
Abstract
Awareness of the various clinical manifestations and diagnostic pitfalls in patients with atrio-oesophageal fistula is necessary among healthcare professionals.
Case report
A 58-year-old male was hospitalised because of increasing dyspnoea since 2 weeks, shivers, fever, dry cough and haemoptysis since 3 days (Figure 1). Because of paroxysmal atrial fibrillation (AF), four pulmonary vein ablations had been carried out during the past 4 years. The latest procedure was a radiofrequency circumferential right pulmonary vein ablation because of reconnection, which had been carried out 19 days before hospital admission. A two-chamber pacemaker had been implanted 3 years previously because of bradycardia. He was on a chronic medication with rivaroxaban 20 mg/d and pantoprazole 40 mg/d. Because of the recent pulmonary vein ablation, the emergency physician considered atrio-oesophageal fistula (AOF) as potential cause of the symptoms and chest computed tomography (CT) was carried out immediately after hospital admission. CT showed no signs of AOF but pulmonary ground-glass opacities. Blood tests showed 17.2 leukocytes (reference value 4.0–10.0), 29.41 mg/dl C-reactive protein (reference value <5), 1502 pg/ml interleukin-6 (reference value <7), 1.45 ng/ml procalcitonin (reference value <0.50) and 24.00 ng/L troponin T-hs (reference value <14.00). Based on the CT findings, the differential diagnosis of AOF was dismissed. The patient was isolated because of suspected Coronavirus disease 2019 (COVID-19) infection, awaiting the results of polymerase chain reaction (PCR) testing. Blood cultures were obtained and an antibiotic therapy with ceftriaxone was started.
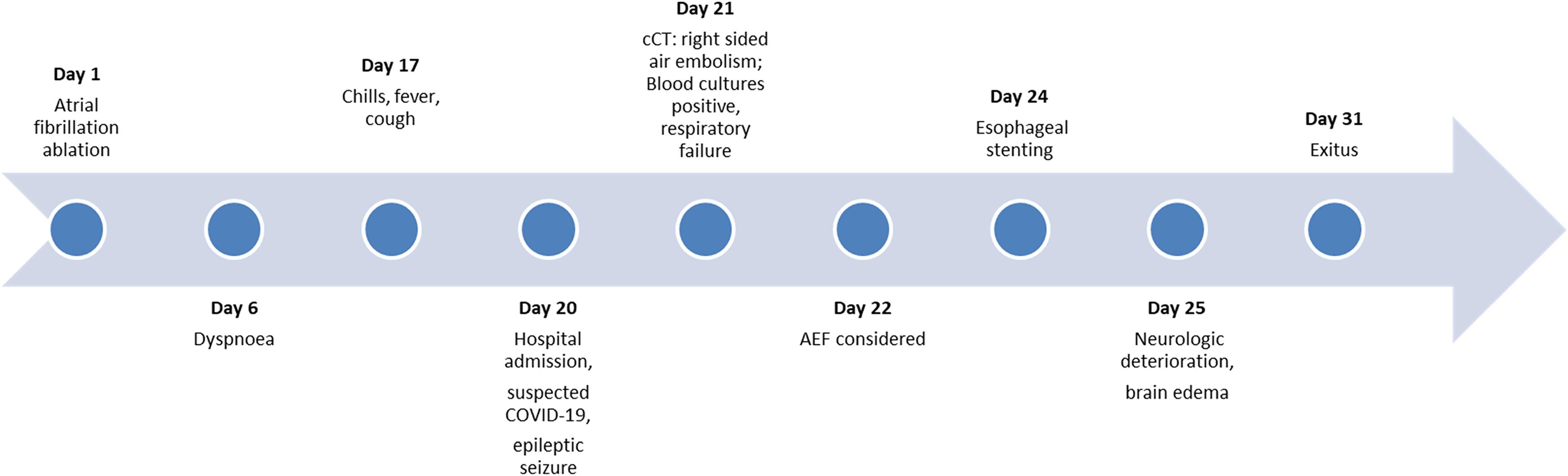
Time course of the presented patient.
During the following hours, the fever regressed but the awareness of the initially alert patient deteriorated. Urine loss was observed and raised the suspicion of an unwitnessed seizure. Neurological investigation revealed left upper and lower limb hemiparesis, facial paralysis, urinary incontinence and tongue bite. An epileptic seizure, cerebral ischaemia or bleeding was suspected. Cerebral CT was inconclusive. However, intravenous levetiracetam was started. The COVID-19 PCR test was negative. Blood cultures were positive for Streptococcus anginosus and Streptococcus oralis.
The alertness deteriorated further, the patient was intubated because of respiratory failure and transferred to the intensive care unit. Because of suspected endocarditis, transesophageal echocardiography (TEE) was carried out. A second cerebral CT now showed bilateral ischaemic lesions and air embolism. Based on these findings, the diagnosis of AOF was reconsidered and substantiated by the incidental CT findings of air in the spleen and abdominal fat.
Endoscopically, the fistula measured 8 mm and was closed by an over the scope clip (OTSC). A partial covered oesophageal stent was implanted and fixed by an additional OTSC. In the following days, the neurological situation deteriorated continuously, cerebral oedema increased (Figure 2) and the patient died 31 days after AF ablation.

Cerebral computed tomography 1 week before death showed air embolism in the right occipital area, multiple ischaemic lesions, few blood deposits and diffuse cerebral oedema with compression of the ventricles.
Discussion
We report a patient with AOF whose initial negative CT findings lead to the erroneous suspicion of COVID-19 and to a fatal outcome because of massive cerebral air embolism.
AOF is a rare but life-threatening complication after AF ablation which occurs, according to a French nationwide survey, in 0.026% cases after AF ablation, which is probably lower than the true incidence. 1 Diagnosing AOF is challenging, since it may occur up to 6 weeks after the procedure and the presenting symptoms – fever, cough, dyspnoea – are non-specific. 2 Fever, cough and dyspnoea, however, are also leading symptoms of COVID-19. 3 Previously, CT has been recommended for detection of AOF.4,5 In the meantime, however, AOF cases with initially negative CT findings have been reported, thus decreasing the sensitivity of chest CT for diagnosing AOF.1,2
The pathophysiology and pathogenesis of AOF after AF ablation remains poorly understood. Some hypotheses have been proposed to explain the development of AOF, such as direct thermal lesions of the oesophagus, ischaemic oesophageal injury after occlusion of the anterior oesophageal arteries, gastroesophageal reflux exacerbation, decrease in oesophageal motility by nerve lesions, or general anaesthesia. 4 It is controversially assessed whether repeated AF ablations, like in our patient, are a risk factor for the development of AOF. In one registry, the majority of AOF occurred in the course of the first ablation, whereas in another international registry, repeat procedures accounted for 55% of AOF cases.1,6
Irrespective of the unclear pathogenesis, the fatal course of the presented patient may teach us several lessons:
The diagnosis of AOF was initially considered by the emergency physician but eventually rejected because of the negative findings on chest CT. This error resulted in a potentially fatal delay of the diagnosis for more than 48 h. At admission, the patient was still free of neurological symptoms, and a prompt diagnosis with subsequent surgical therapy might have saved his life before neurological symptoms due cerebral embolism occurred.1,2 Repeat chest imaging has not been performed in our patient. This is strongly recommended, as an initial normal/unremarkable chest CT does not rule out AOF. In a recently published review, all repeat chest scans of initially negative CT investigations confirmed the diagnosis of AOF.
2
In the presence of a normal/unremarkable chest CT, the suspicion of a pathological process involving the oesophagus after AF ablation can be corroborated by the evidence of signs and symptoms of inflammation/infection and positive blood cultures for oral bacteria.1,2 Our patient presented with both of these findings. Bacteraemia and cerebral embolism lead to the false suspicion of endocarditis and an indication for TEE. It remains unknown, however, whether TEE has caused the fistula to enlarge and therefore aggravated symptoms.7,8 Oesophageal stenting and application of OTSC has been already described in patients with AOF, however carried out as a two-stage hybrid repair of acute heart surgery and endoscopic intervention 6 days later.
9
Isolated endoscopic oesophageal procedures without cardiac surgery, like in the presented patient, are associated with high mortality and are not recommended.1,2
Conclusion
Awareness of the variety of clinical manifestations and of the advantages and pitfalls of available diagnostic and therapeutic modalities should be promoted among healthcare professionals of any specialty who might be involved in the treatment of patients with AOF.
Footnotes
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Written consent to publication was given by the patient's brother
Guarantor
Claudia Stöllberger.
Contributorship
Both authors had full access to all of the data in the study. Both authors take responsibility for the accuracy of the data analysis. The paper was produced collaboratively.
Provenance
Not commissioned, peer reviewed by Sanjana Gupta.