
Abstract
Vascular access–related complications can lead to patient morbidity and reduced patient quality of life. Some of the common arteriovenous access complications include failure to mature, stenosis formation, and thrombosis.
Vascular access–related complications can lead to patient morbidity and reduced patient quality of life. An individual’s likelihood of developing various vascular access complications varies over time. 3 Some of the common arteriovenous access complications include failure to mature, stenosis formation, and thrombosis. Management and treatment of these complications are outlined below.
Arteriovenous Fistula Primary Failure
The definitions of fistula maturation and primary failure vary greatly in the literature. The definition usually relates to anatomical changes (size and flow), the ability to cannulate the fistula for hemodialysis, and whether interventions were required to promote maturation of the fistula. The period of follow-up is also an important component of the definition because longer follow-up reduces failure rates in slow to mature fistulas.
Clinical studies generally use more objective definitions of primary failure. For example, the National Institute of Health, NIH fistula maturation study 4 (see “Arteriovenous Access Selection and Evaluation Fistula Maturation” section) uses the primary outcome of unassisted clinical maturation, defined as fistula use with 2 needles for more than 75% of dialysis sessions over a continuous 4-week period and either (1) 4 consecutive sessions during the 4-week period in which 2 needles are used and the mean dialysis machine blood pump speed is greater than 300 mL/min, or (2) a measured single-pool Kt/V greater than 1.4 or urea reduction ratio greater than 70% during any session in which 2 needles are used within the 4-week period. The clinical maturation criteria can be satisfied at any time within 9 months of fistula creation surgery or within 8 weeks of dialysis therapy initiation, whichever comes later. This lengthy definition speaks to the complexities of defining fistula maturation in clinical research.
Definitions

The frequently cited study by Dember et al 5 defined fistula suitability as the ability to use the fistula for dialysis with 2 needles and maintain a dialysis machine blood flow rate adequate for optimal dialysis (≥300 mL/min) during 8 of 12 dialysis sessions occurring during a 30-day suitability ascertainment period. An alternate definition would be whether the fistula provided reliable enough use to avoid the use of a catheter. This is a much more objective definition (the patient either has a catheter in place or they do not), and catheter avoidance is the goal of fistula creation so it should be the measure of success. Regardless of the definition used, it is very important to understand exactly how maturation (lack of primary failure) was defined in studies when interpreting risks and counseling patients.
A good estimate of risk of fistula primary failure is reported in a meta-analysis by Al-Jaishi et al 6 examining fistula studies published in the year 2000 and later. This study defined primary failure as immediate failure of fistulae within 72 hours of surgery and early dialysis suitability failure, or late dialysis suitability failure based on definitions proposed by the North American Vascular Access Consortium.7,8 The overall risk of primary failure was 23% but increased to 37% in the elderly. The studies had a high degree of heterogeneity, however, reflecting the different definitions of primary failure.
Predictors of Primary Failure
Patient factors that predict primary failure include age, sex, race, diabetes, history of coronary artery disease, peripheral vascular disease, obesity, and location of the fistula.7-9 Lok et al 9 developed and validated a risk predication model for fistula failure that included patient age greater than or equal to 65 years, peripheral vascular disease, coronary artery disease, and race. The risk of primary failure was 69% in the highest risk category suggesting that the benefits of fistula creation are uncertain. However, caution should be exercised when applying risk models to specific patient populations as widespread applicability is limited. 10 Furthermore, surgical factors such as extent of surgical training, 11 the type of anesthesia during access creation, 12 and the anastomosis angle 13 may also impact primary failure rates (see “Impact of Primary Failure” section in MacRae et al 14 ).
Prevention of Fistula Primary Failure
Interventions for the prevention of primary failure include (1) health care process or team interventions, (2) medical interventions, (3) endovascular or surgical manipulations, and (4) device interventions.
Health care processes
Primary failure may be mitigated by vein preservation programs prior to access placement, although evidence for this strategy is lacking. Ontario and British Columbia have implemented “Save My Veins” and “Vein Preservation” (www.bcrenalagency.ca/resource-gallery/Documents/VeinPreservationRenalPatientsPPtFinalSept2012.pdf) programs, respectively, with the intent of preventing vein damage from venipuncture, intravenous cannulation, and peripherally inserted central catheters (PICC).
Not only are preoperative surgical factors becoming increasingly recognized as important for the successful maturation of fistula (as mentioned above), but standardized postoperative care may also play a role. Specifically, involvement of an experienced and interested surgeon may also prevent failure. For example, McLafferty et al 15 found that a surgeon-directed follow-up program detected 69% of fistulae with maturation problems and salvaged 83% of them for use.
The patient should also play a role in fistula maturation with careful protection of the fistula extremity from external trauma.
Medical interventions
There are currently no proven pharmacologic therapies to prevent primary failure of fistula. Clopidogrel was previously tested in a randomized trial and found to reduce the risk of early fistula thrombosis from 19.5% to 12.2% but did not increase overall suitability of the fistulas for hemodialysis. 5 However, a meta-analysis that included more than 3000 patients explored the role of antiplatelet agents around the time of fistula creation and found that access failure was significantly reduced in fistulas but not grafts. Most of the improvement occurs in the reduction in early thrombotic events. 7 A large multicenter trial is underway to determine the effect of fish oil either alone or in combination with aspirin to prevent primary failure (Australia New Zealand Clinical Trials Registry 12607000569404).
Exercise, either prior to surgery or after fistula creation, may play a role in promoting fistula maturation. However, the studies are generally small and despite showing improvements in vessel diameter with isometric exercise, this has not yet been shown to influence maturation fistula outcomes.16,17
Infrared therapy may upregulate nitric oxide synthesis and result in improved endothelial function and subsequent vascular dilation leading to improved fistula maturation. In a recent meta-analysis of 4 randomized trials including 666 patients with fistulas, the unassisted primary patency at 12 months after creation appears to be improved with infrared therapy (probability ratio for patency of 1.23, 95% confidence interval [CI], 1.12-1.35). 18
Management of Primary Failure
Endovascular or surgical manipulations
The main anatomic reasons for fistula nonmaturation are insufficient arterial inflow, insufficient venous dilation, and obstructions to the venous outflow tract. A particular common abnormality is juxta-anastomotic stenosis which develops after fistula creation in approximately 50% of newly created fistulas after 4 to 6 weeks of follow-up. 19 However, stenosis of the arterial anastomosis and draining veins, including cephalic arch stenosis, can also develop. Endovascular treatment of these lesions can facilitate maturation in many cases. For example, Beathard et al 20 reported 98% to 100% immediate technical success rates for angioplasty and eventual fistula use in 92% of their cases. Other procedures such as obliteration of collateral veins, elevation of fistula, and transposition of fistula can also facilitate maturation.
Future device interventions
Many other medical devices and therapeutic treatments are in development to reduce the risk of fistula failure caused by underlying stenosis. These include new types of anastomotic connectors, hybrid grafts, sirolimus- and paclitaxel-coated materials, and bioengineered vessels, all of which are designed to reduce stenosis formation. 21 The impact of these devices and therapies is unknown at present but are a clear sign of the efforts underway to reduce fistula failure.
Key Relevant Arteriovenous Access Patency Rates
Table 1 outlines the patency rates for grafts and fistulas.
Comparison of Fistula Versus Graft Survival.
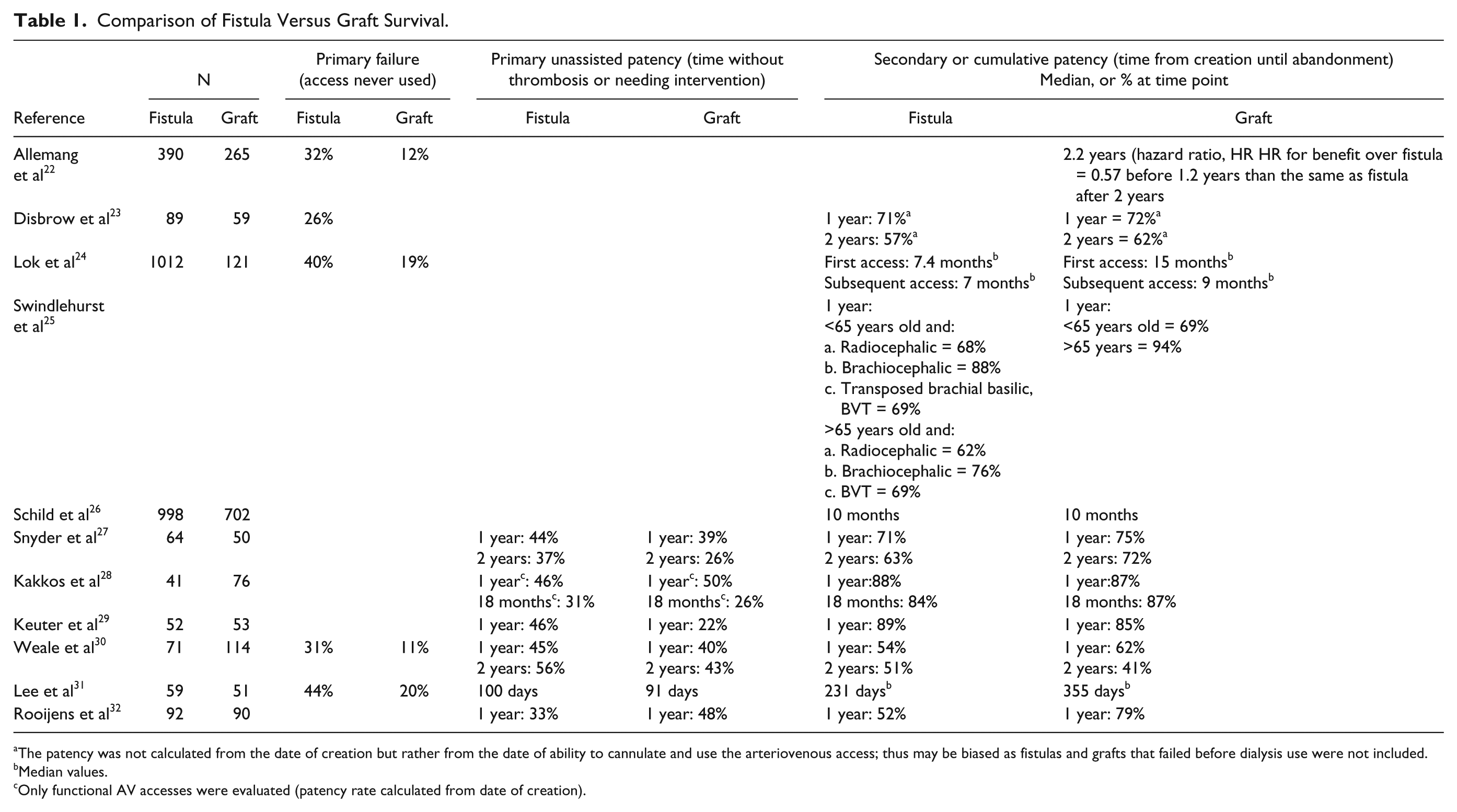
The patency was not calculated from the date of creation but rather from the date of ability to cannulate and use the arteriovenous access; thus may be biased as fistulas and grafts that failed before dialysis use were not included.
Median values.
Only functional AV accesses were evaluated (patency rate calculated from date of creation).
Arteriovenous Fistula
As indicated in Table 1, the primary failure rate of a fistula varies significantly in the literature, which leads to heterogeneity in published primary patency rates. In addition, the primary patency rates of fistula vary according to whether the primary failure rate is incorporated into the denominator and, in a 2014 meta-analysis, ranged from 60% at 1 year, 51% at 2 years (primary failure rate included) or 67% at 1 year and 51% at 2 years (excluding primary failure rate). 6 Secondary patency rates for fistula were much higher at 82% at 1 year and 73% at 2 years. 6
Arteriovenous Grafts
The primary failure rate for grafts is less than that for fistulas. However, given the increased number of interventions required for graft maintenance, the primary patency rate for grafts is less than that for fistulas. The secondary patency rates for grafts range widely in the literature from 57% at 1 year with standard polytetrafluoroethylene, PTFE 33 to 82% with a bovine mesenteric graft (excluding primary failure rate). 34 In general, PTFE forearm grafts have lower secondary patency as compared with upper arm grafts. 35
Summary
Primary failure is a common complication for fistulas; the reported rates vary widely in the literature.
Interventions aimed at reducing the risk of primary failure include promoting early vein preservation, consideration of antiplatelet agents to reduce early thrombosis, and intervention with endovascular or surgical techniques to facilitate maturation.
Grafts tend to have a lower primary failure rate than fistulas but a worse primary patency rate as compared with fistulas. Fistulas tend to have superior primary patency rates but equivalent secondary patency rates, compared with grafts.
Arteriovenous Access (Peripheral Vein) Stenosis
The development of peripheral vein stenosis is the primary cause of fistula and graft thrombosis. The formation of stenosis is initiated by endothelial cell injury which leads to smooth muscle proliferation and neointimal hyperplasia.36-38 The following factors may lead to endothelial injury: shear stress from turbulent blood flow,38-40 mechanical trauma from venipuncture, and angioplasties. 41 The most common site for stenosis in grafts occurs at the graft-vein anastomosis in 80% to 85% of the time followed by intragraft stenosis 11% to 15% and the graft-artery anastomosis 2% to 5% of the time. 42 Fistulas tend to develop stenosis most commonly either at the juxta-anastomotic site and the outflow vein (70%-85%). In the remaining 15% to 30% of the time, the lesion develops on the arterial site, which includes the feeding artery and anastomosis.
Clinical Features
In a newly created fistula, maturation failure and sometimes thrombosis occur as a result of an inflow or outflow stenosis. Venous stenosis may also be discovered during access flow surveillance whereby a decrease in the access flow from the usual baseline triggers an angiogram of the arteriovenous access. In some cases, the access may present with difficulty needling, prolonged bleeding times after dialysis, or elevated venous and arterial pressures. Depending on the site of the stenosis, the fistula may have physical exam findings43,44 as described in Table 2.
Physical Examination of Fistula.

Treatment Options
The treatment of choice for stenotic lesions of graft and fistula is percutaneous angioplasty. Randomized studies have not demonstrated that preemptive (elective) angioplasty of stenotic lesions improves graft survival.45,46 Despite this, many programs continue to treat graft stenosis, partly because so few grafts are utilized in Canada that it is easier to use the same surveillance protocols as for fistulas (see “Prevention: Role of arteriovenous access monitoring and surveillance” section). Furthermore, some believe that the elective treatment of graft stenosis decreases the need for catheter placement. Older studies demonstrated that surgical management has better patency than angioplasty but more recent endovascular studies suggest equivalent outcomes.
Percutaneous angioplasty
Percutaneous angioplasty has a 90% initial technical success rate for both graft and fistula stenosis. 47 The primary unassisted patency is worse for graft than fistula with 25% to 30% patency at 1 year for graft as compared with 67% patency for fistula. 6 The secondary (assisted) patency rates are similar for both graft and fistula at approximately 82% patency at 1 year and 70% patency at 2 years.6,8 The complication rate for angioplasty is approximately 4% with hematoma formation as the most common side effect followed by oxygen desaturation and reaction to medication. 47
Options for percutaneous angioplasty of recurring stenotic lesions
Angioplasty using high or ultrahigh pressure balloons has an improved immediate success rate (100%) 48 compared with standard pressure balloon (92%) 48 but higher risk of vein rupture. Angioplasty using a cutting balloon may increase the time to next intervention49,50 and may eliminate the need for the use of a high-pressure balloon. However, a recent randomized trial reported patency rates equivalent to those of conventional angioplasty, but greater risk of venous rupture and dissections with the use of a cutting balloon. 49
Angioplasty with a drug-eluting balloon provides an antiproliferative medication such as paclitaxel to the entire area of the stenosis. This technique may have a higher 6-month patency rates (70% vs 20%) using paclitaxel eluting balloon angioplasty as compared with standard balloon angioplasty; in 1 small randomized study. 51 At this time, longer term data are lacking, but a large randomized trial is underway. 52
Angioplasty using stents does not appear to improve the patency rate for AV access. The main types of stents used in dialysis vascular access include self-expandable stents, covered stents (stent grafts), or drug-eluting stents. Stent grafts are increasingly used for pseudoaneurysms or in areas that are to be cannulated. Stents are only recommended when the stenotic lesion has failed conventional angioplasty with a significant amount of recoil postplasty and if surgery is not an option. Stents are also used as a treatment for vessel rupture associated with angioplasty. Drug-eluting stents (sirolimus, paclitaxel, nitinol, and others) may reduce neointimal hyperplasia and improve patency.53,54 A meta-analysis of stent placement versus angioplasty in arteriovenous access 55 suggests that 6-month patency may be improved with nitinol as compared with bare metal stents although these findings are limited by significant heterogeneity and small sample size.
Concerns with using stents
The main concerns regarding the use of stents include possible vein depletion with reduced options for future surgeries, limited area of cannulation, stent migration or stent fracture, and intrastent thrombosis. 56 There are no guidelines or studies on the use of anticoagulation or antiplatelet agents as prophylaxis. Furthermore, the cost of stents is prohibitive in some programs.
Surgery
The surgical revision of peripheral stenosis generally provides results that are comparable 57 or better than angioplasty. Surgery, however, often cannot be provided as rapidly as a percutaneous approach and has the further disadvantage that it sometimes leads to a loss of a small portion of the vein. Surgery is best considered in resistant cases when percutaneous angioplasty is not successful or when the lesion is felt to not to be amenable to angioplasty (long lengths of stenosis or significant elastic recoil).
Summary
Peripheral venous stenosis is the most common cause of fistula and graft dysfunction and may lead to access thrombosis
First-line treatment of stenosis should be balloon angioplasty
Stent placement in the peripheral vein is generally not recommended except in special circumstances
Resistant lesions should be revised surgically when the lesion is not amenable to angioplasty (long lengths of stenosis or significant elastic recoil).
Arteriovenous Access Thrombosis
A fistula can thrombose either early or late after its creation. Early thrombosis of a fistula is most often due to an inflow problem (juxta-anastomosis stenosis or accessory vein) while late thrombosis tends to be due to an outflow stenosis. If either of these lesions is left untreated, this results in thrombosis of the fistula. There are 2 types of thrombosis that can occur: soft, friable clot that disintegrates and a firm fibrin plug. 58
Similar to fistulas, graft thrombosis is most often due to neointimal hyperplasia which forms stenosis and subsequent decrease in access flow and thrombosis. The most common lesion is juxta-anastomotic stenosis.
Systemic factors such as hypotension, higher hemoglobin target, 59 and hypercoagulabiity 60 result in increased risk of access thrombosis for both fistulas and grafts. Patient factors such as sex (female) and diabetes increase risk of fistula thrombosis as well. Thrombosis can be a complication of needling, with a 25% increased risk of thrombosis associated with hematoma from a needle complication. 61
Clinical Features
A history of recent onset of difficulty needling, a significant drop in access flow (>25% drop from baseline), a new onset of low access flow (<500 mL/min) or significant recirculation all may be clues to an impending fistula thrombosis. Often there is a history of increased venous and/or arterial pressures noted with a pump speed of 200 mL/min during the first few minutes of dialysis (pressure trend monitoring). Grafts, however, often present with no warning symptoms prior to thrombosis.
The physical examination of a thrombosed fistula or graft demonstrates a lack or a reduced thrill along with an absent or abnormal bruit. The anastamosis may be pulsatile. At times, fistula thrombosis may be confused with cellulitis due to erythema and tenderness at the site. The diagnosis of access thrombosis is usually made on clinical grounds but an ultrasound can confirm the presence of thrombus and a low flow state. Treatment should be initiated as soon as possible.
Treatment Options
Surgery
Surgery is an established technique for salvage of a thrombosed access. The surgical technique involves the use of a Fogarty thrombectomy combined with retrograde manual removal of clot. Initial success rates for surgical thrombectomy of arteriovenous access range from 70% to 94%62-64 with a 12-month patency rate that ranges from 68% to 88% for either fistula 62 or graft. 64 For patients who undergo surgical thrombectomy, a venogram with angioplasty of culprit lesions is always recommended; this may be one reason that many centers prefer an endovascular salvage of thrombosed fistula or graft. The identification and correction of underlying stenosis is an important part of postthrombosis care.
Ideally, both fistula and graft thrombosis should be treated within 48 hours in order to avoid placement of a catheter. Furthermore, older thrombi are adherent to the wall and very difficult to remove. Grafts can be salvaged up to 1 week after thrombosis, but fistulas have a shorter window of opportunity, typically 48 hours.
Endovascular intervention
An endovascular approach involves pharmacologically or mechanically disrupting and removing the thrombus, then correcting the underlying lesion. This typically involves infusion of a thrombolytic such as tissue plasminogen activator, tPA in conjunction with using a lacerating device or a balloon catheter to remove the clot. Following mechanical or pharmacologic thrombolysis, an angioplasty is done to correct any underlying stenosis.
An endovascular approach to thrombosed fistulas is associated with an 80% to 90% success rate and improved primary patency rates of 34% to 50% at 12 months.8,62,65 An endovascular approach to thrombosed graft is associated with an initial success rate of 73% with a primary patency rate of only 32% at 1 month. 66
Prevention: Role of arteriovenous access monitoring and surveillance
Physical examination and clinical monitoring and assessment are the keys to AV access maintenance and should be a part of the standard care of dialysis patients.15,67-71 Physical examination and clinical monitoring of the arteriovenous access should include an assessment at each dialysis treatment and include LOOK, LISTEN for bruit, and FEEL for thrill. Clinical findings that have been associated with arteriovenous access dysfunction include physical findings of persistent swelling of the arm, presence of collateral veins, prolonged bleeding after needle withdrawal, or altered characteristics of pulse or thrill in outflow vein or graft. 67 Any additional surveillance of arteriovenous access using technology is intended to supplement clinical monitoring.
The goal of clinical monitoring and access surveillance is to identify early access dysfunction and correct it with preemptive angioplasty or surgery prior to access thrombosis or loss. Access surveillance and management is an interdisciplinary team function. The patient, nephrologist, nephrology nurse, technician, interventional radiologist/nephrologist, surgeon, and primary care physician should all be participants of the team.
An ideal surveillance method should quickly, accurately, noninvasively, and economically evaluate access anatomy (eg, stenosis) and function. Measurement of dynamic venous pressure (DVP), measurement of access flow (Qa) and access recirculation, and duplex Doppler ultrasound (usually performed in radiology) are noninvasive methods of measuring the blood flow in the arteriovenous access and may be useful ancillary tests that can help confirm clinical suspicion of stenosis or access dysfunction. Access flow (Qa) and DVP are, however, surrogates for stenosis rather than direct measurements. Although these tests are associated with thrombosis, they lack the predictive accuracy needed to be the sole basis for intervention referrals. Thus, Qa and DVP should be emphasized as ancillary tests to be used in combination with information obtained from clinical monitoring. Duplex Doppler ultrasound has the advantage of directly visualizing stenosis while providing flow and velocity measurements that help determine the physiological significance of stenosis. Thus, duplex Doppler ultrasound may avoid inaccuracies inherent in surrogate measurements. However, the few available randomized controlled trials did not demonstrate improved outcomes in grafts when this form of monitoring was compared with either clinical 72 or access flow monitoring. 46
Access monitoring and surveillance detects underlying fistula and graft stenosis
An accurate physical exam (monitoring) combined with an access surveillance method (including lower access flows) can successfully reveal an underlying access stenosis, particularly when the stenosis is at the venous anastomosis. The duplex Doppler ultrasound accuracy for identifying stenosis was reported as 81% in fistulas, 73 with a sensitivity of 93% and specificity of 60%. 74 The accuracy for grafts has been reported as 86% for in-graft stenosis and 96% for outflow stenosis, 73 and a 100% sensitivity and 50% specificity using duplex ultrasound. 74
Access surveillance does not predict graft thrombosis
Access flow and DVP surveillance were both found to be inaccurate predictors of graft thrombosis.75-77 To date, there have been several randomized controlled trials that do not show any benefit of access flow surveillance as a means to improve graft survival,45,46,78 although the time to thrombosis may be reduced. For example, Ram et al 75 studied 176 patients who underwent a total of 1957 monthly Qa measurements over 6 years. They evaluated the accuracy of monthly Qa measurements, or percentage decrease in Qa, in predicting thrombosis within the next month. They found that Qa had a sensitivity of 74% and specificity 71% using a threshold of a flow less than 1200 mL/min and a decrease in flow by more than 20%. The mean Qa for grafts that did not thrombose over the next month was 1345 mL/min (range, 90-4000), and the mean Qa for grafts that did thrombose was 895 mL/min (range, 105-2115): values overlapped widely. Moreover, the majority of thromboses were not preceded by a decrease in Qa measurement, usually because thrombosis occurred before a second measurement could be taken.
Access surveillance reduces risk of fistula thrombosis and access loss
In a 2008 meta-analysis of 12 randomized studies of which 4 included fistula only, Tonelli et al 79 found that access flow surveillance of fistulas was associated with a significantly reduced relative risk of thrombosis (relative risk [RR], 0.47; 95% CI, 0.28-0.77) but not access loss (RR, 0.65; CI, 0.28-1.51).
A more recent meta-analysis 80 including 7 randomized studies in fistulas reported a similar reduction in access thrombosis (RR, 0.50; CI, 0.35-0.71) as well as access loss (RR, 0.50; CI, 0.29-0.86). The reduction in access loss is based on 4 studies72,81-83 of which 3 studies81-83 are from the same center. The preemptive correction of a stenosis in 1000 patients using a fistula will prevent thrombosis in 200 patients; however, this approach will lead to a significant increase in the number of radiologic interventions with an additional 234 fistulograms.
Guidelines
The 2006 National Kidney Foundation Kidney Disease Quality Outcomes Initiative, NKF-KDOQI guidelines 84 recommend surveillance of fistulas and grafts monthly for hemodynamically significant stenosis, when combined with correction of the anatomic stenosis, in the hope that this will improve patency rates and decrease the incidence of thrombosis. However, there is a growing body of evidence that surveillance with access flow measurements with subsequent angioplasty in the arteriovenous access with low blood flows may not improve access survival, is costly, and may even be harmfull.79,85-87 Future larger randomized trials are needed to determine the true benefits and potential harms of access flow surveillance. At this time, the frequency and the method of access surveillance are a subject of ongoing controversy.
Prevention: Role of antiplatelet and anticoagulation medication
Antiplatelet agents (aspirin, ticlopidine, and clopidogrel) have been studied for their role in prevention of fistula thrombosis; a recent meta-analysis 7 demonstrated a protective effect from early thrombosis and loss of patency in fistula but unclear effect on graft patency. There does not appear to be an increased risk in major bleeding events for single antiplatelet use. 7 The long-term effect of antiplatelet therapy on arteriovenous access patency remains unclear. Warfarin appears to have no role in the prevention of thrombosis. 88 Fish oil appears to have a protective role for graft thrombosis; the randomized trial by Lok et al 89 showed a 50% reduction in the number of thrombotic episodes (1.71 vs 3.41 per 1000 access days) as well as a reduced number of interventions required to maintain the graft (2.89 vs 4.92 per 1000 access days).
Summary
Access clinical monitoring using history and physical exam is the standard of practice for arteriovenous access.
Access surveillance involves the use of tools like dynamic or static venous pressure monitoring or access flow measurements.
Intervention based on surveillance does not prevent thrombosis or prolong survival in grafts but in fistulas leads to fewer thrombosis at the expense of increased interventions and does appear to prolong survival.
Thrombosed arteriovenous access is a medical emergency, and a salvage attempt should be made as soon as possible in order to avoid catheter placement and admission.
Central Vein Stenosis
Manifestations of central vein stenosis often become apparent when a patient has an ipsilateral access that drains into the side of the central vein stenosis. Signs of venous hypertension, with arm and hand swelling, dusky, rubor (red color) of the hand, and dilated veins on the arm and or chest wall are common. The development of central vein stenosis is thought to be related to a history of catheter 90 pacemaker91,92 or PICC insertion,93,94 but cases of central vein stenosis do occur in absence of these risk factors.
The treatment of choice for symptomatic central vein stenosis is percutaneous angioplasty, with long-term patency often requiring repeated interventions. 95 The role of stenting is not clear and should be reserved for lesions that have significant elastic recoil or for lesions that recur within 3 months of treatment. 84 Asymptomatic lesions do not require intervention and should be monitored (see “Management of Central Vein Stenosis” in Miller et al 96 ).
Footnotes
Acknowledgements
The authors thank Kirsten Campbell for her editing and management expertise and Adam Bass, Rob Quinn, and Pietro Ravani for reviewer expertise.
Ethics Approval and Consent to Participate
Ethics approval and consent to participate was not required for this trial.
Consent for Publication Availability
Consent for publication was obtained from all authors.
Availability of Data and Materials
There is no data to share.
Author Contributions
J.M.M. conceived, designed, and coordinated the review; drafted the manuscript; and critically revised the manuscript. C.D., M.O., L.M., C.L., E.C., S.H., M.K., J.K., and R.L. helped draft the manuscript and provided critical review. L.M.M. helped design and coordinate the review and provide critical review. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Vascular Access Work Group was supported by the Canadian Society of Nephrology through an unrestricted educational grant from Roche Pharmaceuticals, Canada.