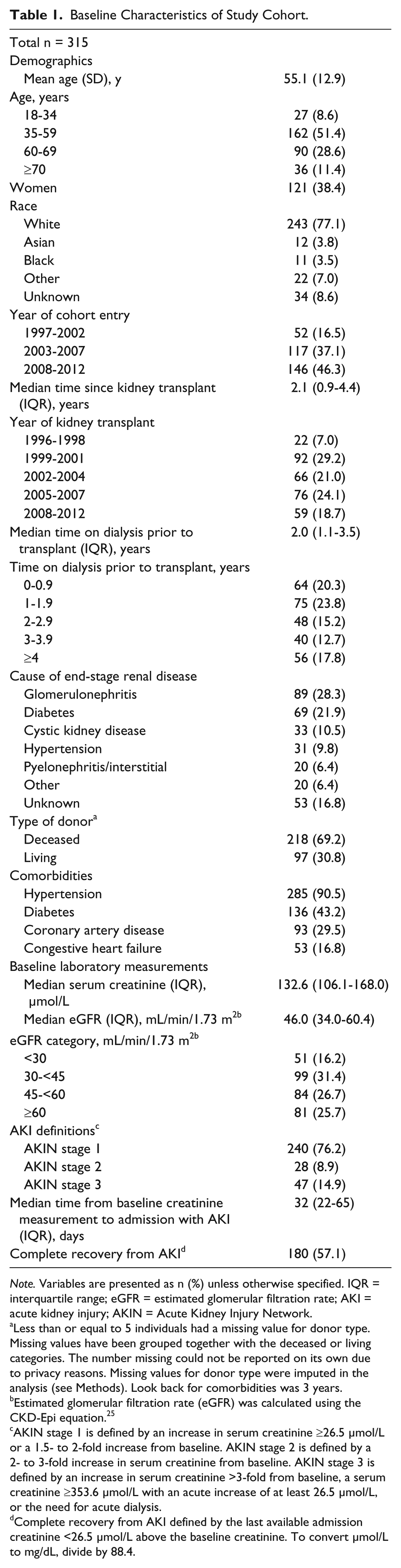
Note. Variables are presented as n (%) unless otherwise specified. IQR = interquartile range; eGFR = estimated glomerular filtration rate; AKI = acute kidney injury; AKIN = Acute Kidney Injury Network.
Less than or equal to 5 individuals had a missing value for donor type. Missing values have been grouped together with the deceased or living categories. The number missing could not be reported on its own due to privacy reasons. Missing values for donor type were imputed in the analysis (see Methods). Look back for comorbidities was 3 years.
Estimated glomerular filtration rate (eGFR) was calculated using the CKD-Epi equation. 25
AKIN stage 1 is defined by an increase in serum creatinine ≥26.5 µmol/L or a 1.5- to 2-fold increase from baseline. AKIN stage 2 is defined by a 2- to 3-fold increase in serum creatinine from baseline. AKIN stage 3 is defined by an increase in serum creatinine >3-fold from baseline, a serum creatinine ≥353.6 µmol/L with an acute increase of at least 26.5 µmol/L, or the need for acute dialysis.
Complete recovery from AKI defined by the last available admission creatinine <26.5 µmol/L above the baseline creatinine. To convert µmol/L to mg/dL, divide by 88.4.
Outcomes
The median (IQR) follow-up time was 6.7 (3.3-10.3) years, and there were 1377 person-years of observation time. Eighty-seven (27.9%) patients had graft loss, 71 (22.5%) patients died prior to experiencing graft loss, and 157 patients (49.8%) were censored at the end of the observation period.
Regression Model for Graft Loss With Death as a Competing Event
We found that younger age, failure to recover from AKI, and lower baseline eGFR were all independently associated with an increased risk of graft loss (P < .05) (Table 2, Figures 1 and 2). Baseline eGFR and age had the strongest association with graft loss. Each increase of 1 mL/min/1.73 m2 in baseline eGFR was associated with a 4% (95% confidence interval [CI], 3%-6%) reduction in the risk of graft loss (Figure 1). Similarly, older age was associated with a lower risk of graft loss (Figure 2). A history of CHF, diabetes, type of kidney donor, (Table 2), year of kidney transplant (Supplementary Figure 2), time on dialysis prior to kidney transplant (Supplementary Figure 3), and time from kidney transplant to admission with AKI (Supplementary Figure 4) were not significantly associated with graft loss (P > .05). When examined in univariate analysis, AKI severity was associated with graft loss (hazard ratio [95% CI], 0.69 [0.29-1.64] and 1.76 [1.04-2.96]; AKI stage AKIN 2 and AKIN 3 respectively); however, this association was no longer significant in multivariate analysis (Table 2). The regression model used to create the risk score for graft loss is presented in Table 3.
Competing Risk Multivariate Regression Analysis for Time to Graft Loss.

Note. Competing risk analysis with death treated as a competing event. The association of continuous variables with time to graft loss is presented graphically in Figures 1 and 2 and Supplementary Figures 2 to 4. CI = confidence interval; AKIN = Acute Kidney Injury Network; AKI = acute kidney injury.
Recovery from AKI defined by the last available admission creatinine <26.5 µmol/L above the baseline creatinine.

Adjusted hazard ratio for graft loss: Baseline eGFR.

Adjusted hazard ratio for graft loss: Age.
Multivariate Regression Model Used to Create the Risk Score for the Prediction of Graft Loss. a

Note. CI = confidence interval; AKIN = Acute Kidney Injury Network; AKI = acute kidney injury; eGFR = estimated glomerular filtration rate.
A competing risk model with death as a competing event was used. Variables in Table 2 with a P value ≤ .05, AKI-specific variables, as well as type of donor and time since kidney transplant, due to prior data, were maintained in this model.
Hazard ratios are not presented. Age (per decade) and time since transplant were transformed; therefore, their hazard ratios cannot be directly interpreted. Age (per decade) was transformed to 1 / age2 and time since transplant was transformed to 1 / √time since transplant.
Recovery from AKI defined as the last available admission creatinine <26.5 µmol/L above the baseline creatinine.
Prognostic Risk Score for Graft Loss With Death as a Competing Event
A prognostic risk score was derived with graft loss as the outcome of interest. The final prognostic index variables, along with the scoring system, are presented in Table 4. Potential risk scores ranged from −5 to 26, corresponding to a 5-year predicted probability of graft loss between 1.2% and 100%, respectively (Table 5). An individual patient’s risk score can be calculated by summing up the points for each risk factor presented in Table 4. For example, a 55-year-old woman (−3) with AKI AKIN stage 2 (2), a baseline eGFR of 45 mL/min/1.73 m2 (5), and a deceased donor kidney transplant (1) performed 3 years ago (1) who has not completely recovered from her AKI event (2) has a risk score of 8 with a predicted risk of graft loss within 5 years of 20.8%.
Risk Score to Predict Graft Loss in Patients With a Kidney Transplant Hospitalized for AKI. a

Note. AKI = acute kidney injury; eGFR = estimated glomerular filtration rate; AKIN = Acute Kidney Injury Network.
The methods of Sullivan et al 31 were used to convert the model in Table 3 to a simple point system. The risk score was derived from a competing risk model with time to graft loss as the outcome and death as the competing event. To calculate the risk score, points for all factors are summed. The predicted risk of graft loss within 5 years for each risk score is presented in Table 5.
Recovery from AKI defined by the last available admission creatinine being <26.5 µmol/L above the baseline creatinine.
Predicted and Observed 5 Year Risk of Graft Loss (Death as a Competing Event) by Risk Score.
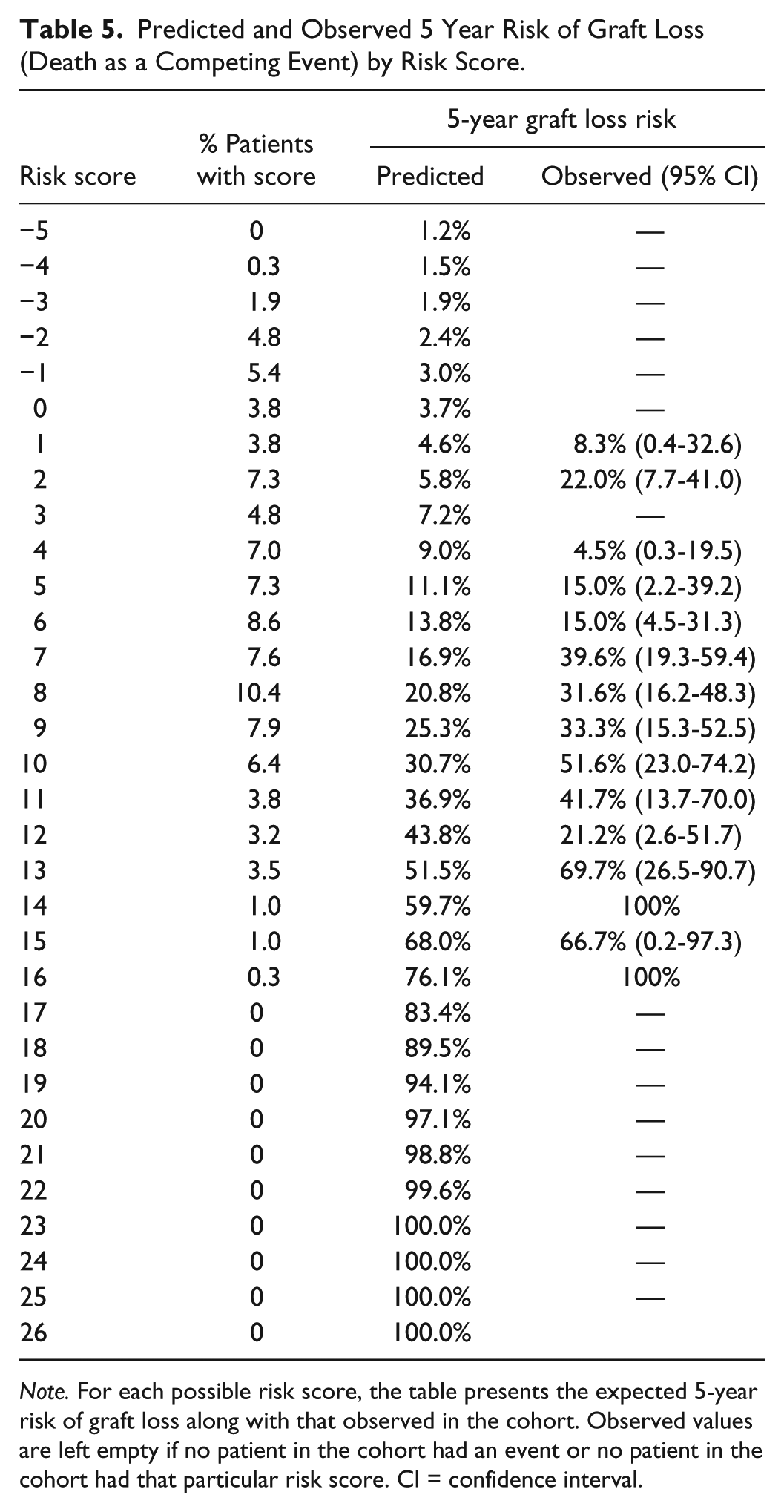
Note. For each possible risk score, the table presents the expected 5-year risk of graft loss along with that observed in the cohort. Observed values are left empty if no patient in the cohort had an event or no patient in the cohort had that particular risk score. CI = confidence interval.
The prognostic risk score had a concordance statistic of 0.75 (95% CI, 0.69-0.82). A bootstrapping procedure was performed to internally validate the risk score, which generated a concordance statistic of 0.81 (95% credible interval, 0.79-0.82) and an optimism of 0.002. The model generated predicted 5-year risk of graft loss fell within the 95% CI of the observed risk more than 95% of the time; however, due to the small size of the cohort, the CIs for the observed risk were wide, especially at the highest risk scores. Overall, the observed risk tended to be greater than the predicted risk (Figure 3, Table 5).

Comparison of predicted and observed risks of graft loss within 5 years by risk score.
Discussion
We derived a risk score that predicts graft loss following a hospital admission with AKI in kidney transplant patients. The score uses objective, readily available information to estimate the risk of graft loss within 5 years after the AKI event. Our risk score requires validating; however, it serves as a first step toward prognosticating kidney transplant patients who develop AKI in the months to years following transplant and was reasonably discriminative in our derivation cohort.
When a competing risk analysis was performed with graft loss as the outcome of interest, the risk substantially increased with younger age. As a result, younger patients are given the greatest number of points in our derived risk score. The association of younger age with an increased risk of graft loss has been demonstrated in prior studies.33,34 Younger individuals may be more likely to experience graft loss defined by a return to dialysis or repeat kidney transplant due to the fact that they live longer. 35 Moreover, younger recipients may be more prone to acute rejection.36,37 Although the rate of acute rejection was likely very low in our cohort due to the timing of the AKI events,38,39 the youngest patients may have had proportionately more AKI caused by late acute rejection from nonadherence. 40 As expected, older age was strongly associated with death with graft function. When a composite outcome of death or graft loss was considered, the risk decreased with increasing age, contrary to what was expected, illustrating the bias that can occur when a composite outcome is used.
Similar to previously published studies, reduced baseline eGFR was a very strong predictor for graft loss.33-35,39,41-46 CHF and diabetes, representative of patients with greater cardiovascular risk, were associated with a higher risk of death with graft function but not graft loss. Receipt of a deceased donor kidney transplant was not significantly associated with any of the outcomes of interest. Based on prior nationally collected Canadian data, we expected that having a deceased donor kidney would increase the risk of graft loss. 47 Our results may conflict with prior data due to a number of reasons: statistical power, previously published national data were unadjusted, and donor type may have less of an effect on graft loss in high-risk transplant patients (ie, patients admitted with AKI). Due to type of donor being commonly accepted as a risk factor for graft loss, it was maintained in the risk score despite the lack of statistical significance. Although not statistically significant, there was a trend toward an increased risk of death with graft function in more recent transplant years. We suspect that this is due to the transplantation of older, sicker individuals in more recent years. Although the analysis was adjusted for age and comorbidities, residual confounding may remain. Time spent on dialysis prior to transplant increased the risk of death with graft function but not graft loss. This is likely due to the fact that patients who spend more time on dialysis develop more comorbidities and are at increased risk for cardiovascular disease. 48 More severe AKI was associated with an increased risk of graft loss in unadjusted analyses, but this result was no longer significant upon adjustment for important confounders, including recovery from AKI, which remained a significant predictor of graft loss in adjusted analyses. This suggests that failure to recover from AKI is a more important predictor than severity of the AKI event.
Our study has several strengths. First, we included AKI-specific factors and quantified the risk of graft loss following a hospitalized AKI event, items lacking from prior models.49-51 Second, to our knowledge, our study is the first to derive a risk score that predicts graft loss in kidney transplants using a competing risk model. Many studies in kidney transplantation use a composite outcome of death or graft loss or a “pseudo-competing event” model with death-censored graft loss as the outcome.16,45,49-53 As demonstrated in our study, risk factors for graft loss and for death may differ significantly; combining the 2 outcomes may produce a biased estimate. Performing a death-censored analysis will also lead to a biased estimate, in particular if the mortality rate is high, as it was in our cohort.24,54 Third, despite the relatively small sample size (n = 315 patients), this is the largest study, that we are aware of, to examine AKI in the kidney transplant population defined by serum creatinine values rather than administrative codes.16,17,55 Moreover, this was a high-risk population with a high event rate. Last, all of the variables included in our risk score are objective and readily available to clinicians.
There are important limitations worth noting. First, this was a retrospective study. As a result, data on important factors, such as proteinuria, prior rejection episodes, and delayed graft function,35,53,56-63 were not available. However, some of these missing factors would be partially accounted for by the inclusion of baseline eGFR. Second, the cause of AKI could not be determined from the data sets; however, acute rejection at this time post-transplantation would be rare38,39 (median time from transplant to AKI admission was 2 years). Prior studies on AKI in this setting suggest that infection is the most common cause.17,55 Third, due to the limited sample size, we were unable to divide the cohort into derivation and validation samples; however, we utilized bootstrapping as an alternate means of internally validating the risk score. Fourth, model overfitting is possible due to the limited sample size. Last, our cohort only included in-hospital AKI. As a result, our risk score may not apply to outpatient AKI.
Conclusions
In conclusion, kidney transplant patients admitted with AKI are at high risk for poor outcomes. Our prognostic risk score serves as a first step toward identifying transplant patients at the highest risk for graft loss. If validated, this predictive model will allow clinicians to identify high-risk patients who may benefit from closer follow-up or targeted enrollment in future intervention trials designed to improve outcomes.
Footnotes
Acknowledgements
This study was conducted at the Institute for Clinical Evaluative Sciences (ICES) Western and Ottawa Sites. ICES is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. Core funding for ICES Western is provided by the Academic Medical Organization of Southwestern Ontario (AMOSO), the Schulich School of Medicine and Dentistry (SSMD), Western University, and the Lawson Health Research Institute (LHRI). This project was conducted with members of the provincial ICES Kidney, Dialysis and Transplantation Research Program (![]() ), which receives programmatic grant funding from the Canadian Institutes of Health Research. Parts of this material are based on data and information compiled and provided by CIHI. The opinions, results, and conclusions are those of the authors and are independent from the funding sources. No endorsement by ICES, AMOSO, SSMD, LHRI, CIHI, or the Ministry of Health and Long Term Care (MOHLTC) is intended or should be inferred. Parts of this material are based on data and information provided by Cancer Care Ontario (CCO). The opinions, results, view, and conclusions reported in this article are those of the authors and do not necessarily reflect those of CCO. No endorsement by CCO is intended or should be inferred. Dr. Amit Garg is supported by the Dr. Adam Linton Chair in Kidney Health Analytics. Research personnel who worked on this project were supported by the Lilibeth Caberto Kidney Clinical Research Unit. Dr. Greg Knoll is supported by the University of Ottawa Chair in Clinical Transplantation Research. Dr. Carl van Walraven is supported by the University of Ottawa Department of Medicine. Dr. Amber Molnar received salary support from the KRESCENT Foundation and the University of Ottawa Department of Medicine.
), which receives programmatic grant funding from the Canadian Institutes of Health Research. Parts of this material are based on data and information compiled and provided by CIHI. The opinions, results, and conclusions are those of the authors and are independent from the funding sources. No endorsement by ICES, AMOSO, SSMD, LHRI, CIHI, or the Ministry of Health and Long Term Care (MOHLTC) is intended or should be inferred. Parts of this material are based on data and information provided by Cancer Care Ontario (CCO). The opinions, results, view, and conclusions reported in this article are those of the authors and do not necessarily reflect those of CCO. No endorsement by CCO is intended or should be inferred. Dr. Amit Garg is supported by the Dr. Adam Linton Chair in Kidney Health Analytics. Research personnel who worked on this project were supported by the Lilibeth Caberto Kidney Clinical Research Unit. Dr. Greg Knoll is supported by the University of Ottawa Chair in Clinical Transplantation Research. Dr. Carl van Walraven is supported by the University of Ottawa Department of Medicine. Dr. Amber Molnar received salary support from the KRESCENT Foundation and the University of Ottawa Department of Medicine.
List of Abbreviations
AKIN, Acute Kidney Injury Network; CHF, congestive heart failure; CORR, Canadian Organ Replacement Register; DAD, Discharge Abstract Database; eGFR, estimated glomerular filtration rate; OHDW, Ottawa Hospital Data Warehouse; ORRS, Ontario Renal Reporting System; RPDB, Registered Persons Database.
Ethics Approval and Consent to Participate
The study was conducted according to a prespecified protocol approved by the Ottawa Hospital Research Ethics Board.
Consent for Publication
Not applicable.
Availability of Data and Materials
The data sets supporting the conclusions of this article cannot be made publicly available due to privacy regulations and restrictions of the Institute for Clinical Evaluative Sciences.
Author Contributions
Research idea and study design: AOM, CvW, DF, AXG, GK; we thank Eric McArthur for his help with data acquisition and cleaning; data analysis/cleaning/interpretation: AOM, CvW, GK; statistical analysis: AOM, CvW; supervision or mentorship: CvW, DF, GK. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. AOM takes responsibility that this study has been reported honestly, accurately, and transparently; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Amit X Garg: Investigator initiated grant from Astellas Pharma and Roche to support a Canadian Institutes of Health Research study in living kidney donors, and his institution received unrestricted research funding unrelated to this project from Pfizer. All other authors have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Amber Molnar received salary support from the KRESCENT Foundation and the University of Ottawa Department of Medicine. Dr. Amit Garg is supported by the Dr. Adam Linton Chair in Kidney Health Analytics. Dr. Greg Knoll is supported by the University of Ottawa Chair in Clinical Transplantation Research. Dr. Carl van Walraven is supported by the University of Ottawa Department of Medicine.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.