
Abstract
Lesson
Intra-ocular corticosteroids have the potential to cause adrenal insufficiency when used long term. Patients and clinicians should be counselled on the risks of long-term steroid use and consider appropriate monitoring.
Corticosteroids are widely used in the management of a variety of medical conditions, from autoimmune and inflammatory, to malignancies and after organ transplantation. The main mechanism of action of corticosteroids, making them so widely used, is through their anti-inflammatory and immunosuppressive properties. 1
Though beneficial in numerous ways, it is widely researched and documented that the chronic use of exogenous glucocorticoids has the potential to lead to the suppression of the hypothalamic-pituitary-adrenal (HPA) axis due to negative feedback, with no substantive correlation with dose of steroid or duration of treatment. 2 Though topical administration of corticosteroids is deemed to be safer than the oral or parenteral routes, there is still a risk of adrenal insufficiency (AI) with prolonged use due to systemic absorption. 3 This case report discusses an incidence of adrenal insufficiency following the prolonged use of corticosteroid eye drops.
Case
A young boy had been diagnosed at birth with bilateral Peter's anomaly - a condition characterised by central, paracentral, or complete corneal opacities, congenital glaucoma, iridocorneal adhesions and cataracts. 4 He had been treated with glaucoma tube implant surgery, bilateral penetrating keratoplasties (full thickness corneal transplants), and dexamethasone 0.1% eye drops twice daily for prevention of rejection.
By the age of 9, he presented with cushingoid features and symptoms of possible adrenal insufficiency. As a possible precipitant for his symptoms, his daily dexamethasone eye drops were therefore held for 1 week. During this time, his parents were educated on the possibility of developing adrenal crisis and sent home with an emergency hydrocortisone supply. The following week a short synacthen test was arranged which demonstrated a suppressed corticosteroid response of serum cortisol <10 at 0, 30 and 60 min. Additionally, his ACTH level was <5 (ref 7.2–63.3 ng/L) and demonstrated negative adrenal antibodies. Subsequent assessments of the HPA axis have demonstrated complete adrenal suppression.
Due to the need to continue dexamethasone eye drops for his chronic ophthalmic condition, he is concurrently treated with hydrocortisone replacement therapy to manage his adrenal insufficiency.
Discussion
Secondary adrenal insufficiency is a widely proven yet under-recognised complication of most forms of long-term glucocorticoid therapy. Adrenal suppression can often present asymptomatically or with non-specific symptoms, and a high clinical suspicion is needed to make the appropriate diagnoses. Undiagnosed AI can have serious consequences, and is associated with significant morbidity, including poor response to illness, hypoglycaemic seizure, coma and even death following adrenal crisis.
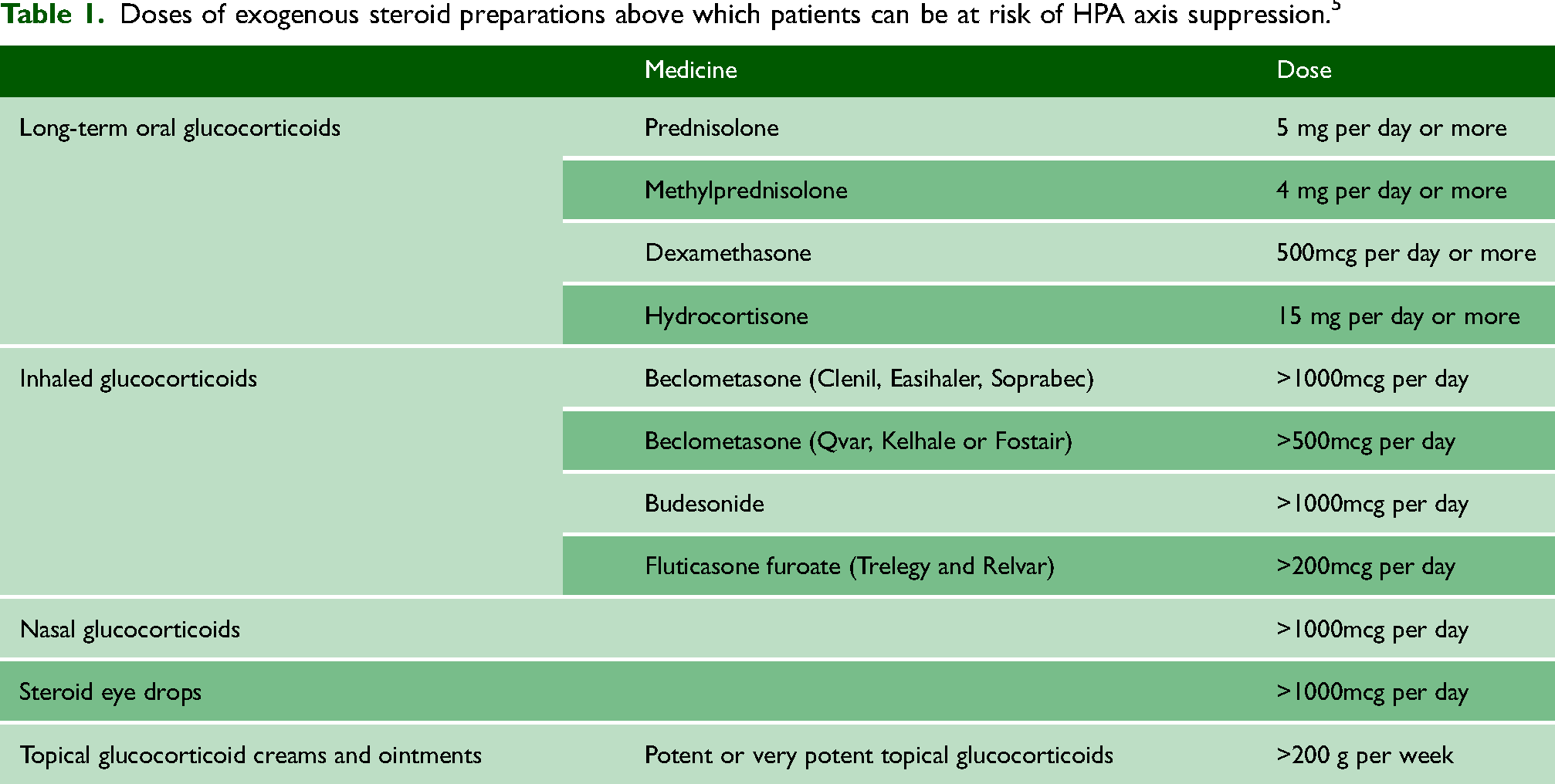
The development of adrenal insufficiency following intra-ocular steroid treatment is rare and unusual. The Society for Endocrinology guidance suggests an indicative threshold of 1000 micrograms per day, and they reason that this dose limit would be very unlikely to be reached with available steroid eye drops, and therefore HPA axis suppression would be unlikely. 5 The current research available on this topic provides mixed results, with no conclusive association between ophthalmic corticosteroid use and adrenal suppression.
A study analysing the incidence of HPA axis suppression in infants with the use of steroid eye drops after surgery found that they were at risk of receiving high dose steroids per weight by topical ocular administration. 6 Another similar study analysing incidence of AI in infants treated with steroid eye drops following cataract surgery found that two thirds of the infants showed evidence of adrenal suppression, with there being a correlation between cumulative daily dose of steroid and the test result. 7
On the contrary, a study by Sandhu et al. sought to establish whether HPA axis suppression is possible following long-term topical ophthalmic corticosteroid use in patients who have undergone penetrating keratoplasty (PKP) suggests there is no evidence that long-term low dose use of corticosteroid eye drops to prevent graft rejection causes adrenal suppression in adults. 8 The study acknowledges that many conditions require higher strengths of corticosteroids and therefore those patients may be more at risk of AI, especially if used in combination with systemic steroids (Table 1).
Doses of exogenous steroid preparations above which patients can be at risk of HPA axis suppression. 5
Many conditions require the use of corticosteroids and hence their use in medical treatment is often unavoidable. However, measures can be put in place to minimise the adverse effects of their use. When commencing patients on exogenous corticosteroids, potential risk factors that could potentiate AI should be identified, such as physical stressors, dose and duration of steroid use, and warning of sudden cessation of treatment. Particularly in infants and children frequent monitoring for adverse effects is advised, with follow up including growth charts, BMI tracking, and cortisol tests. 9
Clinicians should aim to achieve the lowest effective dose for treatment and regularly review the need for continuation of treatment. There is some evidence that opting for alternate day steroid prescribing could result in lower risk of AI. Similarly, using multiple doses throughout the day or nightly doses may result in greater adrenal suppression as this counters the body's natural cortisol rhythm.
Most importantly, patient and family education are key. They should be educated regarding the risks of long-term steroid use, to be aware of signs and symptoms of adrenal suppression and actions if AI is suspected. They should be reassured that though these risks exist, this should not be a barrier to continuation of treatment, and that appropriate medication adherence and regular follow-up are advised to monitor for any adverse effects. Patients should carry their steroid treatment card in case of emergency, be educated on stress dosing and when and how to administer intramuscular hydrocortisone in the instance of severe illness or adrenal crisis.
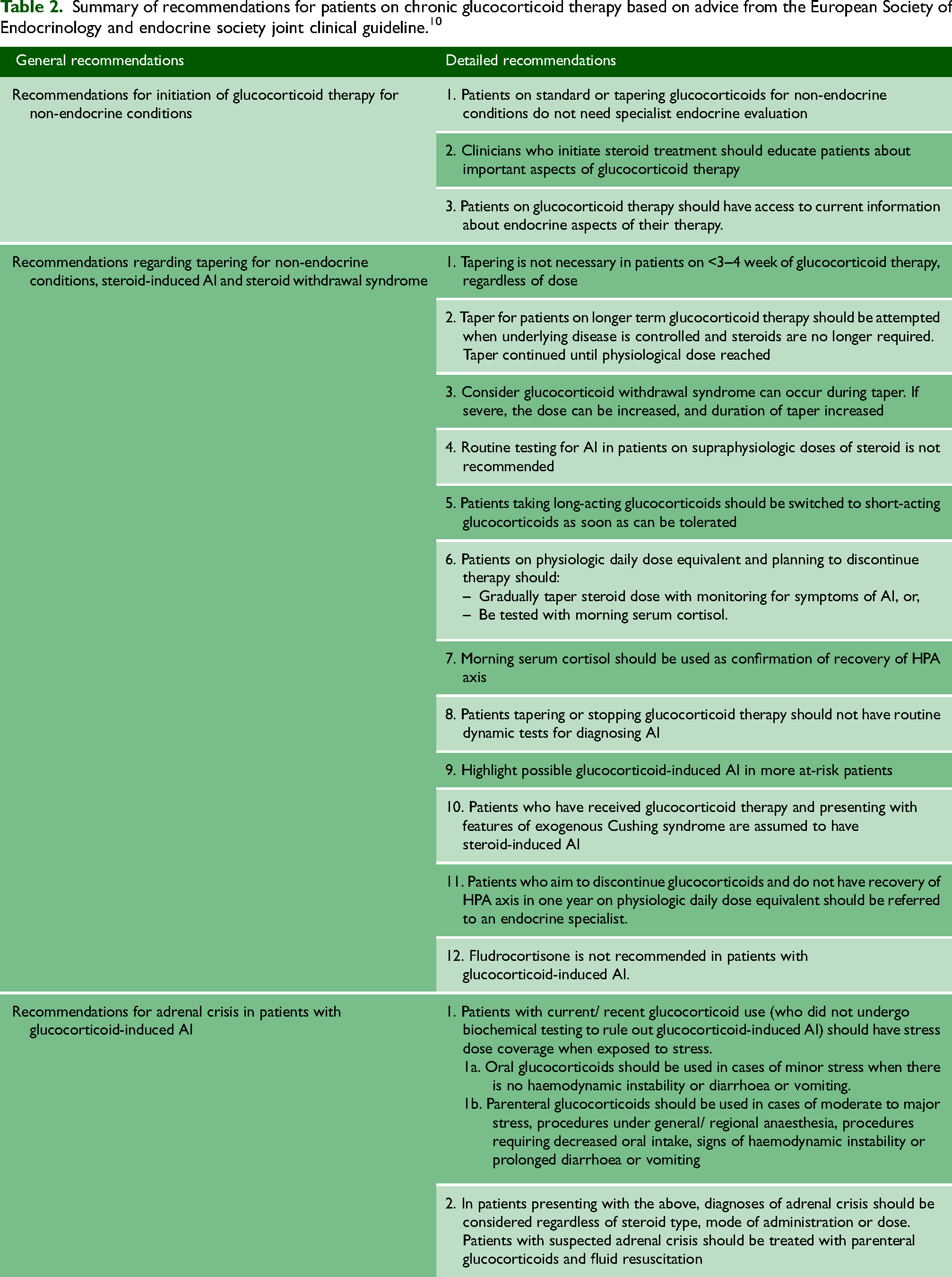
The European Society for Endocrinology and Endocrine Society have outlined recommendations for patients on long-term glucocorticoid therapy, reinforcing the importance of patient education, advice for the approach to steroid-tapering, and when to refer to endocrine specialists. They also highlight the current guidance on diagnosing with morning serum cortisol levels, and treatment options of adrenal crisis in patients with steroid induced AI. 10 These recommendations are further summarised in Table 2.
Summary of recommendations for patients on chronic glucocorticoid therapy based on advice from the European Society of Endocrinology and endocrine society joint clinical guideline. 10
Conclusion
Secondary adrenal insufficiency induced by intra-ocular corticosteroid eye drops, although rare, is an important cause of AI that should be assessed and investigated appropriately. Clinicians and patients should be educated on the potential adverse effects of long-term steroid treatment, how to reduce risks of this and when to seek prompt medical attention. The recommendations in this review are applicable to a wide range of specialties and AI is a pertinent and clinically relevant condition to consider in the ever-growing landscape of exogenous steroid treatment, regardless of therapy route. Though there is a risk of adrenal suppression with the use of corticosteroids, for many conditions this constitutes necessary treatment, and should not be a hindrance to their continued use.
Footnotes
Competing interests
None declared
Funding
None declared
Ethical approval
Ethical board approval was not required. Written informed consent for publication was obtained from the patient's father.
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by George Iype Varughese.