
Abstract
Objectives
This qualitative study captured the perspectives of patients and healthcare professionals to better understand COVID-19 vaccine decision-making among South Asians in London.
Design
In-depth semi-structured telephone and virtual interviews were conducted using convenience and purposive sampling to explore narratives about COVID-19 decision-making processes, pandemic experiences, and perceptions of living through a period of unprecedented uncertainty and turbulence.
Setting
UK.
Participants
12 London-based individuals including patients, clinicians, and a medical receptionist.
Main Outcome Measures
Respondents were categorised as either COVID-19 vaccine compliant or non-compliant based on their vaccination status.
Results
The variation and dynamic nature of the vaccination trajectories described in this study suggest that the decision to vaccinate or not against COVID-19 comprises a fluid, continually evolving process shaped by personal experiences and ongoing risk assessments. This study examines the possibility that some individuals form an ‘epistemic community of uncertainty,’ influenced by the pervasive ‘infodemic’ surrounding COVID-19 vaccines, which has created substantial ambiguity about truth and trust, reminiscent of the Rashōmon effect. Developing a nuanced understanding of this effect in the context of the COVID-19 era is a critical step towards addressing such ambiguity and fostering deeper critical thinking about vaccine decision-making.
Conclusions
This research highlights the need for more flexible and innovative strategies to navigate the complex factors influencing decision-making. Furthermore, the study advocates for a more refined and discerning personalised approach to engagement, which is vital for improving scientific and health literacy within society and overcoming common barriers to making informed and autonomous choices.
Introduction
Shortly after the start of the UK COVID-19 vaccination programme in December 2020, literature emerged, highlighting the suboptimal uptake of vaccines among UK South Asians.1,2 Vaccine hesitancy is consistently identified as a major factor contributing to suboptimal vaccination uptake.3,4 A systematic review of UK evidence shows that lack of trust in authorities, concerns about vaccine safety, and the rampant spread of misinformation are the principal drivers behind vaccine hesitancy.1–6
This lack of trust stems from the perception that medical science rests on shaky ground, driven by heightened rhetoric and political polarisation, along with increasing concerns about conflicts of interest and scientific misconduct. 7 These concerns are further exacerbated by other key contributors to vaccine hesitancy, including apprehension about vaccine side effects, the rapid pace of their development, and anxieties surrounding potential effects on women's fertility.1,3,4 Some authors 8 argue, however, that the pandemic merely amplified pre-existing social anxieties and distrust, particularly those rooted in systemic racism and discrimination within healthcare systems, wherein the health and safety of the global majority are accorded lower priority by political and institutional leaders.3,4
Several writers have also argued that an overabundance of information that includes a mixture of truth as well as false or misleading information, circulating across digital and physical spaces has further complicated this hesitancy thus distorting perceptions of risks and benefit concerning COVID-19 vaccines.3,4,7,9,10 Such overwhelming volumes of information have the effect of leading to a multitude of conflicting and incomprehensible truths, reminiscent of the Rashōmon effect – where the same event is interpreted in significantly different ways from the perspectives of different people.11–14
While these arguments offer valuable insights, they remain limited in key respects.
One such limitation is in how context is framed. Much of the literature prioritises contextual factors such as ethnicity, while some authors duly highlight the role of education 15 and psychographics4,16 in shaping vaccine decision-making, and others point to gaps in knowledge – for example, why vaccine uptake in London remains lower than in other UK regions. 15 This approach can create the impression that such elements can be analysed in isolation or hierarchically ranked, rather than examined alongside one another and within the wider context in which they are entangled, and in this specific context, the COVID-19 era.
Another important limitation lies in the literature's repeated emphasis on vaccine hesitancy. This risks oversimplification, presenting South Asians as a homogenous group defined primarily by hesitancy – something that the ‘herd’ must ‘overcome’. Such framing often shifts attention towards uptake strategies2,17,18 while obscuring the broader decision-making landscape. As many authors acknowledge, decision-making is inherently multifaceted and complex.3,4 Vaccine hesitancy, therefore, only presents one aspect of the decision-making process.
A third limitation is evident in the way concerns about the sheer abundance of information in digital and physical environments are overshadowed by preoccupations with digital misinformation. This often obscures the complex ways individuals engage with both spaces. This emphasis also risks reducing individuals to passive bystanders, thereby overlooking their role as active agents. As Mirzoeff observes, digital algorithms continually feed us information that aligns with our existing beliefs, values, and biases. 19 In this sense, digital spaces, and by extension, physical environments, can resemble Rashōmon-like spheres, wherein individuals navigate fragmented and often contradictory realities.
Given that there is little discussion on the decision-making trajectories that have informed COVID-19 vaccine uptake or refusal among UK South Asians, this qualitative study explores the decision-making processes of South Asian individuals thus allowing for a more flexible and inclusive understanding of the factors shaping individual choices. Investigating how these dynamics unfold in the context of COVID-19 vaccination can inform new communication and policy strategies, helping to build stronger, more trusting relationships between individuals and the healthcare sector worldwide and across communities.
Method
Study design
To explore COVID-19 vaccine decision-making among British South Asian individuals, we designed a qualitative study using 12 in-depth interviews conducted between July 29 and November 02, 2021.
Seven participants were registered at an NHS general practice in Southall during the study period. One participant also worked as a receptionist at the same practice. Southall, located in the Borough of Ealing, has well-established South Asian communities.
The study additionally included four healthcare professionals. Among the participants, 11 were from Indian, Pakistani, and Afghani backgrounds, while one of the health professionals identified as White British.
Participant recruitment and sample
The sample was recruited using a combination of convenience and purposive sampling methods. For the latter, the study was advertised to all patients at the general practice through text messages containing a web link outlining the project. This outreach did not initially involve checking whether individuals had been vaccinated or not against COVID-19. This approach carried a significant ethical advantage, as it enabled us to respect the privacy of participants during recruitment. Simultaneously, it increased the likelihood of investigating individuals exhibiting diverse vaccination decisions.
Prospective participants were able to contact the researcher via email, telephone, text message, or a ‘walk-in’ service at the general practice, which helped facilitate rapport building. Healthcare professionals were selected through convenience sampling, targeting individuals with extensive experience treating South Asian patients and direct involvement in addressing COVID-19 vaccine hesitancy within South Asian communities. A clinical fellow and three General Practitioners (GPs) agreed to participate in an interview, with the latter being known to the lead GP Partner at the general practice in Southall.
As this project was part of a quality improvement initiative aimed at advancing an understanding of decision-making processes related to COVID-19 vaccination, it was approved by an internal review board comprising members of the general practice team in Southall. Notably, the project did not require NHS ethics approval, aligning with guidance from the NHS Health Research Agency.
Data collection and analysis
COVID-19 vaccination is a highly polarising, emotionally charged, and potentially stigmatising topic. 20 To facilitate open and candid discussions, private interviews were conducted with the researcher, who had no prior relationship with the participants. These semi-structured interviews were conducted either by telephone or via Zoom (see Appendix). The interviews, lasting between 30 and 90 minutes, were recorded in audio or video format, following explicit consent from participants. Subsequently, the recordings were transcribed and anonymised.
We analysed the data using thematic analysis to identify and categorise the main themes and recurring patterns. 21 The themes used to establish our findings are the contextual challenges influencing COVID-19 decision-making (Table 1); and the driving factor(s) influencing COVID-19 vaccine decision-making processes (Table 2).
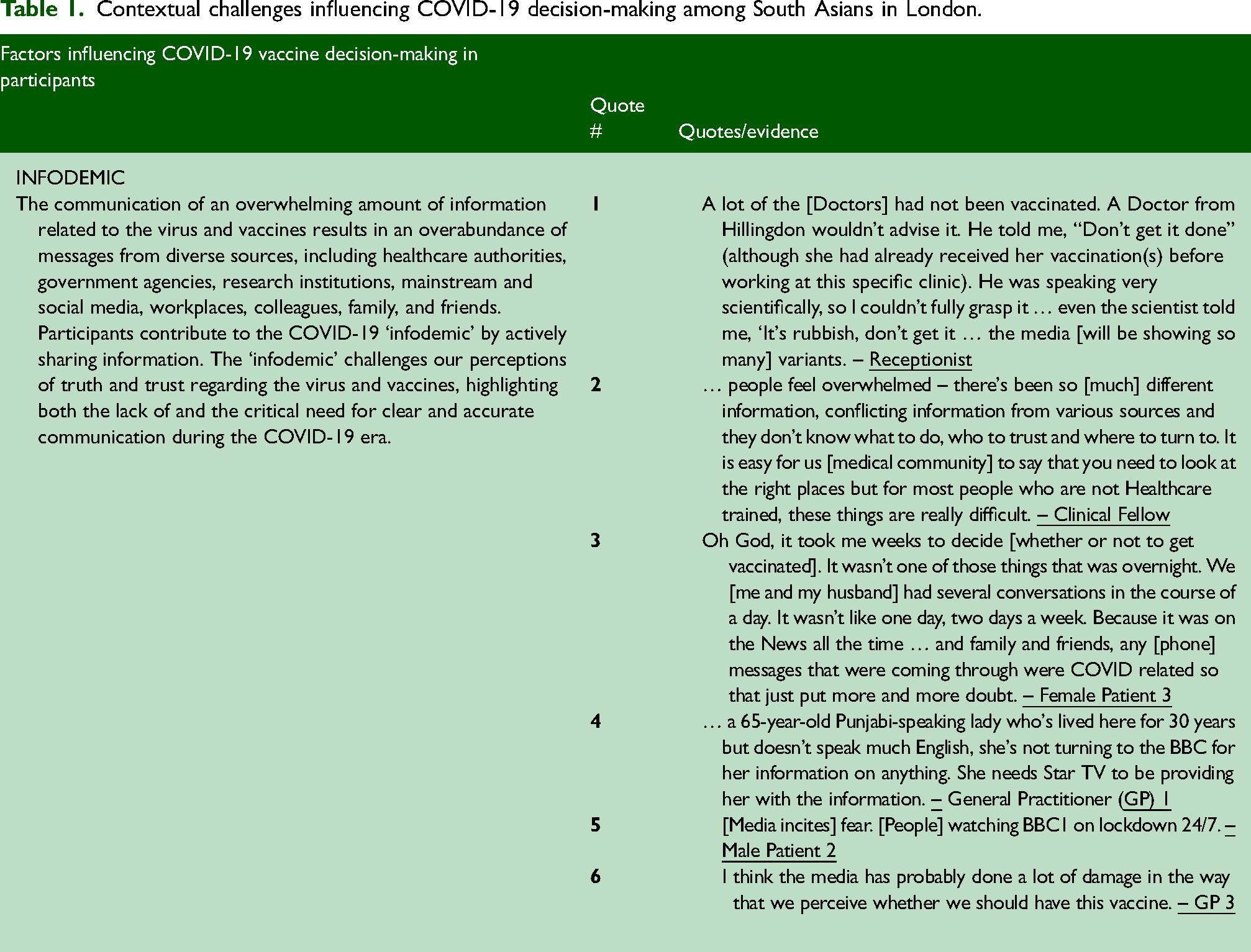
Contextual challenges influencing COVID-19 decision-making among South Asians in London.
Driving factors influencing COVID-19 decision-making among South Asians in London.

Results
Our findings indicate that COVID-19 vaccine decision-making is not a straightforward binary process. 22 Rather, it reflects a spectrum of ‘complex multifaceted decisions taken along a continuum’, 23 emphasising the nuanced nature of these decisions.
Before COVID-19, all participants appeared to have an unproblematic relationship with vaccines; thus, highlighting that their concerns, apprehensions, and queries were specific to COVID-19 vaccines and the overall COVID-19 vaccination rollout programme. 4 Therefore, our participants’ decision to comply or not to comply with COVID-19 vaccination inherently warrants examination, as this choice cannot be disentangled from the broader, ongoing experience of the pandemic and its consequent impact on their lives. 22
We use the terms COVID-19 vaccine compliant and COVID-19 vaccine non-compliant to characterise and differentiate our respondents based on their decision to vaccinate or not vaccinate against COVID-19 (except for the healthcare professionals who had all been vaccinated, without any equivocation or reservation). The COVID-19 vaccine compliant group comprised five individuals, four patients and a receptionist, each of whom had received two doses. The COVID-19 vaccine non-compliant group included three participants who had not received the vaccine. This choice was not an absolute or permanent refusal but a time-dependent decision shaped by emerging information and changing circumstances.
Discussion
Statement of principle findings
This study aimed to explore the decision-making process concerning COVID-19 vaccination in a diverse group of South Asian individuals. A core finding was the ambiguity around truth and trust, both of which played a fundamental role in preventing the participants from arriving at a rational, balanced, well-founded, and informed decision about whether to vaccinate against COVID-19.
In the context of the COVID-19 pandemic, our participants’ narratives disclose a complex reality characterised by conflict, evolving choice, decision criteria, and triggers, indicating a trajectory towards closure while inviting further inquiry into the interplay of truth and trust. These five features – context, complexity, conflict, choice, and closure mirror the features of the Rashōmon effect,11,24,25 and it is for this reason that we used the Rashōmon effect as a guide to illustrate our findings (see infographic).
The film, Rashōmon, as Anderson observes,11,24 depicts two instances of the Rashōmon effect. The first instance is grounded in the context of a compelling situation that centres on the murder of a samurai and the conflicting yet convincing accounts of the four witnesses.11,24,26 Such an environment inevitably becomes an ideal breeding ground for undermining the concept of a singular objective truth.
The second instance of the Rashōmon effect, places the onus on the film's audience to ‘work through’ the different interpretations offered by the four witnesses. The differing perspectives gain their significance precisely because of the lack of evidence to either support or discredit any version of the truth. This effect is further intensified when interests, culture, and power intersect – creating a demand for immediate explanations as well as a strong drive towards closure. 11
In the era of COVID-19, the first occurrence of the Rashōmon effect is characterised by the onset of the pandemic – our ‘once-in-a-lifetime’ health crisis – and thus, represents a unique and unprecedented experience. The profound changes COVID-19 introduced into every aspect of life, combined with the novelty and uncertainty of the pandemic, created fertile ground for questioning the truth about the virus and the vaccines.
All our participants felt overwhelmed by the continuous stream of information related to the virus and vaccines. This information overload ('infodemic') came from diverse sources, including healthcare authorities, government, research institutions, mainstream media, social media, work, colleagues, family and friends, as well as our participants, who played an active role in the COVID-19 ‘infodemic;’ actively sharing ‘news’ about the virus and vaccines with others, especially through instant messaging services like WhatsApp, and social media platforms such as Instagram and TikTok, among others. The sheer volume of information as experienced by our participants resulted in a landscape flooded with incomplete, confusing, and contradictory messages (#1–6).
In turn, and as the second instance of the COVID-19 Rashōmon effect reveals, the effects of the first instance (the ‘infodemic’), combined with other contextual factors, culminated in multiple plausible but conflicting decision criteria about the vaccines among our participants. This, in turn, produced multiple subjective realities and decisions, making a single objective truth incomprehensible.
As our findings illustrate, two participants (female patients 2 and 3) detailed their decision-making process within the framework of ‘I weighed things up’ (#7–8). Their decisions however were also influenced by all the information and opinions they had and continued to consume, including that of their workplace where they described the vaccines as being ‘pushed’. Both participants, upon reflection, would have taken more time in the decision-making process if their workplaces had not exerted so much pressure.
Also worth noting is that such events signal coercive methods being exercised whereby not only may people's livelihoods be threatened but equally, individuals are denied an avenue for autonomous decision making. One of the participants (the receptionist) for example, while she personally disagreed with the vaccine, coercive tactics exerted by her previous employer at an elderly care home led her to take the COVID-19 vaccine (#9). While COVID-19 vaccination was briefly mandated for care home staff, this requirement was later rescinded by the government. 27
The Rashōmon effect illustrates how dialogue and negotiation operate within a dialectical process, where different perspectives coupled with power dynamics interact and shape meaning. 11 Individuals may contemplate choices more or less in solitude, and yet, the decisions made are also influenced (and sometimes forced upon) by the dialogue that has been established socially (ibid: 74). It is, therefore, reasonable to consider the extent to which closure is attainable and what it might look like.
Against this complex interplay of truth and trust, conflict and choice operate simultaneously side by side (#10 and #13). Given that their simultaneous existence can remain ongoing and unresolved, our study like others, therefore demonstrates that individual perspectives on vaccination are neither permanent nor monolithic.22,28 As the Rashōmon effect illustrates, decisions are made within the quagmire of the inherently ambiguous and uncertain nature of a particular situation, in this case, the COVID-19 era. According to Anderson, 11 individuals involved in this complex set of processes form ‘a kind of epistemic community of uncertainty’ that is unique to the specific time and context in which it is experienced. Amid this backdrop of uncertainty, where decisions continue to be made, our findings suggest that such decisions may generate unintended consequences, giving rise to new, unanticipated, and competing truths.
In the case of all five respondents who initially chose to be vaccinated, all reported being unlikely to take a booster dose. Three participants cited ongoing side effects as their main reason, and all expressed reluctance to face the question again: ‘to vax or not to vax’. This suggests that the participants’ need to prioritise autonomy and place greater trust in their own lived experience increasingly took precedence over any previous or existing ‘truth(s)’.
Two of our participants, (Male Patients 2 and 3) chose not to be vaccinated due to deep distrust (#11–12); this led them to engage in extensive research, leaving them confident that they had found sources supporting their stance against the dominant discourse. This also raises questions about information-seeking behaviour – for instance, whether individuals search for information in pursuit of truth, to confirm their existing beliefs, or perhaps a combination of both.
One participant, GP 3, had not anticipated that his experiences during COVID-19 would force him to confront difficult questions about his career. Although he supported vaccinations, he disagreed with the pressure placed on individuals, a conflict that caused moral distress and prompted him to reconsider his relationship with the NHS – including the possibility of early retirement.
Our findings demonstrate that the Rashōmon effect challenges us to critically examine how we might effectively navigate and articulate the profound ambiguities introduced by the pandemic, ambiguities that reach far beyond questions of safety and vaccine efficacy, touching upon the very nature of our shared – and, at times, divided – reality.
Strengths and weaknesses of the study
To the best of our knowledge, this is the first study to apply the Rashōmon effect as a guiding framework. Although it focused specifically on the perspectives of UK South Asians, the framework can be applied more broadly to decision-making processes across diverse groups and contexts. The Rashōmon effect captures a universal human condition, cutting across ‘races’, cultures, and perspectives, thus promoting a more inclusive understanding of the pandemic and vaccine decision-making. 29
Given the sampling and data collection methods used, these qualitative findings cannot be generalised to broader contexts in this developing and exploratory field.
Strengths and weaknesses in relation to other studies, discussing particularly any differences in results
This was a small, detailed study. While medical sciences are often seen as seeking ‘black-and-white’ explanations for complex phenomena, the Rashōmon effect highlights that some situations demand a more nuanced appreciation of ambiguity. 30 As illustrated in this study, embracing ambiguity through the Rashōmon effect fosters openness and supports flexible, creative approaches to addressing novel circumstances.
Meaning of the study: Possible mechanisms and implications for clinicians or policymakers
Promoting critical thinking and science literacy to enhance impact and help overcome common barriers to informed, autonomous decision-making is particularly important for COVID-19 vaccination and other multi-dose vaccines, where sustained public understanding and engagement are vital. 22 In a world where social media and AI are deeply embedded in daily life and strongly influence knowledge formation, strengthening health and science literacy is essential.
Unanswered questions and future research
British institutions and social media companies encouraged individuals to add frames, graphics, and stickers such as ‘I’ve had my COVID vaccination’ and ‘I’ll get my COVID vaccine’ to their profiles. This illustrates that authorities recognise the importance and influence of visual markers. Yet, while engaging, these markers risk obscuring the diversity and complexity of lived experiences. Future research should examine how such tools might not only enhance understandings of health but also cultivate critical reflection. Approaches of this nature humanise experiences and demonstrate ongoing care and respect for individuals’ varied realities.
Supplemental Material
sj-pdf-1-shr-10.1177_20542704251408587 - Supplemental material for The Rashōmon Effect and COVID-19 vaccine decision-making: A qualitative study
Supplemental material, sj-pdf-1-shr-10.1177_20542704251408587 for The Rashōmon Effect and COVID-19 vaccine decision-making: A qualitative study by Poonam Madar, Raj S. Chandok and Azeem Majeed in JRSM Open
Footnotes
Declarations of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The practice team at the general practice approved our interviews. The project did not require NHS ethics approval, in line with guidance from the NHS Health Research Agency. Participants gave written consent before interviews.
Contributorship
RSC conceived the research idea. PM carried out the interviews. PM and RSC analysed the data. PM drafted the paper. RSC helped to draft and revise the paper. AM reviewed and edited the manuscript. All authors revised the paper and approved the final version.
Acknowledgements
The authors would like to thank all the participants who took part in this study. Azeem Majeed is supported by the NIHR Applied Research Collaboration NW London. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Provenance
Not commissioned: peer reviewed by Josefina Nunez Sahr and Julie Morris
Supplemental material
Supplemental material for this article is available online.
Appendix: Semi-structured interview guide

| Date: | Interviewer: | Participant: |
| Interview Medium: Zoom / Telephone | Start Time: | End Time: |
Re-introduce yourself (noting that you have previously introduced yourself via email) Thank the participant for their time and for agreeing to be part of the interview Remind the participant of the consent process and confidentiality parameters; including: - Participation is voluntary - Participants can skip any question - Participants can take a break and / or stop the interview at any time. As whether the participant has any questions before you begin. |
||
Tell me a little about yourself; your background, your work, and what you do. How has the pandemic affected you personally and / or professionally? Encourage participants to consider how the situation has evolved over time. What is your general outlook on the COVID-19 vaccine rollout? |
||
Ask the participant to confirm their COVID-19 vaccination status. How did you go about making the decision to vaccinate—or not to vaccinate? Can you walk me through the process of making that decision? (If and when appropriate), encourage participants to discuss: - Key moments that influenced their choices - Their attitudes towards COVID-19 vaccination - Concerns, thoughts, or uncertainties they experienced - Motives and goals underlying their decisions - Direct and indirect experiences with vaccination - Social norms influencing their decision-making process - Relationships or interactions with colleagues, family, friends, and / or community members Trust in information sources Risk assessment and management regarding vaccination, risk management, and communication with others about COVID-19 vaccination. |
||
What impact has the pandemic and the subsequent lockdown had on your mental health? What has been the most challenging aspect of the pandemic for you? Have there been any unexpected benefits or positive surprises during this time? - Encourage participants to share any observations they have made about themselves. |
||
Would you like to ask me any questions—about the research or anything else? Do you have any additional thoughts that you would like to share? |
||
Thank the participant again for their time and contribution. Remind the participant that they are welcome to contact you via email should they have any questions about the research. |
||
Only prompt / probe and / or ask participants for examples when deemed appropriate Avoid leading questions, be consistent in active listening, and follow up on emotional cues. |
||
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.